
Antibiotic Therapy for Difficult-to-Treat Infections in Lung Transplant Recipients: A Practical Approach

Abstract
:1. Introduction
2. MDR/XDR Pseudomonas aeruginosa Infection
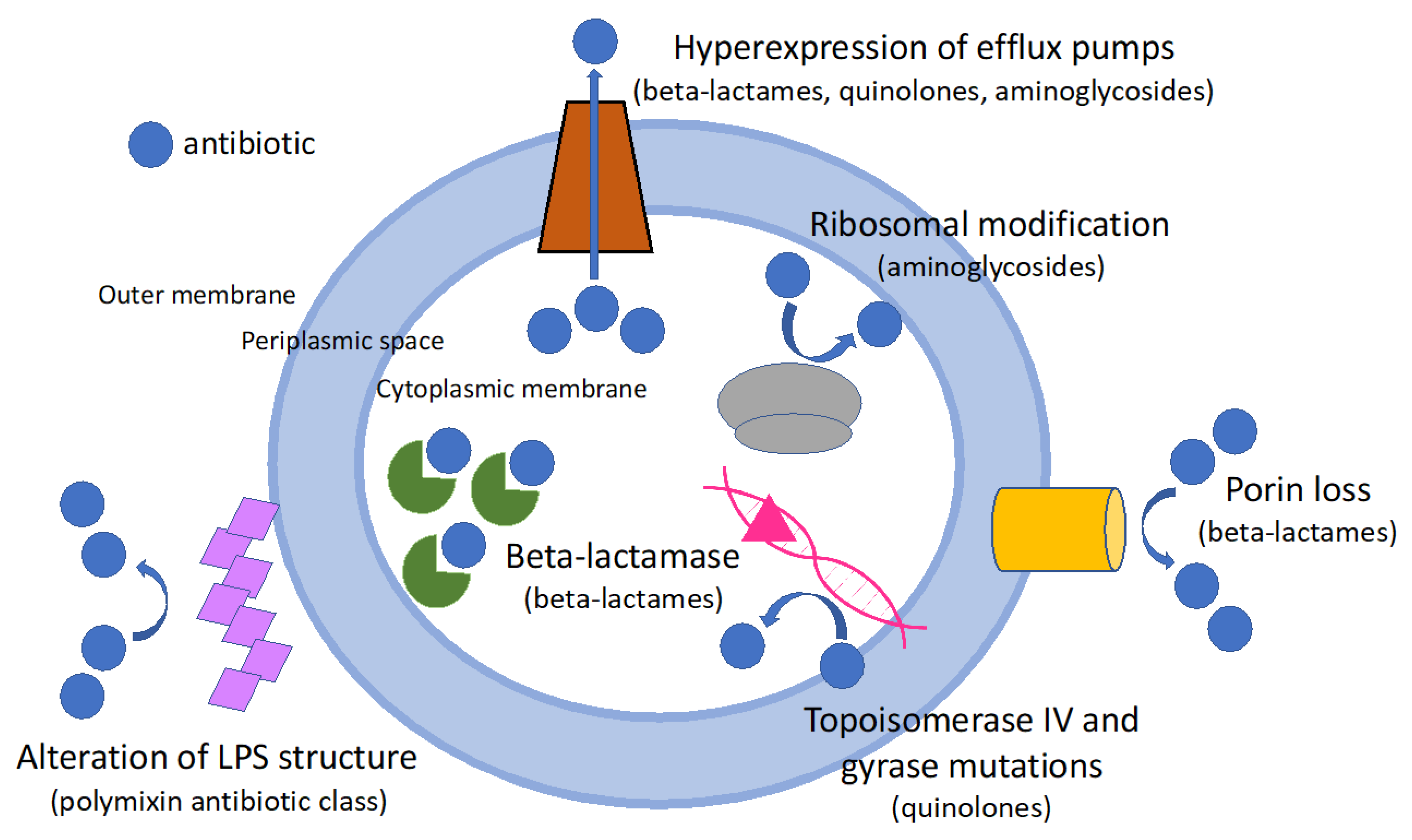
2.1. Mechanism of Resistance in Pseudomonas aeruginosa
2.2. Respiratory Tract Colonization by P. aeruginosa in Lung Transplant Recipients: To Eradicate or Not?
2.3. Antibiotic Therapy for MDR/XDR P. aeruginosa Infection
3. Burkholderia cepacia Complex (BCC) Infection
3.1. Antibiotic Therapy for Burkholderia cepacia Complex (BCC) Infection
3.2. Other Therapeutic Approaches
4. Mycobacterum abscessus Complex (MABc) Infection
4.1. Microbiology and Resistance Mechanism
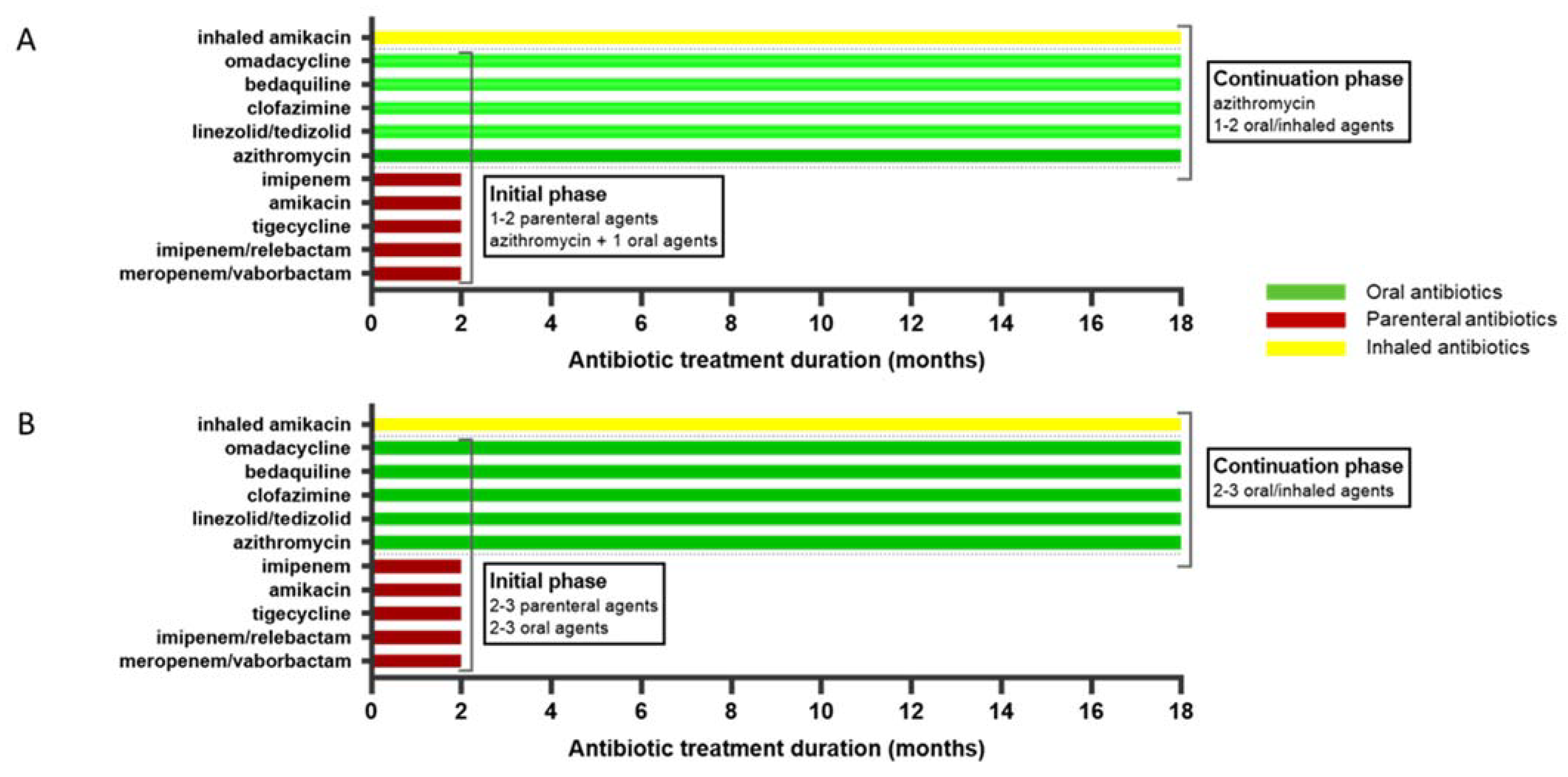
4.2. Antibiotic Therapy for MABc Infection in Lung Transplant Recipients
4.3. Other Treatments
5. Nocardiosis
Therapeutic Management
6. Expert Opinion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- McCort, M.; MacKenzie, E.; Pursell, K.; Pitrak, D. Bacterial infections in lung transplantation. J. Thorac. Dis. 2021, 13, 6654–6672. [Google Scholar] [CrossRef] [PubMed]
- Nykanen, A.; Raivio, P.; Perakyla, L.; Stark, C.; Huuskonen, A.; Lemstrom, K.; Halme, M.; Hammainen, P. Incidence and impact of chronic lung allograft dysfunction after lung transplantation—Single-center 14-year experience. Scand. Cardiovasc. J. 2020, 54, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial resistance surveillance in Europe. 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/ECDC-WHO-AMR-report.pdf (accessed on 28 March 2022).
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguado, J.M.; Silva, J.T.; Fernandez-Ruiz, M.; Cordero, E.; Fortun, J.; Gudiol, C.; Martinez-Martinez, L.; Vidal, E.; Almenar, L.; Almirante, B.; et al. Management of multidrug resistant Gram-negative bacilli infections in solid organ transplant recipients: SET/GESITRA-SEIMC/REIPI recommendations. Transplant. Rev. 2018, 32, 36–57. [Google Scholar] [CrossRef] [Green Version]
- Camargo, L.F.; Marra, A.R.; Pignatari, A.C.; Sukiennik, T.; Behar, P.P.; Medeiros, E.A.; Ribeiro, J.; Girao, E.; Correa, L.; Guerra, C.; et al. Nosocomial bloodstream infections in a nationwide study: Comparison between solid organ transplant patients and the general population. Transpl. Infect. Dis. 2015, 17, 308–313. [Google Scholar] [CrossRef]
- Johnson, L.E.; D’Agata, E.M.; Paterson, D.L.; Clarke, L.; Qureshi, Z.A.; Potoski, B.A.; Peleg, A.Y. Pseudomonas aeruginosa bacteremia over a 10-year period: Multidrug resistance and outcomes in transplant recipients. Transpl. Infect. Dis. 2009, 11, 227–234. [Google Scholar] [CrossRef]
- Bodro, M.; Sabe, N.; Tubau, F.; Llado, L.; Baliellas, C.; Gonzalez-Costello, J.; Cruzado, J.M.; Carratala, J. Extensively drug-resistant Pseudomonas aeruginosa bacteremia in solid organ transplant recipients. Transplantation 2015, 99, 616–622. [Google Scholar] [CrossRef]
- Holm, A.E.; Schultz, H.H.L.; Johansen, H.K.; Pressler, T.; Lund, T.K.; Iversen, M.; Perch, M. Bacterial Re-Colonization Occurs Early after Lung Transplantation in Cystic Fibrosis Patients. J. Clin. Med. 2021, 10, 1275. [Google Scholar] [CrossRef]
- Karakonstantis, S.; Kritsotakis, E.I.; Gikas, A. Treatment options for K. pneumoniae, P. aeruginosa and A. baumannii co-resistant to carbapenems, aminoglycosides, polymyxins and tigecycline: An approach based on the mechanisms of resistance to carbapenems. Infection 2020, 48, 835–851. [Google Scholar] [CrossRef]
- Horcajada, J.P.; Montero, M.; Oliver, A.; Sorli, L.; Luque, S.; Gomez-Zorrilla, S.; Benito, N.; Grau, S. Epidemiology and Treatment of Multidrug-Resistant and Extensively Drug-Resistant Pseudomonas aeruginosa Infections. Clin. Microbiol. Rev. 2019, 32, e00031-19. [Google Scholar] [CrossRef]
- Nordmann, P.; Poirel, L. Epidemiology and Diagnostics of Carbapenem Resistance in Gram-negative Bacteria. Clin. Infect. Dis. 2019, 69 (Suppl. S7), S521–S528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottlieb, J.; Mattner, F.; Weissbrodt, H.; Dierich, M.; Fuehner, T.; Strueber, M.; Simon, A.; Welte, T. Impact of graft colonization with gram-negative bacteria after lung transplantation on the development of bronchiolitis obliterans syndrome in recipients with cystic fibrosis. Respir. Med. 2009, 103, 743–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verleden, S.E.; Ruttens, D.; Vandermeulen, E.; Vaneylen, A.; Dupont, L.J.; Van Raemdonck, D.E.; Verleden, G.M.; Vanaudenaerde, B.M.; Vos, R. Bronchiolitis obliterans syndrome and restrictive allograft syndrome: Do risk factors differ? Transplantation 2013, 95, 1167–1172. [Google Scholar] [CrossRef] [PubMed]
- Vos, R.; Vanaudenaerde, B.M.; Geudens, N.; Dupont, L.J.; Van Raemdonck, D.E.; Verleden, G.M. Pseudomonal airway colonisation: Risk factor for bronchiolitis obliterans syndrome after lung transplantation? Eur. Respir. J. 2008, 31, 1037–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botha, P.; Archer, L.; Anderson, R.L.; Lordan, J.; Dark, J.H.; Corris, P.A.; Gould, K.; Fisher, A.J. Pseudomonas aeruginosa colonization of the allograft after lung transplantation and the risk of bronchiolitis obliterans syndrome. Transplantation 2008, 85, 771–774. [Google Scholar] [CrossRef]
- Smith, S.; Rowbotham, N.J.; Regan, K.H. Inhaled anti-pseudomonal antibiotics for long-term therapy in cystic fibrosis. Cochrane Database Syst. Rev. 2018, 3, CD001021. [Google Scholar] [CrossRef]
- Langton Hewer, S.C.; Smyth, A.R. Antibiotic strategies for eradicating Pseudomonas aeruginosa in people with cystic fibrosis. Cochrane Database Syst. Rev. 2017, 4, CD004197. [Google Scholar] [CrossRef]
- Mogayzel, P.J., Jr.; Naureckas, E.T.; Robinson, K.A.; Brady, C.; Guill, M.; Lahiri, T.; Lubsch, L.; Matsui, J.; Oermann, C.M.; Ratjen, F.; et al. Cystic Fibrosis Foundation pulmonary guideline. pharmacologic approaches to prevention and eradication of initial Pseudomonas aeruginosa infection. Ann. Am. Thorac. Soc. 2014, 11, 1640–1650. [Google Scholar] [CrossRef]
- Varannai, O.; Gede, N.; Juhasz, M.F.; Szakacs, Z.; Dembrovszky, F.; Nemeth, D.; Hegyi, P.; Parniczky, A. Therapeutic Approach of Chronic Pseudomonas Infection in Cystic Fibrosis-A Network Meta-Analysis. Antibiotics 2021, 10, 936. [Google Scholar] [CrossRef]
- Taccetti, G.; Bianchini, E.; Cariani, L.; Buzzetti, R.; Costantini, D.; Trevisan, F.; Zavataro, L.; Campana, S.; on behalf of the Italian Group for P aeruginosa eradication in cystic fibrosis. Early antibiotic treatment for Pseudomonas aeruginosa eradication in patients with cystic fibrosis: A randomised multicentre study comparing two different protocols. Thorax 2012, 67, 853–859. [Google Scholar] [CrossRef] [Green Version]
- De Muynck, B.; Van Herck, A.; Sacreas, A.; Heigl, T.; Kaes, J.; Vanstapel, A.; Verleden, S.E.; Neyrinck, A.P.; Ceulemans, L.J.; Van Raemdonck, D.E.; et al. Successful Pseudomonas aeruginosa eradication improves outcomes after lung transplantation: A retrospective cohort analysis. Eur. Respir. J. 2020, 56, 2001720. [Google Scholar] [CrossRef] [PubMed]
- Hirama, T.; Tomiyama, F.; Notsuda, H.; Watanabe, T.; Watanabe, Y.; Oishi, H.; Okada, Y. Outcome and prognostic factors after lung transplantation for bronchiectasis other than cystic fibrosis. BMC Pulm. Med. 2021, 21, 261. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.A.; Pilewski, J.M.; Venkataramanan, R.; Robinson, K.M.; Morrell, M.R.; Wisniewski, S.R.; Zeevi, A.; McDyer, J.F.; Ensor, C.R. Effect of aerosolized antipseudomonals on Pseudomonas positivity and bronchiolitis obliterans syndrome after lung transplantation. Transpl. Infect. Dis. 2017, 19, e12688. [Google Scholar] [CrossRef] [PubMed]
- Suhling, H.; Rademacher, J.; Greer, M.; Haverich, A.; Warnecke, G.; Gottlieb, J.; Welte, T. Inhaled colistin following lung transplantation in colonised cystic fibrosis patients. Eur. Respir. J. 2013, 42, 542–544. [Google Scholar] [CrossRef] [Green Version]
- Tamma, P.D.; Cosgrove, S.E.; Maragakis, L.L. Combination therapy for treatment of infections with gram-negative bacteria. Clin. Microbiol. Rev. 2012, 25, 450–470. [Google Scholar] [CrossRef] [Green Version]
- Pouch, S.M.; Patel, G.; on behalf of the AST Infectious Diseases Community of Practice. Multidrug-resistant Gram-negative bacterial infections in solid organ transplant recipients-Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13594. [Google Scholar] [CrossRef]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of Extended-Spectrum beta-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 2021, 72, 1109–1116. [Google Scholar] [CrossRef]
- Paul, M.; Carrara, E.; Retamar, P.; Tangden, T.; Bitterman, R.; Bonomo, R.A.; de Waele, J.; Daikos, G.L.; Akova, M.; Harbarth, S.; et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). Clin. Microbiol. Infect. 2022, 28, 521–547. [Google Scholar] [CrossRef]
- Pogue, J.M.; Kaye, K.S.; Veve, M.P.; Patel, T.S.; Gerlach, A.T.; Davis, S.L.; Puzniak, L.A.; File, T.M.; Olson, S.; Dhar, S.; et al. Ceftolozane/Tazobactam vs. Polymyxin or Aminoglycoside-based Regimens for the Treatment of Drug-resistant Pseudomonas aeruginosa. Clin. Infect. Dis. 2020, 71, 304–310. [Google Scholar] [CrossRef]
- Hart, D.E.; Gallagher, J.C.; Puzniak, L.A.; Hirsch, E.B.; C/T Alliance to deliver Real-world Evidence (CARE). A Multicenter Evaluation of Ceftolozane/Tazobactam Treatment Outcomes in Immunocompromised Patients With Multidrug-Resistant Pseudomonas aeruginosa Infections. Open Forum. Infect. Dis. 2021, 8, ofab089. [Google Scholar] [CrossRef]
- Young, K.; Painter, R.E.; Raghoobar, S.L.; Hairston, N.N.; Racine, F.; Wisniewski, D.; Balibar, C.J.; Villafania, A.; Zhang, R.; Sahm, D.F.; et al. In Vitro studies evaluating the activity of imipenem in combination with relebactam against Pseudomonas aeruginosa. BMC Microbiol. 2019, 19, 150. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Viaggi, B.; Rossolini, G.M.; Pea, F.; Viale, P. An Evidence-Based Multidisciplinary Approach Focused on Creating Algorithms for Targeted Therapy of Infection-Related Ventilator-Associated Complications (IVACs) Caused by Pseudomonas aeruginosa and Acinetobacter baumannii in Critically Ill Adult Patients. Antibiotics 2021, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, T.; Niki, Y.; Paterson, D.L.; et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): A randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet. Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef]
- Papp-Wallace, K.M.; Zeiser, E.T.; Becka, S.A.; Park, S.; Wilson, B.M.; Winkler, M.L.; D’Souza, R.; Singh, I.; Sutton, G.; Fouts, D.E.; et al. Ceftazidime-Avibactam in Combination With Fosfomycin: A Novel Therapeutic Strategy against Multidrug-Resistant Pseudomonas aeruginosa. J. Infect. Dis. 2019, 220, 666–676. [Google Scholar] [CrossRef] [Green Version]
- Carugati, M.; Piazza, A.; Peri, A.M.; Cariani, L.; Brilli, M.; Girelli, D.; Di Carlo, D.; Gramegna, A.; Pappalettera, M.; Comandatore, F.; et al. Fatal respiratory infection due to ST308 VIM-1-producing Pseudomonas aeruginosa in a lung transplant recipient: Case report and review of the literature. BMC Infect. Dis. 2020, 20, 635. [Google Scholar] [CrossRef] [PubMed]
- Pollini, S.; Maradei, S.; Pecile, P.; Olivo, G.; Luzzaro, F.; Docquier, J.D.; Rossolini, G.M. FIM-1, a new acquired metallo-beta-lactamase from a Pseudomonas aeruginosa clinical isolate from Italy. Antimicrob. Agents Chemother. 2013, 57, 410–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunz Coyne, A.J.; El Ghali, A.; Holger, D.; Rebold, N.; Rybak, M.J. Therapeutic Strategies for Emerging Multidrug-Resistant Pseudomonas aeruginosa. Infect. Dis. Ther. 2022, 11, 661–682. [Google Scholar] [CrossRef]
- Lee, M.; Abbey, T.; Biagi, M.; Wenzler, E. Activity of aztreonam in combination with ceftazidime-avibactam against serine- and metallo-beta-lactamase-producing Pseudomonas aeruginosa. Diagn. Microbiol. Infect. Dis. 2021, 99, 115227. [Google Scholar] [CrossRef]
- Zhu, Y.; Monsel, A.; Roberts, J.A.; Pontikis, K.; Mimoz, O.; Rello, J.; Qu, J.; Rouby, J.J.; on behalf of the European Investigator Network for Nebulized Antibiotics in Ventilator-Associated Pneumonia (ENAVAP). Nebulized Colistin in Ventilator-Associated Pneumonia and Tracheobronchitis: Historical Background, Pharmacokinetics and Perspectives. Microorganisms 2021, 9, 1154. [Google Scholar] [CrossRef]
- Valachis, A.; Samonis, G.; Kofteridis, D.P. The role of aerosolized colistin in the treatment of ventilator-associated pneumonia: A systematic review and metaanalysis. Crit. Care Med. 2015, 43, 527–533. [Google Scholar] [CrossRef]
- Liu, D.; Zhang, J.; Liu, H.X.; Zhu, Y.G.; Qu, J.M. Intravenous combined with aerosolised polymyxin versus intravenous polymyxin alone in the treatment of pneumonia caused by multidrug-resistant pathogens: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2015, 46, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Vardakas, K.Z.; Mavroudis, A.D.; Georgiou, M.; Falagas, M.E. Intravenous plus inhaled versus intravenous colistin monotherapy for lower respiratory tract infections: A systematic review and meta-analysis. J. Infect. 2018, 76, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Lipuma, J.J. Update on the Burkholderia cepacia complex. Curr. Opin. Pulm. Med. 2005, 11, 528–533. [Google Scholar] [CrossRef] [PubMed]
- De Soyza, A.; Meachery, G.; Hester, K.L.; Nicholson, A.; Parry, G.; Tocewicz, K.; Pillay, T.; Clark, S.; Lordan, J.L.; Schueler, S.; et al. Lung transplantation for patients with cystic fibrosis and Burkholderia cepacia complex infection: A single-center experience. J. Heart Lung Transplant. 2010, 29, 1395–1404. [Google Scholar] [CrossRef]
- Murray, S.; Charbeneau, J.; Marshall, B.C.; LiPuma, J.J. Impact of Burkholderia infection on lung transplantation in cystic fibrosis. Am. J. Respir. Crit. Care Med. 2008, 178, 363–371. [Google Scholar] [CrossRef] [Green Version]
- De Soyza, A.; McDowell, A.; Archer, L.; Dark, J.H.; Elborn, S.J.; Mahenthiralingam, E.; Gould, K.; Corris, P.A. Burkholderia cepacia complex genomovars and pulmonary transplantation outcomes in patients with cystic fibrosis. Lancet 2001, 358, 1780–1781. [Google Scholar] [CrossRef]
- Aris, R.M.; Routh, J.C.; LiPuma, J.J.; Heath, D.G.; Gilligan, P.H. Lung transplantation for cystic fibrosis patients with Burkholderia cepacia complex. Survival linked to genomovar type. Am. J. Respir. Crit. Care Med. 2001, 164, 2102–2106. [Google Scholar] [CrossRef]
- Wang, R.; Welsh, S.K.; Budev, M.; Goldberg, H.; Noone, P.G.; Gray, A.; Zaas, D.; Boyer, D. Survival after lung transplantation of cystic fibrosis patients infected with Burkholderia dolosa (genomovar VI). Clin. Transplant. 2018, 32, e13236. [Google Scholar] [CrossRef]
- Mitchell, A.B.; Glanville, A.R. The Impact of Resistant Bacterial Pathogens including Pseudomonas aeruginosa and Burkholderia on Lung Transplant Outcomes. Semin. Respir. Crit. Care Med. 2021, 42, 436–448. [Google Scholar] [CrossRef]
- Koutsokera, A.; Varughese, R.A.; Sykes, J.; Orchanian-Cheff, A.; Shah, P.S.; Chaparro, C.; Tullis, E.; Singer, L.G.; Stephenson, A.L. Pre-transplant factors associated with mortality after lung transplantation in cystic fibrosis: A systematic review and meta-analysis. J. Cyst. Fibros. 2019, 18, 407–415. [Google Scholar] [CrossRef]
- Papp-Wallace, K.M.; Becka, S.A.; Zeiser, E.T.; Ohuchi, N.; Mojica, M.F.; Gatta, J.A.; Falleni, M.; Tosi, D.; Borghi, E.; Winkler, M.L.; et al. Overcoming an Extremely Drug Resistant (XDR) Pathogen: Avibactam Restores Susceptibility to Ceftazidime for Burkholderia cepacia Complex Isolates from Cystic Fibrosis Patients. ACS Infect. Dis. 2017, 3, 502–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Duin, D.; van Delden, C.; the AST Infectious Diseases Community of Practice. Multidrug-resistant gram-negative bacteria infections in solid organ transplantation. Am. J. Transplant. 2013, 13 (Suppl. S4), 31–41. [Google Scholar] [CrossRef] [PubMed]
- Dacco, V.; Claut, L.; Piconi, S.; Castellazzi, L.; Garbarino, F.; Teri, A.; Colombo, C. Successful ceftazidime-avibactam treatment of post-surgery Burkholderia multivorans genomovar II bacteremia and brain abscesses in a young lung transplanted woman with cystic fibrosis. Transpl. Infect. Dis. 2019, 21, e13082. [Google Scholar] [CrossRef]
- Barlow, G.; Morice, A. Successful treatment of resistant Burkholderia multivorans infection in a patient with cystic fibrosis using ceftazidime/avibactam plus aztreonam. J. Antimicrob. Chemother. 2018, 73, 2270–2271. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Fan, Y.; Bergman, Y.; Sick-Samuels, A.C.; Hsu, A.J.; Timp, W.; Simner, P.J.; Prokesch, B.C.; Greenberg, D.E. Successful Treatment of Persistent Burkholderia cepacia Complex Bacteremia with Ceftazidime-Avibactam. Antimicrob. Agents Chemother. 2018, 62, e02213-17. [Google Scholar] [CrossRef] [Green Version]
- Zeiser, E.T.; Becka, S.A.; Wilson, B.M.; Barnes, M.D.; LiPuma, J.J.; Papp-Wallace, K.M. “Switching Partners”: Piperacillin-Avibactam Is a Highly Potent Combination against Multidrug-Resistant Burkholderia cepacia Complex and Burkholderia gladioli Cystic Fibrosis Isolates. J. Clin. Microbiol. 2019, 57, e00181-19. [Google Scholar] [CrossRef] [Green Version]
- Becka, S.A.; Zeiser, E.T.; LiPuma, J.J.; Papp-Wallace, K.M. Activity of Imipenem-Relebactam against Multidrug- and Extensively Drug-Resistant Burkholderia cepacia Complex and Burkholderia gladioli. Antimicrob. Agents Chemother. 2021, 65, e0133221. [Google Scholar] [CrossRef]
- Karlowsky, J.A.; Hackel, M.A.; Tsuji, M.; Yamano, Y.; Echols, R.; Sahm, D.F. In Vitro Activity of Cefiderocol, a Siderophore Cephalosporin, Against Gram-Negative Bacilli Isolated by Clinical Laboratories in North America and Europe in 2015–2016: SIDERO-WT-2015. Int. J. Antimicrob. Agents 2019, 53, 456–466. [Google Scholar] [CrossRef]
- Zeiser, E.T.; Becka, S.A.; Barnes, M.D.; Taracila, M.A.; LiPuma, J.J.; Papp-Wallace, K.M. Resurrecting Old beta-Lactams: Potent Inhibitory Activity of Temocillin against Multidrug-Resistant Burkholderia Species Isolates from the United States. Antimicrob. Agents Chemother. 2019, 6, e02315-18. [Google Scholar] [CrossRef] [Green Version]
- Zeriouh, M.; Sabashnikov, A.; Patil, N.P.; Schmack, B.; Zych, B.; Mohite, P.N.; Garcia Saez, D.; Koch, A.; Mansur, A.; Soresi, S.; et al. Use of taurolidine in lung transplantation for cystic fibrosis and impact on bacterial colonization. Eur. J. Cardiothorac. Surg. 2018, 53, 603–609. [Google Scholar] [CrossRef]
- Ledson, M.J.; Gallagher, M.J.; Robinson, M.; Cowperthwaite, C.; Williets, T.; Hart, C.A.; Walshaw, M.J. A randomized double-blinded placebo-controlled crossover trial of nebulized taurolidine in adult cystic fibrosis patients infected with Burkholderia cepacia. J. Aerosol. Med. 2002, 15, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Roux, A.L.; Catherinot, E.; Ripoll, F.; Soismier, N.; Macheras, E.; Ravilly, S.; Bellis, G.; Vibet, M.A.; Le Roux, E.; Lemonnier, L.; et al. Multicenter study of prevalence of nontuberculous mycobacteria in patients with cystic fibrosis in france. J. Clin. Microbiol. 2009, 47, 4124–4128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strnad, L.; Winthrop, K.L. Treatment of Mycobacterium abscessus Complex. Semin. Respir. Crit. Care Med. 2018, 39, 362–376. [Google Scholar] [CrossRef] [PubMed]
- Zelazny, A.M.; Root, J.M.; Shea, Y.R.; Colombo, R.E.; Shamputa, I.C.; Stock, F.; Conlan, S.; McNulty, S.; Brown-Elliott, B.A.; Wallace, R.J., Jr.; et al. Cohort study of molecular identification and typing of Mycobacterium abscessus, Mycobacterium massiliense, and Mycobacterium bolletii. J. Clin. Microbiol. 2009, 47, 1985–1995. [Google Scholar] [CrossRef] [Green Version]
- Koh, W.J.; Jeon, K.; Lee, N.Y.; Kim, B.J.; Kook, Y.H.; Lee, S.H.; Park, Y.K.; Kim, C.K.; Shin, S.J.; Huitt, G.A.; et al. Clinical significance of differentiation of Mycobacterium massiliense from Mycobacterium abscessus. Am. J. Respir. Crit. Care Med. 2011, 183, 405–410. [Google Scholar] [CrossRef]
- Harada, T.; Akiyama, Y.; Kurashima, A.; Nagai, H.; Tsuyuguchi, K.; Fujii, T.; Yano, S.; Shigeto, E.; Kuraoka, T.; Kajiki, A.; et al. Clinical and microbiological differences between Mycobacterium abscessus and Mycobacterium massiliense lung diseases. J. Clin. Microbiol. 2012, 50, 3556–3561. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Cho, J.; Lee, C.H.; Han, S.K.; Yim, J.J. Progression and Treatment Outcomes of Lung Disease Caused by Mycobacterium abscessus and Mycobacterium massiliense. Clin. Infect. Dis. 2017, 64, 301–308. [Google Scholar] [CrossRef]
- Kavaliunaite, E.; Harris, K.A.; Aurora, P.; Dixon, G.; Shingadia, D.; Muthialu, N.; Spencer, H. Outcome according to subspecies following lung transplantation in cystic fibrosis pediatric patients infected with Mycobacterium abscessus. Transpl. Infect. Dis. 2020, 22, e13274. [Google Scholar] [CrossRef]
- Qvist, T.; Pressler, T.; Thomsen, V.O.; Skov, M.; Iversen, M.; Katzenstein, T.L. Nontuberculous mycobacterial disease is not a contraindication to lung transplantation in patients with cystic fibrosis: A retrospective analysis in a Danish patient population. Transplant. Proc. 2013, 45, 342–345. [Google Scholar] [CrossRef]
- Lobo, L.J.; Chang, L.C.; Esther, C.R., Jr.; Gilligan, P.H.; Tulu, Z.; Noone, P.G. Lung transplant outcomes in cystic fibrosis patients with pre-operative Mycobacterium abscessus respiratory infections. Clin. Transplant. 2013, 27, 523–529. [Google Scholar] [CrossRef]
- Tissot, A.; Thomas, M.F.; Corris, P.A.; Brodlie, M. NonTuberculous Mycobacteria infection and lung transplantation in cystic fibrosis: A worldwide survey of clinical practice. BMC Pulm. Med. 2018, 18, 86. [Google Scholar] [CrossRef] [Green Version]
- Hamad, Y.; Pilewski, J.M.; Morrell, M.; D’Cunha, J.; Kwak, E.J. Outcomes in Lung Transplant Recipients With Mycobacterium abscessus Infection: A 15-Year Experience From a Large Tertiary Care Center. Transplant. Proc. 2019, 51, 2035–2042. [Google Scholar] [CrossRef] [PubMed]
- Daley, C.L.; Iaccarino, J.M.; Lange, C.; Cambau, E.; Wallace, R.J., Jr.; Andrejak, C.; Bottger, E.C.; Brozek, J.; Griffith, D.E.; Guglielmetti, L.; et al. Treatment of Nontuberculous Mycobacterial Pulmonary Disease: An Official ATS/ERS/ESCMID/IDSA Clinical Practice Guideline. Clin. Infect. Dis. 2020, 71, e1–e36. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, A.; Ammerman, N.C.; Lee, J.; Martins, O.; Kreiswirth, B.N.; Lamichhane, G.; Parrish, N.M.; Nuermberger, E.L. In Vitro Activity of the New beta-Lactamase Inhibitors Relebactam and Vaborbactam in Combination with beta-Lactams against Mycobacterium abscessus Complex Clinical Isolates. Antimicrob. Agents Chemother. 2019, 63, e02623-18. [Google Scholar] [CrossRef] [Green Version]
- Poon, Y.K.; La Hoz, R.M.; Hynan, L.S.; Sanders, J.; Monogue, M.L. Tedizolid vs. Linezolid for the Treatment of Nontuberculous Mycobacteria Infections in Solid Organ Transplant Recipients. Open Forum. Infect. Dis. 2021, 8, ofab093. [Google Scholar] [CrossRef] [PubMed]
- Morrisette, T.; Alosaimy, S.; Philley, J.V.; Wadle, C.; Howard, C.; Webb, A.J.; Veve, M.P.; Barger, M.L.; Bouchard, J.; Gore, T.W.; et al. Preliminary, Real-world, Multicenter Experience with Omadacycline for Mycobacterium abscessus Infections. Open Forum. Infect. Dis. 2021, 8, ofab002. [Google Scholar] [CrossRef] [PubMed]
- Olivier, K.N.; Griffith, D.E.; Eagle, G.; McGinnis, J.P., 2nd; Micioni, L.; Liu, K.; Daley, C.L.; Winthrop, K.L.; Ruoss, S.; Addrizzo-Harris, D.J.; et al. Randomized Trial of Liposomal Amikacin for Inhalation in Nontuberculous Mycobacterial Lung Disease. Am. J. Respir. Crit. Care Med. 2017, 195, 814–823. [Google Scholar] [CrossRef]
- Jeon, K.; Kwon, O.J.; Lee, N.Y.; Kim, B.J.; Kook, Y.H.; Lee, S.H.; Park, Y.K.; Kim, C.K.; Koh, W.J. Antibiotic treatment of Mycobacterium abscessus lung disease: A retrospective analysis of 65 patients. Am. J. Respir. Crit. Care Med. 2009, 180, 896–902. [Google Scholar] [CrossRef]
- Uyttebroek, S.; Chen, B.; Onsea, J.; Ruythooren, F.; Debaveye, Y.; Devolder, D.; Spriet, I.; Depypere, M.; Wagemans, J.; Lavigne, R.; et al. Safety and efficacy of phage therapy in difficult-to-treat infections: A systematic review. Lancet. Infect. Dis. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Dedrick, R.M.; Guerrero-Bustamante, C.A.; Garlena, R.A.; Russell, D.A.; Ford, K.; Harris, K.; Gilmour, K.C.; Soothill, J.; Jacobs-Sera, D.; Schooley, R.T.; et al. Engineered bacteriophages for treatment of a patient with a disseminated drug-resistant Mycobacterium abscessus. Nat. Med. 2019, 25, 730–733. [Google Scholar] [CrossRef]
- Coussement, J.; Lebeaux, D.; van Delden, C.; Guillot, H.; Freund, R.; Marbus, S.; Melica, G.; Van Wijngaerden, E.; Douvry, B.; Van Laecke, S.; et al. Nocardia Infection in Solid Organ Transplant Recipients: A Multicenter European Case-control Study. Clin. Infect. Dis. 2016, 63, 338–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebeaux, D.; Coussement, J.; Bodilsen, J.; Tattevin, P. Management dilemmas in Nocardia brain infection. Curr. Opin. Infect. Dis. 2021, 34, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Margalit, I.; Lebeaux, D.; Tishler, O.; Goldberg, E.; Bishara, J.; Yahav, D.; Coussement, J. How do I manage nocardiosis? Clin. Microbiol. Infect. 2021, 27, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, A.; Clark, N.M.; Infectious Diseases Community of Practice of the American Society of Transplantation. Nocardia infections in solid organ transplantation: Guidelines from the Infectious Diseases Community of Practice of the American Society of Transplantation. Clin. Transplant. 2019, 33, e13509. [Google Scholar] [CrossRef] [PubMed]
- Davidson, N.; Grigg, M.J.; McGuinness, S.L.; Baird, R.J.; Anstey, N.M. Safety and Outcomes of Linezolid Use for Nocardiosis. Open Forum. Infect. Dis. 2020, 7, ofaa090. [Google Scholar] [CrossRef]
- Peleg, A.Y.; Husain, S.; Qureshi, Z.A.; Silveira, F.P.; Sarumi, M.; Shutt, K.A.; Kwak, E.J.; Paterson, D.L. Risk factors, clinical characteristics, and outcome of Nocardia infection in organ transplant recipients: A matched case-control study. Clin. Infect. Dis. 2007, 44, 1307–1314. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| First-Line Treatment | Other Options | |
|---|---|---|
| ESBL P. aeruginosa | Meropenem 1–2 g q8h (3 h-infusion) | Ceftolozane/tazobactam 1.5 g q8h (for infection other than pneumonia); 3 g q8h (for pneumonia) Ceftazidime/avibactam 2.5 g q8h Imipenem/relebactam 1 g q6h |
| DTR P. aeruginosa (not MBL-producer) | Ceftolozane/tazobactam 3 g q8h (3 h-infusion) Ceftazidime/avibactam 2.5 g/qh (3 h-infusion) Imipenem/relebactam 1.25 g q6h (30 min-infusion) | Cefiderocol 2 g q8h (3 h-infusion) |
| DTR P. aeruginosa (not MBL-producer; resistant to ceftolozane/tazobactam) | Ceftazidime/avibactam 2.5 g q8h (3 h-infusion) | Cefiderocol 2 g q8h (3 h-infusion) Ceftazidime/avibactam 2.5 g q8h (3 h-infusion) + Fosfomycin 12–24 g per day |
| DTR P. aeruginosa (MBL-producer) * | Cefiderocol 2 g q8h (3 h-infusion) Colistin 9 × 106 IU per day Cefiderocol 2 g q8h (3 h-infusion) + inhaled colistin 0.5–2 × 106 q12h | Ceftazidime/avibactam 2.5 g q8h + aztreonam 2 g q8h (3 h-infusion) Colistin + fosfomycin + aminoglycoside Bacteriophage therapy |
| First-Line Treatment | Alternative Treatment | |
|---|---|---|
| BCC |
|
|
| MDR BCC * |
|
|
| MDR BCC resistant to ceftazidime/avibactam * |
|
|
| Localization | Empiric Induction Treatment *,± | Maintenance Oral Therapy ± | Duration |
|---|---|---|---|
| Primary skin Pulmonary stable | TMP/SMX orally Linezolid orally | TMP/SMXM inocycline Amoxicillin/clavulanate | 6–12 months |
| Pulmonary moderate/severe | TMP/SMX iv + imipenem OR amikacin TMP/SMX iv + ceftriaxone ± linezolid Linezolid+ ceftriaxone OR imipenem | TMP/SMX Minocycline Amoxicillin/clavulanate | 6–12 months |
| CNS involvement | TMP/SMX iv + imipenem ± amikacin TMP/SMX iv + imipenem + linezolid Linezolid + imipenem Imipenem + amikacin | TMP/SMX | 9–12 months |
| Disseminated (>two organs without CNS involvement) | TMP/SMX iv + imipenem OR amikacin TMP/SMX iv + linezolid + imipenem OR amikacin Imipenem + amikacin | TMP/SMX Minocycline Amoxicillin/clavulanate | 6–12 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van den Bogaart, L.; Manuel, O. Antibiotic Therapy for Difficult-to-Treat Infections in Lung Transplant Recipients: A Practical Approach. Antibiotics 2022, 11, 612. https://doi.org/10.3390/antibiotics11050612
van den Bogaart L, Manuel O. Antibiotic Therapy for Difficult-to-Treat Infections in Lung Transplant Recipients: A Practical Approach. Antibiotics. 2022; 11(5):612. https://doi.org/10.3390/antibiotics11050612
Chicago/Turabian Stylevan den Bogaart, Lorena, and Oriol Manuel. 2022. "Antibiotic Therapy for Difficult-to-Treat Infections in Lung Transplant Recipients: A Practical Approach" Antibiotics 11, no. 5: 612. https://doi.org/10.3390/antibiotics11050612