
Effectiveness of Educational Interventions for Health Workers on Antibiotic Prescribing in Outpatient Settings in China: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.2.1. Participants
2.2.2. Interventions
2.2.3. Comparisons and Outcomes
2.2.4. Study Design
2.3. Data Extracting
2.4. Risk of Bias Assessment
2.5. Data Analysis
3. Results
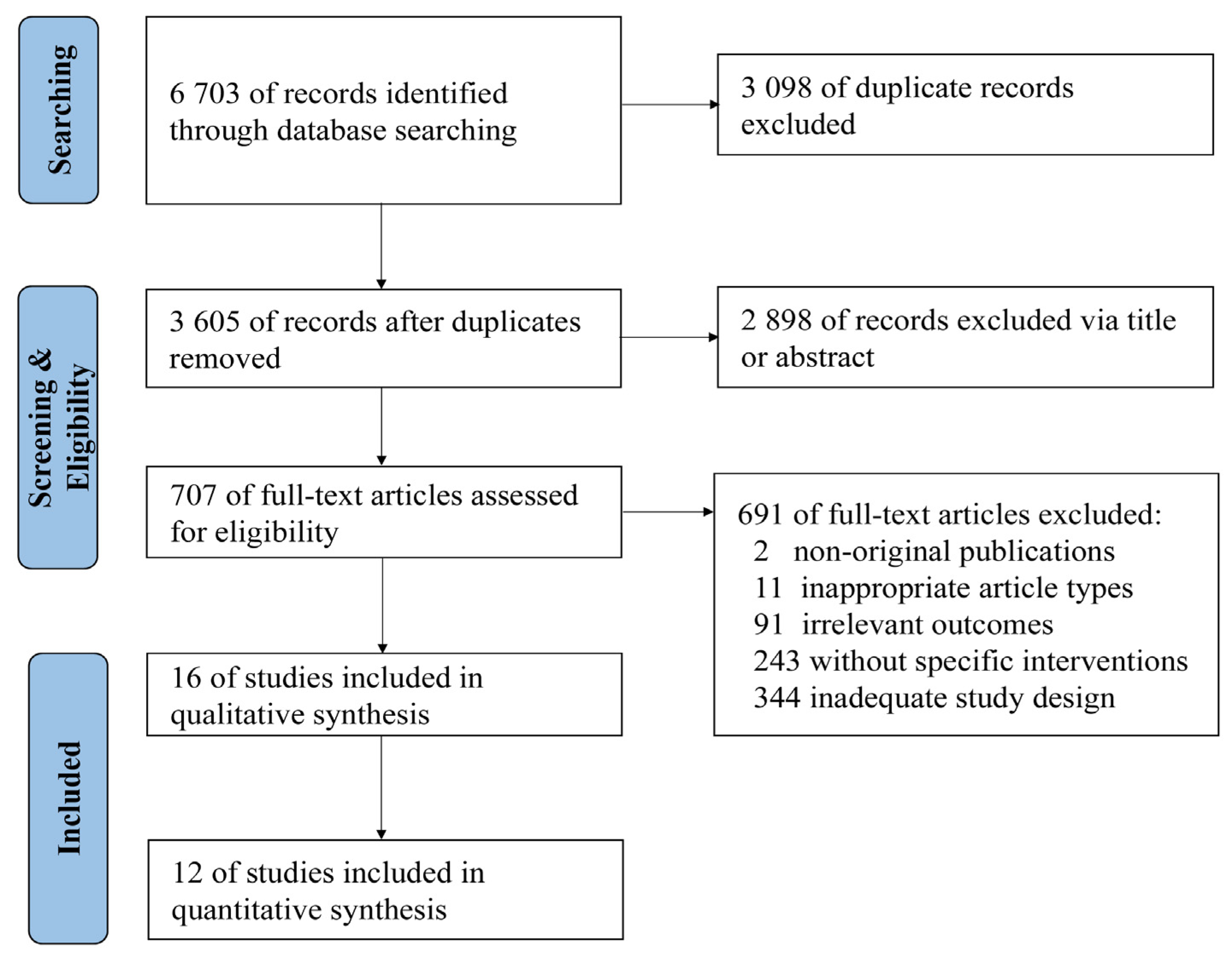
3.1. Study Selection
3.2. Study Characteristic
3.2.1. Population
3.2.2. Intervention
3.2.3. Outcomes of Interest
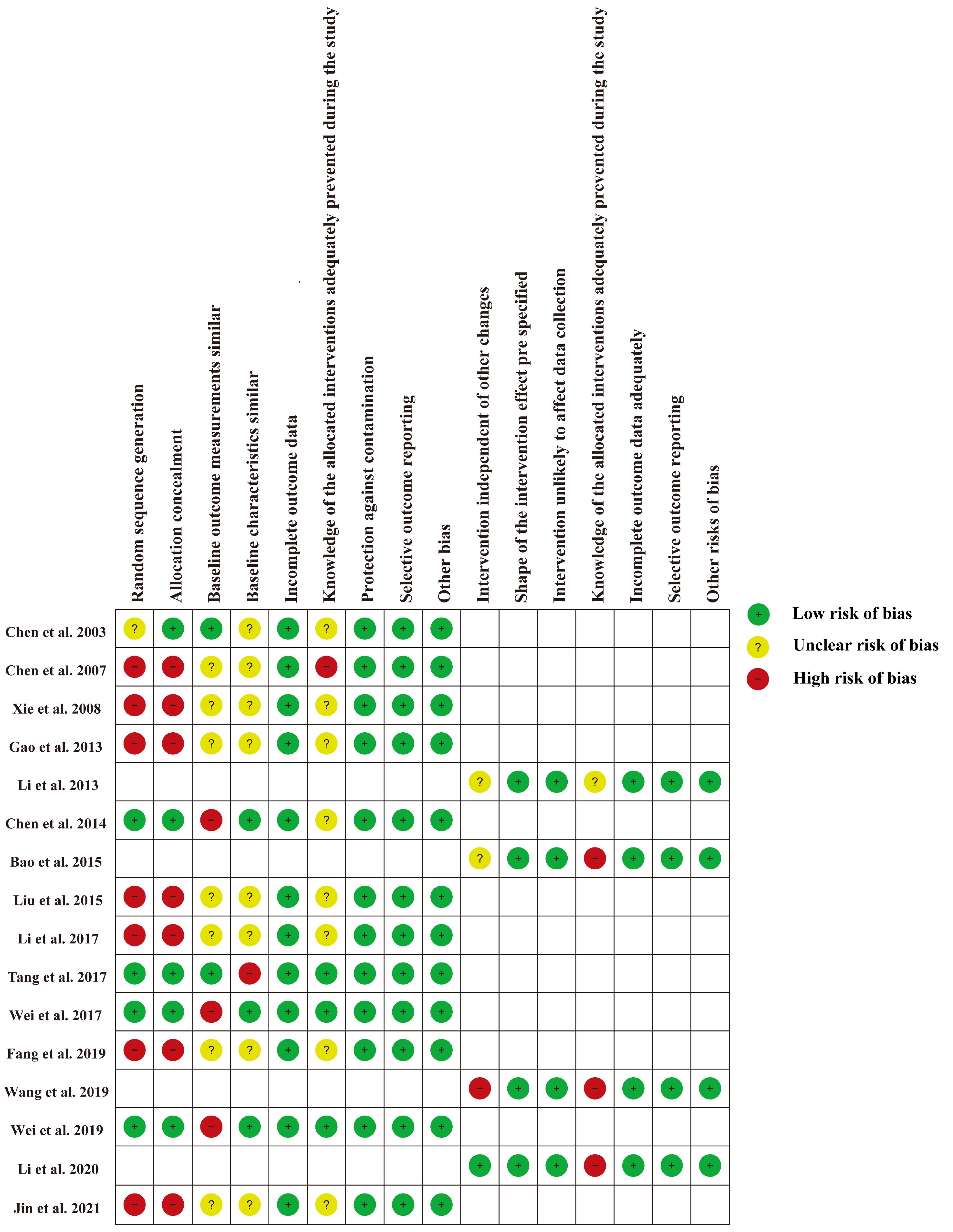
3.3. Risk of Bias Assessment
3.4. Effects of the Interventions
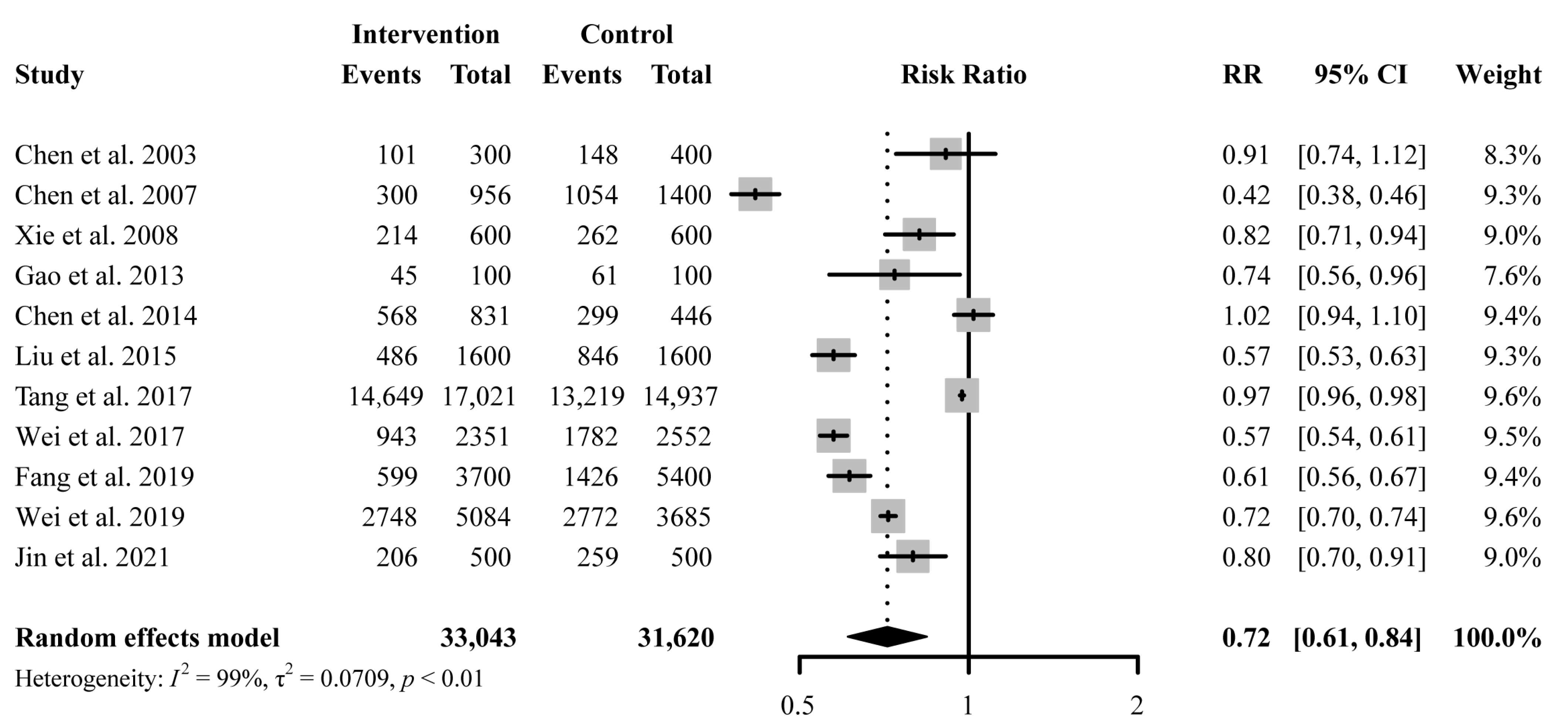
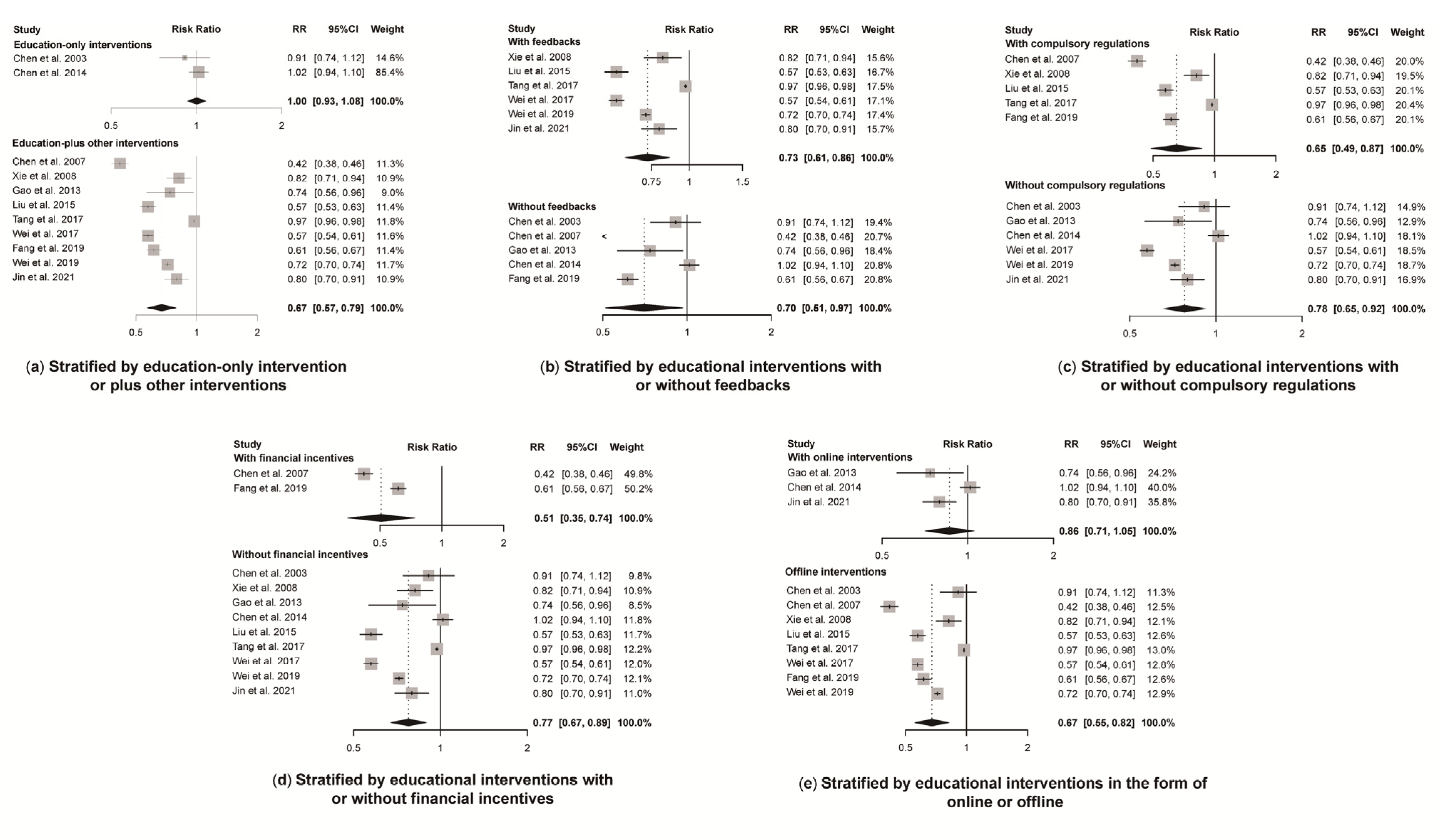
3.4.1. Antibiotic Prescription Rate
3.4.2. Parenteral Use of Antibiotics
3.4.3. Multiple Antibiotic Rates
3.4.4. Antibiotic Prescription Inappropriateness Rate
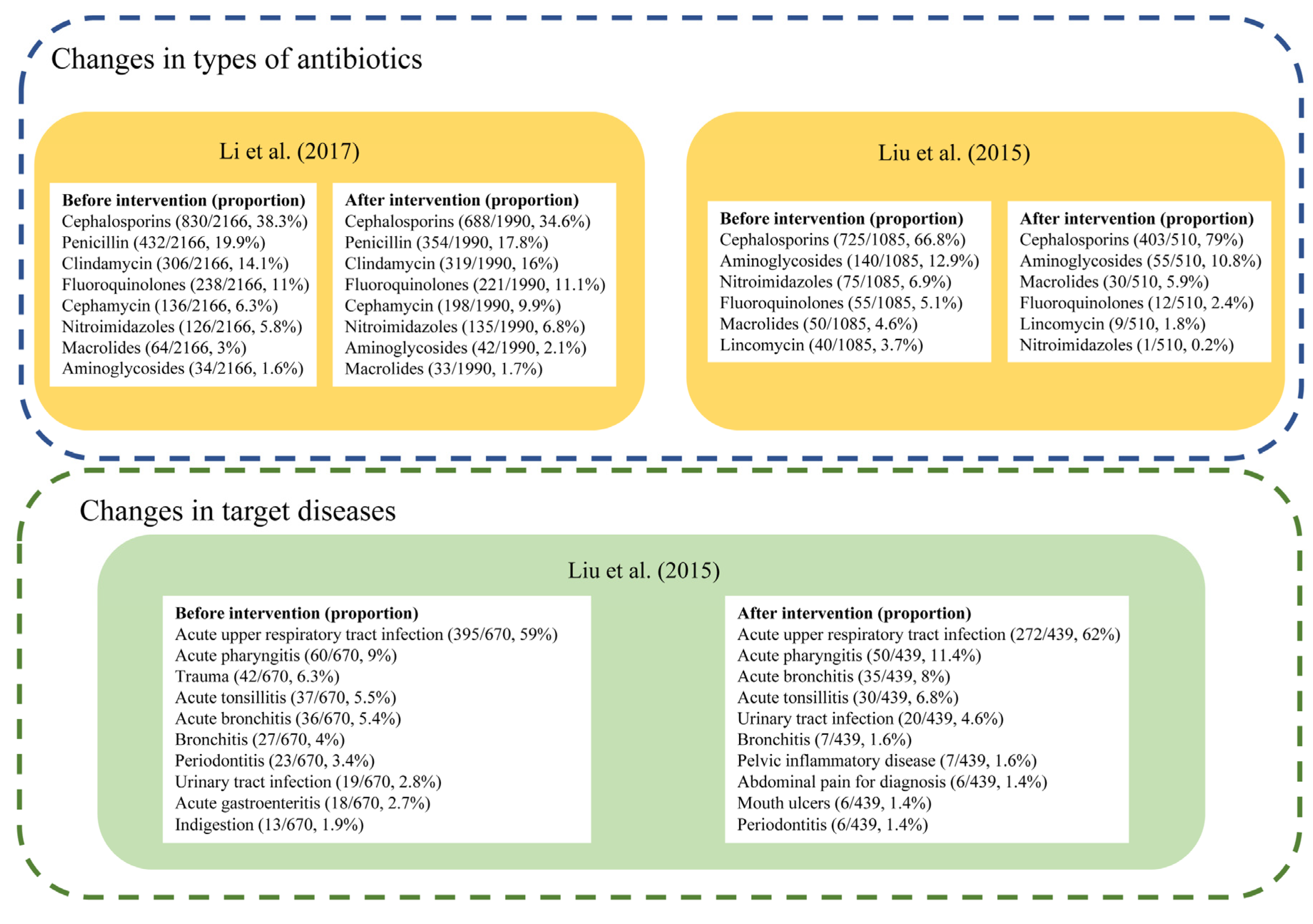
3.4.5. Changes in Types of Antibiotics or Target Diseases
3.4.6. Knowledge Improvement
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Future Health and Wealth of Nations. Available online: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf (accessed on 14 October 2021).
- World Bank. By 2050, Drug-Resistant Infections Could Cause Global Economic Damage on Par with 2008 Financial Crisis. Available online: https://www.worldbank.org/en/news/press-release/2016/09/18/by-2050-drug-resistant-infections-could-cause-global-economic-damage-on-par-with-2008-financial-crisis (accessed on 3 March 2022).
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Zhang, Q.Q.; Ying, G.G.; Pan, C.G.; Liu, Y.S.; Zhao, J.L. Comprehensive evaluation of antibiotics emission and fate in the river basins of China: Source analysis, multimedia modeling, and linkage to bacterial resistance. Environ. Sci. Technol. 2015, 49, 6772–6782. [Google Scholar] [CrossRef] [PubMed]
- He, P.; Sun, Q.; Shi, L.; Meng, Q. Rational use of antibiotics in the context of China’s health system reform. BMJ 2019, 365, l4016. [Google Scholar] [CrossRef] [Green Version]
- The National Action Plan to Contain Antibacterial Resistance (2016–2020). Available online: http://www.gov.cn/xinwen/2016-08/25/content_5102348.htm (accessed on 14 October 2021).
- Teixeira Rodrigues, A.; Roque, F.; Falcão, A.; Figueiras, A.; Herdeiro, M.T. Understanding physician antibiotic prescribing behaviour: A systematic review of qualitative studies. Int. J. Antimicrob. Agents 2013, 41, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Messina, G.; Nante, N. Bacterial lysates (OM-85 BV): A cost-effective proposal in order to contrast antibiotic resistance. J. Prev. Med. Hyg. 2021, 62, E564–E573. [Google Scholar] [CrossRef]
- Duffy, E.; Ritchie, S.; Metcalfe, S.; Van Bakel, B.; Thomas, M.G. Antibacterials dispensed in the community comprise 85%–95% of total human antibacterial consumption. J. Clin. Pharm. Ther. 2018, 43, 59–64. [Google Scholar] [CrossRef]
- Hicks, L.A.; King, L.M.; Fleming-Dutra, K.E. Improving outpatient antibiotic prescribing. BMJ 2019, 364, l289. [Google Scholar] [CrossRef]
- Zhao, H.; Wei, L.; Li, H.; Zhang, M.; Cao, B.; Bian, J.; Zhan, S. Appropriateness of antibiotic prescriptions in ambulatory care in China: A nationwide descriptive database study. Lancet Infect. Dis. 2021, 21, 847–857. [Google Scholar] [CrossRef]
- Yao, L.; Yin, J.; Huo, R.; Yang, D.; Shen, L.; Wen, S.; Sun, Q. The effects of the primary health care providers’ prescription behavior interventions to improve the rational use of antibiotics: A systematic review. Glob. Health Res. Policy 2020, 5, 45. [Google Scholar] [CrossRef]
- Finch, R.G.; Metlay, J.P.; Davey, P.G.; Baker, L.J. Educational interventions to improve antibiotic use in the community: Report from the international forum on antibiotic resistance (IFAR) colloquium, 2002. Lancet Infect. Dis. 2004, 4, 44–53. [Google Scholar] [CrossRef]
- Roque, F.; Herdeiro, M.T.; Soares, S.; Teixeira Rodrigues, A.; Breitenfeld, L.; Figueiras, A. Educational interventions to improve prescription and dispensing of antibiotics: A systematic review. BMC Public Health 2014, 14, 1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyaw, B.M.; Tudor Car, L.; van Galen, L.S.; van Agtmael, M.A.; Costelloe, C.E.; Ajuebor, O.; Campbell, J.; Car, J. Health professions digital education on antibiotic management: Systematic review and meta-analysis by the digital health education collaboration. J. Med. Internet Res. 2019, 21, e14984. [Google Scholar] [CrossRef]
- Srinivasan, A.; Song, X.; Richards, A.; Sinkowitz-Cochran, R.; Cardo, D.; Rand, C. A survey of knowledge, attitudes, and beliefs of house staff physicians from various specialties concerning antimicrobial use and resistance. Arch. Intern. Med. 2004, 164, 1451–1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers Van Katwyk, S.; Jones, S.L.; Hoffman, S.J. Mapping educational opportunities for healthcare workers on antimicrobial resistance and stewardship around the world. Hum. Resour. Health 2018, 16, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochrane Effective Practice and Organisation of Care (EPOC). What Study Designs Can Be Considered for Inclusion in an EPOC Review and What Should They be Called? Available online: https://zenodo.org/record/5106085#.YqMCYexBxPZ (accessed on 2 September 2021).
- Cochrane Effective Practice and Organisation of Care (EPOC). Suggested Risk of Bias Criteria for EPOC Reviews. Available online: https://epoc.cochrane.org/sites/epoc.cochrane.org/files/public/uploads/Resources-for-authors2017/suggested_risk_of_bias_criteria_for_epoc_reviews.pdf (accessed on 2 September 2021).
- Mas-Morey, P.; Valle, M. A systematic review of inpatient antimicrobial stewardship programmes involving clinical pharmacists in small-to-medium-sized hospitals. Eur. J. Hosp. Pharm. 2018, 25, e69–e73. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, L.; Peng, R.; Wang, Y.; Ma, R.; Ren, X.; Meng, W.; Sun, F.; Fang, J.; Chen, P.; Wang, Y.; et al. Significant reduction of antibiotic consumption and patients’ costs after an action plan in China, 2010–2014. PLoS ONE 2015, 10, e0118868. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, K.; Jing, T.; Tian, J.; Shen, X.; Xie, C.; Ma, B.; Liu, Y.; Yao, L.; Cao, X. Use of text messages to communicate clinical recommendations to health workers in rural China: A cluster-randomized trial. Bull. World Health Organ. 2014, 92, 474–481. [Google Scholar] [CrossRef]
- Gao, S.; Xiao-Ming, M.A.; Liu, J. Investigation and Analysis of the Implementation of National Essential Drug System in Division 4 of XPCC before and after Intervention. China Pharm. 2013, 24, 305–307. [Google Scholar]
- Li, H.; Gong, Y.; Han, J.; Zhang, S.; Chen, S.; Xu, X.; Lu, Z.; Yin, X. Interrupted time-series analysis to evaluate the impact of a national antimicrobial stewardship campaign on antibiotic prescribing: A typical practice in China’s primary care. Clin. Infect. Dis. 2021, 73, e4463–e4471. [Google Scholar] [CrossRef]
- Liu, S.L.; Liao, W.H.; Huan-Jiao, O.U.; Zheng, Z.M. Investigation on the rational use of antibacterial drugs before and after intervention of rural community health service stations affiliated to our hospital. China Pharm. 2015, 5072–5075. [Google Scholar]
- Tang, Y.; Liu, C.; Zhang, X. Performance associated effect variations of public reporting in promoting antibiotic prescribing practice: A cluster randomized-controlled trial in primary healthcare settings. Prim. Health Care Res. Dev. 2017, 18, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, H.; Yu, X.; Zhou, H.; Li, B.; Chen, G.; Ye, Z.; Wang, Y.; Cui, X.; Zheng, Y.; et al. Impact of antimicrobial stewardship managed by clinical pharmacists on antibiotic use and drug resistance in a Chinese hospital, 2010–2016: A retrospective observational study. BMJ Open 2019, 9, e026072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, X.; Zhang, Z.; Hicks, J.P.; Walley, J.D.; King, R.; Newell, J.N.; Yin, J.; Zeng, J.; Guo, Y.; Lin, M.; et al. Long-term outcomes of an educational intervention to reduce antibiotic prescribing for childhood upper respiratory tract infections in rural China: Follow-up of a cluster-randomised controlled trial. PLoS Med. Public Libr. Sci. 2019, 16, e1002733. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.; Zhang, Z.; Walley, J.D.; Hicks, J.P.; Zeng, J.; Deng, S.; Zhou, Y.; Yin, J.; Newell, J.N.; Sun, Q.; et al. Effect of a training and educational intervention for physicians and caregivers on antibiotic prescribing for upper respiratory tract infections in children at primary care facilities in rural China: A cluster-randomised controlled trial. Lancet. Glob. Health 2017, 5, e1258–e1267. [Google Scholar] [CrossRef] [Green Version]
- Xie, S. Multicenter intervention study on international RDU indices in Shenzhen’s hospitals. China Pharm. 2008, 11, 1429–1431. [Google Scholar]
- Zhen, L.I.; Bo, Q.U.; Mei-Xia, H.U.; Guo, C.Z.; Chen, L.; Jin, C.G. The impact of a peer review and feedback intervention on antibiotic prescribing: Interrupted time series analysis at village clinics in Qingdao, Shangdong Province. Chin. J. Health Policy 2013, 6, 54–59. [Google Scholar]
- Chen, L.; Wang, S.; Wang, Q.; Shi, L.; Wang, H.; Li, H.; Xu, Y.; Gao, Y.; Wu, M.; Wu, L.; et al. Multicentre controlled study of international indicators of rational drug use—A field survey. Chin. J. Hosp. Pharm. 2003, 23, 438–440. [Google Scholar] [CrossRef]
- Chen, W.; Lu, Q.; Guan, X.; CHen, J.; Chen, D.; Li, Y.; Hong, Y.; Zhao, Y.; Li, W.; Li, M.; et al. Using intervention countermeasures to reduce the overuse of antimicrobials and injectables in six hospitals in Zhuhai. Chin. J. Pharmacoepidemiol. 2007, 16, 353–355. [Google Scholar] [CrossRef]
- Fang, S.; Chen, X.; Wang, N.; Tang, H. Research on the management and policy of rational use of antibacterial drugs in primary care institutions. Anti-Infect. Pharm. 2019, 16, 283–285. [Google Scholar] [CrossRef]
- Jin, Z.; Chen, H.; Zhang, Y.; Wang, Q. Effectiveness of medical consortium model in outpatient antimicrobial drug management in primary health centers. Drug Eval. 2021, 18, 582–584. [Google Scholar] [CrossRef]
- Li, X.; Zhang, Q.; Xiong, W. Rationality analysis of antibioticss prescription in 17 primary health institutions and emergency department in jiande district: Before and after intervention. Eval. Anal. Drug-Use Hosp. China 2017, 17, 534–536. [Google Scholar] [CrossRef]
- Dempsey, P.P.; Businger, A.C.; Whaley, L.E.; Gagne, J.J.; Linder, J.A. Primary care clinicians’ perceptions about antibiotic prescribing for acute bronchitis: A qualitative study. BMC Fam. Pract. 2014, 15, 194. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, G.V.; Roberts, R.M.; Albert, A.P.; Johnson, D.D.; Hicks, L.A. Effects of knowledge, attitudes, and practices of primary care providers on antibiotic selection, United States. Emerg. Infect. Dis. 2014, 20, 2041–2047. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Walley, J.; Chou, R.; Tucker, J.D.; Harwell, J.I.; Wu, X.; Yin, J.; Zou, G.; Wei, X. Interventions to reduce childhood antibiotic prescribing for upper respiratory infections: Systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 1162–1170. [Google Scholar] [CrossRef] [Green Version]
- Cullen, M.W.; Geske, J.B.; Anavekar, N.S.; McAdams, J.A.; Beliveau, M.E.; Ommen, S.R.; Nishimura, R.A. Reinvigorating continuing medical education: Meeting the challenges of the digital age. Mayo Clin. Proc. 2019, 94, 2501–2509. [Google Scholar] [CrossRef] [Green Version]
- van der Velden, A.W.; Pijpers, E.J.; Kuyvenhoven, M.M.; Tonkin-Crine, S.K.; Little, P.; Verheij, T.J. Effectiveness of physician-targeted interventions to improve antibiotic use for respiratory tract infections. Br. J. Gen. Pract. 2012, 62, e801–e807. [Google Scholar] [CrossRef] [Green Version]
- Arnold, S.R.; Straus, S.E. Interventions to improve antibiotic prescribing practices in ambulatory care. Cochrane Database Syst. Rev. 2005, 2005, CD003539. [Google Scholar] [CrossRef]
- Sanchez, G.V.; Fleming-Dutra, K.E.; Roberts, R.M.; Hicks, L.A. Core elements of outpatient antibiotic stewardship. MMWR Recomm. Rep. 2016, 65, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Meeker, D.; Linder, J.A.; Fox, C.R.; Friedberg, M.W.; Persell, S.D.; Goldstein, N.J.; Knight, T.K.; Hay, J.W.; Doctor, J.N. Effect of behavioral interventions on inappropriate antibiotic prescribing among primary care practices: A randomized clinical trial. JAMA 2016, 315, 562–570. [Google Scholar] [CrossRef]
- Linder, J.A.; Meeker, D.; Fox, C.R.; Friedberg, M.W.; Persell, S.D.; Goldstein, N.J.; Doctor, J.N. Effects of behavioral interventions on inappropriate antibiotic prescribing in primary care 12 months after stopping interventions. JAMA 2017, 318, 1391–1392. [Google Scholar] [CrossRef] [PubMed]
- Hallsworth, M.; Chadborn, T.; Sallis, A.; Sanders, M.; Berry, D.; Greaves, F.; Clements, L.; Davies, S.C. Provision of social norm feedback to high prescribers of antibiotics in general practice: A pragmatic national randomised controlled trial. Lancet 2016, 387, 1743–1752. [Google Scholar] [CrossRef] [Green Version]
- Rogers Van Katwyk, S.; Grimshaw, J.M.; Nkangu, M.; Nagi, R.; Mendelson, M.; Taljaard, M.; Hoffman, S.J. Government policy interventions to reduce human antimicrobial use: A systematic review and evidence map. PLoS Med. 2019, 16, e1002819. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Study Design | Participants | Setting and District | Intervention Details | Target Illness | Duration of Intervention and Data Collection | Key Outcomes |
|---|---|---|---|---|---|---|---|
| Chen et al., 2003 [33] | Cluster-RCT | Clinicians and pharmacists in 7 hospitals | 7 hospitals in Peking (tertiary 1 vs. 1; secondary 1 vs. 1; primary 1 vs. 2) | Lectures on rational drug use and training on international standards; A brochure on rational drug use | Not specific | Duration: 3 months. Data were collected for 5 months both before baseline and after endline | The antibiotic prescribing rate declined (intervention: from 37.7% to 33.7%; control: 38.5% to 37.0%). |
| Chen et al., 2007 [34] | CBA | Medical staff | Six secondary and tertiary hospitals in Zhuhai, Guangdong | Clinical guidelines, lectures, and knowledge competition on rational antibiotic use; Financial punishment; A Monitoring-Training-Plan Team Working System | URIs | Duration: 1 year. Data were collected for 3 months before three to four rounds of intervention at four-week intervals | The antibiotics prescribing rate declined from 75.3% to 31.4%. |
| Xie et al., 2008 [31] | CBA | Doctors, pharmacists and caregivers | Six secondary and tertiary hospitals in Shenzhen, Guangdong | Seminars on the rational use of medicines; Books and manuals related to rational drug use; Intervention program and expected targets; Feedbacks on antibiotic prescribing | Not specific | Duration: 10 months. Data were collected for 2 months both during 1 month both before baseline and after endline | The rate of antibiotic prescription significantly reduced (from 52.9% to 30.4%). |
| Li et al., 2013 [32] | ITS | Doctors | 123 village health clinics in Qingdao, Shandong | Prescription feedback; Trainings on antibiotic use. | Not specific | Duration: 1 year. Data were collected monthly for 10 months before intervention and 12 months after intervention | A significant 0.88% decline in average antibiotic prescription rates. |
| Gao et al., 2013 [24] | CBA | Doctors, pharmacists and caregivers | 186 township health lefts in Xinjiang Uygur Autonomous Region | Training brochures and television program on antibiotics; Financial penalties | Not specific | Duration: 2 months Data were collected for one month both during 7 months both before baseline and 5 months after endline | The antibiotic prescribing rate declined from 61% to 45% significantly. |
| Chen et al., 2014 [23] | Cluster-RCT | 977 health workers at recruitment | 100 township health lefts in Gansu province (52 vs. 48) | (1) intervention group: text messages about recommendations for the management of the infections three times a week by computers (2) control group: a traditional one-day training program | URIs | Duration: 2 months. Data were collected for 3 months (including half month before endline) and the same period one year before the trial | Antibiotic prescription rate increased (from 50% to 67%) in the control group, unchanged (68%) in the intervention group. The knowledge score increased by 16% in the intervention group, with no significant changes in the control group. |
| Liu et al., 2015 [26] | CBA | Doctors | 8 township health lefts in Xiaolan, Guangdong | Optimize administrative structure; Set specific antibiotic targets; Training to improve antibiotic application capacity; Prescribing feedback | Not specific | Duration: 1 year. Data were collected for 1 year both during 1 year both before baseline and after endline | The rate of antibiotic prescription (from 52.9% to 30.4%) and multiple antibiotics (from 43.5% to 22.8%) reduced. The most used antibiotics were still Cephalosporins with increasing proportion. The proportion of antibiotic prescriptions for acute URI increased (from 46.7% to 56.0%). |
| Bao et al., 2015 [22] | ITS | Medical workers | 30 tertiary hospitals and 35 secondary hospitals nationwide | A national education programs for doctors and managerial personnel; Enforcement of mandatory administrative regulations | Not specific | Duration: 1 year. Data were collected monthly in three defined segments: Segment 1: the preparation period (July 2010 to June 2011); Segment 2: the policy intervention period (July 2011 to June 2012); and Segment 3: the assessment period (July 2012 to June 2014) | Antibiotic prescription rate significantly decreased (26.4% vs. 12.9%, 1.07% decline monthly) during the intervention period. |
| Tang et al., 2017 [27] | Cluster-RCT | 60 doctors | Qianjiang city of Hubei province, involving 20 primary care organizations | Dissemination posters and brochures with a brief introduction on health risks of excessive use of antibiotics; Feedbacks on antibiotic prescription; Display ranking information | Duration: 1 year. Data were collected for 6 months from 4 months after baseline and for 1 year before baseline | Antibiotics prescribing rate declined (intervention: from 90.7% to 86.1%; control: from 90.6% to 88.0%). No effect on reducing the overall prescribing rate of injection antibiotics (p > 0.05). | |
| Wei et al., 2017 [30] | Cluster-RCT | Doctors | 25 township hospitals within the rural, low-income province of Guangxi in western China | Clinical guidelines based on the latest Chinese and international antibiotic-use guidelines; 2-h interactive training session; Monthly peer-review meetings with feedbacks; Leaflets and a video about antibiotics | URIs for children aged 2–14 | Duration: 6 months. Data were collected during the 3 months prior to the baseline, and during the final 3 months of endline | The antibiotics prescribing rate declined (intervention: from 82% to 40%; control: from 75% to 70%; p < 0.01). No difference of multiple and injection antibiotic prescription rates between the two groups was observed at endline (p > 0.05). |
| Li et al., 2017 [37] | CBA | Health workers | 17 primary health lefts in Jiande, Zhejiang | Training in rational drug use; Inclusion of antibiotic use in assessment indicators; Feedback and audit of junior centre doctors’ prescriptions; | Not specific | Duration: 3 months. Data were collected for one month both during 1 month both before baseline and after endline | The rates of inappropriate antibiotic prescription (from 28.7% to 20.8%), multiple antibiotics (from 26.7% to 16.8%), and antibiotic injection (from 60.7% to 47.3%) reduced significantly. No major change in the types of antibiotics used, and cephalosporins were the most used. |
| Wang et al., 2019 [28] | ITS | Medical staff | Beijing Chaoyang Hospital in Peking | Clinical pharmacists trained the medical staff on rational use of antibiotics both online and offline; Program and regulations on antibiotic use; Automatic prescription screening system; Financial reward and punishment; Prescription audit and feedback | Not specific | Duration: 36 months. Data were collected monthly in three defined stages: Stage 1: baseline phase (July 2010 to June 2011); stage 2: intervention phase (July 2011 to December 2013); and stage 3: stability phase (January 2014 to December 2016) | The average antibiotic prescription rates declined 0.33% during the intervention period. |
| Wei et al., 2019 [29] | Cluster-RCT | Doctors | 25 township hospitals within the rural, low-income province of Guangxi | Clinical guidelines based on the latest Chinese and international antibiotic-use guidelines; 2-h interactive training session; Monthly peer-review meetings with feedbacks; Leaflets and a video about antibiotics | URIs for children aged 2–14 | Duration: 6 months. Data were collected for 3 months prior to baseline, the final 3 months of endline, and at 18-month follow-up (during the final 3 months of the 18-month period since the intervention was first implemented) | the antibiotics prescribing rate declined (intervention: from 84% to 54%; control: from 76% to 75%; adjusted risk difference 36%, p < 0.01). No difference of injection antibiotic prescription rate Reported better knowledge and confidence in qualitative study. |
| Fang et al., 2019 [35] | CBA | Health workers | all township (town or village) health lefts in Zhenjiang, Jiangsu | Training for medical personnel by experts (14 sessions were organized, with more than 1400 people trained); helped formulate the program of stewardship | Not specific | Duration: 1 year. Data were collected for one month both during 1 month both before baseline and after endline | The rates of total antibiotic prescription (from 26.4% to 16.9%), inappropriate antibiotic prescription (from 34.1% to 17.4%) and antibiotic injection rate (from 15.2% to 41.1%) significantly declined. |
| Li et al., 2020 [25] | ITS | Doctors | 11 CHCs in Shenzhen, Guangdong | Educational programs for clinicians every 6 months containing a test; A system of reward and punishment; Antibiotic prescribing management and audit | Not specific | Duration: 2 years. Data were collected monthly: 24 months before the intervention (January 2010–December 2011) and 48 months after the intervention (January 2012–December 2015) | A 3.1% decline in average antibiotic prescription rate during the intervention period with a cumulative effect of 74.0% decline by the end of the study. |
| Jin et al., 2021 [36] | CBA | Doctors and pharmacists | 5 township health lefts in Yichun, Sichuan | Higher-level hospitals form medical associations and regularly visit township health lefts to give lectures; Feedback on prescriptions through WeChat and telephone | Not specific | Duration: 1 year. Data were collected during 1 year before and 1 year after implementation of intervention | The rates of antibiotic prescription (from 51.8% to 41.2%, p < 0.05), inappropriate antibiotic prescription (75.3% to 52.4%, p < 0.05), multiple antibiotics (12.3% to 12.1%, p > 0.05), and antibiotic injection reduced (60.0% to 47.1%, p < 0.05). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, K.; Xie, Y.; Dan, L.; Mao, M.; Chen, J.; Li, R.; Wang, X.; Hesketh, T. Effectiveness of Educational Interventions for Health Workers on Antibiotic Prescribing in Outpatient Settings in China: A Systematic Review and Meta-Analysis. Antibiotics 2022, 11, 791. https://doi.org/10.3390/antibiotics11060791
Zheng K, Xie Y, Dan L, Mao M, Chen J, Li R, Wang X, Hesketh T. Effectiveness of Educational Interventions for Health Workers on Antibiotic Prescribing in Outpatient Settings in China: A Systematic Review and Meta-Analysis. Antibiotics. 2022; 11(6):791. https://doi.org/10.3390/antibiotics11060791
Chicago/Turabian StyleZheng, Kunhua, Ying Xie, Lintao Dan, Meixian Mao, Jie Chen, Ran Li, Xuanding Wang, and Therese Hesketh. 2022. "Effectiveness of Educational Interventions for Health Workers on Antibiotic Prescribing in Outpatient Settings in China: A Systematic Review and Meta-Analysis" Antibiotics 11, no. 6: 791. https://doi.org/10.3390/antibiotics11060791