
Fighting Antimicrobial Resistance: Development and Implementation of the Ghanaian National Action Plan (2017–2021)

 ,
,
Abstract
:1. Background
1.1. AMR-Related Politics and the Development of the NAP
1.2. NAP: Its Final Shape
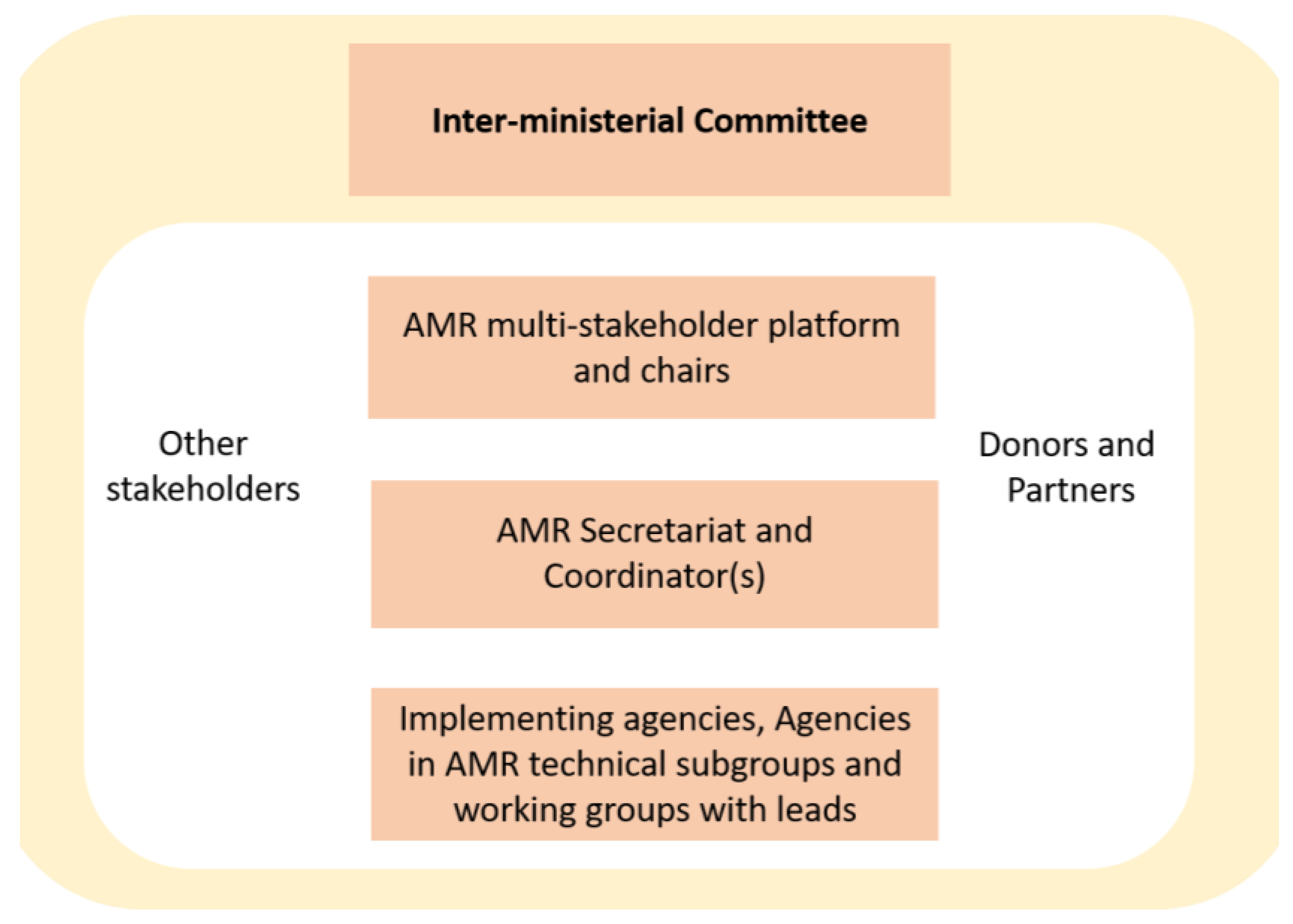
1.3. AMR Policy Structure in Ghana
1.4. Overall Research Objectives
2. Methods
2.1. Study Design
2.2. Study Participants
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Emerging Areas of Research
- ○
- Establish a well-functioning One Health governance structure for AMR and AMU surveillance;
- ○
- Establish a government led system of collecting, collating, analysing, reporting and disseminating AMR and AMU data on national and international platforms in alignment with the requirements of the WHO GLASS;
- ○
- Strengthen AMR and AMU surveillance in animals.
3.2. Results from Interviews and Most Recent Information
3.2.1. Incomplete Implementation of Surveillance Systems
“…when you come to antimicrobial consumption, …there was a pilot… done, through the support of WHO Ghana, to get the data from various selected health facilities. And so, that is one of the first pilots that we’ve done on how to capture antimicrobial consumption data in Ghana. And then also under the Fleming Fund, we started a process to get the data on import, local production, local export of pharmaceuticals; the drugs, so that we can know the quantity of antimicrobials consumed in a year in the country. And that process was also started but it has been put on hold. Maybe for second phase of the FF, it will be completed. So, there’s a process in place.”
3.2.2. Importance of the One Health Concept
“…now we share our information at the CC [AMR coordinating committee] meeting every quarter. … we know what is happening in the human health sector, we know what is happening in the environment. This is what we are doing now as a committee at the AMR level”(R13)
3.2.3. Insufficient Enforcement of Regulations for Procurement and Dispensing
“…the pharmaceutical- the health professional regulatory act, talks about what we’re supposed to do when a medicine is dispensed in Ghana. Such implementations are not ongoing. There’s no national intervention to ensure that …the recommendation from the law is being implemented. So, then we still have, I’ll say, lack of control… over the dispensing of drugs in the country”.(R2)
“There may be promoters of resistance in the society by their activities. They have no knowledge about the antimicrobial that they sell around. All they want is money. So, any sickness mentioned, they’ll give you the antibiotics. Whether it will kill the bacteria, whether the sickness is caused by a bacterial infection, they don’t care”.(R2)
“[Smugglers] pass through the unapproved routes, the borders. Yes. So, they always smuggle antibiotics into the country. Whether they are safe or they are efficacious or not, is another issue” (R2). “It’s a whole cartel that is working, a kind of a global menace. …These drugs come through illegal routes … Let’s stick to antibiotics. Antibiotics will need to be stored appropriately… to retain its efficacy. So, I go out I buy some boxes of amoxicillin injection or a few parts of …meropenem or, aminoglycosides…Because they’re not bulky, so if I have a suitcase, I can buy let’s say 10, 20 right, then I come and supply it…. I can buy it at a cheaper cost than the ones that have been imported by those who have registered the products to use. So, we cannot be sure of the supply chain integrity of such products”.(R1)
“we’ve been trying for… more than a decade. …Finally, it became quite clear that we will not be able to make any headway in Ghana. So, we left Ghana and we spent time in Nigeria and Kenya and other places. And yes, in those countries, particularly in Nigeria which is the most advanced, the solution and others like it is used for controlling authenticity.” He further stressed: “… I see the traceability and supply chain solution as the base on which you can build other higher value adding solutions some of which include antimicrobial resistance, surveillance and monitoring systems”.(R12)
3.2.4. Governance Structures for Implementing the NAP (Institutions and Regulations)
“Well, health systems in general in Ghana, is not at its peak... if you take one aspect, governance alone is good on paper but practically it’s not so strong”.(R9)
“When you look at the NAP or the policy, there is a governance structure [description of the governance framework presented in Figure 1]…the secretariat coordinates all the activities, and the inter-ministerial body is the highest decision-making body, and the platform is like a clearing house where everything is brought there... decisions are made, directives are given and we go and work. That is the governance structure. In terms of reporting, the secretariat is supposed to demand reports from all agencies including the GHS and collate that into one as Ghana report. That is how the system works. … But... close to 60, 65 percent of activities in the NAP are still hanging... not started at all because of funding issues so you can see that if they have not started you will not get any report” (R9). The same respondent added (after a long explanation on the ubiquitous access to antibiotics): “So, there are laws but the enforcement is weak. It is a system-wide problem. It is not just about the regulatory agencies. I keep saying that it is more of access and equity …” (referring to difficult access to pharmacies in remote regions).(R9, also R1)
“…we were able to take up pieces of legislation on AMR from all sectors. From environment, from health, from Agric; if it comes to Agric, from animal side, from crop side, from fishery side. So, we were able to pick those pieces, put them together as AMR legislation for Ghana… Now, we have gotten to a stage where we are working on passing … the revised version into law and if that is completed, then we can use that law to implement most of the AMR activities because everything should be backed by law… So, with time, as and when we get this recommendation passed into law, the enforcement will be good. But as at now, we haven’t achieved what we want to achieve in that area”.(R4)
“…let’s push budget there and be able to implement them. So, now, the policies are being used in the various organizations for the implementation of the AMR activities, and another thing we did was to help ministry departments and agencies to mainstream the NAP into the medium-term development plans, so that AMR activities become part of their organizational plans for implementation”.(R4)
“I think the challenge is very much there and what we are trying to do is to leverage on certain existing laws which are luckily been reviewed now, so that we can leverage on these reviews to enforce the law. So that problem still persists, so this is how we intend to address the problem”.(R6)
3.2.5. Mobilizing Financial Means for Implementing NAP
“The key problem I see is financial. When you look at the NAP activities, all the institutions involved have the capacities to implement the activities as stated in the NAP, so if we get the funding the NAP can be implemented according to the plan”.(R10)
“All the researchers on the platform have redirected our research into AMR related issues, but I have not seen a kind of dedicated budget of these ministries. If there are dedicated budgets…perhaps there would have been more frequent engagements with our partners and stakeholders…towards the implementation”.(R1)
“The NAP was supposed to be integrated into the sector ministries budget… as we speak now, I can’t tell whether it’s been done yet. So again, the reliance has been on external funding… if we should really want things to work then we should be looking at budgeting for it and getting it implemented… I don’t think the sector ministries have them in their budget”.(R11)
“You know when the AMR policy and the National Action Plan were ready, it was the President himself that launched those documents at the International Conference Center, and that day, he urged the Minister of Finance to support the implementation of AMR and the national action plan. So that is a plus. Soon after that, the Minister of Health in a very good initiative brought the Global Call to Action on AMR to Ghana. …And that brought international AMR stakeholders to Ghana. Ghana was given money from the UK Government for AMR implementation…. And again, I always tell at our meetings, …, yes, government is supporting AMR in so many ways that we don’t see directly. For example, …infection prevention activity is purely AMR activity…Likewise, …the Veterinary Services, they’ve also got budgets for infection prevention activities. The vaccinations that we have been doing all around every year is part of AMR, is pure AMR activity. If you do vaccination you… prevent the development of diseases, then you don’t use antimicrobials. So, in this way, I think the government is mobilizing funds for the support of the AMR. What…we haven’t seen is actively… bringing in money … with the title that this money is going for AMR. But there are so many funds that are coming to the system for implementation of development plans. …if we are able to quantify those things, then we can see that yes, there’s enough budget allocation from the government for AMR”.(R4)
“Some of these international communities, they want to see government commitment. But in terms of government commitment, I haven’t seen that level of commitment. May be the environment sector’s implementation is strengthened because UNEP is now involved”.(R10)
3.2.6. Mechanisms of Mobilising International Partners
“I think, it would be great to even bring all of the supporting institutions to work together synergistically, some of these are very disjointed. So it’s only those of us who are working with the platform, we get to know about them and we inform… and they try to embrace or try to get information from … their [partners]… and then how relevant it is towards the NAP implementation”.(R1)
“But then we have had these challenges, where even at a point in time, you know, equipment that are needed in the field to work and generate the needed data has not still gone down to the field, in spite of the fact that capacity of the practitioners has been developed [reference to the interruption of the Fleming Fund project on surveillance, see above]. There are also fears that even once [human] capacity is developed, and they get some lucrative job, they may leave so there may be the need for retraining, once we’re able to get things in place. But I agree that there has to be, … somebody who is looking at; the … AMR Secretariat is being actually tasked, … but I don’t know if they have the powers to work with [international organisations]”.(R1)
“We cannot implement AMR activities without international cooperation; most of the funding comes from WHO and FAO. They supported in developing the National Action Plan. Coordination at the national level is spearheaded by WHO. So, if WHO is going to undertake some activity, they consult FAO, OIE and now UNEP. MoH hosts the AMR secretariat and they organize the platform meetings”.(R10)
“I’ll say that the Tripartite in general actively supported the country to come out with the AMR policy and then the NAP and of course, we are still supporting them to implement some aspects of it… We basically provide technical support and some funding to ensure activities are implemented. …Collaborations with FAO and OIE are excellent, I know, there are AMS activities ongoing by various agencies (Kintampo Health Research Center, KCCR, KNUST). What I can say too is that there is a project coming... the Multi-Partner Trust Fund Project which seeks to pool these agencies together in One Health. Out of that there are crosscutting activities which are supposed to be implemented across the three agencies and that project would hopefully begin somewhere April if all things are put in perspective..(R9)
“We don’t have any role, we were part of the development; our organization contributed, we supported with a letter, everything but when the grant came, we are not involved so we don’t know what exactly they are doing…Our social media team also support creating […] a lot of information but we don’t have any project that is funded by anybody. …For now… ReAct Africa is doing a lot of awareness work”.(R7)
“With the implementation of the Ghana Integrated Logistics Management Information System (GhILMIS) which is being rolled out nationally, we are hoping that we will be able to obtain consumption data moving forward. This roll out is ongoing…, we are planning a meeting where we will ask each region and even each district to nominate a focal AMR person, who will be tasked to make sure the consumption data is collected and reported nationally to feed into the [..] systems and eventually into the WHO GLASS”.(R6)
3.2.7. AMR-Related Teaching, Training and Research in Academic Institutions
[Modules of AMR and AMS?] “No. Currently there are not. … But you know, universities are independent, so we are suggesting but universities have to take time to buy it into their own system…I would not say that there’s no strong interest on AMR in the universities. I suspect that because the NAP has come and has to be integrated into the curricula of the universities, it is now something that they are trying to put in place, because they already had their own programme before and I think that curriculum is not changed every year in the universities”.(R13)
“…in pharmacy, we have actually incorporated antimicrobial stewardship and the role of the pharmacists in AMR containment, at different levels, graduate levels, undergraduate levels and all of that is actually part of the curricula for infectious disease management. But I think we should go beyond that, we should be able to see that in the curricula of Veterinary Medicine, we should see that in the curricula of School of Medicine and Dentistry, we should see that in the curricula of Laboratory Science, you know, all of that so I think we need to move on”.(R1; similar R3)
[Interest among students?]” Yes, huge, you know, … very, very, very huge. A lot of them even take up mini projects, alright, on that …. So, if what is happening in pharmacy can also be replicated, you know, medical school, nursing, at least in their final years or a year to the final year, if they are actually taught about some of these issues, I think that would really be great. But I don’t know which institution or organisation will lead that kind of advocacy”.(R1)
[Oversight by the secretariat] “You know the NAP recommended, that we should have AMR issues included in the curriculum of the teaching of the universities… So, we know that one university, KNUST, started and they’ve done some inclusion already. But the others, we’re yet to find out from them whether they’ve included issues of AMR in their curriculum…. From time to time, the secretariat goes through some of the training institutions, to create awareness…”.(R2)
3.2.8. Awareness Building and the Role of Civil Society (Societal Embedding)
“It will interest you to know that I was not even aware of this AMR thing, until I joined the whole AMR discussion. I think in 2018 there was the WAAW week, they held a programme at the Ministry of Health, that was the first time I participated in it and I understood the whole AMR discussion. So, you see it means that a lot of people are not aware of this whole AMR issue. And I think the awareness creation has been limiting for a long time. Apart from the WAAW week I don’t see any rigorous awareness on this whole AMR thing”.(R10)
“At least every November onwards [WAAW] something should happen and people are aware. … But I can tell you a lot of plans are put on paper but our basic challenge has been funding because people are prepared to work…. People don’t put money into awareness issues because the deliverables are not tangible. I’ll say that gradually the awareness is catching up”.(R9)
“I think the problem with the media is …to do more of the training. I think they have to understand the AMR issues. … even when you have spoken to them about it, when they are reporting, sometimes you realise that the substance in what you shared with them is not what actually they are reporting… When we are doing World Antimicrobial Awareness Week we are going to see more of the media, … we see people going there, buying airtime, or maybe as part of their corporate social responsibility, giving them the platform to talk about AMR issues. … And I think that, you know, we should also work very hard to make the media guys very strong advocates, once they understand the issues, and they make noise about it, and I think that’s one sure way of ensuring massively a real change”.(R1)
[Around 2015] “… the awareness level was measured to be so low, even among the health workers, let alone the general public. The Kintampo Health Research Centre for instance, did the KAPP [Knowledge, attitude and perception/practices) [50] research on awareness creation—Awareness on antimicrobial resistance among the health workers… Objective one [in the NAP] … is awareness creation; every year we do this awareness creation, CSOs are doing the awareness creation, but nobody has gone back to find out what is the level of awareness among the general public”.(R2)
“So, the regions where we [HfFG] have projects actively working, yes. …So, if you ask me about awareness, I think its limited, I will say maybe 0.5, 0.3% of people are aware, maybe listening to TV and radio. You know, when we are celebrating AMR week… I don’t think people are aware because when you talk to people … they become surprised, so we are not doing much when it comes to awareness creation.… Civil society can do more than what they are doing because that is our field; because working with community members, communicating in their language is our work. So, I think we need to just really appreciate, there is a gap that we have, big gap that we must address…you know we work a lot in the communities. When we are meeting mothers for our maternal health, we talk about it, but receiving money purposely for this, no.… Communication [with the NPAR] was very active when we set up the platform. Now the communication, I don’t see it very active but periodically you will see some information on the platform”.(R7)
3.2.9. Ghana’s AMR Politics in the International Context
“Ghana plays a leading role in the fight against AMR in the sub-region and also globally” (R4). “But …I think countries like Kenya, South Africa, okay, and perhaps Ethiopia are overtaking Ghana, right when it comes to implementation… So, we need to step up”.(R1)
“The Call to Action Conference that was funded by Wellcome and the other partners, was really really great. I mean, it brought in a lot more stakeholders, you know, experts who are working in that area, to share ideas…. Usually at the conferences of the International Pharmaceutical Federation, students who have done [work] with the AMR space have had the opportunity to showcase their work”.(R1)
“So far, research and conferences are more geared towards trying to achieve targets for the development of researchers. You are under pressure to publish or perish. So, regarding policy implementation and informing policy that is on our mind, we try to do that, but we focus more on publish or perish. So much more has to be done regarding impact on policy”.(R5)
“… if you look at GLASS reporting… Ghana has not reported anything yet… I think we have worked very hard to be putting the systems and infrastructure in place and probably when we take off we would have smooth systems running. So, we contribute, attending international conferences for most of the international engagement; on the African continent and beyond. For me, I mostly have the opportunity to be sharing data… but that is not enough as far as I am concerned. We must hit the ground and get the evidence. The evidence at the moment is not there, so it is like we are not doing anything”.(R11)
[Role of WHO, FAO, OIE?] “I think without them we would have just been sitting without doing anything. They have been very pressing and pushy. These abilities have gotten us this far. We alone would have been standing aloof”.(R5)
3.2.10. Progress Reports and Evaluation of the NAP (2017–2021): Preparations for a NAP 2?
[Enforcement of existing regulations?] “… during the mid-term review, the AMR secretariat did a rapid review on the implementation of the NAP, and one of the main activities is enforcement of regulation on antimicrobial use in Ghana. No work has started on that arm”.(R2)
“In fact, I happen to be part of a team that did an evaluation of the NAP. We did it early last year. What we did was that we looked at the various actions and evaluated the progress made. All focal persons from the various institutions were on board. So, you ask yourself, this one have we done it, this one have we not done, why? Then we raise the questions; if we have done it, to what level, what is left? It was teamwork, I will say that the focal points of the various institutions involved did their own evaluation. The thinking was that an external person will be contracted to do the evaluation again, but you know all these things require financial resources to undertake so I don’t think that has happened”.(R10)
“…because the plan that we have currently is expiring and we need a new plan. The problem is, you know, they will be doing some monitoring and evaluation, it will be highly technocratic, they will hire some consultation, they’ll do the evaluation but you’ll be very surprised to learn that real consultation in Ghana is often conducted in a manner that, to me, suggest it is perfunctory; they are just checking the box. And I think a lot of that problem persist. I don’t blame the technocrats at specific ministries or bureaucracies alone. I think it is just a general culture that we have in the country that makes accountability just difficult”.(R12)
“I can say our implementation is quite slow from where I sit. If you look at it critically people are prepared to work but everything is about money and if government should put in some money, because I can say the government has taken some of the NAP into the NDPC Plan. And you know, the president also co-chairs the SDGs, …, I remember … he asked that some of the indicators be pushed into SDGs and the National Development... forty-year plan”(R9; reference to Long-term National Development Plan of Ghana (2018–2057), of which only an Outline is available online [52].
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- WHO. Global Action Plan on Antimicrobial Resistance, Geneva. 2015. Available online: https://www.who.int/publications/i/item/978924150976 (accessed on 8 March 2022).
- Koduah, A.; Asare, B.A.; Gavor, E.; Gyansa-Lutterodt, M.; Annan, E.A.; Ofei, F.W. Use of evidence and negotiation in the review of national standard treatment guidelines and essential medicines list: Experience from Ghana. Health Policy Plan. 2019, 34, ii104–ii120. [Google Scholar] [CrossRef] [PubMed]
- React. Report on Stakeholder Analysis for AMR Policy Development Process. Ghana ReAct Project. November 2013. Available online: https://www.reactgroup.org/wp-content/uploads/2016/09/Annex-1-Stakeholder-Analysis.pdf (accessed on 8 March 2022).
- ReAct. Situational Analysis on Antibiotic Resistance in Ghana. ReAct Antibacterial Resistance Project. 2016. Available online: https://www.reactgroup.org/wp-content/uploads/2016/09/Annex-6-Situational-Analysis.pdf (accessed on 8 March 2022).
- Yevutsey, S.K.; Buabeng, K.O.; Aikins, M.; Anto, B.P.; Biritwum, R.B.; Frimodt-Møller, N.; Martha Gyansa-Lutterodt, M. Situational analysis on antibiotic use and resistance in Ghana: Policy and regulation. BMC Public Health 2017, 17, 896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aglanu, L.M. Antibiotic/Antimicrobial Use and Resistance in Ghana and Africa; Kumasi Centre for Collaborative Research in Tropical Medicine: Kumasi, Ghana, 2021; (unpublished manuscript). [Google Scholar]
- DANIDA Research Portal. Antibiotic Drug Use, Monitoring and Evaluation of Resistance in Ghana (ADMER)—A Research Capacity Building Project. Available online: http://drp.dfcentre.com/project/antibiotic-drug-use-monitoring-and-evaluation-resistance-ghana-admer-research-capacity (accessed on 8 March 2022).
- ReACT. About Us. Our Funding. Available online: https://www.reactgroup.org/about-us/funding/ (accessed on 8 March 2022).
- Koduah, A.; Gyansa-Lutterodt, M.; Hedidor, G.K.; Sekyi-Brown, R.; Asiedu-Danso, M.; Adu Asare, B.; Ama Ackon, A.; Andrews Annan, E. Antimicrobial resistance national level dialogue and action in Ghana: Setting and sustaining the agenda and outcomes. One Health Outlook 2021, 3, 18. [Google Scholar] [CrossRef]
- WHO. Health Topics. One Health. Available online: https://www.who.int/news-room/questions-and-answers/item/one-health (accessed on 9 March 2022).
- Republic of Ghana, Ministry of Health. Policy on Antimicrobial Use and Resistance. 2017. Available online: https://www.moh.gov.gh/wp-content/uploads/2018/04/AMR-POLICY-A5_09.03.2018-Signed.pdf (accessed on 10 March 2022).
- Republic of Ghana, Ministry of Health, Ministry of Food and Agriculture, Ministry of Environment, Science Technology and Innovation, Ministry of Fisheries and Aquaculture Development. Ghana National Action Plan for Antimicrobial Use and Resistance, 2017–2021; Ministry of Health: Accra, Ghana, 2017.
- WHO/FAO/OIE/. Antimicrobial Resistance: A Manual for Developing National Action Plans. 2016. Available online: https://apps.who.int/iris/handle/10665/204470 (accessed on 15 March 2022).
- Nortey, P. National AMR Strategies: The Ghana Story. In Proceedings of the 2nd Global Network for Antimicrobial Resistance and Infection Prevention Symposium, Makarere University, Kampala, Uganda, 4–7 March 2019; Available online: https://cdn.southampton.ac.uk/assets/imported/transforms/content-block/UsefulDownloads_Download/A96E467D9D1044B1A621ACEFAD9668D9/P%20Nortey%20-%20Ghana%20AMR%20Strategy.pdf (accessed on 15 March 2022).
- Harant, A. Assessing Transparency and Accountability of National Action Plans on Antimicrobial Resistance in 15 African Countries. Antimicrob. Resist. Infect. Control 2022, 11, 15. [Google Scholar] [CrossRef]
- Frumence, G.; Mboera, L.E.G.; Sindato, C.; Katale, B.Z.; Kimera, S.; Metta, E.; Durrance-Bagale, A.; Jung, A.-S.; Mshana, S.E.; Clark, T.G.; et al. The Governance and Implementation of the National Action Plan on Antimicrobial Resistance in Tanzania: A Qualitative Study. Antimicrob. Resist. Infect. Control Antibiot. 2021, 10, 273. [Google Scholar] [CrossRef]
- Amin, E.T.; Omeichu, A.A.; Shu, D.M.; Ekome, S.R.E.; Njumkeng, C.; van der Sande, M.A.B. Control of Antimicrobial Resistance in Cameroon: Feasibility of Implementing the National Action Plan. Trop. Med. Int. Health. 2021, 26, 1231–1239. [Google Scholar] [CrossRef]
- Okeke, I.N.; Laxminarayan, R.; Bhutta, Z.A.; Duse, A.G.; Jenkins, P.; O’Brien, T.F.; Pablos-Mendez, A.; Klugman, K.P. AMR resistance in developing countries. Part I: Recent trends and current status. Lancet Infect. Dis. 2005, 5, 481–493. [Google Scholar] [CrossRef]
- van Dijck, C.; Vlieghe, E.; Cox, J.A. Antibiotic stewardship interventions in hospitals in low-and middle-income countries: A systematic review. Bull. World Health Organ. 2018, 96, 266–280. [Google Scholar] [CrossRef]
- Cox, J.A.; Vlieghe, E.; Mendelson, M.; Wertheim, H.; Ndegwa, L.; Villegas, M.V.; Gould, I.; Levy Hara, G. Antibiotic stewardship in low- and middle-income countries: The same but different? Clin. Microbiol. Infect. 2017, 23, 812–818. [Google Scholar] [CrossRef] [Green Version]
- ReAct. Ghana’s national policy (Toolbox, Policy. Inspirational Examples). Available online: https://www.reactgroup.org/toolbox/policy/examples-from-the-field/ghanas-national-antibiotic-policy/ (accessed on 1 May 2022).
- WHO. Resource Mobilisation for Antimicrobial Resistance (AMR): Getting AMR into Plans and Budgets of Government and Development Partners. Ghana Country Level Report. 2018. Available online: https://www.who.int/antimicrobial-resistance/national-action-plans/Ghana-AMR-integration-report-WHO-June-2018.pdf?ua=1 (accessed on 15 March 2022).
- ReAct. Ghana’s National Action Plan on AMR—ReAct Africa Supports the Process. (News and Opinions 2018). Available online: https://www.reactgroup.org/news-and-views/news-and-opinions/year-2018/ghana-national-action-plan-on-amr-react-africa-supports-the-process/ (accessed on 15 March 2022).
- Anderson, M.; Schulze, K.; Cassini, A.; Plachouras, D.; Mossialos, E. A Governance Framework for Development and Assessment of National Action Plans on Antimicrobial Resistance. Lancet Infect Dis. 2019, 19, e371–e384. [Google Scholar] [CrossRef] [Green Version]
- García-Vello, P.; González-Zorn, B.; Setsoafia Saba, C.K. Antibiotic Resistance Patterns in Human, Animal, Food and Environmental Isolates in Ghana: A Review. Pan Afr. Med. J. 2020, 35, 37. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7245977/pdf/PAMJ-35-37.pdf (accessed on 15 March 2022). [CrossRef] [PubMed]
- Opintan, J.A.; Newman, M.J.; Arhin, R.E.; Donkor, E.S.; Gyansa-Lutterodt, M.; Mills-Pappoe, W. Laboratory-Based Nationwide Surveillance of Antimicrobial Resistance in Ghana. Infect. Drug Resist. 2015, 8, 379–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report 2021. 2021. Available online: https://apps.who.int/iris/rest/bitstreams/1350455/retrieve (accessed on 15 March 2022).
- The Fleming Fund. Terms of Reference for Request for Proposals. Ghana First Country Grant. 2018. Available online: https://www.flemingfund.org/wp-content/uploads/c9321a9a51d977b11bec3e95c8fb9438.pdf (accessed on 16 March 2022).
- Hitch, G.; Danquah, C.A.; Owusu-Ofori, A.; Agyarko-Poku, T.; Manfrin, A.; Owusu-Dabo, E.; Buabeng, K.O. Public Perceptions on the Use of Antibiotics at a Market Place in Kumasi, Ghana: A Cross-Sectional Study. Glob. J. Med. Public Health 2020. Available online: http://clok.uclan.ac.uk/35806/ (accessed on 16 March 2022).
- Republic of Ghana. The Budget Statement and Economic Policy of the Government of Ghana for the 2019 Financial Year. 2019. Available online: https://www.mofep.gov.gh/sites/default/files/budget-statements/2019-Budget-Statement-and-Economic-Policy.pdf (accessed on 16 March 2022).
- Opintan, J. Leveraging Donor Support to Develop a National Antimicrobial Resistance Policy and Action Plan: Ghana’s Success Story. Afr. J. Lab. Med. 2018, 7, a825. [Google Scholar] [CrossRef]
- The Fleming Fund (Website): Our Activities: Governance. Support Strong National AMR Governance. Available online: https://www.flemingfund.org/wp-content/uploads/debcf5faea0903a502c05326a4ac3c1c.pdf (accessed on 16 March 2022).
- Jimah, T.; Fenny, A.P.; Ogunseiten, O. Antibiotics stewardship in Ghana: A cross-sectional study of public knowledge, attitudes, and practices among communities. One Health Outlook 2020, 2, 12. [Google Scholar] [CrossRef]
- ReAct. About Us. Our Story. (Section: 2015: ReAct Africa). 2015. Available online: https://www.reactgroup.org/about-us/our-story// (accessed on 16 March 2022).
- WHO. Monitoring and Evaluation of the Global Action Plan on Antimicrobial Resistance. Regional Expert Consultation on Monitoring and Evaluation of AMR Interventions. 2017. Available online: https://www.paho.org/hq/dmdocuments/2017/2017-cha-walford-global-dc.pdf (accessed on 16 March 2022).
- Zaney, G.D. Ghana’s National Action Plan on AMR Implementation on Course? But It Requires Support From All. GH Headlines, All Africa News Ghana. 27 August 2019. Available online: http://www.ghheadlines.com/agency/all-africanews--ghana/20190827/130866936/ghanas-national-action-plan-on-amr-implementation-on-coursebut-it-requires-support-from-all (accessed on 16 March 2022).
- Isawumi, A.; Mosi, L. Monitoring Antimicrobial Resistance in Ghana: A Focus on the Hospital Environment, REVIVE. Advancing antimicrobial R&D (GARDP). 18 January 2021. Available online: https://revive.gardp.org/monitoring-antimicrobial-resistance-in-ghana-a-focus-on-the-hospital-environment/ (accessed on 16 March 2022).
- The Fleming Fund. Ghana: Country Grant 2. 2020. Available online: https://www.flemingfund.org/grants/ghana-country-grant-2/ (accessed on 16 March 2022).
- Amponsah, O.K.O.; Buabeng, K.O.; Owusu-Ofori, A.; Hämeen-Anttila, K.; Enlund, H. Point Prevalence Survey of Antibiotic consumption across Three Hospitals in Ghana. JAC-Antimicrob. Resist. 2021, 3, dlab008. Available online: https://pubmed.ncbi.nlm.nih.gov/34223086/ (accessed on 16 March 2022). [CrossRef]
- Sneddon, J.; Afriyie, D.; Sefah, I.; Cockburn, A.; Kerr, F.; Byrne-Davis, L.; Cameron, E. Developing a Sustainable Antimicrobial Stewardship, (AMS) Programme in Ghana: Replicating the Scottish Triad Model of Information, Education and Quality Improvement. Antibiotics 2020, 9, 636. [Google Scholar] [CrossRef]
- Doodoo, C.C.; Orman, E.; Alalbila, T.; Mensah, A.; Jato, J.; Mfoafo, K.A.; Folitse, I.; Hutton-Nyameaye, A.; Okon Ben, I.; Mensah-Kane, P.; et al. Antimicrobial Prescription Pattern in Ho Teaching Hospital, Ghana: Seasonal Determination Using a Point Prevalence Survey. Antibiotics 2021, 10, 199. [Google Scholar] [CrossRef]
- Valeix, S.F. One Health Integration: A Proposed Framework for a Study on Veterinarians and Zoonotic Disease Management in Ghana. Front. Vet. Sci. 2018, 5, 85. Available online: https://pubmed.ncbi.nlm.nih.gov/29770324/ (accessed on 17 March 2022). [CrossRef] [Green Version]
- FAO. FAO Builds Capacities of Poultry Farmers on Behavior Change in Antimicrobial Use in Ghana. 3 April 2021. Available online: http://www.fao.org/ghana/news/detail-events/en/c/1392699/ (accessed on 17 March 2022).
- Republic of Ghana. Ministry of Health. Policy, Planning, Monitoring & Evaluation (Website): Units. Available online: https://www.moh.gov.gh/policy-planning-monitoring-evaluation/ (accessed on 1 May 2022).
- WCO (WHO Ghana Country Office). Ghana Annual Report 2019, Accra . 2020. Available online: https://www.afro.who.int/sites/default/files/2020-10/Ghana%20Annual%20report%202019.pdf (accessed on 17 March 2022).
- Republic of Ghana. MoH. News and Events (7 November 2018). Ministry of Health Launches GhiLMIS to Improve Supply Chain in the Health Sector. Available online: https://www.moh.gov.gh/ministry-of-health-launches-ghilmis-to-improve-supply-chain-in-the-health-sector/ (accessed on 17 March 2022).
- GhILMIS Video. The Ghana Integrated Logistics Management Information System Launch (7 July 2021). Available online: https://www.youtube.com/watch?v=tZCp3h2wKZQ (accessed on 17 March 2022).
- Republic of Ghana. MoH, Ghana Health Commodity Supply Chain Master Plan: Logistics Management Information System Assessment Report. 2018. Available online: https://www.moh.gov.gh/wp-content/uploads/2018/02/LMIS-ASSESSMENT-REPORT.pdf (accessed on 17 March 2022).
- Kintampo Health Research Center. Ghana Health Service. The Knowledge, Perceptions and Practices of Prescribers on Antibiotic Use and Resistance in the Brong Ahafo Region of Ghana. 2016. Available online: https://www.reactgroup.org/wp-content/uploads/2016/09/Annex-2-KAPP.pdf (accessed on 18 March 2022).
- WCO (WHO Ghana country office). Ghana Annual Report 2020, Accra 2020. 2020. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/WCO%20Annual%20Report%202020.pdf (accessed on 1 May 2022).
- Republic of Ghana. Long-Term National Development Plan of Ghana. Outline (2018–2057), Accra 2017. 2017. Available online: https://s3-us-west-2.amazonaws.com/new-ndpc-static1/CACHES/PUBLICATIONS/2017/10/24/OUTLINE+-+LONG-TERM++PLAN.pdf (accessed on 17 March 2022).
- Republic of Ghana. Ministry of Health. Medium Term Expenditure Framework (Mtef) For 2018—2021. 2018. Available online: https://mofep.gov.gh/sites/default/files/pbb-estimates/2018/2018-PBB-MoH.pdf (accessed on 18 March 2022).
- Republic of Ghana, Ministry of Health. National Health Policy: Ensuring Healthy Lives for All. Revised Edition January 2020. 2020. Available online: https://www.moh.gov.gh/wp-ontent/uploads/2020/07/NHP_12.07.2020.pdf-13072020-FINAL.pdf (accessed on 18 March 2022).
- Republic of Ghana. The Coordinated Programme of Economic and Social Development Policies (2017–2024). Available online: https://s3-us-west-2.amazonaws.com/new-ndpc-static1/CACHES/PUBLICATIONS/2018/04/11/Coordinate+Programme-Final+(November+11,+2017)+cover.pdf (accessed on 18 March 2022).
- WHO, Stronger Collaboration, Better Health. Global Action Plan for Healthy Lives and Well-Being for All. 2021. Available online: https://www.who.int/initiatives/sdg3-global-action-plan (accessed on 18 March 2022).
- WHO Africa. Ghana Advances towards Developing a National Action Plan for Health Security. 6 July 2018. Available online: https://www.afro.who.int/news/ghana-advances-towards-developing-national-action-plan-health-security (accessed on 18 March 2022).
- Hera. Right to Health and Development. Review of The Global Health Preparedness Programme (GHPP), Reet (Belgium). December 2019. Available online: https://www.hera.eu/site/assets/files/215990/200113_final_report_ghpp_reviewed.pdf (accessed on 18 March 2022).
- Wernli, D.; Jørgensen, P.S.; Harbarth, S.; Carroll, S.P.; Laxminarayan, R.; Levrat, N.; Røttingen, J.A.; Pittet, D. Antimicrobial re-sistance: The complex challenge of measurement to inform policy and the public. PLoS Med. 2017, 14, e1002378. [Google Scholar] [CrossRef] [PubMed]
- Jimah, T.; Ogunseitan, O. National Action Plan on Antimicrobial Resistance: Stakeholder analysis of implementation in Ghana. J. Glob. Health Rep. 2020, 4, e2020067. [Google Scholar] [CrossRef]
- Orubu, E.S.; Zaman, M.H.; Rahman, M.T.; Wirtz, V.J. Veterinary antimicrobial resistance containment in Bangladesh: Evaluating the national action plan and scoping the evidence on implementation. J. Glob. Antimicrob. Resist. 2020, 21, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Jean Bosco Ndihokubwayo, J.B.; Yahaya, A.A.; Desta, A.T.; Georges Ki-Zerbo, G.; Asamoah-Odei, E.; Keita, B.; Pana, A.P.; Nkhoma, W. Antimicrobial resistance in the African Region: Issues, challenges and actions proposed. Afr. Health Monit. March 2013, 16, 27–30. [Google Scholar]
- Sommanustweechai, A.; Tangcharoensathien, V.; Malathum, K.; Sumpradit, N.; Kiatying-Angsulee, N.; Janejai, N.; Jaroenpoj, S. Implementing national strategies on antimicrobial resistance in Thailand: Potential challenges and solutions. Public Health 2018, 157, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Durrance-Bagale, A.; Mateus, A.; Sultana, Z.; Hasan, R.; Hanefeld, J. What are the barriers to implementing nation-al antimicrobial resistance action plans? A novel mixed-methods policy analysis in Pakistan. Health Policy Plan. 2020, 35, 973–982. [Google Scholar] [CrossRef]
- Johnson, S.; Bugyei, K.; Nortey, P.; Tasiame, W. Antimicrobial drug usage and poultry production: Case study in Ghana. Animal Production Science, published December 2017. 2017. Available online: https://www.publish.csiro.au/an/AN16832 (accessed on 16 March 2022).
- Republic of Ghana. The Budget Statement and Economic Policy of the Government of Ghana for the 2020 Financial Year. 2020. Available online: https://www.mofep.gov.gh/sites/default/files/budget-statements/2020-Budget-Statement-and-Economic-Policy_v3.pdf (accessed on 16 March 2022).




{kind=link}
{kind=link}
{kind=link}
| Goal One | Goal Two | Goal Three | Goal Four | Goal Five | |
|---|---|---|---|---|---|
| Strategic Objective | Improve awareness and understanding of antimicrobial resistance through effective communication, education and training. | Strengthen knowledge and evidence base through surveillance and research. | Reduce the incidence of infection through effective sanitation, hygiene and infection prevention measures and good agricultural and biosecurity practices. | Optimise the use of antimicrobial agents in humans, aquaculture, plant production and animal health in the “One Health” approach. | Develop the economic case and create an enabling environment for sustainable investment that takes into account Ghana’s needs, and increase investment in new machines, diagnostic tools, vaccines and other interventions. |
| Outcome Statement | Awareness and knowledge of AMR is improved. | Evidence-based knowledge to reduce the burden of AMR increased. | Occurrence of infections in establishments reduced. | Use of antimicrobials in animal and human health optimized. | Enhance the enabling environment for sustainable investment of AMR reduction. |
| No. of Expert | Institution(s) | Sector(s) |
|---|---|---|
| R1 | Kwame Nkrumah University of Science and Technology; National Platform on Antimicrobial Resistance | Research and academia |
| R2 | AMR Secretariat; Ghana Health Service | Health |
| R3 | Komfo Anokye Teaching Hospital; National Platform on Antimicrobial Resistance | Health |
| R4 | Food Agriculture Organization | International agency |
| R5 | Council for Scientific and Industrial Research, Water Research Institute | Research and academia |
| R6 | Ministry of Health | Health |
| R7 | Hope for Future Generations; member of various Civil Society Organisations (CSOs) | Non-governmental organisation |
| R8 | Antibiotic Drug use, Monitoring and Evaluation of Resistance in Ghana (ADMER); Danish International Development Agency (DANIDA) | International agency |
| R9 | World Health Organisation Country Office Ghana; Ministry of Health; Ghana National Drug Information and Resource Centre | International agency/ Health |
| R10 | Environmental Protection Agency | Environment |
| R11 | University of Ghana; National Platform on Antimicrobial Resistance; Antibiotic Drug use, Monitoring and Evaluation of Resistance in Ghana (ADMER) | Research and academia/ International agency |
| R12 | IMANI Centre for Policy and Education | Non-governmental organisation |
| R13 | Ministry of Food and Agriculture | Agriculture and veterinary |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hein, W.; Aglanu, L.M.; Mensah-Sekyere, M.; Harant, A.; Brinkel, J.; Lamshöft, M.; Lorenz, E.; Eibach, D.; Amuasi, J. Fighting Antimicrobial Resistance: Development and Implementation of the Ghanaian National Action Plan (2017–2021). Antibiotics 2022, 11, 613. https://doi.org/10.3390/antibiotics11050613
Hein W, Aglanu LM, Mensah-Sekyere M, Harant A, Brinkel J, Lamshöft M, Lorenz E, Eibach D, Amuasi J. Fighting Antimicrobial Resistance: Development and Implementation of the Ghanaian National Action Plan (2017–2021). Antibiotics. 2022; 11(5):613. https://doi.org/10.3390/antibiotics11050613
Chicago/Turabian StyleHein, Wolfgang, Leslie Mawuli Aglanu, MacDonnel Mensah-Sekyere, Anne Harant, Johanna Brinkel, Maike Lamshöft, Eva Lorenz, Daniel Eibach, and John Amuasi. 2022. "Fighting Antimicrobial Resistance: Development and Implementation of the Ghanaian National Action Plan (2017–2021)" Antibiotics 11, no. 5: 613. https://doi.org/10.3390/antibiotics11050613