
The Dynamics of Antimicrobial Resistance among Enterobacteriaceae Isolates in Russia: Results of the 2012–2018 INFORM and ATLAS International Program Studies

Abstract
:1. Introduction
2. Results
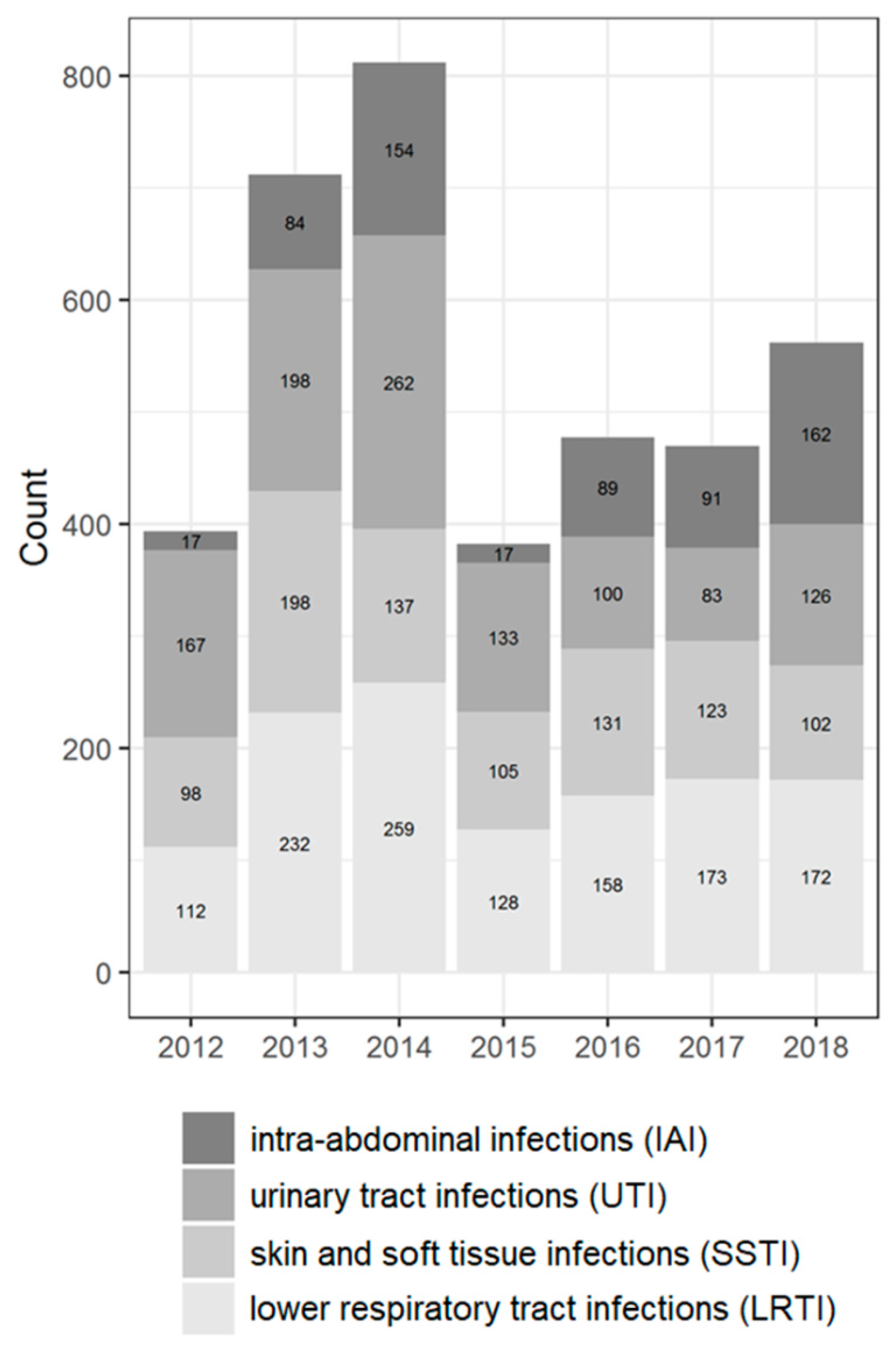
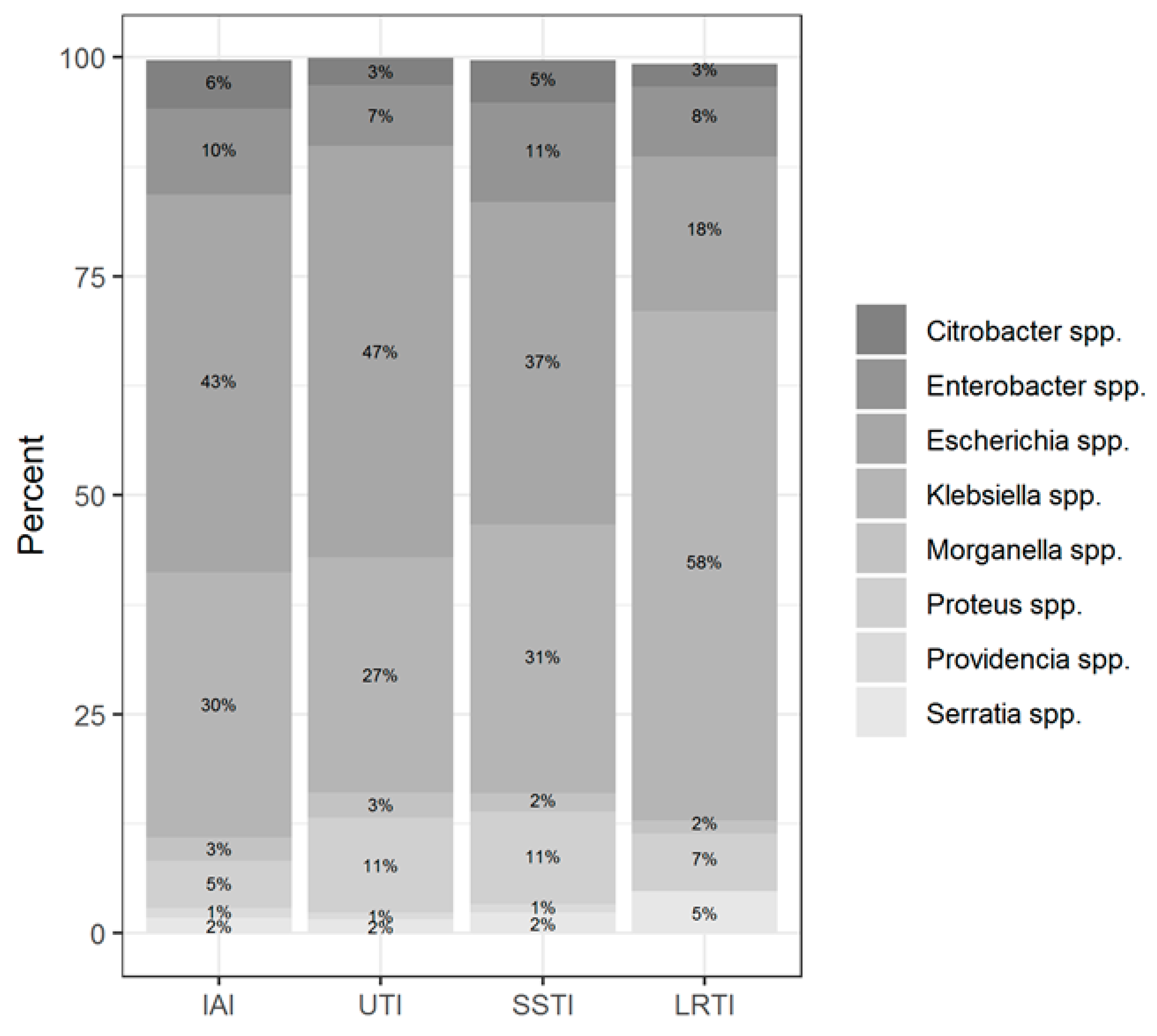
2.1. Distribution of Isolates
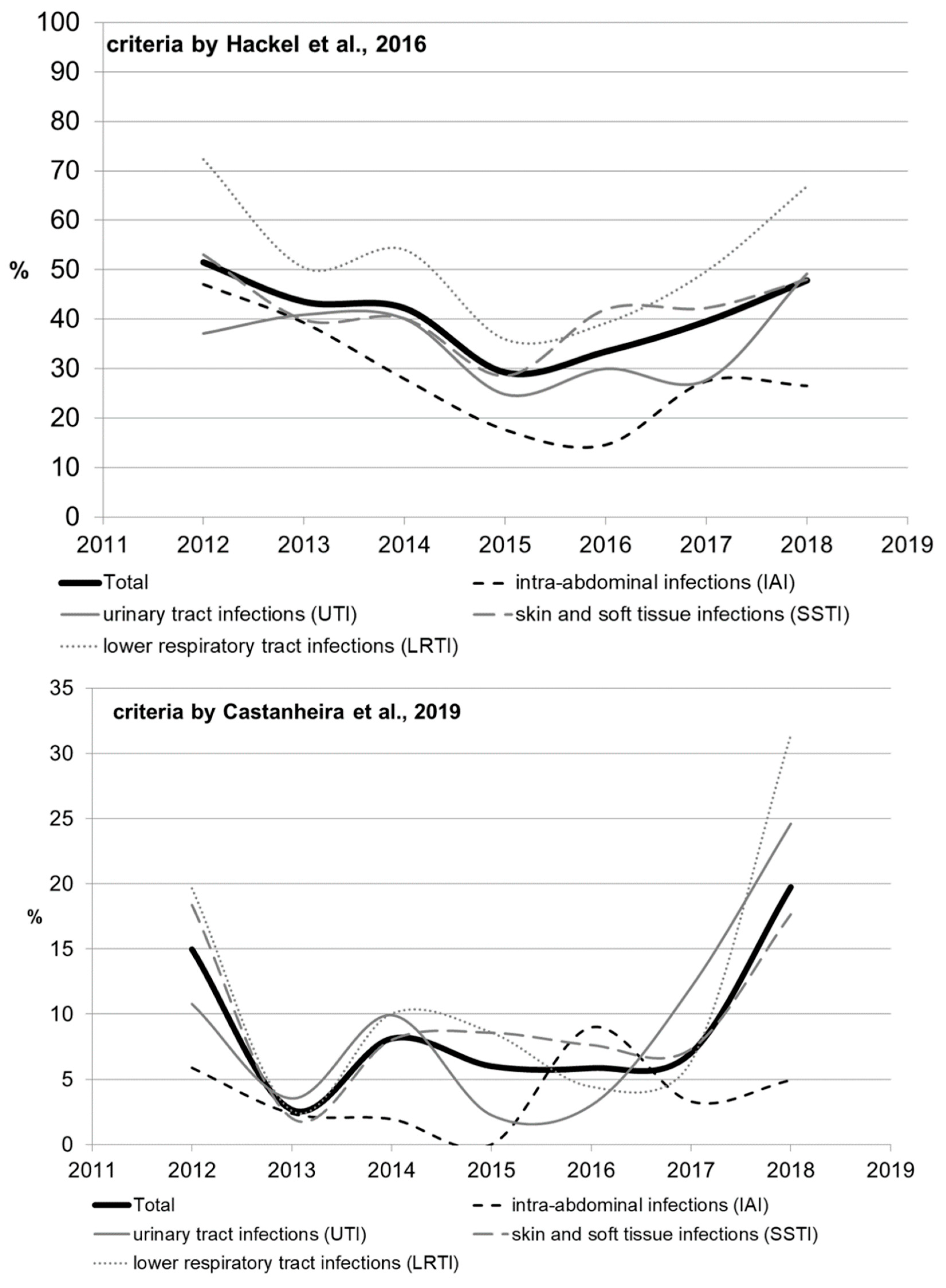
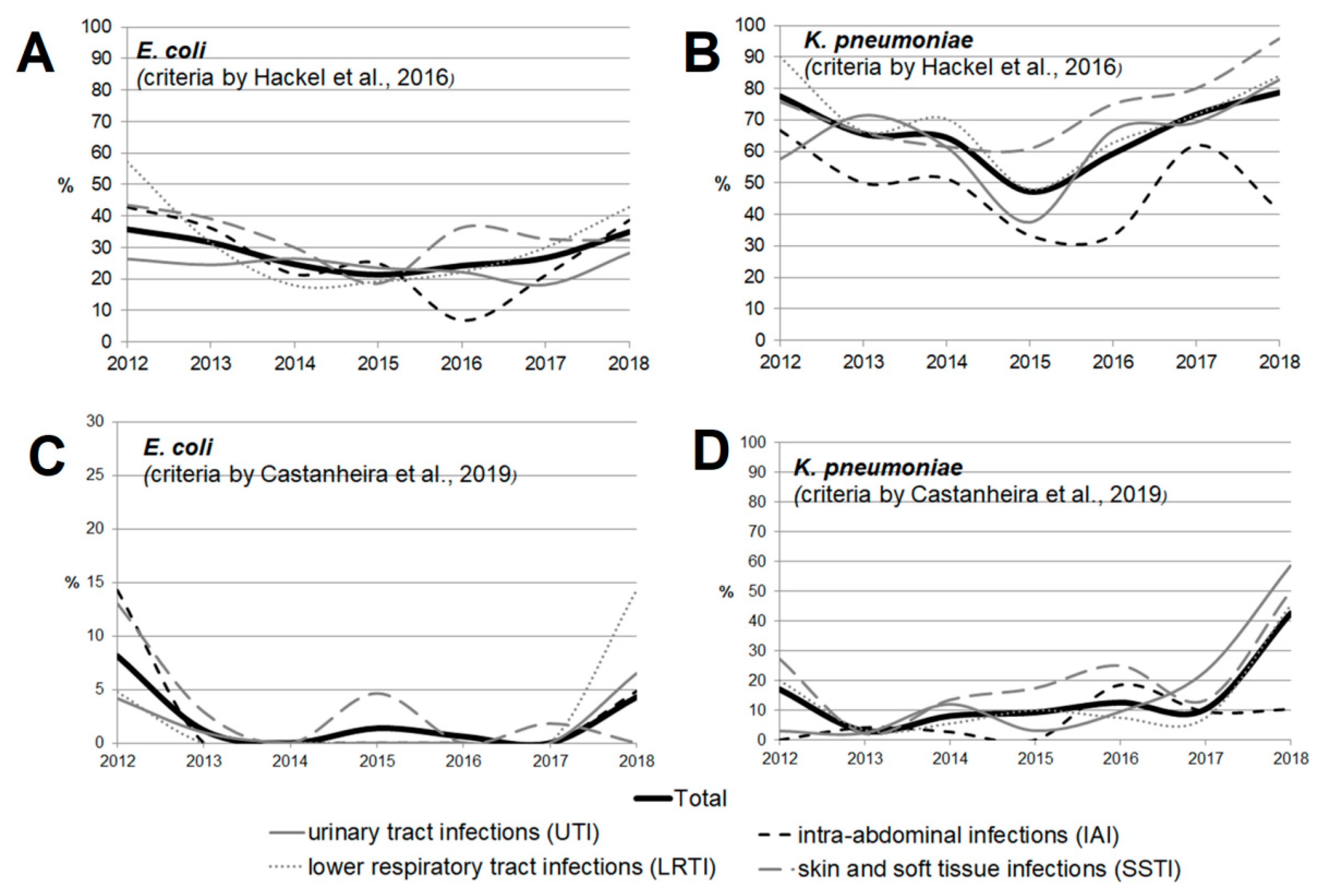
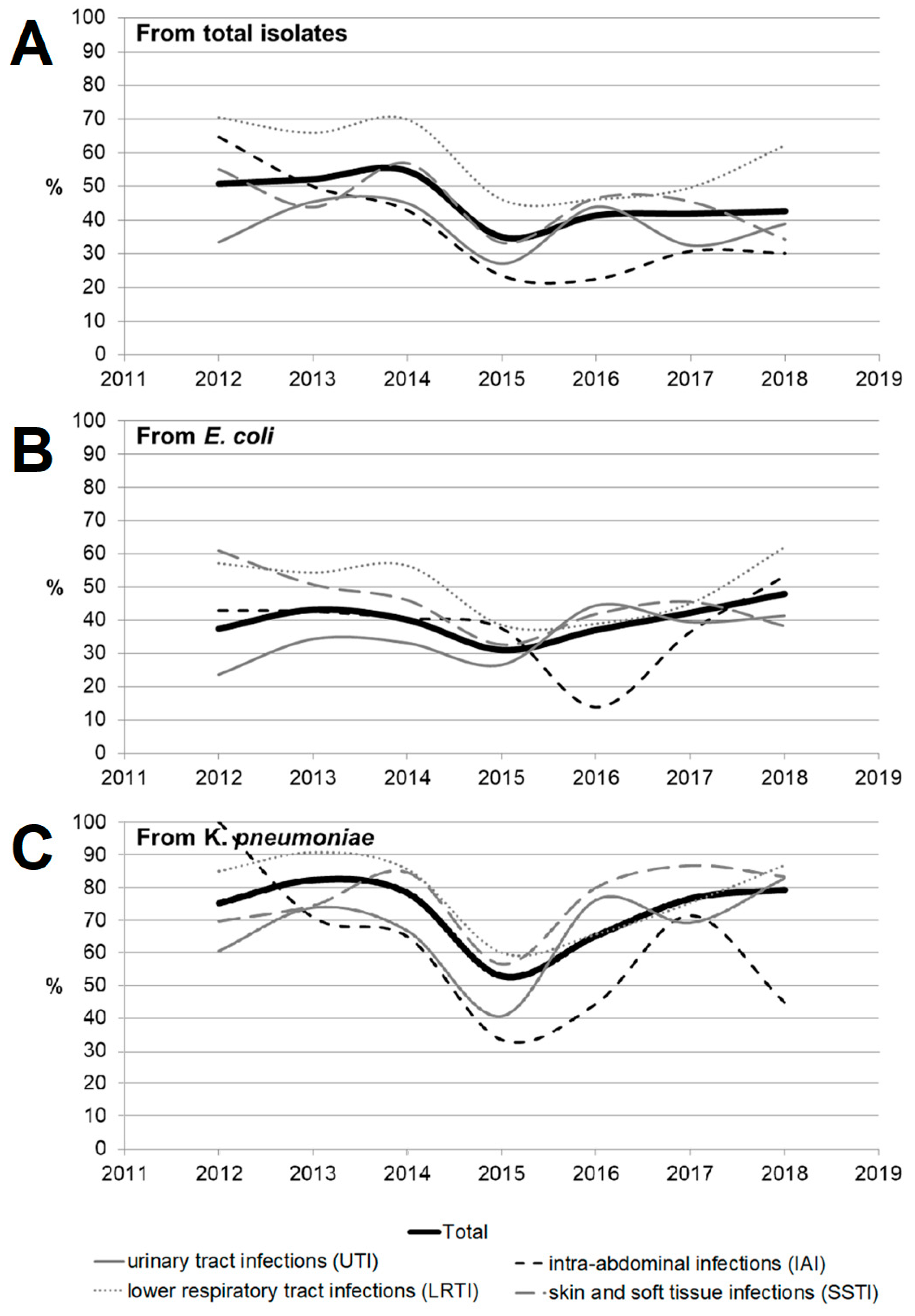
2.2. Antimicrobial Susceptibility and Resistance
2.3. Multidrug Resistance of Isolates
2.4. ESBL Characterization of the Isolates
3. Discussion
4. Methods
4.1. Study Design
4.2. Antimicrobial Susceptibility Testing
4.3. Characterization of Phenotype Features
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Livorsi, D.J.; Chorazy, M.L.; Schweizer, M.L.; Balkenende, E.C.; Blevins, A.E.; Nair, R.; Samore, M.H.; Nelson, R.E.; Khader, K.; Perencevich, E.N. A systematic review of the epidemiology of carbapenem-resistant Enterobacteriaceae in the United States. Antimicrob. Resist. Infect. Control 2018, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Giani, T.; Antonelli, A.; Caltagirone, M.; Mauri, C.; Nicchi, J.; Arena, F.; Nucleo, E.; Bracco, S.; Pantosti, A.; Vismara, C.; et al. Evolving beta-lactamase epidemiology in Enterobacteriaceae from Italian nationwide surveillance, October 2013: KPC-carbapenemase spreading among outpatients. Eurosurveillance 2017, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Spiliopoulou, I.; Kazmierczak, K.; Stone, G.G. In vitro activity of ceftazidime/avibactam against isolates of carbapenem-non-susceptible Enterobacteriaceae collected during the INFORM global surveillance programme (2015–2017). J. Antimicrob. Chemother. 2020, 75, 384–391. [Google Scholar] [CrossRef] [Green Version]
- Xu, A.; Zheng, B.; Xu, Y.C.; Huang, Z.G.; Zhong, N.S.; Zhuo, C. National epidemiology of carbapenem-resistant and extensively drug-resistant Gram-negative bacteria isolated from blood samples in China in 2013. Clin. Microbiol. Infect. 2016, 22, S1–S8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrado, G.; Canichella, A.; Serrao, M. Epidemiology of Carbapenem Resistant Klebsiella pneumoniae Infections in Mediterranean Countries. J. Hematol. Infect. Dis. 2016, 8, e2016032. [Google Scholar]
- Hawkey, P.M.; Warren, R.E.; Livermore, D.M.; McNulty, C.A.M.; Enoch, D.A.; Otter, J.A.; Wilson, A.P.R. Treatment of infections caused by multidrug-resistant gram-negative bacteria: Report of the British society for antimicrobial chemotherapy/healthcare infection society/british infection association joint working party. J. Antimicrob. Chemother. 2018, 73, iii2–iii78. [Google Scholar] [CrossRef] [Green Version]
- Logan, L.K.; Weinstein, R.A. The epidemiology of Carbapenem-resistant enterobacteriaceae: The impact and evolution of a global menace. J. Infect. Dis. 2017, 215 (Suppl. 1), S28–S36. [Google Scholar] [CrossRef] [Green Version]
- Giammanco, A.; Calà, C.; Fasciana, T.; Dowzicky, M.J. Global Assessment of the Activity of Tigecycline against Multidrug-Resistant Gram-Negative Pathogens between 2004 and 2014 as Part of the Tigecycline Evaluation and Surveillance Trial. mSphere 2017, 2, e00310-16. [Google Scholar] [CrossRef] [Green Version]
- Musicha, P.; Cornick, J.E.; Bar-Zeev, N.; French, N.; Masesa, C.; Denis, B.; Kennedy, N.; Mallewa, J.; Gordon, M.A.; Msefula, C.L.; et al. Trends in antimicrobial resistance in bloodstream infection isolates at a large urban hospital in Malawi (1998–2016): A surveillance study. Lancet Infect. Dis. 2017, 17, 1042–1052. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Zhao, S.Y.; Xiao, S.Z.; Gu, F.F.; Liu, Q.Z.; Tang, J.; Guo, X.K.; Ni, Y.X.; Han, L.Z. Antimicrobial resistance and molecular epidemiology of Escherichia coli causing bloodstream infections in three hospitals in Shanghai, China. PLoS ONE 2016, 11, e0147740. [Google Scholar] [CrossRef]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. World health organization releases global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. JMS J. Med. Soc. 2018, 32, 76–77. [Google Scholar] [CrossRef]
- Zhang, Z.; Chen, M.; Yu, Y.; Liu, B.; Liu, Y. In vitro activity of ceftaroline and comparators against staphylococcus aureus isolates: Results from 6 years of the ATLAS program (2012 to 2017). Infect. Drug Resist. 2019, 12, 3349–3358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbán, E.; Stone, G.G. Impact of EUCAST ceftaroline breakpoint change on the susceptibility of methicillin-resistant Staphylococcus aureus isolates collected from patients with complicated skin and soft-tissue infections. Clin. Microbiol. Infect. 2019, 25, 1429.e1–1429.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackel, M.; Kazmierczak, K.M.; Hoban, D.J.; Biedenbach, D.J.; Bouchillon, S.K.; De Jonge, B.L.M.; Stone, G.G. Assessment of the in vitro activity of ceftazidime-avibactam against multidrug-resistant Klebsiella spp. collected in the INFORM Global Surveillance Study, 2012 to 2014. Antimicrob. Agents Chemother. 2016, 60, 4677–4683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castanheira, M.; Deshpande, L.M.; Mendes, R.E.; Canton, R.; Sader, H.S.; Jones, R.N. Variations in the occurrence of resistance phenotypes and carbapenemase genes among enterobacteriaceae isolates in 20 years of the SENTRY antimicrobial surveillance program. Open Forum Infect. Dis. 2019, 6 (Suppl. 1), S23–S33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hovan, M.R.; Narayanan, N.; Cedarbaum, V.; Bhowmick, T.; Kirn, T.J. Comparing mortality in patients with carbapenemase-producing carbapenem resistant Enterobacterales and non-carbapenemase-producing carbapenem resistant Enterobacterales bacteremia. Diagn. Microbiol. Infect. Dis. 2021, 101, 115505. [Google Scholar] [CrossRef]
- Moghnieh, R.; Abdallah, D.; Jadayel, M.; Zorkot, W.; El Masri, H.; Dib, M.J.; Omar, T.; Sinno, L.; Lakkis, R.; Jisr, T. Epidemiology, risk factors, and prediction score of carbapenem resistance among inpatients colonized or infected with 3rd generation cephalosporin resistant Enterobacterales. Sci. Rep. 2021, 11, 14757. [Google Scholar] [CrossRef]
- Kazmierczak, K.M.; Bradford, P.A.; Stone, G.G.; De Jonge, B.L.M.; Sahm, D.F. In vitro activity of ceftazidime-avibactam and aztreonam-avibactam against OXA-48-carrying Enterobacteriaceae isolated as part of the International Network for Optimal Resistance Monitoring (INFORM) global surveillance program from 2012 to 2015. Antimicrob. Agents Chemother. 2018, 62, e00592-18. [Google Scholar] [CrossRef] [Green Version]
- Seifert, H.; Blondeau, J.; Dowzicky, M.J. In vitro activity of tigecycline and comparators (2014–2016) among key WHO ‘priority pathogens’ and longitudinal assessment (2004–2016) of antimicrobial resistance: A report from the T.E.S.T. study. Int. J. Antimicrob. Agents 2018, 52, 474–484. [Google Scholar] [CrossRef]
- Jean, S.S.; Coombs, G.; Ling, T.; Balaji, V.; Rodrigues, C.; Mikamo, H.; Kim, M.J.; Rajasekaram, D.G.; Mendoza, M.; Tan, T.Y.; et al. Epidemiology and antimicrobial susceptibility profiles of pathogens causing urinary tract infections in the Asia-Pacific region: Results from the Study for Monitoring Antimicrobial Resistance Trends (SMART), 2010–2013. Int. J. Antimicrob. Agents 2016, 47, 328–334. [Google Scholar] [CrossRef]
- Fernández-Martínez, M.; González-Rico, C.; Gozalo-Margüello, M.; Marco, F.; Gracia-Ahufinger, I.; Aranzamendi, M.; Sánchez-Díaz, A.M.; Vicente-Rangel, T.; Chaves, F.; Calvo Montes, J.; et al. Molecular characterization of multidrug resistant Enterobacterales strains isolated from liver and kidney transplant recipients in Spain. Sci. Rep. 2021, 11, 11875. [Google Scholar] [CrossRef] [PubMed]
- Rossolini, G.M.; Bochenska, M.; Fumagalli, L.; Dowzicky, M. Trends of major antimicrobial resistance phenotypes in enterobacterales and gram-negative non-fermenters from ATLAS and EARS-net surveillance systems: Italian vs. European and global data, 2008-2018. Diagn. Microbiol. Infect. Dis. 2021, 101, 115512. [Google Scholar] [CrossRef] [PubMed]
- Garpvall, K.; Duong, V.; Linnros, S.; Quốc, T.N.; Mucchiano, D.; Modeen, S.; Lagercrantz, L.; Edman, A.; Le, N.K.; Huong, T.; et al. Admission screening and cohort care decrease carbapenem resistant enterobacteriaceae in Vietnamese pediatric ICU’s. Antimicrob. Resist. Infect. Control 2021, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- van Duin, D.; Arias, C.A.; Komarow, L.; Chen, L.; Hanson, B.M.; Weston, G.; Cober, E.; Garner, O.B.; Jacob, J.T.; Satlin, M.J.; et al. Molecular and Clinical Epidemiology of Carbapenem-Resistant Enterobacteriaceae in the United States: A Prospective Cohort Study. Lancet Infect Dis. 2020, 20, 731–741. [Google Scholar] [CrossRef]
- Sukhorukova, M.V.; Edelstein, M.V.; Ivanchik, N.V.; Skleenova, E.Y.; Shajdullina, E.R.; Azyzov, I.S.; Shek, E.A.; Kuzmenkov, A.Y.; Dekhnich, A.V.; Kozlov, R.S.; et al. Antimicrobial resistance of nosocomial Enterobacterales isolates in Russia: Results of multicenter epidemiological study “MARATHON 2015–2016”. Clin. Microbiol. Antimicrob. Chemother. 2019, 21, 147–159. [Google Scholar] [CrossRef]
- Kazmierczak, K.M.; De Jonge, B.L.M.; Stone, G.G.; Sahm, D.F. In vitro activity of ceftazidime/avibactam against isolates of Enterobacteriaceae collected in European countries: INFORM global surveillance 2012–2015. J. Antimicrob. Chemother. 2018, 73, 2782–2788. [Google Scholar] [CrossRef]
- Decousser, J.W.; Woerther, P.L.; Soussy, C.J.; Fines-Guyon, M.; Dowzicky, M.J. The tigecycline evaluation and surveillance trial; assessment of the activity of tigecycline and other selected antibiotics against gram-positive and gram-negative pathogens from France collected between 2004 and 2016. Antimicrob. Resist. Infect. Control 2018, 7, 68. [Google Scholar] [CrossRef]
- Vihta, K.D.; Stoesser, N.; Llewelyn, M.J.; Quan, T.P.; Davies, T.; Fawcett, N.J.; Dunn, L.; Jeffery, K.; Butler, C.C.; Hayward, G.; et al. Trends over time in Escherichia coli bloodstream infections, urinary tract infections, and antibiotic susceptibilities in Oxfordshire, UK, 1998–2016: A study of electronic health records. Lancet Infect. Dis. 2018, 18, 1138–1149. [Google Scholar] [CrossRef] [Green Version]
- Yasmin, M.; Fouts, D.E.; Jacobs, M.R.; Haydar, H.; Marshall, S.H.; White, R.; D’Souza, R.; Lodise, T.P.; Rhoads, D.D.; Hujer, A.M.; et al. Monitoring ceftazidime-avibactam and aztreonam concentrations in the treatment of a bloodstream infection caused by a multidrug- resistant enterobacter sp. carrying both klebsiella pneumoniae carbapenemase-4 and new delhi metallo-β-lactamase-1. Clin. Infect. Dis. 2020, 71, 1095–1098. [Google Scholar] [CrossRef]
- Meredith, H.R.; Kularatna, S.; Nagaro, K.; Nagahawatte, A.; Bodinayake, C.; Kurukulasooriya, R.; Wijesingha, N.; Harden, L.B.; Piyasiri, B.; Hammouda, A.; et al. Colonization with multidrug-resistant Enterobacteriaceae among infants: An observational study in southern Sri Lanka. Antimicrob. Resist. Infect. Control 2021, 10, 72. [Google Scholar] [CrossRef]
- Paveenkittiporn, W.; Lyman, M.; Biedron, C.; Chea, N.; Bunthi, C.; Kolwaite, A.; Janejai, N. Molecular epidemiology of carbapenem-resistant Enterobacterales in Thailand, 2016–2018. Antimicrob. Resist. Infect. Control 2021, 10, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Daikos, G.L.; Giusy, T.; Bassoulis, D.; Giordano, C.; Valentina, G.; Leonildi, A.; Tagliaferri, E.; Barnini, S.; Sani, S.; et al. Efficacy of ceftazidime-avibactam plus aztreonam in patients with bloodstream infections caused by MBL-producing Enterobacterales. Clin. Infect. Dis. 2021, 72, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Karlowsky, J.A.; Kazmierczak, K.M.; Bouchillon, S.K.; De Jonge, B.L.M.; Stone, G.G.; Sahm, D.F. In Vitro Activity of Ceftazidime-Avibactam against Clinical Isolates of Enterobacteriaceae and Pseudomonas aeruginosa Collected in Latin American Countries: Results from the INFORM global surveillance program, 2012 to 2015. Antimicrob. Agents Chemother. 2019, 63, 1–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, G.G.; Bradford, P.A.; Newell, P.; Wardman, A. In Vitro Activity of Ceftazidime- Avibactam against Isolates in a Phase 3 Open-Label Clinical Trial for Complicated Intra-Abdominal and Urinary Tract Infections Caused by Ceftazidime- Nonsusceptible Gram-Negative Pathogens. Antimicrob. Agents Chemother. 2016, 61, e01820-16. [Google Scholar] [CrossRef] [Green Version]
- Sader, H.S.; Carvalhaes, C.G.; Duncan, L.R.; Flamm, R.K.; Shortridge, D. Susceptibility trends of ceftolozane/tazobactam and comparators when tested against European Gram-negative bacterial surveillance isolates collected during 2012-18. J. Antimicrob. Chemother. 2020, 75, 2907–2913. [Google Scholar] [CrossRef]
- Tsutsui, A.; Yahara, K.; Shibayama, K. Trends and patterns of national antimicrobial consumption in Japan from 2004 to 2016. J. Infect. Chemother. 2018, 24, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Perez, F.; El Chakhtoura, N.G.; Papp-Wallace, K.M.; Wilson, B.M.; Bonomo, R.A. Treatment options for infections caused by carbapenem-resistant Enterobacteriaceae: Can we apply “precision medicine” to antimicrobial chemotherapy? Expert Opin. Pharmacother. 2016, 17, 761–781. [Google Scholar] [CrossRef] [Green Version]
- Patel, G.; Huprikar, S.; Factor, S.H.; Jenkins, S.G.; Calfee, D.P. Outcomes of Carbapenem-Resistant Klebsiella pneumoniae Infection and the Impact of Antimicrobial and Adjunctive Therapies. Infect. Control Hosp. Epidemiol. 2008, 29, 1099–1106. [Google Scholar] [CrossRef]
- CLSI Standard M07; Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically, 11th ed. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018.
- EUCAST. The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 10.0. 2020. Available online: http://www.eucast.org (accessed on 8 June 2022).
- Lob, S.H.; Kazmierczak, K.M.; Badal, R.E.; Hackel, M.A.; Bouchillon, S.K.; Biedenbach, D.J.; Sahm, D.F. Trends in susceptibility of Escherichia coli from intra-abdominal infections to ertapenem and comparators in the United States according to data from the SMART program, 2009 to 2013. Antimicrob. Agents Chemother. 2015, 59, 3606–3610. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | |
|---|---|---|
| Patient gender: | Male | 1969 [51.67%] |
| Female | 1832 [48.07%] | |
| Unknown | 10 [0.26%] | |
| Patient age, Me (IQR) | 54 (31:65) | |
| Age group: | 0 to 2 years | 242 [6.35%] |
| 3 to 12 years | 285 [7.48%] | |
| 13 to 18 years | 55 [1.44%] | |
| 19 to 44 years | 898 [23.56%] | |
| 45 to 64 years | 1290 [33.85%] | |
| 65 to 84 years | 922 [24.19%] | |
| 85 and over | 105 [2.76%] | |
| Unknown | 14 [0.37%] | |
| Source | Intra-abdominal infection | 614 [16.11%] |
| Urinary tract infection | 1069 [28.05%] | |
| Skin and soft tissue infection | 894 [23.46%] | |
| Lower respiratory tract infection | 1234 [32.38%] | |
| Referring ward | Non-intensive care unit | 3018 [79.19%] |
| Intensive care unit | 753 [19.76%] | |
| Unknown | 40 [1.05%] | |
| Species | Number of Isolates (% of the Total Number) |
|---|---|
| Escherichia coli | 1314 [34.48%] |
| Klebsiella pneumoniae | 1246 [32.69%] |
| Enterobacter cloacae | 297 [7.79%] |
| Proteus mirabilis | 255 [6.69%] |
| Klebsiella oxytoca | 130 [3.41%] |
| Citrobacter freundii | 100 [2.62%] |
| Serratia marcescens | 100 [2.62%] |
| Morganella morganii | 85 [2.23%] |
| Klebsiella aerogenes | 76 [1.99%] |
| Proteus vulgaris | 56 [1.47%] |
| Citrobacter braakii | 24 [0.63%] |
| Enterobacter asburiae | 16 [0.42%] |
| Providencia rettgeri | 15 [0.39%] |
| Klebsiella variicola | 12 [0.31%] |
| Enterobacter, non-speciated | 11 [0.29%] |
| Proteus hauseri | 10 [0.26%] |
| Citrobacter koseri | 9 [0.24%] |
| Raoultella ornithinolytica | 9 [0.24%] |
| Enterobacter kobei | 6 [0.16%] |
| Serratia liquefaciens | 6 [0.16%] |
| Citrobacter farmeri | 5 [0.13%] |
| Enterobacter ludwigii | 5 [0.13%] |
| Providencia alcalifaciens | 5 [0.13%] |
| Providencia stuartii | 5 [0.13%] |
| Citrobacter amalonaticus | 4 [0.1%] |
| Hafnia alvei | 3 [0.08%] |
| Proteus penneri | 3 [0.08%] |
| Pluralibacter gergoviae | 1 [0.03%] |
| Raoultella planticola | 1 [0.03%] |
| Serratia odorifera | 1 [0.03%] |
| Serratia ureilytica | 1 [0.03%] |
| Species | Total | Intra-Abdominal Infections | Urinary Tract Infections | Skin and Soft Tissue Infections | Lower Respiratory Tract Infections |
|---|---|---|---|---|---|
| All Isolates | N = 3811 | N = 614 | N = 1069 | N = 894 | N = 1234 |
| Klebsiella spp. | 1464 [38.42%] | 186 [30.29%] | 287 [26.85%] | 274 [30.65%] | 717 [58.1%] |
| Escherichia spp. | 1314 [34.48%] | 265 [43.16%] | 502 [46.96%] | 329 [36.8%] | 218 [17.67%] |
| Enterobacter spp. | 335 [8.79%] | 60 [9.77%] | 74 [6.92%] | 102 [11.41%] | 99 [8.02%] |
| Proteus spp. | 324 [8.5%] | 33 [5.37%] | 116 [10.85%] | 94 [10.51%] | 81 [6.56%] |
| Citrobacter spp. | 142 [3.73%] | 34 [5.54%] | 33 [3.09%] | 43 [4.81%] | 32 [2.59%] |
| Serratia spp. | 108 [2.83%] | 11 [1.79%] | 17 [1.59%] | 21 [2.35%] | 59 [4.78%] |
| Morganella spp. | 85 [2.23%] | 16 [2.61%] | 31 [2.9%] | 19 [2.13%] | 19 [1.54%] |
| Providencia spp. | 25 [0.66%] | 7 [1.14%] | 8 [0.75%] | 9 [1.01%] | 1 [0.08%] |
| Raoultella spp. | 10 [0.26%] | 1 [0.16%] | 1 [0.09%] | 2 [0.22%] | 6 [0.49%] |
| Hafnia spp. | 3 [0.08%] | 1 [0.16%] | 0 [0%] | 0 [0%] | 2 [0.16%] |
| Pluralibacter spp. | 1 [0.03%] | 0 [0%] | 0 [0%] | 1 [0.11%] | 0 [0%] |
| Concentrations, mg/L | Cumulative Rate | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | ≤0.015 | 0.03 | 0.06 | 0.12 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | 16 | 32 | 64 | 128 | ≥256 | Susceptible | Intermediate | Resistant |
| Aztreonam/avibactam | 16.2 | 39.3 | 68.6 | 87.9 | 96.1 | 98.2 | 98.8 | 99.3 | 99.6 | 99.8 | 99.9 | 99.9 | 99.9 | 99.9 | 100 | 98.8 | 0.8 | 0.4 |
| Ceftazidime/avibactam | 3.2 | 9.9 | 29.7 | 55.4 | 74.2 | 88.9 | 95.4 | 97.2 | 97.9 | 98 | 98 | 98 | 98 | 98.1 | 100 | 98 | 0 | 2.1 |
| Ceftaroline/avibactam | 7.9 | 27.6 | 53.7 | 77.9 | 90.2 | 96.2 | 98.8 | 99.5 | 99.6 | 99.7 | 99.8 | 99.8 | 99.8 | 99.8 | 100 | 96.2 | 0 | 3.8 |
| Doripenem | 4 | 36.6 | 66.6 | 81.3 | 88.6 | 93 | 95.6 | 96.8 | 97.7 | 99.1 | 100 | 95.6 | 1.1 | 3.2 | ||||
| Tigecycline | 0 | 1.7 | 15.3 | 41.8 | 68.4 | 85.2 | 94.8 | 98.5 | 99.8 | 100 | 94.8 | 3.7 | 1.6 | |||||
| Meropenem | 8.8 | 42.3 | 77.9 | 87.8 | 90.6 | 91.3 | 92.5 | 94.1 | 95.6 | 96.2 | 98.3 | 100 | 92.5 | 1.6 | 5.9 | |||
| Ertapenem | 27.9 | 46.6 | 59.4 | 71 | 79.4 | 89.1 | 92 | 100 | 89.1 | 3 | 8 | |||||||
| Amikacin | 0.1 | 2.8 | 21.5 | 50.5 | 74.8 | 85.3 | 88.7 | 89.8 | 97.4 | 100 | 88.7 | 1.1 | 10.2 | |||||
| Imipenem | 0 | 2 | 26.3 | 58.9 | 74 | 82.7 | 89.4 | 95.4 | 96.8 | 100 | 82.7 | 6.7 | 10.6 | |||||
| Ceftolozane/tazobactam | 0.2 | 0.4 | 1.9 | 21.7 | 54.5 | 67.5 | 76.4 | 79.4 | 82.1 | 85.3 | 88.5 | 89.6 | 100 | 79.4 | 2.8 | 17.9 | ||
| Piperacillin/tazobactam | 0.2 | 5 | 10.1 | 22.9 | 47.2 | 60.7 | 67.1 | 75.2 | 80.1 | 83.5 | 89.9 | 100 | 75.2 | 8.3 | 16.5 | |||
| Cefoperazone/sulbactam | 0 | 1.6 | 22.6 | 29 | 39.2 | 43.6 | 48.2 | 55.2 | 62.1 | 68.7 | 82.8 | 87 | 100 | 68.7 | 14.1 | 17.3 | ||
| Gentamicin | 1.8 | 26.3 | 54.8 | 64.1 | 66.4 | 66.7 | 67.3 | 69 | 100 | 66.7 | 0.5 | 32.7 | ||||||
| Ceftazidime | 0.2 | 1.7 | 9 | 27.5 | 42.1 | 48.4 | 50.9 | 54.3 | 57.4 | 60.8 | 65.4 | 72 | 79.5 | 87.8 | 100 | 57.4 | 3.4 | 39.2 |
| Aztreonam | 6.4 | 11.7 | 29.1 | 42.6 | 47.2 | 49.1 | 50.4 | 51.5 | 54.1 | 57 | 61 | 68.1 | 77.4 | 89.9 | 100 | 54.1 | 2.9 | 43 |
| Levofloxacin | 0.1 | 16.4 | 31.9 | 38.7 | 47.4 | 53.1 | 56.9 | 59.6 | 63.5 | 85.8 | 100 | 53.1 | 3.8 | 43.1 | ||||
| Cefepime | 0 | 0 | 45 | 47.7 | 49.4 | 51.1 | 52.9 | 55.3 | 59.1 | 63.8 | 94.6 | 100 | 52.9 | 6.2 | 40.9 | |||
| Ceftriaxone | 37.9 | 44.6 | 49.4 | 50.2 | 51.3 | 52 | 52.6 | 53.1 | 54.4 | 100 | 51.3 | 0.7 | 48 | |||||
| Co-trimoxazole | 47.7 | 50.2 | 51.1 | 53 | 53.4 | 54.1 | 100 | 50.2 | 0 | 49.8 | ||||||||
| Ciprofloxacin | 41.1 | 44.7 | 47.7 | 51.4 | 53.2 | 56.1 | 100 | 44.7 | 3 | 52.3 | ||||||||
| Ceftaroline | 0.5 | 5 | 18.4 | 32.6 | 40.7 | 44.3 | 46.3 | 47.4 | 48.1 | 49.1 | 58.1 | 59.1 | 60.7 | 63 | 100 | 44.3 | 2 | 53.7 |
| Amoxicillin/clavulanate | 0 | 0.4 | 3.1 | 16.5 | 28.3 | 40.5 | 63.7 | 92.1 | 100 | 40.5 | 23.2 | 36.3 | ||||||
| Ampicillin/sulbactam | 2.5 | 8 | 19.6 | 31.2 | 41.8 | 57.5 | 68.3 | 100 | 31.1 | 10.7 | 58.2 | |||||||
| Ampicillin | 0.3 | 2 | 6.9 | 13.7 | 16.4 | 19.2 | 35.9 | 100 | 16.4 | 2.8 | 80.8 | |||||||
| Colistin | 0.2 | 2.5 | 29.5 | 64.9 | 85.2 | 86.3 | 86.8 | 90.7 | 100 | 0 | 86.3 | 13.8 | ||||||
| Antimicrobial | Resistance Rate | Dynamics over Years | ||
|---|---|---|---|---|
| Enterobacteriaceae | E. coli | K. pneumoniae | ||
| Aminoglycosides | 10.23% | 2.97% | 17.26% |  |
| Carbapenems | 11.6% | 1.22% | 19.1% |  |
| Cephalosporins | 53.98% | 45.21% | 78.25% |  |
| Glycylcyclines | 1.55% | 0% | 0.4% |  |
| Polymyxins | 9.76% | 0.46% | 0.8% |  |
| Monobactams | 43.03% | 33.33% | 73.35% |  |
| Penicillins in combination with a β-lactamase-inhibitor | 38.65% | 10.96% | 48.64% |  |
| Quinolones | 43.09% | 42.16% | 65.73% |  |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozlov, R.; Kuzmenkov, A. The Dynamics of Antimicrobial Resistance among Enterobacteriaceae Isolates in Russia: Results of the 2012–2018 INFORM and ATLAS International Program Studies. Antibiotics 2022, 11, 790. https://doi.org/10.3390/antibiotics11060790
Kozlov R, Kuzmenkov A. The Dynamics of Antimicrobial Resistance among Enterobacteriaceae Isolates in Russia: Results of the 2012–2018 INFORM and ATLAS International Program Studies. Antibiotics. 2022; 11(6):790. https://doi.org/10.3390/antibiotics11060790
Chicago/Turabian StyleKozlov, Roman, and Alexey Kuzmenkov. 2022. "The Dynamics of Antimicrobial Resistance among Enterobacteriaceae Isolates in Russia: Results of the 2012–2018 INFORM and ATLAS International Program Studies" Antibiotics 11, no. 6: 790. https://doi.org/10.3390/antibiotics11060790