
Antibiotic Resistance of Haemophilus influenzae in Nasopharyngeal Carriage of Children with Acute Otitis Media and in Middle Ear Fluid from Otorrhea

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
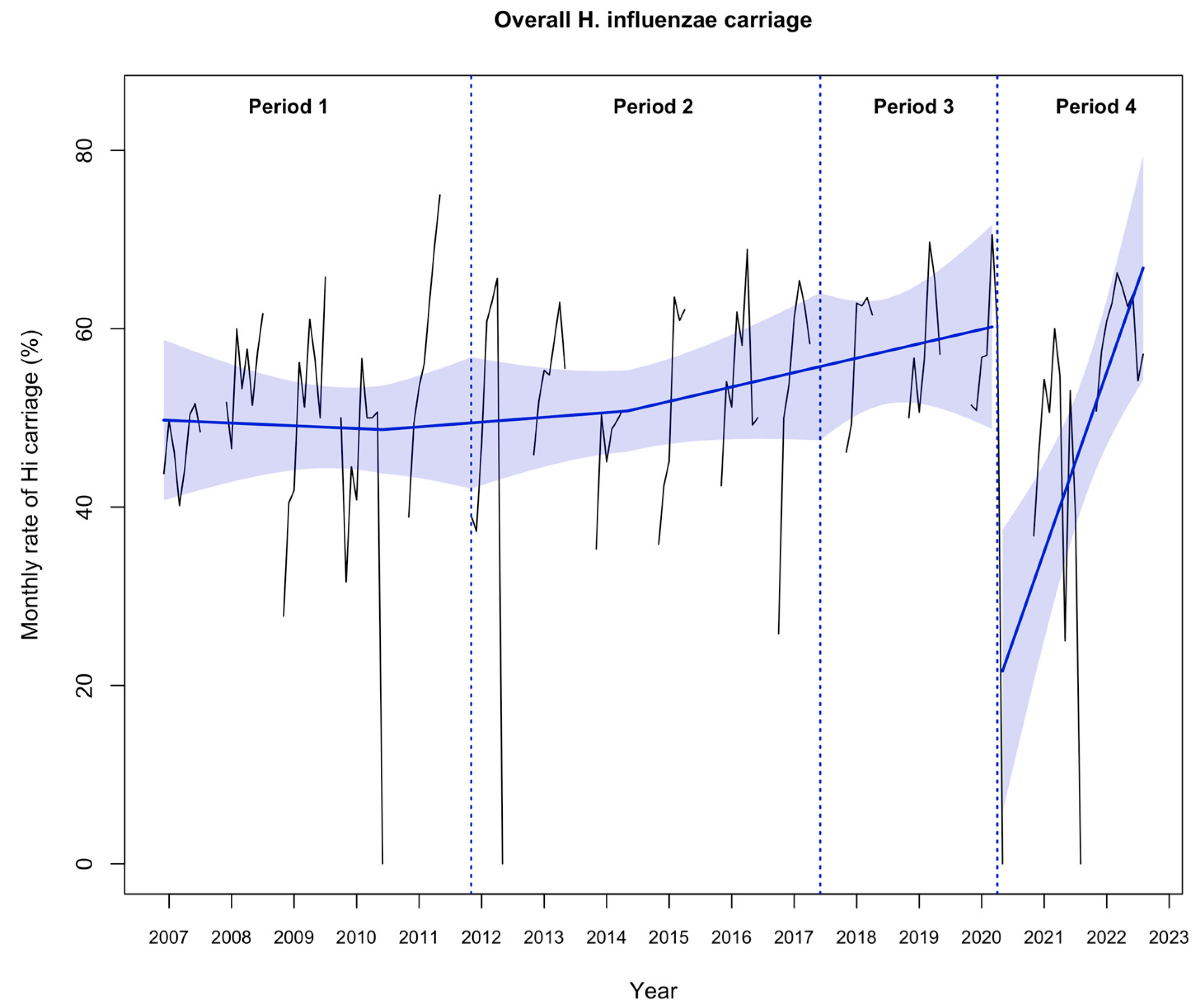
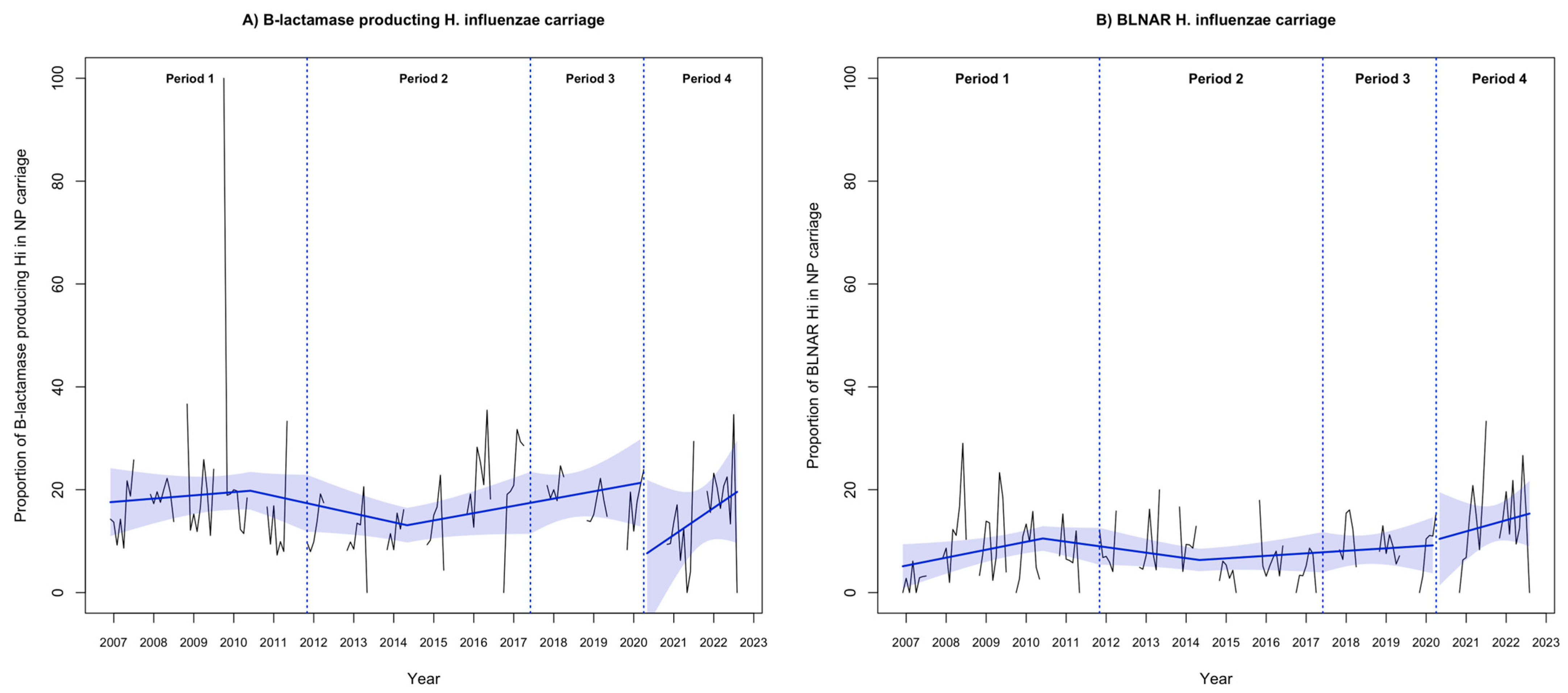
2.2. Nasopharyngeal Carriage and β-Lactam Resistance in Haemophilus Influenzae Strains
2.3. Factors Associated with Nasopharyngeal Carriage of Antibiotic-Resistant Hi Strains
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Sampling and Microbiological Investigations
4.3. Study Periods
4.4. Outcome Measures
4.5. Statistical Analysis
4.6. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sabuncu, E.; David, J.; Bernède-Bauduin, C.; Pépin, S.; Leroy, M.; Boëlle, P.-Y.; Watier, L.; Guillemot, D. Significant reduction of antibiotic use in the community after a nationwide campaign in France, 2002–2007. PLoS Med. 2009, 6, e1000084. [Google Scholar] [CrossRef]
- Hu, T.; Done, N.; Petigara, T.; Mohanty, S.; Song, Y.; Liu, Q.; Lemus-Wirtz, E.; Signorovitch, J.; Sarpong, E.; Weiss, T. Incidence of acute otitis media in children in the United States before and after the introduction of 7- and 13-valent pneumococcal conjugate vaccines during 1998–2018. BMC Infect. Dis. 2022, 22, 294. [Google Scholar] [CrossRef] [PubMed]
- Gehanno, P.; Panajotopoulos, A.; Barry, B.; Nguyen, L.; Levy, D.; Bingen, E.; Berche, P. Microbiology of otitis media in the Paris, France, area from 1987 to 1997. Pediatr. Infect. Dis. J. 2001, 20, 570–573. [Google Scholar] [CrossRef] [PubMed]
- Potts, C.C.; Rodriguez-Rivera, L.D.; Retchless, A.C.; Buono, S.A.; Chen, A.T.; Marjuki, H.; Blain, A.E.; Wang, X. Antimicrobial Susceptibility Survey of Invasive Haemophilus influenzae in the United States in 2016. Microbiol. Spectr. 2022, 10, e0257921. [Google Scholar] [CrossRef] [PubMed]
- Wald, E.R.; DeMuri, G.P. Commentary: Antibiotic recommendations for acute otitis media and acute bacterial sinusitis in 2013--the conundrum. Pediatr. Infect. Dis. J. 2013, 32, 641–643. [Google Scholar] [CrossRef]
- Pichichero, M.E.; Wright, T. The use of tympanocentesis in the diagnosis and management of acute otitis media. Curr. Infect. Dis. Rep. 2006, 8, 189–195. [Google Scholar] [CrossRef]
- van Dongen, T.M.A.; van der Heijden, G.J.M.G.; van Zon, A.; Bogaert, D.; Sanders, E.A.M.; Schilder, A.G.M. Evaluation of Concordance Between the Microorganisms Detected in the Nasopharynx and Middle Ear of Children with Otitis Media. Pediatr. Infect. Dis. J. 2013, 32, 549–552. [Google Scholar] [CrossRef]
- Ouldali, N.; Bellêttre, X.; Milcent, K.; Guedj, R.; De Pontual, L.; Cojocaru, B.; Soussan-Banini, V.; Craiu, I.; Skurnik, D.; Gajdos, V.; et al. Impact of Implementing National Guidelines on Antibiotic Prescriptions for Acute Respiratory Tract Infections in Pediatric Emergency Departments: An Interrupted Time Series Analysis. Clin. Infect. Dis. 2017, 65, 1469–1476. [Google Scholar] [CrossRef]
- Levy, C.; Varon, E.; Bidet, P.; Béchet, S.; Batard, C.; Wollner, A.; Thollot, F.; Bonacorsi, S.; Cohen, R. Otorrhea bacterial profile, epidemiology before widespread use of the third-generation pneumococcal conjugate vaccine in French children, a prospective study from 2015 to 2023. Infect. Dis. Now 2023, 53, 104738. [Google Scholar] [CrossRef]
- Taha, A.; Adeline, F.; Taha, M.-K.; Deghmane, A.-E. Haemophilus influenzae drug resistance in France from 2017 to 2021: Consideration for treatment of otitis media. J. Glob. Antimicrob. Resist. 2022, 31, 222–227. [Google Scholar] [CrossRef]
- Launay, T.; Souty, C.; Vilcu, A.-M.; Turbelin, C.; Blanchon, T.; Guerrisi, C.; Hanslik, T.; Colizza, V.; Bardoulat, I.; Lemaître, M.; et al. Common communicable diseases in the general population in France during the COVID-19 pandemic. PLoS ONE 2021, 16, e0258391. [Google Scholar] [CrossRef] [PubMed]
- Alde, M.; Di Berardino, F.; Marchisio, P.; Cantarella, G.; Ambrosetti, U.; Consonni, D.; Zanetti, D. Effects of COVID-19 Lockdown on Otitis Media With Effusion in Children: Future Therapeutic Implications. Otolaryngol. Head Neck Surg. 2021, 165, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Maison, N.; Peck, A.; Illi, S.; Meyer-Buehn, M.; Von Mutius, E.; Hübner, J.; Von Both, U. The rising of old foes: Impact of lockdown periods on “non-SARS-CoV-2” viral respiratory and gastrointestinal infections. Infection 2022, 50, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Shaw, D.; Abad, R.; Amin-Chowdhury, Z.; Bautista, A.; Bennett, D.; Broughton, K.; Cao, B.; Casanova, C.; Choi, E.H.; Chu, Y.-W.; et al. Trends in invasive bacterial diseases during the first 2 years of the COVID-19 pandemic: Analyses of prospective surveillance data from 30 countries and territories in the IRIS Consortium. Lancet Digit. Health 2023, 5, e582–e593. [Google Scholar] [CrossRef]
- Rose, M.A.; Laurenz, M.; Sprenger, R.; Imöhl, M.; van der Linden, M. Nasopharyngeal Carriage in Children After the Introduction of Generalized Infant Pneumococcal Conjugate Vaccine Immunization in Germany. Front. Med. 2021, 8, 719481. [Google Scholar] [CrossRef]
- Vergison, A. Microbiology of otitis media: A moving target. Vaccine 2008, 26 (Suppl. 7), G5–G10. [Google Scholar] [CrossRef]
- Imöhl, M.; Perniciaro, S.; Busse, A.; van der Linden, M. Bacterial Spectrum of Spontaneously Ruptured Otitis Media in a 7-Year, Longitudinal, Multicenter, Epidemiological Cross-Sectional Study in Germany. Front. Med. 2021, 8, 675225. [Google Scholar] [CrossRef]
- Cilveti, R.; Olmo, M.; Pérez-Jove, J.; Picazo, J.-J.; Arimany, J.-L.; Mora, E.; Pérez-Porcuna, T.M.; Aguilar, I.; Alonso, A.; Molina, F.; et al. Epidemiology of Otitis Media with Spontaneous Perforation of the Tympanic Membrane in Young Children and Association with Bacterial Nasopharyngeal Carriage, Recurrences and Pneumococcal Vaccination in Catalonia, Spain—The Prospective HERMES Study. PLoS ONE 2017, 12, e0170316. [Google Scholar] [CrossRef]
- Sugita, G.; Hotomi, M.; Sugita, R.; Kono, M.; Togawa, A.; Yamauchi, K.; Funaki, T.; Yamanaka, N. Genetic characteristics of Haemophilus influenzae and Streptococcus pneumoniae isolated from children with conjunctivitis-otitis media syndrome. J. Infect. Chemother. 2014, 20, 493–497. [Google Scholar] [CrossRef]
- Suzuki, H.G.; Dewez, J.E.; Nijman, R.G.; Yeung, S. Clinical practice guidelines for acute otitis media in children: A systematic review and appraisal of European national guidelines. BMJ Open 2020, 10, e035343. [Google Scholar] [CrossRef]
- Rybak, A.; Levy, C.; Ouldali, N.; Bonacorsi, S.; Béchet, S.; Delobbe, J.-F.; Batard, C.; Donikian, I.; Goldrey, M.; Assouline, J.; et al. Dynamics of Antibiotic Resistance of Streptococcus pneumoniae in France: A Pediatric Prospective Nasopharyngeal Carriage Study from 2001 to 2022. Antibiotics 2023, 12, 1020. [Google Scholar] [CrossRef]
- Wen, S.; Feng, D.; Chen, D.; Yang, L.; Xu, Z. Molecular epidemiology and evolution of Haemophilus influenzae. Infect. Genet. Evol. 2020, 80, 104205. [Google Scholar] [CrossRef] [PubMed]
- Nørskov-Lauritsen, N.; Ridderberg, W.; Erikstrup, L.T.; Fuursted, K. Evaluation of disk diffusion methods to detect low-level β-lactamase-negative ampicillin-resistant Haemophilus influenzae. Apmis 2011, 119, 385–392. [Google Scholar] [CrossRef]
- Ben-Ami, R.; Rodríguez-Baño, J.; Arslan, H.; Pitout, J.D.D.; Quentin, C.; Calbo, E.S.; Azap, K.; Arpin, C.; Pascual, A.; Livermore, D.M.; et al. A Multinational Survey of Risk Factors for Infection with Extended-Spectrum β-Lactamase–Producing Enterobacteriaceae in Nonhospitalized Patients. Clin. Infect. Dis. 2009, 49, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Witherden, E.A.; Montgomery, J.; Henderson, B.; Tristram, S.G. Prevalence and genotypic characteristics of β-lactamase-negative ampicillin-resistant Haemophilus influenzae in Australia. J. Antimicrob. Chemother. 2011, 66, 1013–1015. [Google Scholar] [CrossRef] [PubMed]
- EUCAST Clinical Breakpoints. Available online: https://www.eucast.org/clinical_breakpoints (accessed on 1 September 2023).
- Paradise, J.L. On classifying otitis media as suppurative or nonsuppurative, with a suggested clinical schema. J. Pediatr. 1987, 111, 948–951. [Google Scholar] [CrossRef] [PubMed]
- Levy, C.; Varon, E.; Ouldali, N.; Wollner, A.; Thollot, F.; Corrard, F.; Werner, A.; Béchet, S.; Bonacorsi, S.; Cohen, R. Bacterial causes of otitis media with spontaneous perforation of the tympanic membrane in the era of 13 valent pneumococcal conjugate vaccine. PLoS ONE 2019, 14, e0211712. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Nasopharyngeal Carriage a (n = 13,865) | Otorrhea b (n = 783) | ||||
|---|---|---|---|---|---|---|
| Period 1 | Period 2 | Period 3 | Period 4 | Total | ||
| Male, n (%) | 2366 (52.7) | 2896 (53.7) | 1319 (51.9) | 819 (56.8) | 7400 (53.4) | 409 (52.2) |
| Age (months), median (IQR) | 12.7 (9.4–17.3) | 13.1 (9.5–17.4) | 12.4 (9.1–17.1) | 12.4 (9.0–17.0) | 12.7 (9.3–17.3) | 20 (12.3–37.8) |
| Daycare/school attendance, n (%) | 1904/4484 (42.5) | 2800 (51.9) | 1524 (59.9) | 936/1438 (65.1) | 7164/13,859 (51.7) | 592 (75.6) |
| Siblings, n (%) | 2517/4486 (56.1) | 3071 (56.9) | 1470/2541 (57.8) | 817 (56.7) | 7875/13,863 (56.8) | NA |
| Otalgia, n (%) | 3333/4484 (74.3) | 3794 (70.3) | 1575 (62.0) | 962/1424 (67.6) | 9664/13,845 (69.8) | 559/780 (71.7) |
| Fever (temperature ≥38.5 °C), n (%) | 2616/4452 (58.8) | 2977/5335 (55.8) | 1333/2491 (53.5) | 691/1430 (48.3) | 7617/13,708 (55.6) | 248/769 (32.2) |
| Conjunctivitis, n (%) | 1152/4485 (25.7) | 1567 (29.0) | 668 (26.3) | 380/1437 (26.4) | 3767/13,859 (27.2) | 86/783 (11.0) |
| Otorrhea, n (%) | 356 (7.9) | 382/5394 (7.1) | 222 (8.7) | 85/1439 (5.9) | 1046/13,862 (7.5) | 783 (100) |
| Bilateral AOM, n (%) | 1009/1926 (52.4) | 2701/5394 (50.1) | 1201 (47.6) | 467/1436 (32.5) | 5387/11,298 (47.7) | 136/782 (17.4) |
| History of AOM, n (%) | 1573/2795 (56.3) | 2882 (53.4) | 1244 (48.9) | 674 (46.8) | 6373/12,173 (52.3) | NA |
| History of otorrhea, n (%) | NA | NA | NA | NA | NA | 50/782 (6.4) |
| Otitis-prone children, n (%) | 528/2795 (18.9) | 888 (16.5) | 339 (13.3) | 215/1440 (14.9) | 1970/12,172 (16.2) | NA |
| Recent use of ATB c, n (%) | 2073/4483 (46.2) | 2187 (40.5) | 918/2541 (36.1) | 474 (32.9) | 5652/13,860 (40.8) | 36/783 (4.6) |
| Broad-spectrum ATB d, n (%) | 1899/2066 (91.9) | 928/2179 (33.9) | 309/912 (33.9) | 137/468 (29.3) | 3273/5,625 (58.2) | NA |
| Carriage Study Periods 3 and 4 a n = 3983 (%) | Otorrhea Study b n = 783 (%) | p-Value c | |
|---|---|---|---|
| Hi-positive cultures | 2235 (56.1) | 177 (22.6) | <0.001 |
| β-lactamase-producing strains | 392/2230 (17.6) | 22/175 (12.6) | 0.11 |
| BLNAR strains | 254/2900 (8.8) | 13/175 (7.4) | 0.64 |
| Serogroup b | 0/2225 | 0 (0) | . |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | aOR | 95% CI | p-Value | |
| Nasopharyngeal carriage of β-lactamase-producing Hi (n = 1439) | ||||||
| Age < 1 year | 0.84 | 0.58 to 1.22 | 0.36 | |||
| Siblings | 0.87 | 0.60 to 1.25 | 0.45 | |||
| Recent use of antibiotics a | 0.92 | 0.62 to 1.36 | 0.66 | |||
| Recent use of broad antibiotics b | 1.11 | 0.61 to 2.04 | 0.73 | |||
| Daycare center attendance | 1.42 | 0.95 to 2.14 | 0.09 | |||
| Fever (temperature ≥ 38.5 °C) | 1.11 | 0.77 to 1.62 | 0.56 | |||
| Otalgia | 0.89 | 0.60 to 1.31 | 0.56 | |||
| History of AOM | 1.13 | 0.78 to 1.63 | 0.52 | |||
| Otitis-prone children | 1.09 | 0.66 to 1.80 | 0.73 | |||
| Otorrhea | 0.79 | 0.33 to 1.84 | 0.58 | |||
| Conjunctivitis | 2.35 | 1.61 to 3.42 | <0.001 | 2.19 | 1.49 to 3.21 | <0.001 |
| Bilateral AOM | 1.65 | 1.14 to 2.40 | 0.008 | 1.48 | 1.01 to 2.17 | 0.04 |
| Nasopharyngeal carriage of BLNAR Hi (n = 1441) | ||||||
| Age < 1 year | 0.84 | 0.56 to 1.24 | 0.38 | |||
| Siblings | 0.89 | 0.60 to 1.32 | 0.57 | |||
| Recent use of antibiotics a | 0.84 | 0.54 to 1.28 | 0.41 | |||
| Recent use of broad antibiotics b | 1.07 | 0.56 to 2.05 | 0.83 | |||
| Daycare center attendance | 1.88 | 1.19 to 2.98 | 0.007 | 1.71 | 1.07 to 2.74 | 0.02 |
| Fever (temperature ≥ 38.5 °C) | 1.39 | 0.94 to 2.06 | 0.10 | 1.56 | 1.04 to 2.35 | 0.03 |
| Otalgia | 0.99 | 0.65 to 1.50 | 0.95 | |||
| History of AOM | 0.96 | 0.65 to 1.42 | 0.84 | |||
| Otitis-prone children | 0.69 | 0.37 to 1.27 | 0.23 | |||
| Otorrhea | 0.43 | 0.13 to 1.39 | 0.16 | |||
| Conjunctivitis | 3.86 | 2.59 to 5.74 | <0.001 | 3.98 | 2.66 to 5.96 | <0.001 |
| Bilateral AOM | 1.70 | 1.14 to 2.53 | 0.008 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assad, Z.; Cohen, R.; Varon, E.; Levy, C.; Bechet, S.; Corrard, F.; Werner, A.; Ouldali, N.; Bonacorsi, S.; Rybak, A. Antibiotic Resistance of Haemophilus influenzae in Nasopharyngeal Carriage of Children with Acute Otitis Media and in Middle Ear Fluid from Otorrhea. Antibiotics 2023, 12, 1605. https://doi.org/10.3390/antibiotics12111605
Assad Z, Cohen R, Varon E, Levy C, Bechet S, Corrard F, Werner A, Ouldali N, Bonacorsi S, Rybak A. Antibiotic Resistance of Haemophilus influenzae in Nasopharyngeal Carriage of Children with Acute Otitis Media and in Middle Ear Fluid from Otorrhea. Antibiotics. 2023; 12(11):1605. https://doi.org/10.3390/antibiotics12111605
Chicago/Turabian StyleAssad, Zein, Robert Cohen, Emmanuelle Varon, Corinne Levy, Stéphane Bechet, François Corrard, Andreas Werner, Naïm Ouldali, Stéphane Bonacorsi, and Alexis Rybak. 2023. "Antibiotic Resistance of Haemophilus influenzae in Nasopharyngeal Carriage of Children with Acute Otitis Media and in Middle Ear Fluid from Otorrhea" Antibiotics 12, no. 11: 1605. https://doi.org/10.3390/antibiotics12111605