
Pulmonary Pharmacokinetic and Pharmacodynamic Evaluation of Ampicillin/Sulbactam Regimens for Pneumonia Caused by Various Bacteria, including Acinetobacter baumannii
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Lung Tissue/Serum Ratio and Ampicillin/Sulbactam Ratio in Serum and Lung Tissue
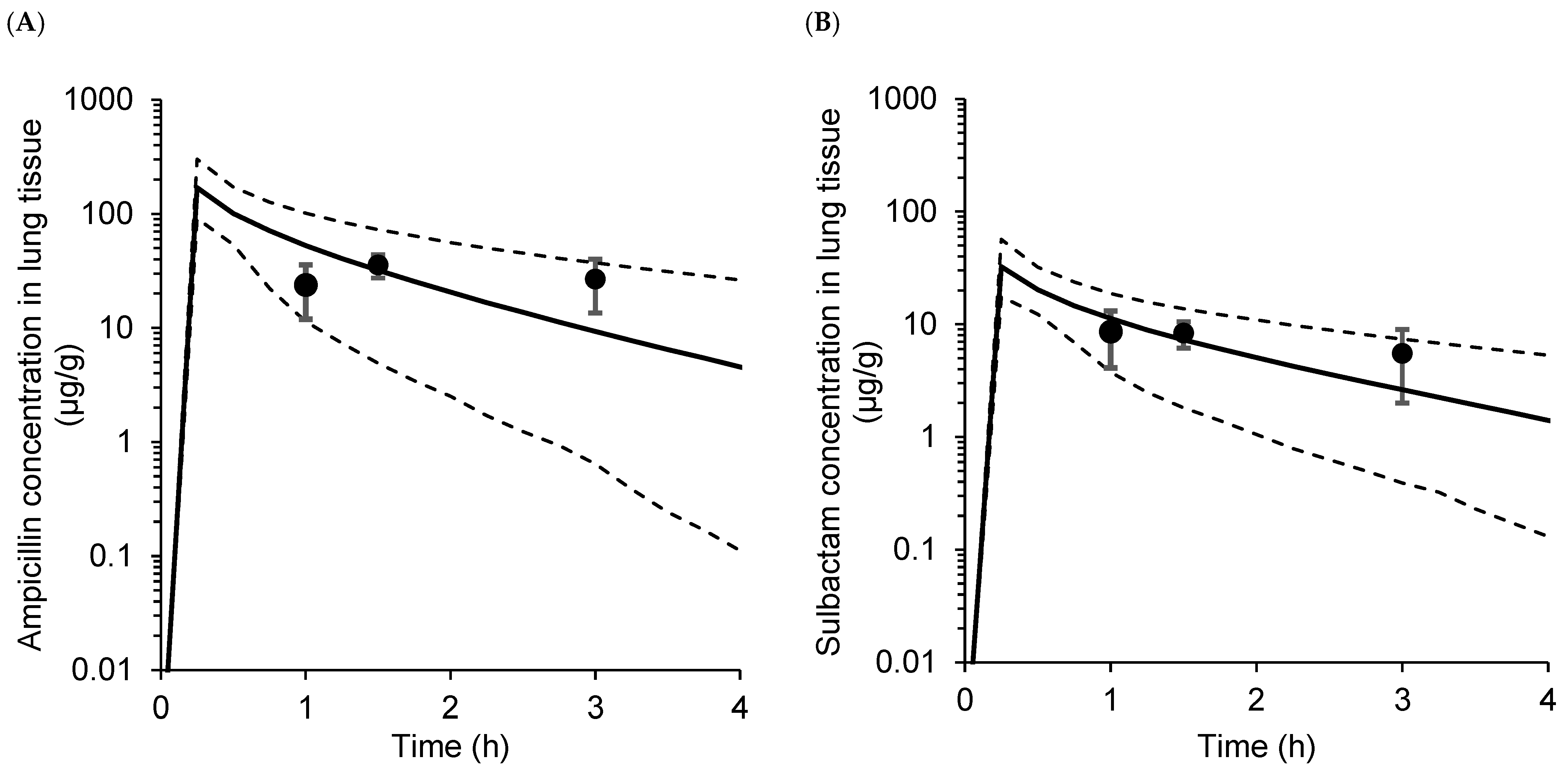
2.2. Model Validation
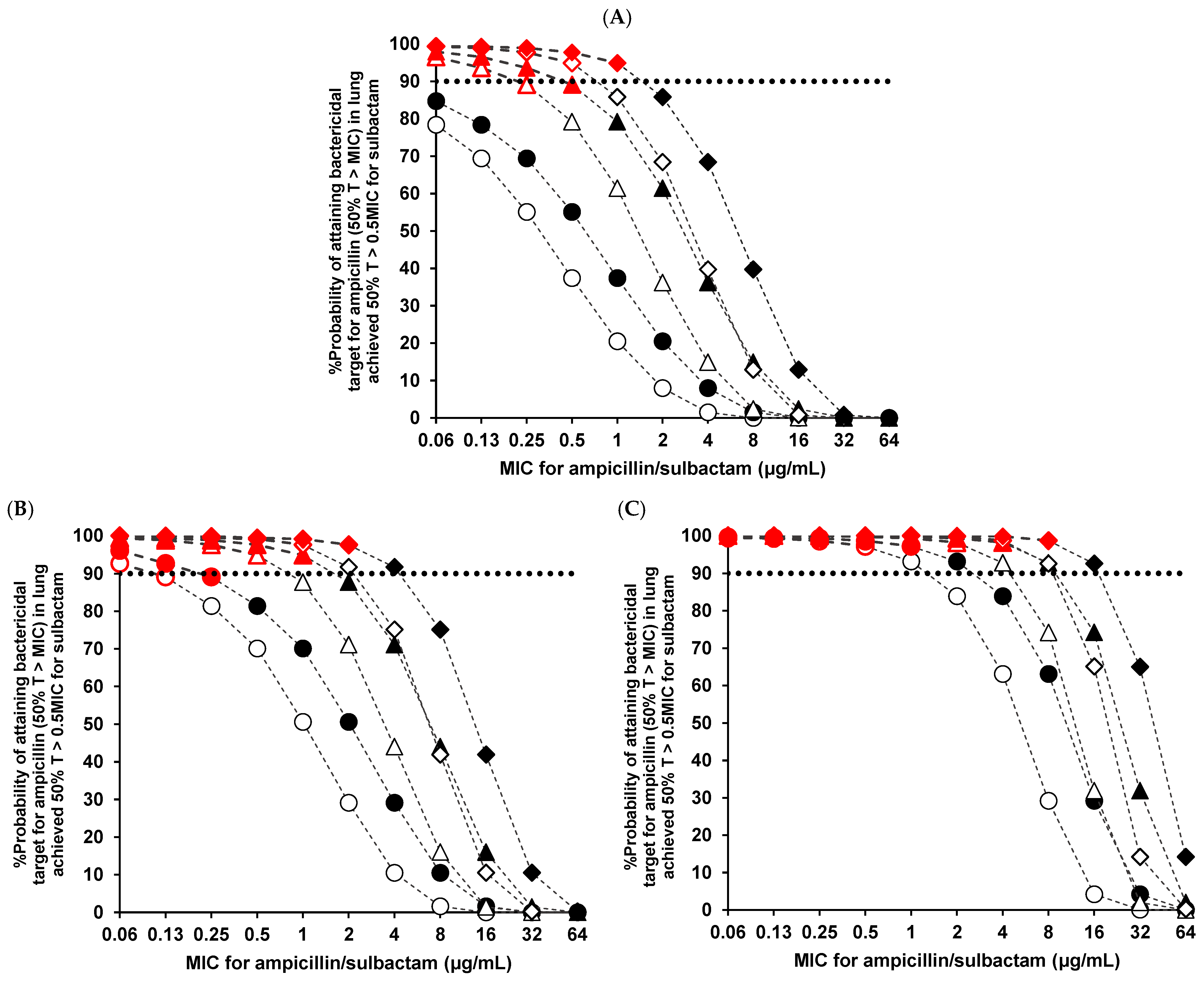
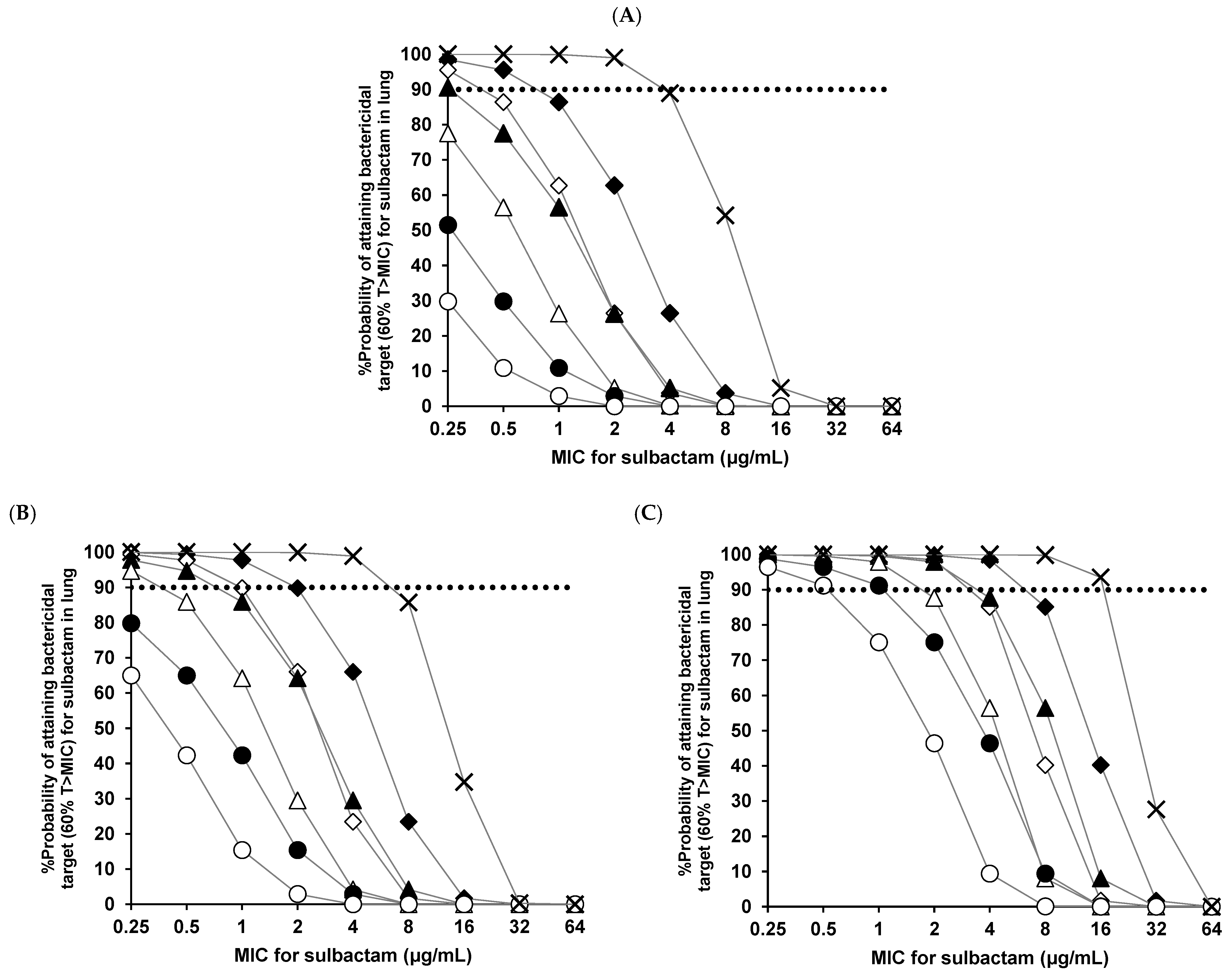
2.3. PK and PD Evaluation
3. Discussion
4. Materials and Methods
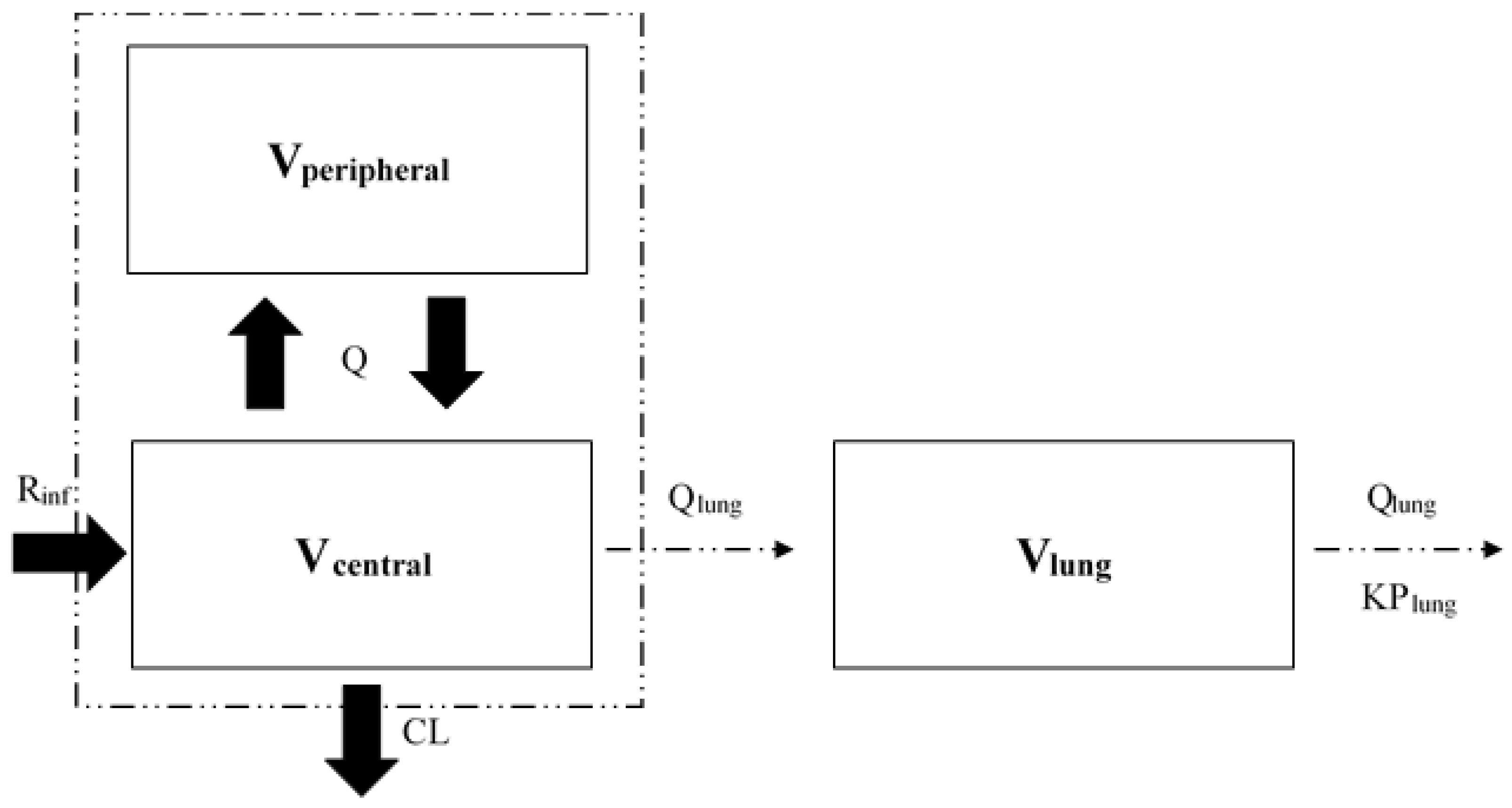
4.1. Pulmonary PK Modeling for Ampicillin and Sulbactam
4.2. Calculation of the Lung Tissue/Serum Ratio and Ampicillin/Sulbactam Ratio in Serum and Lung Tissue
4.3. Model Validation
4.4. PK/PD Simulation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- USP, UNASYN (Ampicillin Sodium/Sulbactam Sodium). 2017. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/050608s044lbl.pdf (accessed on 16 June 2021).
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M., Jr.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America; American Thoracic Society Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44, S27–S72. [Google Scholar] [CrossRef] [PubMed]
- Postma, D.F.; van Werkhoven, C.H.; van Elden, L.J.; Thijsen, S.F.; Hoepelman, A.I.; Kluytmans, J.A.; Boersma, W.G.; Compaijen, C.J.; van der Wall, E.; Prins, J.M.; et al. CAP-START Study Group Antibiotic treatment strategies for community-acquired pneumonia in adults. N. Engl. J. Med. 2015, 372, 1312–1323. [Google Scholar] [CrossRef] [PubMed]
- Wertzel, H.; Swoboda, L.; Joos-Würtemberger, A.; Frank, U.; Hasse, J. Perioperative antibiotic prophylaxis in general thoracic surgery. Thorac. Cardiovasc. Surg. 1992, 40, 326–329. [Google Scholar] [CrossRef]
- Yamazaki, S.; Yamagishi, K.; Murata, S.; Yokoyama, I.; Yahaba, M.; Takayanagi, S.; Kawasaki, Y.; Taniguchi, T.; Ishii, I.; Igari, H. Antibiotics prescriptions for pneumonia analyzed by claim information in Japan. Int. J. Clin. Pharmacol. Ther. 2021, 59, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Mikasa, K.; Aoki, N.; Aoki, Y.; Abe, S.; Iwata, S.; Ouchi, K.; Kasahara, K.; Kadota, J.; Kishida, N.; Kobayashi, O.; et al. JAID/JSC Guidelines for the Treatment of Respiratory Infectious Diseases: The Japanese Association for Infectious Diseases/Japanese Society of Chemotherapy-The JAID/JSC Guide to Clinical Management of Infectious Disease/Guideline-preparing Committee Respiratory Infectious Disease WG. J. Infect. Chemother. 2021, 22, S1–S65. [Google Scholar]
- Hasegawa, S.; Shiraishi, A.; Yaegashi, M.; Hosokawa, N.; Morimoto, K.; Mori, T. Ceftriaxone versus ampicillin/sulbactam for the treatment of aspiration-associated pneumonia in adults. J. Comp. Eff. Res. 2019, 8, 1275–1284. [Google Scholar] [CrossRef]
- Song, J.Y.; Cheong, H.J.; Choi, W.S.; Heo, J.Y.; Noh, J.Y.; Kim, W.J. Clinical and micro-biological characterization of carbapenem-resistant Acinetobacter baumannii bloodstream infections. J. Med. Microbiol. 2011, 60, 605–611. [Google Scholar] [CrossRef]
- Gaynes, R.; Edwards, J.R. National Nosocomial Infections Surveillance System Overview of nosocomial infections caused by Gram-negative bacilli. Clin. Infect. Dis. 2005, 41, 848–854. [Google Scholar]
- Peleg, A.Y.; Seifert, H.; Paterson, D.L. Acinetobacter baumannii emergence of a successful pathogen. Clin. Microbiol. Rev. 2008, 21, 538–582. [Google Scholar] [CrossRef]
- Corbella, X.; Ariza, J.; Ardanuy, C.; Vuelta, M.; Tubau, F.; Sora, M.; Pujol, M.; Gudiol, F. Efficacy of sulbactam alone and in combination with ampicillin in nosocomial infections caused by multiresistant Acinetobacter baumannii. J. Antimicrob. Chemother. 1998, 42, 793–802. [Google Scholar] [CrossRef]
- Pfizer, Incorporated. Unasyn-S (Ampicillin Sodium/Sulbactam Sodium for Injection) Prescribing Information. Available online: https://www.info.pmda.go.jp/go/interview/3/672212_6139504F1022_3_1F.pdf (accessed on 22 January 2023).
- Craig, W.A. Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men. Clin. Infect. Dis. 1998, 26, quiz 11–12. [Google Scholar] [CrossRef]
- Craig, W.A. Does the dose matter? Clin. Infect. Dis. 2001, 33, S233–S237. [Google Scholar] [CrossRef] [PubMed]
- Soto, E.; Shoji, S.; Muto, C.; Tomono, Y.; Marshall, S. Population pharmacokinetics of ampicillin and sulbactam in patients with community-acquired pneumonia: Evaluation of the impact of renal impairment. Br. J. Clin. Pharmacol. 2014, 77, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Frank, U.; Schmidt-Eisenlohr, E.; Joos-Württemberger, A.; Hasse, J.; Daschner, F. Concentrations of sulbactam/ampicillin in serum and lung tissue. Infection 1990, 18, 307–309. [Google Scholar] [CrossRef] [PubMed]
- Valcke, Y.J.; Rosseel, M.T.; Pauwels, R.A.; Bogaert, M.G.; Van der Straeten, M.E. Penetration of ampicillin and sulbactam in the lower airways during respiratory infections. Antimicrob. Agents. Chemother. 1990, 34, 958–962. [Google Scholar] [CrossRef]
- Kawasaki, K.; Niimi, H.; Ushirosako, T.; Matsunaga, T. Antibacterial activity of sulbactam ampicillin. Chemotherapy 1988, 36, 34–57. [Google Scholar]
- Onita, T.; Ikawa, K.; Nakamura, K.; Nishikawa, G.; Kobayashi, I.; Ishihara, N.; Tamaki, H.; Yano, T.; Naora, K.; Morikawa, N. Prostatic pharmacokinetic/pharmacodynamic evaluation of ampicillin-sulbactam for bacterial prostatitis and preoperative prophylaxis. J. Clin. Pharmacol. 2021, 61, 820–831. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Matsumoto, K.; Ikawa, K.; Watanabe, E.; Morikawa, N.; Takeda, Y. Population pharmacokinetic-pharmacodynamic target attainment analysis of sulbactam in patients with impaired renal function: Dosing considerations for Acinetobacter baumannii infections. J. Infect. Chemother. 2015, 21, 284–289. [Google Scholar] [CrossRef]
- Suzuki, T.; Sugiyama, E.; Nozawa, K.; Tajima, M.; Takahashi, K.; Yoshii, M.; Suzuki, H.; Sato, V.H.; Sato, H. Effects of dosing frequency on the clinical efficacy of ampicillin/sulbactam in Japanese elderly patients with pneumonia: A single- center retrospective observational study. Pharmacol. Res. Perspect. 2021, 9, e00746. [Google Scholar] [CrossRef]
- Betrosian, A.P.; Frantzeskaki, F.; Xanthaki, A.; Georgiadis, G. High-dose ampicillin-sulbactam as an alternative treatment of late-onset VAP from multidrug-resistant Acinetobacter baumannii. Scand. J. Infect. Dis. 2007, 39, 38–43. [Google Scholar] [CrossRef]
- Gilbert, D.N.; Chambers, H.F.; Saag, M.S.; Pavia, A.T.; Boucher, H.W. The Sanford Guide to Antimicrobial Therapy 51th ed. Sanford Guide; Life Science Publishing: Tokyo, Japan, 2021; pp. 70–71. [Google Scholar]
- Langdon, G.; Gueorguieva, I.; Aarons, L.; Karlsson, M. Linking preclinical and clinical whole-body physiologically based pharmacokinetic models with prior distributions in NONMEM. Eur. J. Clin. Pharmacol. 2007, 63, 485–498. [Google Scholar] [CrossRef]
- Brown, R.P.; Delp, M.D.; Lindstedt, S.L.; Rhomberg, L.R.; Beliles, R.P. Physiological parameter values for physiologically based pharmacokinetic models. Toxicol. Ind. Health. 1997, 13, 407–484. [Google Scholar] [CrossRef]
- Marchand, S.; Chenel, M.; Lamarche, I.; Couet, W. Pharmacokinetic modeling of free amoxicillin concentrations in rat muscle extracellular fluids determined by microdialysis. Antimicrob Agents Chemother. 2005, 49, 3702–3706. [Google Scholar] [CrossRef] [Green Version]
- Germovsek, E.; Lutsar, I.; Kipper, K.; Karlsson, M.O.; Planche, T.; Chazallon, C.; Meyer, L.; Trafojer, U.M.T.; Metsvaht, T.; Fournier, I.; et al. Plasma and CSF pharmacokinetics of meropenem in neonates and young infants: Results from the NeoMero studies. J. Antimicrob. Chemother. 2018, 73, 1908–1916. [Google Scholar] [CrossRef]
- Sasongko, L.; Williams, K.M.; Day, R.O.; McLachlan, A.J. Human subcutaneous tissue distribution of fluconazole: Comparison of microdialysis and suction blister techniques. Br. J. Clin. Pharmacol. 2003, 56, 551–561. [Google Scholar] [CrossRef]
- Ohata, Y.; Tomita, Y.; Sunakawa, K.; Drusano, G.L.; Tanigawara, Y. Cerebrospinal pharmacokinetic and pharmacodynamic analysis of efficacy of meropenem in paediatric patients with bacterial meningitis. Int. J. Antimicrob. Agents 2019, 54, 292–300. [Google Scholar] [CrossRef]
- Jacobs, M.R. Optimisation of antimicrobial therapy using pharmacokinetic and pharmacodynamic parameters. Clin. Microbiol. Infect. 2001, 7, 589–596. [Google Scholar] [CrossRef]
- Drusano, G.L. Prevention of resistance: A goal for dose selection for antimicrobial agents. Clin. Infect. Dis. 2003, 36, S42–S50. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute-CLSI. M100-ED31:2021 Performance Standards for Antimicrobial Susceptibility Testing, 31st Edition. Available online: http://em100.edaptivedocs.net/dashboard.aspx (accessed on 16 June 2021).
- Yokoyama, Y.; Matsumoto, K.; Ikawa, K.; Watanabe, E.; Shigemi, A.; Umezaki, Y.; Nakamura, K.; Ueno, K.; Morikawa, N.; Takeda, Y. Pharmacokinetic/pharmacodynamic evaluation of sulbactam against Acinetobacter baumannii in in vitro and murine thigh and lung infection models. Int. J. Antimicrob. Agents 2014, 43, 547–552. [Google Scholar] [CrossRef]
- Tateda, K.; Ohno, A.; Ishii, Y.; Murakami, H.; Yamaguchi, K. Surveillance of in vitro susceptibilities to levofloxacin and various antibacterial agents for 11,705 clinical isolates obtained from 65 centers in 2016. Jpn. J. Antibiotics. 2018, 298, 71–76. [Google Scholar]
- Yanagihara, K.; Matsumoto, T.; Tokimatsu, I.; Tsukada, H.; Fujikura, Y.; Miki, M.; Morinaga, Y.; Sato, J.; Wakamura, T.; Kiyota, H.; et al. Nationwide surveillance of bacterial respiratory pathogens conducted by the surveillance committee of japanese society of chemotherapy, the japanese association for infectious diseases, and the Japanese society for clinical microbiology in 2016: General view of the pathogens’ antibacterial susceptibility. J. Infect. Chemother. 2020, 26, 873–881. [Google Scholar] [PubMed]
- Kaneko, A.; Yamane, N.; Watanabe, D.; Mizusawa, N.; Matsuzaki, K.; Hasegawa, M.; Sato, Y.; Kobayashi, I. Treatment of aspiration pneumonia based on the antimicrobial susceptibility pattern of oral bacterial pathogens. Jpn. J. Chemother. 2007, 55, 378–381. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Specimen and Parameter | Value | ||
|---|---|---|---|
| Ampicillin 2.0 g (15 subjects) | Sulbactam 1.0 g (15 subjects) | Ampicillin/ Sulbactam Ratio (2.0 g/1.0 g) | |
| Serum | |||
| Cmax (μg/mL) | 40.8 | 25.3 | 1.61 |
| AUC0–3h (μg·h/mL) | 83.5 | 51.2 | 1.63 |
| Lung tissue | |||
| Cmax (μg/g) | 35.6 | 8.6 | 4.14 |
| AUC0–3h (μg·h/g) | 73.6 | 18.9 | 3.89 |
| Lung tissue/serum ratio | |||
| Cmax | 0.873 | 0.339 | |
| AUC0–3h | 0.881 | 0.368 | |
| Ampicillin/Sulbactam Regimen | Bactericidal Target (50% T > MIC for Ampicillin) and 50% T > 0.5 MIC for Sulbactam |
|---|---|
| CLcr = 90 mL/min | |
| 1.5 g twice daily, 0.5-h infusion (total 3 g/day) | - |
| 3.0 g twice daily, 0.5-h infusion (total 6 g/day) | - |
| 1.5 g three times daily, 0.5-h infusion (total 4.5 g/day) | 0.13 |
| 3.0 g three times daily, 0.5-h infusion (total 9 g/day) | 0.25 |
| 1.5 g four times daily, 0.5-h infusion (total 6 g/day) | 0.5 |
| 3.0 g four times daily, 0.5-h infusion (total 12 g/day) | 1 |
| CLcr = 60 mL/min | |
| 1.5 g twice daily, 0.5-h infusion (total 3 g/day) | 0.06 |
| 3.0 g twice daily, 0.5-h infusion (total 6 g/day) | 0.13 |
| 1.5 g three times daily, 0.5-h infusion (total 4.5 g/day) | 0.5 |
| 3.0 g three times daily, 0.5-h infusion (total 9 g/day) | 1 |
| 1.5 g four times daily, 0.5-h infusion (total 6 g/day) | 1 |
| 3.0 g four times daily, 0.5-h infusion (total 12 g/day) | 2 |
| CLcr = 30 mL/min | |
| 1.5 g twice daily, 0.5-h infusion (total 3 g/day) | 0.5 |
| 3.0 g twice daily, 0.5-h infusion (total 6 g/day) | 1 |
| 1.5 g three times daily, 0.5-h infusion (total 4.5 g/day) | 2 |
| 3.0 g three times daily, 0.5-h infusion (total 9 g/day) | 4 |
| 1.5 g four times daily, 0.5-h infusion (total 6 g/day) | 4 |
| 3.0 g four times daily, 0.5-h infusion (total 12 g/day) | 8 |
| Ampicillin/Sulbactam Regimen | Bactericidal Target 60% T > MIC for Sulbactam |
|---|---|
| CLcr = 90 mL/min | |
| 3.0 g twice daily, 0.5-h infusion (total 6 g/day) | - |
| 6.0 g twice daily, 0.5-h infusion (total 12 g/day) | - |
| 3.0 g three times daily, 0.5-h infusion (total 9 g/day) | 0.13 |
| 6.0 g three times daily, 0.5-h infusion (total 18 g/day) | 0.25 |
| 3.0 g four times daily, 0.5-h infusion (total 12 g/day) | 0.25 |
| 6.0 g four times daily, 0.5-h infusion (total 24 g/day) | 0.5 |
| 9.0 g three times daily, 4-h infusion (total 27 g/day) | 2 |
| CLcr = 60 mL/min | |
| 3.0 g twice daily, 0.5-h infusion (total 6 g/day) | - |
| 6.0 g twice daily, 0.5-h infusion (total 12 g/day) | 0.06 |
| 3.0 g three times daily, 0.5-h infusion (total 9 g/day) | 0.25 |
| 6.0 g three times daily, 0.5-h infusion (total 18 g/day) | 0.5 |
| 3.0 g four times daily, 0.5-h infusion (total 12 g/day) | 0.5 |
| 6.0 g four times daily, 0.5-h infusion (total 24 g/day) | 1 |
| 9.0 g three times daily, 4-h infusion (total 27 g/day) | 4 |
| CLcr = 30 mL/min | |
| 3.0 g twice daily, 0.5-h infusion (total 6 g/day) | 0.5 |
| 6.0 g twice daily, 0.5-h infusion (total 12 g/day) | 1 |
| 3.0 g three times daily, 0.5-h infusion (total 9 g/day) | 1 |
| 6.0 g three times daily, 0.5-h infusion (total 18 g/day) | 2 |
| 3.0 g four times daily, 0.5-h infusion (total 12 g/day) | 2 |
| 6.0 g four times daily, 0.5-h infusion (total 24 g/day) | 4 |
| 9.0 g three times daily, 4-h infusion (total 27 g/day) | 16 |
| Parameter | Ampicillin | Sulbactam |
|---|---|---|
| Value (RSE%) | Value (RSE%) | |
| Fixed-effects parameter | ||
| CL (L/h) = θCL × (CLcr/68.3)θCLcr on CL | ||
| θCL(L/h) a | 11.03 (5.1) | 10.50 (5.0) |
| θCLcr on CL a | 0.831 (14.1) | 0.774 (18.6) |
| Vcentral (L) = θVcentral a | 7.80 (5.9) | 8.96 (9.6) |
| Q (L/h) = θQ a | 7.07 (14.3) | 7.29 (21.4) |
| Vperipheral (L) = θVperipheral a | 3.98 (12.3) | 4.93 (13.4) |
| KPlung = θKPlung b | 0.881 Fixed | 0.368 Fixed |
| Qlung(L/h) = θQlung c | 207 Fixed | 207 Fixed |
| Vlung(kg) = θVlung c | 0.47 Fixed | 0.47 Fixed |
| Interindividual variability (exponential error model) | ||
| ηCL a | 0.0985 (26.1) | 0.0626 (26.8) |
| ηVcentral a | 0.160 (21.3) | 0.147 (27.5) |
| ηQ a | 0.588 (44.2) | 0.399 (48.4) |
| ηVperipheral a | 0.298 (37.2) | 0.177 (37.9) |
| Residual variability (additive error model) | ||
| ε a | 2.70 (26.2) | 1.22 (38.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onita, T.; Ikawa, K.; Ishihara, N.; Tamaki, H.; Yano, T.; Naora, K.; Morikawa, N. Pulmonary Pharmacokinetic and Pharmacodynamic Evaluation of Ampicillin/Sulbactam Regimens for Pneumonia Caused by Various Bacteria, including Acinetobacter baumannii. Antibiotics 2023, 12, 303. https://doi.org/10.3390/antibiotics12020303
Onita T, Ikawa K, Ishihara N, Tamaki H, Yano T, Naora K, Morikawa N. Pulmonary Pharmacokinetic and Pharmacodynamic Evaluation of Ampicillin/Sulbactam Regimens for Pneumonia Caused by Various Bacteria, including Acinetobacter baumannii. Antibiotics. 2023; 12(2):303. https://doi.org/10.3390/antibiotics12020303
Chicago/Turabian StyleOnita, Tetsushu, Kazuro Ikawa, Noriyuki Ishihara, Hiroki Tamaki, Takahisa Yano, Kohji Naora, and Norifumi Morikawa. 2023. "Pulmonary Pharmacokinetic and Pharmacodynamic Evaluation of Ampicillin/Sulbactam Regimens for Pneumonia Caused by Various Bacteria, including Acinetobacter baumannii" Antibiotics 12, no. 2: 303. https://doi.org/10.3390/antibiotics12020303