Wearable Movement Exploration Device with Machine Learning Algorithm for Screening and Tracking Diabetic Neuropathy—A Cross-Sectional, Diagnostic, Comparative Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Description
2.2. Description of Reference and Investigational Methods
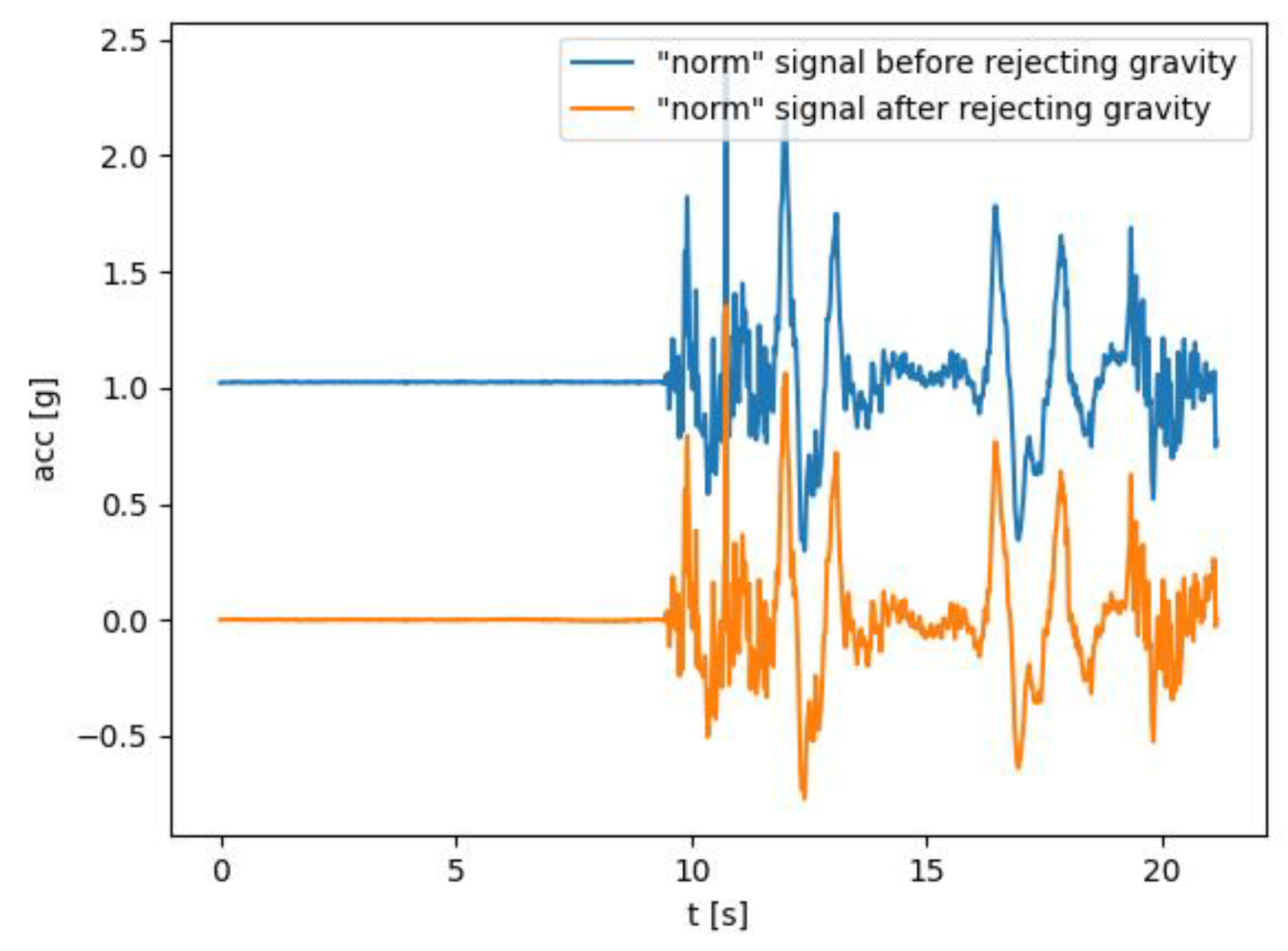
2.3. Raw Signal Processing and Features Extraction
- PSD5Hz
- PSD10Hz
- PSD15Hz
2.4. Statistical Methodology
3. Results
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Geiss, L.S.; Wang, J.; Cheng, Y.J.; Thompson, T.J.; Barker, L.; Li, Y.; Albright, A.L.; Gregg, E.W. Prevalence and Incidence Trends for Diagnosed Diabetes among Adults Aged 20 to 79 Years, United States, 1980–2012. JAMA 2014, 312, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- Menke, A.; Casagrande, S.; Geiss, L.; Cowie, C.C. Prevalence of and Trends in Diabetes among Adults in the United States, 1988–2012. JAMA 2015, 314, 1021–1029. [Google Scholar] [CrossRef]
- Read, S.H.; Kerssens, J.J.; McAllister, D.A.; Colhoun, H.M.; Fischbacher, C.M.; Lindsay, R.S.; McCrimmon, R.J.; McKnight, J.A.; Petrie, J.R.; Sattar, N.; et al. Trends in Type 2 Diabetes Incidence and Mortality in Scotland between 2004 and 2013. Diabetologia 2016, 59, 2106–2113. [Google Scholar] [CrossRef]
- Manuwald, U.; Schoffer, O.; Kugler, J.; Riemenschneider, H.; Kapellen, T.M.; Kiess, W.; Rothe, U. Trends in Incidence and Prevalence of Type 1 Diabetes between 1999 and 2019 Based on the Childhood Diabetes Registry of Saxony, Germany. PLoS ONE 2021, 16, e0262171. [Google Scholar] [CrossRef]
- Magliano, D.J.; Islam, R.M.; Barr, E.L.M.; Gregg, E.W.; Pavkov, M.E.; Harding, J.L.; Tabesh, M.; Koye, D.N.; Shaw, J.E. Trends in Incidence of Total or Type 2 Diabetes: Systematic Review. BMJ 2019, 366, l5003. [Google Scholar] [CrossRef]
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2011, 34 (Suppl. S1), S62–S69. [Google Scholar] [CrossRef]
- Faselis, C.; Katsimardou, A.; Imprialos, K.; Deligkaris, P.; Kallistratos, M.; Dimitriadis, K. Microvascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, B.C.; Gallagher, G.; Fridman, V.; Feldman, E.L. Diabetic Neuropathy: What Does the Future Hold? Diabetologia 2020, 63, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Feldman, E.L.; Callaghan, B.C.; Pop-Busui, R.; Zochodne, D.W.; Wright, D.E.; Bennett, D.L.; Bril, V.; Russell, J.W.; Viswanathan, V. Diabetic Neuropathy. Nat. Rev. Dis. Primers 2019, 5, 42. [Google Scholar] [CrossRef]
- Vinik, A.I.; Nevoret, M.-L.; Casellini, C.; Parson, H. Diabetic Neuropathy. Endocrinol. Metab. Clin. N. Am. 2013, 42, 747–787. [Google Scholar] [CrossRef]
- Hicks, C.W.; Selvin, E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr. Diabetes Rep. 2019, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.; Frank, B.; Marshall, A.; Khalil, R.S.; Ponirakis, G.; Petropoulos, I.N.; Cuthbertson, D.J.; Malik, R.A.; Alam, U. Early Detection of Diabetic Peripheral Neuropathy: A Focus on Small Nerve Fibres. Diagnostics 2021, 11, 165. [Google Scholar] [CrossRef] [PubMed]
- Calcutt, N.A. Diabetic Neuropathy and Neuropathic Pain: A (Con)Fusion of Pathogenic Mechanisms? Pain 2020, 161, S65–S86. [Google Scholar] [CrossRef] [PubMed]
- Røikjer, J.; Mørch, C.D.; Ejskjaer, N. Diabetic Peripheral Neuropathy: Diagnosis and Treatment. Curr. Drug Saf. 2021, 16, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, J.; Fadavi, H.; Ishibashi, F.; Shore, A.C.; Tavakoli, M. Advances in Screening, Early Diagnosis and Accurate Staging of Diabetic Neuropathy. Front. Endocrinol. 2021, 12, 671257. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J.; Fernando, M.; Lazzarini, P.; Najafi, B.; Armstrong, D.G. The Potential Role of Sensors, Wearables and Telehealth in the Remote Management of Diabetes-Related Foot Disease. Sensors 2020, 20, 4527. [Google Scholar] [CrossRef]
- Welch, P.D. The Use of Fast Fourier Transform for the Estimation of Power Spectra: A Method Based on Time Aver. Aging Over Short, Modified Periodograms. IEEE Trans. Audio Electroacoust. 1976, 15, 70–73. [Google Scholar] [CrossRef]
- Pozi, M.S.M.; Mohd, H.O. A Kernel Density Estimation Method to Generate Synthetic Shifted Datasets in Privacy-Preserving Task. J. Internet Serv. Inf. Secur. 2020, 10, 70–89. [Google Scholar]
- Majumder, S.; Mondal, T.; Deen, M.J. Wearable Sensors for Remote Health Monitoring. Sensors 2017, 17, 130. [Google Scholar] [CrossRef]
- Yu, Y. Gold Standard for Diagnosis of DPN. Front. Endocrinol. 2021, 12, 719356. [Google Scholar] [CrossRef]
- Talha, M.; Kyrarini, M.; Buriro, E.A. A Survey of the Diagnosis of Peripheral Neuropathy Using Intelligent and Wearable Systems. Technologies 2023, 11, 163. [Google Scholar] [CrossRef]
- Brognara, L.; Mazzotti, A.; Di Martino, A.; Faldini, C.; Cauli, O. Wearable Sensor for Assessing Gait and Postural Alterations in Patients with Diabetes: A Scoping Review. Medicina 2021, 57, 1145. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Zhou, H.; Varghese, V.; Najafi, B. Characteristics of the Gait Initiation Phase in Older Adults with Diabetic Peripheral Neuropathy Compared to Control Older Adults. Clin. Biomech. 2020, 72, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Yang, J.; Najafi, B. Does the Presence of Cognitive Impairment Exacerbate the Risk of Falls in People with Peripheral Neuropathy? An Application of Body-Worn Inertial Sensors to Measure Gait Variability. Sensors 2020, 20, 1328. [Google Scholar] [CrossRef] [PubMed]
- Esser, P.; Collett, J.; Maynard, K.; Steins, D.; Hillier, A.; Buckingham, J.; Tan, G.D.; King, L.; Dawes, H. Single Sensor Gait Analysis to Detect Diabetic Peripheral Neuropathy: A Proof of Principle Study. Diabetes Metab. J. 2018, 42, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.S.; Mulavara, A.P.; Peters, B.T.; Sangi-Haghpeykar, H.; Kung, D.H.; Mosier, D.R.; Bloomberg, J.J. Sharpening the Tandem Walking Test for Screening Peripheral Neuropathy. South. Med. J. 2013, 106, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Sempere-Bigorra, M.; Brognara, L.; Julian-Rochina, I.; Mazzotti, A.; Cauli, O. Relationship between Deep and Superficial Sensitivity Assessments and Gait Analysis in Diabetic Foot Patients. Int. Wound J. 2023, 20, 3023–3034. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Kang, L.; Lu, Y.; Wang, N.; Lu, Y.; Lo, B.; Yang, G.-Z. Discriminative Information Added by Wearable Sensors for Early Screening—A Case Study on Diabetic Peripheral Neuropathy. In Proceedings of the 2019 IEEE 16th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Chicago, IL, USA, 19–22 May 2019; pp. 1–4. [Google Scholar]
- Maranesi, E.; Di Nardo, F.; Rabini, R.A.; Ghetti, G.G.; Burattini, L.; Mercante, O.; Fioretti, S. Muscle Activation Patterns Related to Diabetic Neuropathy in Elderly Subjects: A Functional Reach Test Study. Clin. Biomech. 2016, 32, 236–240. [Google Scholar] [CrossRef]
- Kim, W.; Kim, Y. Human Body Model Using Multiple Depth Camera for Gait Analysis. In Proceedings of the 2018 19th IEEE/ACIS International Conference on Software Engineering Artificial Intelligence, Networking and Parallel/Distributed Computing (SNPD), Busan, Republic of Korea, 27–29 June 2018; pp. 70–75. [Google Scholar]
- Chikano, M.; Konno, T.; Awai, S. Robust Gait Recognition for Occlusion Caused by Surveillance Cameras. In Proceedings of the 2021 IEEE 10th Global Conference on Consumer Electronics (GCCE), Kyoto, Japan, 12–15 October 2021; pp. 148–149. [Google Scholar] [CrossRef]
- Ferreira, J.P.; Liu, T.; Coimbra, P.; Coimbra, P. Parameter Analysis and Selection for Human Gait Characterization Using a Low Cost Vision System. In Proceedings of the 2017 4th International Conference on Systems and Informatics (ICSAI), Hangzhou, China, 11–13 November 2017; pp. 198–203. [Google Scholar]
- Barthakur, M.; Hazarika, A.; Bhuyan, M. Rule Based Fuzzy Approach for Peripheral Motor Neuropathy (PMN) Diagnosis Based on NCS Data. In Proceedings of the International Conference on Recent Advances and Innovations in Engineering (ICRAIE-2014), Jaipur, India, 9–11 May 2014; pp. 1–9. [Google Scholar]
- Barriga, E.S.; Chekh, V.; Carranza, C.; Burge, M.R.; Edwards, A.; McGrew, E.; Zamora, G.; Soliz, P. Computational Basis for Risk Stratification of Peripheral Neuropathy from Thermal Imaging. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 1486–1489. [Google Scholar] [CrossRef]
- Agurto, C.; Chek, V.; Edwards, A.; Jarry, Z.; Barriga, S.; Simon, J.; Soliz, P. A Thermoregulation Model to Detect Diabetic Peripheral Neuropathy. In Proceedings of the 2016 IEEE Southwest Symposium on Image Analysis and Interpretation (SSIAI), Santa Fe, NM, USA, 6–8 March 2016; pp. 13–16. [Google Scholar] [CrossRef]
- Gallardo, E.; Noto, Y.-I.; Simon, N.G. Ultrasound in the Diagnosis of Peripheral Neuropathy: Structure Meets Function in the Neuromuscular Clinic. J. Neurol. Neurosurg. Psychiatry 2015, 86, 1066–1074. [Google Scholar] [CrossRef]
- Sawada, H.; Uchida, K.; Danjo, J.; Nakamura, Y. Development of a Non-Invasive Screening Device of Diabetic Peripheral Neuropathy Based on the Perception of Micro-Vibration. In Proceedings of the 2016 IEEE Conference on Computational Intelligence in Bioinformatics and Computational Biology (CIBCB), Chiang Mai, Thailand, 5–7 October 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Cao, Z.; Wang, F.; He, Y.; Zhang, Y.; Zhang, J. Analysis of Plantar Pressure in Elderly Diabetic Patients with Peripheral Neuropathy. In Proceedings of the 2021 International Conference on Public Health and Data Science (ICPHDS), Chengdu, China, 9–11 July 2021; pp. 184–187. [Google Scholar] [CrossRef]
- Corpin, R.R.A.; Guingab, H.A.R.; Manalo, A.N.P.; Sampana, M.L.B.; Abello, A.N.A.; dela Cruz, A.R.; Roxas, E.A.; Suarez, C.G.; Serrano, K.K.D. Prediction of Diabetic Peripheral Neuropathy (DPN) Using Plantar Pressure Analysis and Learning Models. In Proceedings of the 2019 IEEE 11th International Conference on Humanoid, Nanotechnology, Information Technology, Communication and Control, Environment, and Management (HNICEM), Laoag, Philippines, 29 November–1 December 2019; pp. 1–6. [Google Scholar]
- Wang, D.; Ouyang, J.; Zhou, P.; Yan, J.; Shu, L.; Xu, X. A Novel Low-Cost Wireless Footwear System for Monitoring Diabetic Foot Patients. IEEE Trans. Biomed. Circuits Syst. 2021, 15, 43–54. [Google Scholar] [CrossRef]
- Botros, F.S.; Taher, M.F.; ElSayed, N.M.; Fahmy, A.S. Prediction of Diabetic Foot Ulceration Using Spatial and Temporal Dynamic Plantar Pressure. In Proceedings of the 2016 8th Cairo International Biomedical Engineering Conference (CIBEC), Cairo, Egypt, 15–17 December 2016; pp. 43–47. [Google Scholar]
- Kukreja, G.S.; Alok, A.; Reddy, A.K.; Nersisson, R. IoT Based Foot Neuropathy Analysis and Remote Monitoring of Foot Pressure and Temperature. In Proceedings of the 2020 5th International Conference on Computing, Communication and Security (ICCCS), Patna, India, 14–16 October 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Silva, S.F.; Loureiro, C.F.M.; Almeida, H.; Otel, I.; Domingues, J.P.; Silva, J.S.; Quadrado, M.J.; Morgado, A.M. Evaluation of Corneal Nerves Morphology for Diabetic Peripheral Neuropathy Assessment. In Proceedings of the 2012 IEEE 2nd Portuguese Meeting in Bioengineering (ENBENG), Coimbra, Portugal, 23–25 February 2012; pp. 1–4. [Google Scholar]
- Lee, J.Y.; Lee, S.W.H. Telemedicine Cost-Effectiveness for Diabetes Management: A Systematic Review. Diabetes Technol. Ther. 2018, 20, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Miner, H.; Fatehi, A.; Ring, D.; Reichenberg, J.S. Clinician Telemedicine Perceptions during the COVID-19 Pandemic. Telemed. e-Health 2021, 27, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Pujara, S.; Sutton, S.; Rhee, M. Telemedicine in the Management of Type 1 Diabetes. Prev. Chronic Dis. 2018, 15, E13. [Google Scholar] [CrossRef] [PubMed]
- Sood, A.; Watts, S.A.; Johnson, J.K.; Hirth, S.; Aron, D.C. Telemedicine Consultation for Patients with Diabetes Mellitus: A Cluster Randomised Controlled Trial. J. Telemed. Telecare 2018, 24, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Haque, F.; Bin Ibne Reaz, M.; Chowdhury, M.E.H.; Srivastava, G.; Hamid Md Ali, S.; Bakar, A.A.A.; Bhuiyan, M.A.S. Performance Analysis of Conventional Machine Learning Algorithms for Diabetic Sensorimotor Polyneuropathy Severity Classification. Diagnostics 2021, 11, 801. [Google Scholar] [CrossRef] [PubMed]
- Baskozos, G.; Themistocleous, A.C.; Hebert, H.L.; Pascal, M.M.V.; John, J.; Callaghan, B.C.; Laycock, H.; Granovsky, Y.; Crombez, G.; Yarnitsky, D.; et al. Classification of Painful or Painless Diabetic Peripheral Neuropathy and Identification of the Most Powerful Predictors Using Machine Learning Models in Large Cross-Sectional Cohorts. BMC Med. Inform. Decis. Mak. 2022, 22, 144. [Google Scholar] [CrossRef]
- Haque, F.; Reaz, M.B.I.; Chowdhury, M.E.H.; Ezeddin, M.; Kiranyaz, S.; Alhatou, M.; Ali, S.H.M.; Bakar, A.A.A.; Srivastava, G. Machine Learning-Based Diabetic Neuropathy and Previous Foot Ulceration Patients Detection Using Electromyography and Ground Reaction Forces during Gait. Sensors 2022, 22, 3507. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DM Neuropathy | p Value | |||
|---|---|---|---|---|
| No (n = 15) | Yes (n = 8) | |||
| Legs | Heel–toe walk | |||
| Feature 1 | 0.011 ± 0.005 | 0.005 ± 0.003 | 0.013 | |
| Feature 2 | 1.481 ± 0.369 | 1.402 ± 0.334 | 0.620 | |
| Feature 3 | 1.459 ± 0.300 | 1.418 ± 0.363 | 0.778 | |
| Feature 4 | 0.107 ± 0.048 | 0.056 ± 0.031 | 0.014 | |
| Tandem walk | ||||
| Feature 5 | 1.481 ± 0.206 | 1.327 ± 0.135 | 0.072 | |
| Feature 6 | 1.307 ± 0.094 | 1.230 ± 0.138 | 0.126 | |
| Heel–knee | ||||
| Feature 7 | 0.036 ± 0.029 | 0.012 ± 0.009 | 0.008 | |
| Feature 8 | 0.068 ± 0.104 | 0.021 ± 0.014 | 0.107 | |
| Feature 9 | 0.052 ± 0.072 | 0.034 ± 0.059 | 0.557 | |
| Feature 10 | 0.695 ± 0.304 | 0.442 ± 0.173 | 0.042 | |
| Arms | Romberg test | |||
| Feature 11 × 103 | 0.164 ± 0.131 | 0.339 ± 0.265 | 0.044 | |
| Feature 12 × 105 | 0.109 ± 0.156 | 0.298 ± 0.282 | 0.050 | |
| Feature 13 | 0.628 ± 0.140 | 0.542 ± 0.169 | 0.206 | |
| Feature 14 | 0.604 ± 0.173 | 0.505 ± 0.190 | 0.218 | |
| Postural tremor | ||||
| Feature 15 | 0.017 ± 0.011 | 0.011 ± 0.012 | 0.236 | |
| Feature 16 | 0.020 ± 0.013 | 0.013 ± 0.008 | 0.184 | |
| Feature 17 | 1.044 ± 0.487 | 0.707 ± 0.244 | 0.082 | |
| Feature 18 | 1.281 ± 0.788 | 0.839 ± 0.370 | 0.151 | |
| Feature 19 | 0.638 ± 0.154 | 0.569 ± 0.159 | 0.326 | |
| Feature 20 | 0.597 ± 0.172 | 0.564 ± 0.164 | 0.664 | |
| Finger–nose test | ||||
| Feature 21 | 1.006 ± 0.025 | 0.960 ± 0.062 | 0.018 | |
| Feature 22 | 0.003 ± 0.012 | −0.021 ± 0.033 | 0.017 | |
| Feature 23 | 0.598 ± 0.195 | 0.548 ± 0.156 | 0.537 | |
| Feature 24 | 0.606 ± 0.202 | 0.616 ± 0.218 | 0.911 | |
| DMN | Feat. 1 | Feat. 4 | Feat. 5 | Feat. 6 | Feat. 7 | Feat. 10 | Feat. 11 | Feat. 12 | Feat. 16 | Feat. 17 | Feat. 21 | Feat. 22 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Motor | |||||||||||||
| Arm | |||||||||||||
| Amp LM ra | −0.109 | 0.255 | 0.268 | 0.147 | 0.160 | 0.379 | 0.185 | 0.264 | 0.255 | ||||
| Lat LM pr | 0.591 | −0.235 | −0.181 | −0.120 | 0.652 | 0.387 | −0.214 | −0.372 | −0.329 | −0.141 | |||
| CV LM pr | −0.872 | 0.650 | 0.596 | 0.593 | 0.443 | −0.200 | −0.199 | 0.329 | 0.182 | 0.426 | 0.437 | 0.526 | 0.413 |
| Lat LU ra | 0.213 | −0.202 | −0.259 | −0.280 | −0.187 | 0.171 | 0.245 | −0.168 | 0.131 | ||||
| AMP LU ra | −0.139 | 0.240 | 0.312 | −0.205 | 0.457 | 0.261 | 0.217 | 0.341 | 0.288 | −0.111 | |||
| Lat LU pr | 0.336 | 0.261 | 0.143 | 0.263 | 0.161 | 0.149 | 0.182 | 0.256 | 0.408 | ||||
| Amp LU pr | −0.128 | 0.243 | 0.277 | −0.136 | 0.375 | 0.359 | 0.332 | 0.332 | 0.302 | ||||
| CV LU pr | −0.363 | −0.444 | −0.496 | −0.171 | −0.174 | −0.167 | −0.221 | ||||||
| Leg | |||||||||||||
| Lat RT sa | 0.584 | −0.162 | −0.155 | −0.335 | −0.344 | 0.417 | 0.458 | −0.119 | −0.189 | ||||
| Amp RT sa | −0.489 | 0.291 | 0.429 | 0.309 | 0.160 | −0.650 | −0.337 | 0.335 | 0.167 | 0.165 | 0.144 | 0.247 | 0.448 |
| Lat LT sa | 0.456 | −0.104 | −0.395 | −0.227 | 0.116 | 0.484 | 0.505 | 0.281 | 0.296 | ||||
| Amp LT sa | −0.233 | 0.101 | 0.184 | −0.506 | 0.143 | 0.161 | 0.128 | 0.116 | |||||
| Lat RP se | 0.260 | −0.145 | 0.508 | 0.254 | 0.199 | −0.201 | −0.140 | ||||||
| Amp RP se | −0.430 | 0.515 | 0.283 | 0.211 | 0.250 | −0.692 | −0.479 | −0.193 | 0.373 | 0.339 | 0.496 | 0.193 | |
| Lat RP ps | 0.303 | 0.120 | 0.149 | −0.127 | 0.350 | 0.236 | 0.285 | 0.202 | |||||
| Amp RP ps | −0.434 | 0.466 | 0.194 | 0.245 | 0.345 | −0.663 | −0.503 | −0.132 | 0.396 | 0.359 | 0.477 | 0.166 | |
| CV RP ps | −0.465 | 0.190 | 0.214 | 0.333 | 0.212 | −0.577 | −0.436 | 0.173 | 0.250 | ||||
| Lat LP se | 0.281 | 0.115 | 0.145 | 0.152 | 0.323 | 0.219 | 0.127 | ||||||
| Amp LP se | −0.292 | 0.505 | 0.287 | 0.327 | 0.357 | −0.643 | −0.227 | 0.362 | 0.330 | 0.716 | 0.448 | ||
| Lat LP ps | 0.371 | 0.622 | 0.300 | 0.200 | |||||||||
| Amp LP ps | −0.348 | 0.536 | 0.351 | 0.292 | 0.341 | −0.640 | −0.282 | 0.402 | 0.380 | 0.704 | 0.493 | ||
| CV LP ps | −0.490 | 0.149 | 0.112 | −0.657 | −0.283 | 0.203 | 0.154 | 0.255 | |||||
| Sensory | |||||||||||||
| Arm | |||||||||||||
| Lat LM rp | 0.499 | −0.339 | −0.435 | −0.233 | −0.171 | 0.722 | 0.282 | −0.144 | −0.583 | −0.544 | −0.352 | −0.131 | |
| Amp LM rp | −0.351 | 0.445 | 0.432 | 0.331 | 0.281 | −0.589 | −0.260 | −0.139 | 0.402 | 0.388 | 0.451 | 0.546 | |
| CV LM rp | −0.559 | 0.345 | 0.454 | 0.201 | 0.176 | −0.658 | −0.345 | 0.124 | 0.179 | 0.429 | 0.405 | 0.421 | 0.273 |
| Lat LU rp | 0.314 | −0.216 | −0.145 | 0.351 | −0.125 | −0.115 | |||||||
| Amp LU rp | −0.413 | 0.418 | 0.474 | 0.411 | −0.498 | −0.157 | −0.105 | 0.294 | 0.283 | 0.391 | 0.402 | ||
| CV LU rp | −0.374 | 0.140 | 0.228 | −0.402 | −0.139 | 0.293 | 0.261 | 0.298 | 0.247 | ||||
| Leg | |||||||||||||
| Lat RS ps | 0.506 | −0.230 | −0.222 | −0.174 | 0.380 | 0.458 | 0.208 | −0.411 | −0.412 | ||||
| Amp RS ps | −0.539 | 0.391 | 0.332 | 0.515 | 0.194 | −0.344 | −0.353 | 0.209 | 0.278 | 0.285 | 0.341 | 0.528 | |
| CV RS ps | −0.674 | 0.320 | 0.353 | 0.226 | −0.446 | −0.596 | 0.197 | 0.126 | 0.312 | 0.311 | 0.264 | 0.148 | |
| Lat LS ps | 0.693 | −0.300 | −0.475 | −0.133 | 0.113 | 0.335 | 0.253 | −0.248 | −0.116 | −0.188 | −0.168 | −0.168 | |
| Amp LS ps | −0.694 | 0.285 | 0.432 | 0.243 | −0.455 | −0.497 | 0.252 | 0.289 | 0.237 | 0.236 | 0.193 | 0.436 | |
| CV LS ps | −0.731 | 0.400 | 0.500 | 0.218 | −0.400 | −0.468 | 0.297 | 0.210 | 0.217 | 0.212 | 0.265 | 0.215 |
| Precision | Recall | f1-Score | Supprt | |
|---|---|---|---|---|
| SVM-no DN | 0.759259 | 0.872340 | 0.811881 | 47.0 |
| SVM-DN | 0.884615 | 0.779661 | 0.828829 | 59.0 |
| Logistic Regression-no DN | 0.592593 | 0.761905 | 0.666667 | 42.0 |
| Logistic Regression-DN | 0.807692 | 0.656250 | 0.724138 | 64.0 |
| Decision Tree-no DN | 0.629630 | 0.809524 | 0.708333 | 42.0 |
| Decision Tree-DN | 0.846154 | 0.687500 | 0.758621 | 64.0 |
| Examination | p Value a | ||
|---|---|---|---|
| EMNG | Moveo | ||
| Unpleasant | |||
| No | 1 (4.3%) | 21 (91.3%) | <0.001 |
| Mild | 7 (30.4%) | 1 (4.3%) | |
| Moderate | 11 (47.8%) | 1 (4.3%) | |
| Severe | 4 (17.4%) | 0 | |
| Pain | |||
| No | 0 | 22 (95.7%) | <0.001 |
| Mild | 8 (34.8%) | 1 (4.3%) | |
| Moderate | 11 (47.8%) | 0 | |
| Severe | 4 (17.4%) | 0 | |
| Fear | |||
| No | 10 (43.5%) | 22 (95.7%) | <0.001 |
| Mild | 5 (21.7%) | 1 (4.3%) | |
| Moderate | 5 (21.7%) | 0 | |
| Severe | 3 (13.0%) | 0 | |
| Duration | |||
| As it should be | 5 (21.7%) | 22 (95.7%) | <0.001 |
| Little longer | 12 (52.2%) | 1 (4.3%) | |
| Much longer | 6 (26.1%) | 0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radunovic, G.; Velickovic, Z.; Pavlov-Dolijanovic, S.; Janjic, S.; Stojic, B.; Jeftovic Velkova, I.; Suljagic, N.; Soldatovic, I. Wearable Movement Exploration Device with Machine Learning Algorithm for Screening and Tracking Diabetic Neuropathy—A Cross-Sectional, Diagnostic, Comparative Study. Biosensors 2024, 14, 166. https://doi.org/10.3390/bios14040166
Radunovic G, Velickovic Z, Pavlov-Dolijanovic S, Janjic S, Stojic B, Jeftovic Velkova I, Suljagic N, Soldatovic I. Wearable Movement Exploration Device with Machine Learning Algorithm for Screening and Tracking Diabetic Neuropathy—A Cross-Sectional, Diagnostic, Comparative Study. Biosensors. 2024; 14(4):166. https://doi.org/10.3390/bios14040166
Chicago/Turabian StyleRadunovic, Goran, Zoran Velickovic, Slavica Pavlov-Dolijanovic, Sasa Janjic, Biljana Stojic, Irena Jeftovic Velkova, Nikola Suljagic, and Ivan Soldatovic. 2024. "Wearable Movement Exploration Device with Machine Learning Algorithm for Screening and Tracking Diabetic Neuropathy—A Cross-Sectional, Diagnostic, Comparative Study" Biosensors 14, no. 4: 166. https://doi.org/10.3390/bios14040166