High-Accuracy Renal Cell Carcinoma Discrimination through Label-Free SERS of Blood Serum and Multivariate Analysis

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Synthesis of the Substrate
2.2. Analyte Deposition and SERS Measurements
2.3. Research Ethics
2.4. Cohort of Patient Samples
2.5. Blood Serum Collection
2.6. Multivariate Analysis
3. Results and Discussion
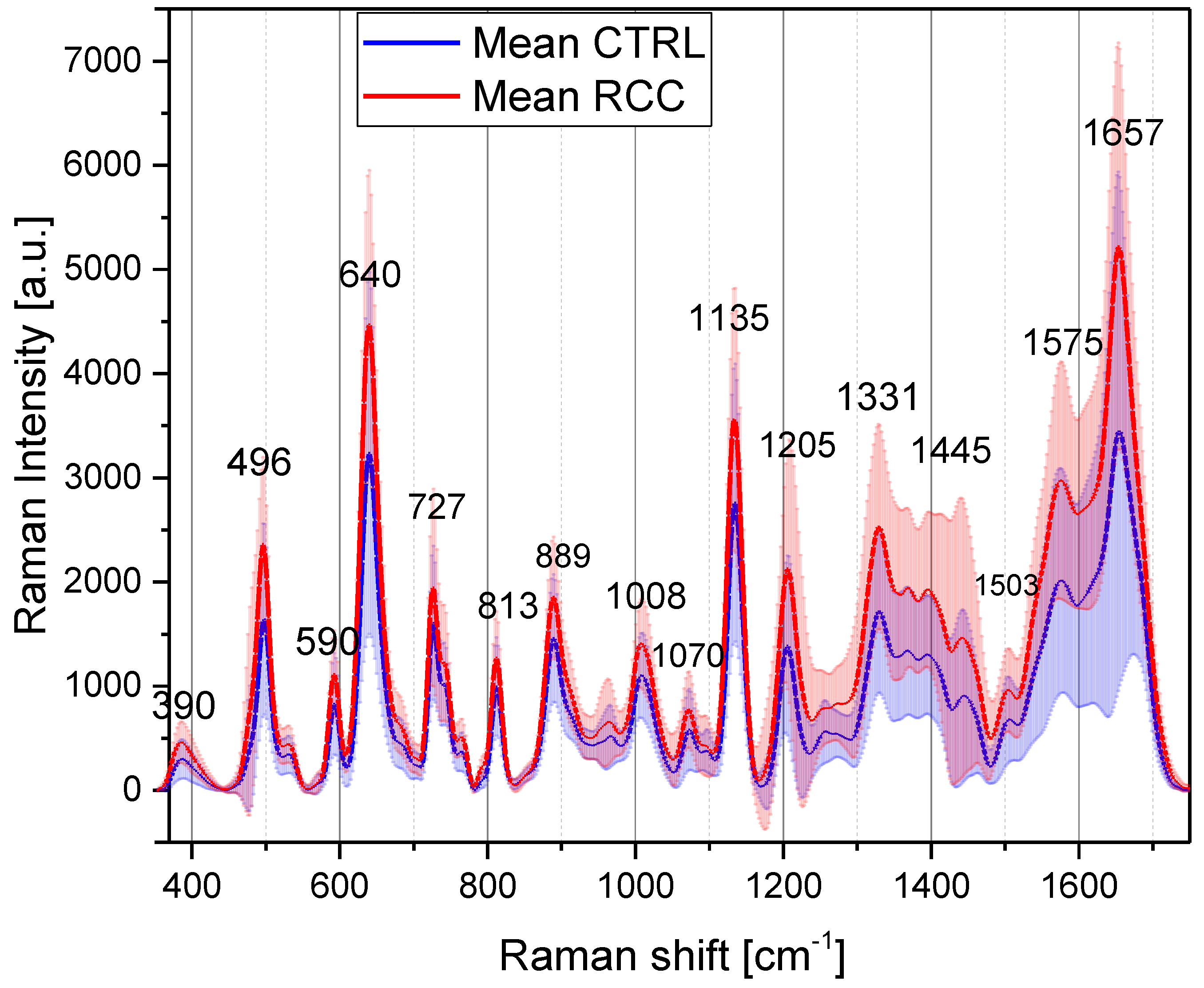
3.1. SERS of Blood Serum Samples
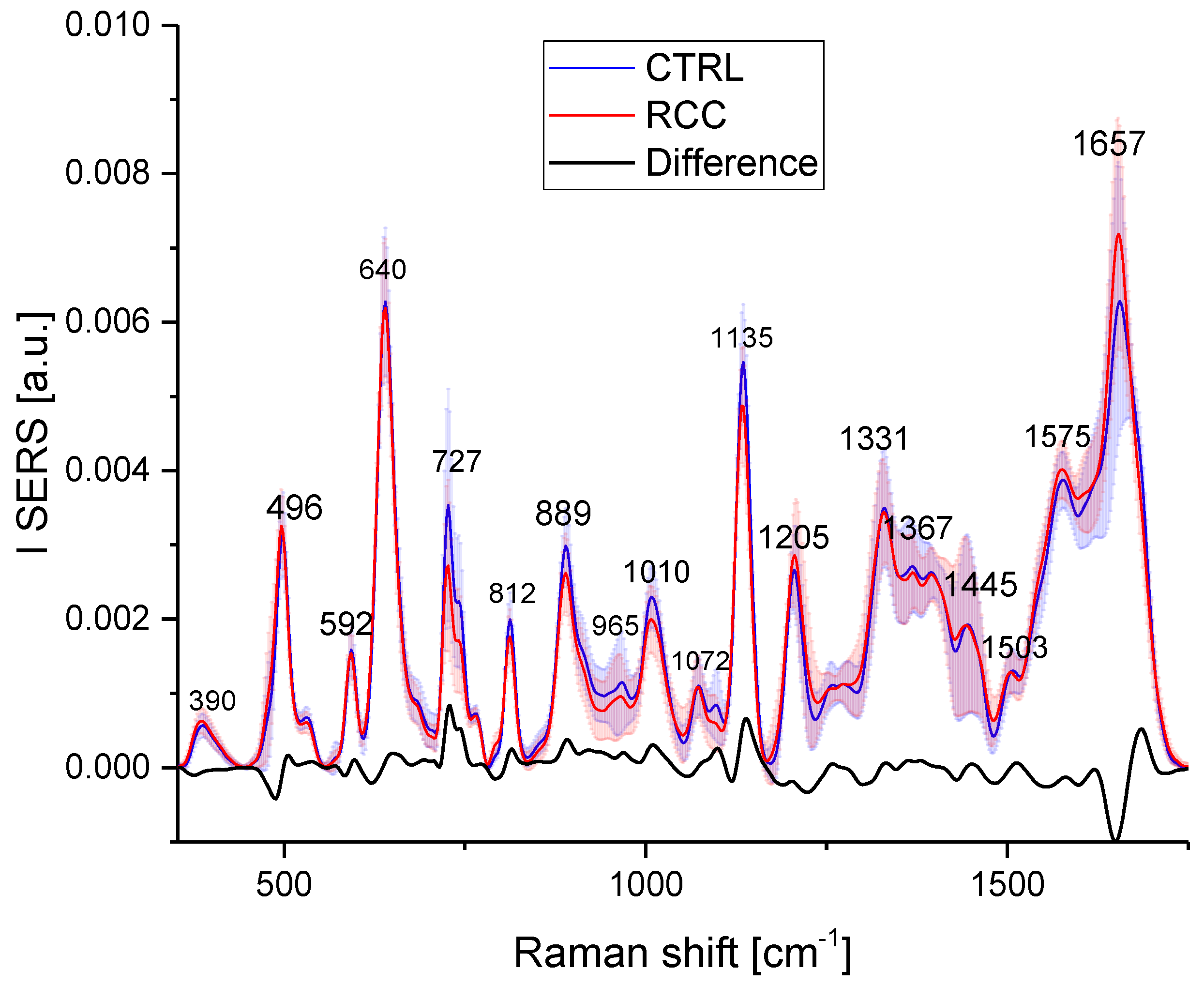
3.1.1. Major SERS Vibrational Peaks in the Serum Samples and Their Tentative Assignment
3.1.2. Correlations between the SERS Intensities of Major Vibrational Peaks
3.2. Descriptive Statistics
3.3. Multivariate Analysis
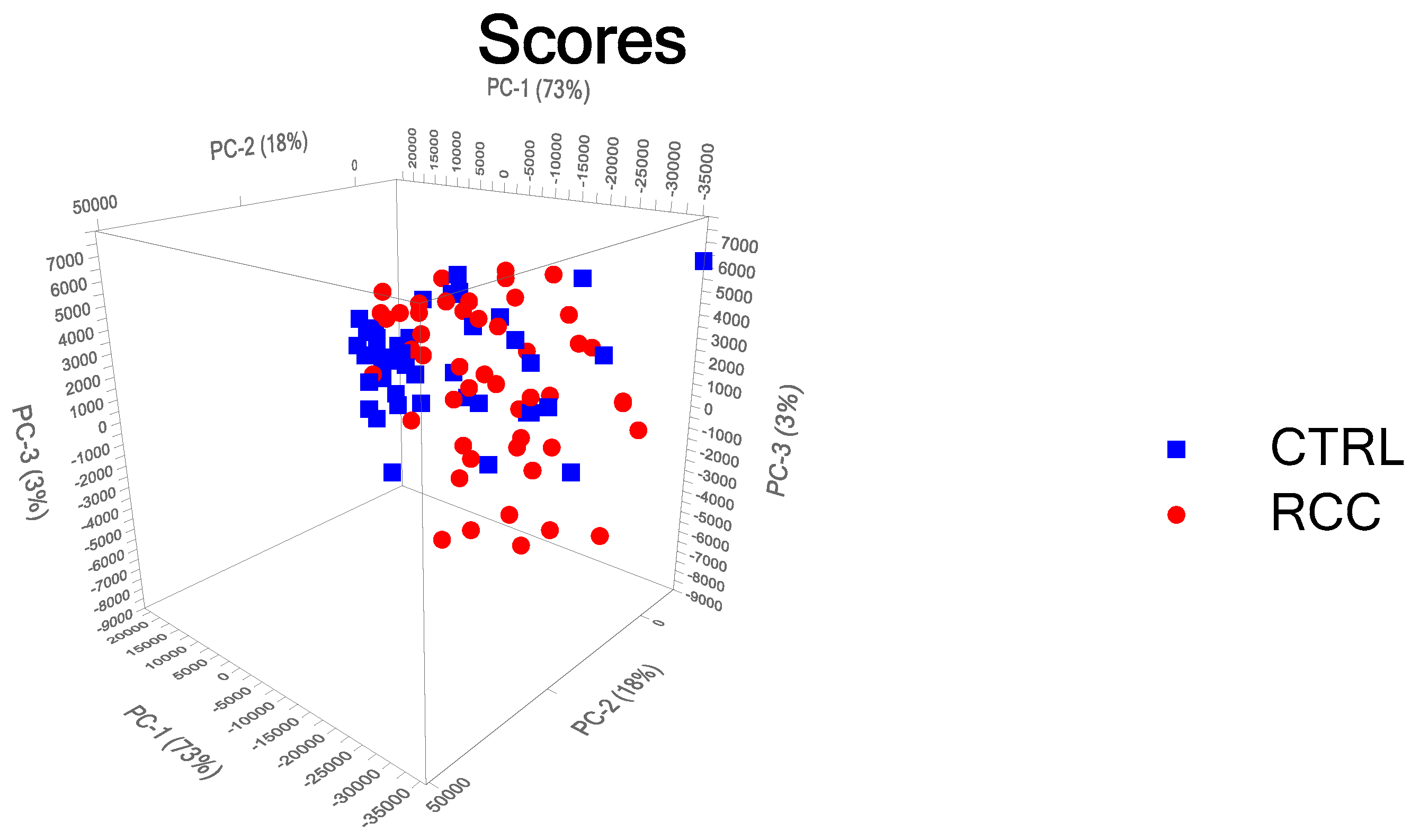
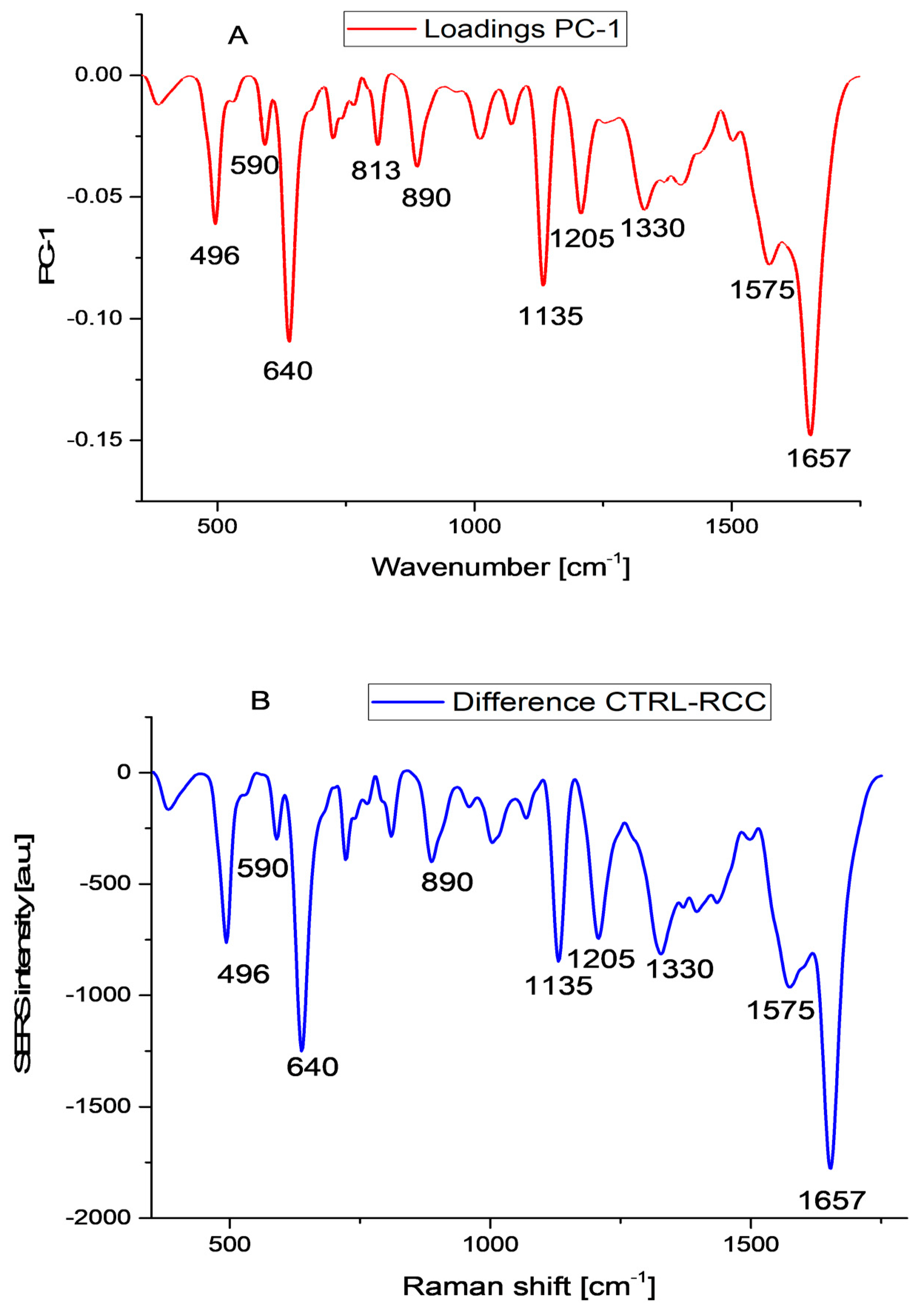
3.3.1. Principal Component Analysis
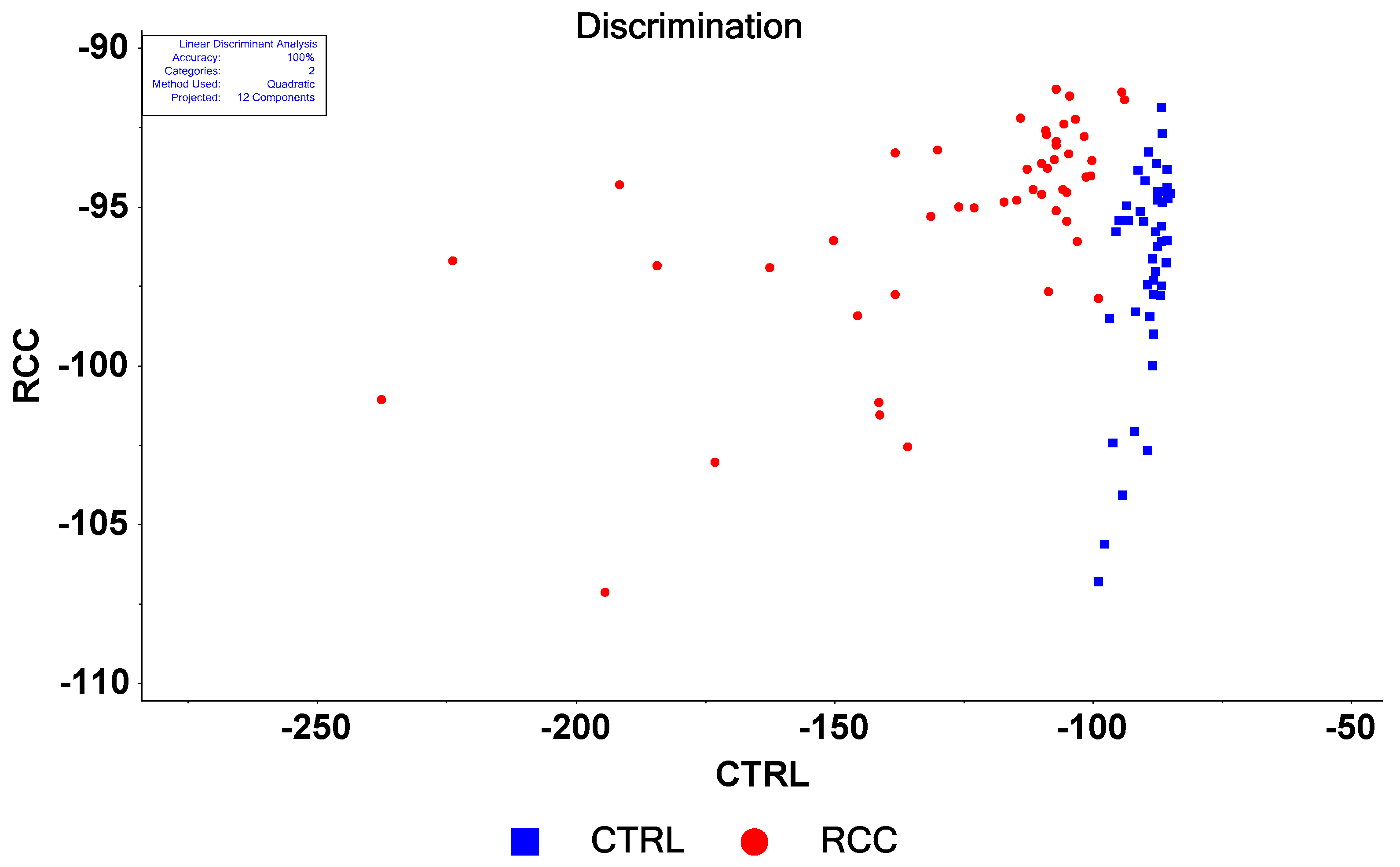
3.3.2. Linear Discriminant Analysis on Raw Data
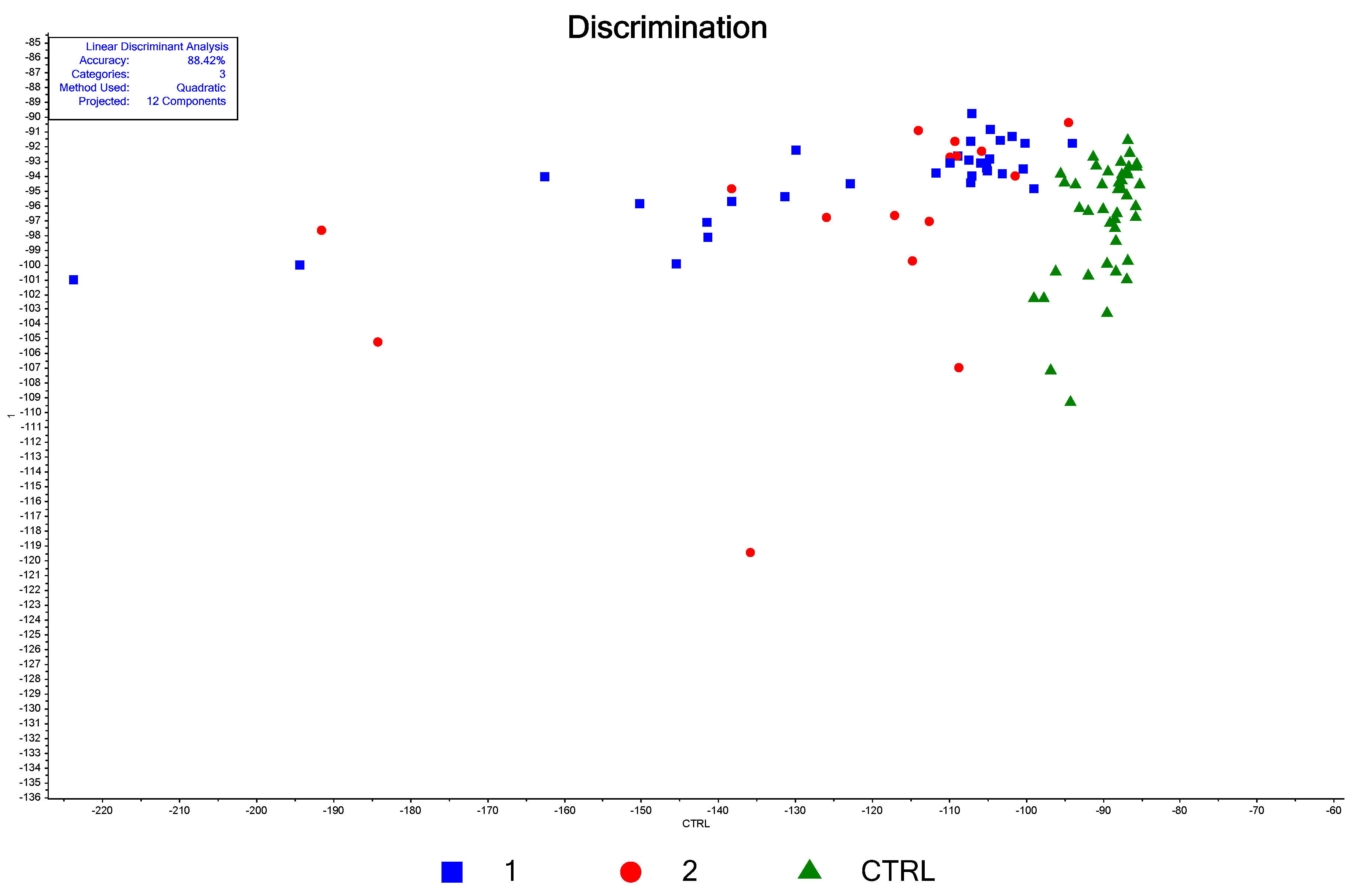
3.3.3. LDA-PCA for the Discrimination between Stages
3.3.4. Multivariate Analysis for Normalized Data
3.3.5. SVM
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Jayson, M.; Sanders, H. Increased incidence of serendipitously discovered renal cell carcinoma. Urology 1998, 51, 203–205. [Google Scholar] [CrossRef]
- Moch, H.; Amin, M.B.; Berney, D.M.; Compérat, E.M.; Gill, A.J.; Hartmann, A.; Menon, S.; Raspollini, M.R.; Rubin, M.A.; Srigley, J.R.; et al. The 2022 World Health Organization Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2022, 82, 458. [Google Scholar] [CrossRef]
- Vasudev, N.S.; Wilson, M.; Stewart, G.D.; Adeyoju, A.; Cartledge, J.; Kimuli, M.; Datta, S.; Hanbury, D.; Hrouda, D.; Oades, G.; et al. Challenges of early renal cancer detection: Symptom patterns and incidental diagnosis rate in a multicentre prospective UK cohort of patients presenting with suspected renal cancer. BMJ Open 2020, 10, e035938. [Google Scholar] [CrossRef] [PubMed]
- Tahbaz, R.; Schmid, M.; Merseburger, A.S. Prevention of kidney cancer incidence and recurrence: Lifestyle, medication, and nutrition. Curr. Opin. Urol. 2018, 28, 62. [Google Scholar] [CrossRef] [PubMed]
- Klatte, T.; Rossi, S.H.; Stewart, G.D. Prognostic factors and prognostic models for renal cell carcinoma: A literature review. World J. Urol. 2018, 36, 1943–1952. [Google Scholar] [CrossRef]
- Keegan, K.A.; Schupp, C.W.; Chamie, K.; Hellenthal, N.J.; Evans, C.P.; Koppie, T.M. Histopathology of Surgically Treated Renal Cell Carcinoma: Survival Differences by Subtype and Stage. J. Urol. 2012, 188, 391–397. [Google Scholar] [CrossRef] [Green Version]
- Patard, J.-J.; Leray, E.; Rodriguez, A.; Rioux-Leclercq, N.; Guillé, F.; Lobel, B. Correlation between Symptom Graduation, Tumor Characteristics and Survival in Renal Cell Carcinoma. Eur. Urol. 2003, 44, 226–232. [Google Scholar] [CrossRef]
- Lee, C.T.; Katz, J.; Fearn, P.A.; Russo, P. Mode of presentation of renal cell carcinoma provides prognostic information. Urol. Oncol. 2002, 7, 135. [Google Scholar] [CrossRef]
- Zheng, B.S.; Wang, S.D.; Zhang, J.Y.; Ge, C.G. Incidence, Prognostic Factors, and Survival of Patients with Renal Cancer: A Population-Based Study. J. Investig. Surg. 2023, 30, 1. [Google Scholar] [CrossRef] [PubMed]
- Diana, P.; Klatte, T.; Amparore, D.; Bertolo, R.; Carbonara, U.; Erdem, S.; Ingels, A.; Kara, O.; Marandino, L.; Marchioni, M.; et al. Screening programs for renal cell carcinoma: A systematic review by the EAU young academic urologists renal cancer working group. World J. Urol. 2022, 41, 929–940. [Google Scholar] [CrossRef]
- Rossi, S.H.; Klatte, T.; Usher-Smith, J.; Stewart, G.D. Epidemiology and screening for renal cancer. World J. Urol. 2018, 36, 1341–1353. [Google Scholar] [CrossRef] [Green Version]
- Usher-Smith, J.A.; Godoy, A.; Burge, S.W.; Burbidge, S.; Cartledge, J.; Crosbie, P.A.J.; Eckert, C.; Farquhar, F.; Hammond, D.; Hancock, N.; et al. The Yorkshire Kidney Screening Trial (YKST): Protocol for a feasibility study of adding non-contrast abdominal CT scanning to screen for kidney cancer and other abdominal pathology within a trial of community-based CT screening for lung cancer. BMJ Open 2022, 12, e063018. [Google Scholar] [CrossRef]
- Glennon, K.I.; Maralani, M.; Abdian, N.; Paccard, A.; Montermini, L.; Nam, A.J.; Arseneault, M.; Staffa, A.; Jand-aghi, P.; Meehan, B.; et al. Rational Development of Liquid Biopsy Analysis in Renal Cell Carcinoma. Cancers 2021, 13, 5825. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Bedke, J.; Bex, A.; Capitanio, U.; Giles, R.H.; Hora, M.; Klatte, T.; Marconi, L.; Powles, T.; et al. EAU Guidelines on Renal Cell Carcinoma. Available online: https://uroweb.org/guidelines/renal-cell-carcinoma (accessed on 5 August 2023).
- Baker, M.J.; Byrne, H.J.; Chalmers, J.; Gardner, P.; Goodacre, R.; Henderson, A.; Kazarian, S.G.; Martin, F.L.; Moger, J.; Stone, N.; et al. Clinical Applications of Infrared and Raman Spectroscopy: State of Play and Future Challenges. Analyst 2018, 143, 1735. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Formoso, M.; Alvarez-Puebla, R.A. Cancer Diagnosis through SERS and Other Related Techniques. Int. J. Mol. Sci. 2020, 21, 2253. [Google Scholar] [CrossRef] [Green Version]
- Langer, J.; Jimenez de Aberasturi, D.; Aizpurua, J.; Alvarez-Puebla, R.A.; Auguié, B.; Baumberg, J.J.; Bazan, G.C.; Bell, S.E.J.; Boisen, A.; Brolo, A.G.; et al. Present and Future of Surface-Enhanced Raman Scattering. ACS Nano 2020, 14, 28–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonifacio, A.; Dalla Marta, S.; Spizzo, R.; Cervo, S.; Steffan, A.; Colombatti, A.; Sergo, V. Surface-enhanced Raman spectroscopy of blood plasma and serum using Ag and Au nanoparticles: A systematic study. Anal. Bioanal. Chem. 2014, 406, 2355–2365. [Google Scholar] [CrossRef]
- Moisoiu, V.; Stefancu, A.; Gulei, D.; Boitor, R.; Magdo, L.; Raduly, L.; Pasca, S.; Kubelac, P.; Mehterov, N.; Chis, V.; et al. SERS-based differential diagnosis between multiple solid malignancies: Breast, colorectal, lung, ovarian and oral cancer. Int. J. Nanomed. 2019, ume 14, 6165–6178. [Google Scholar] [CrossRef] [Green Version]
- Premasiri, W.R.; Lee, J.C.; Ziegler, L.D. Surface-Enhanced Raman Scattering of Whole Human Blood, Blood Plasma, and Red Blood Cells: Cellular Processes and Bioanalytical Sensing. J. Phys. Chem. B 2012, 116, 9376–9386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Știufiuc, G.F.; Toma, V.; Buse, M.; Mărginean, R.; Morar-Bolba, G.; Culic, B.; Tetean, R.; Leopold, N.; Pavel, I.; Lucaciu, C.M.; et al. Solid Plasmonic Substrates for Breast Cancer Detection by Means of SERS Analysis of Blood Plasma. Nanomaterials 2020, 10, 1212. [Google Scholar] [CrossRef]
- Moisoiu, T.; Iancu, S.D.; Burghelea, D.; Dragomir, M.P.; Iacob, G.; Stefancu, A.; Cozan, R.G.; Antal, O.; Bálint, Z.; Muntean, V.; et al. SERS Liquid Biopsy Profiling of Serum for the Diagnosis of Kidney Cancer. Biomedicines 2022, 10, 233. [Google Scholar] [CrossRef]
- Bai, X.; Lin, J.; Wu, X.; Lin, Y.; Zhao, X.; Du, W.; Gao, J.; Hu, Z.; Xu, Q.; Li, T.; et al. Label-free detection of bladder cancer and kidney cancer plasma based on SERS and multivariate statistical algorithm. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2022, 279, 121336. [Google Scholar] [CrossRef] [PubMed]
- Leopold, N.; Lendl, B. A New Method for Fast Preparation of Highly Surface-Enhanced Raman Scattering (SERS) Active Silver Colloids at Room Temperature by Reduction of Silver Nitrate with Hydroxylamine Hydrochloride. J. Phys. Chem. B 2003, 107, 5723–5727. [Google Scholar] [CrossRef]
- Trefry, J.C.; Monahan, J.L.; Weaver, K.M.; Meyerhoefer, A.J.; Markopolous, M.M.; Arnold, Z.S.; Wooley, D.P.; Pavel, I.E. Size Selection and Concentration of Silver Nanoparticles by Tangential Flow Ultrafiltration for SERS-Based Biosensors. J. Am. Chem. Soc. 2010, 132, 10970–10972. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Lin, D.; Lin, J.; Li, B.; Huang, Z.; Chen, G.; Zhang, W.; Wang, L.; Pan, J.; Chen, R.; et al. Blood plasma surface-enhanced Raman spectroscopy for non-invasive optical detection of cervical cancer. Analyst 2013, 138, 3967–3974. [Google Scholar] [CrossRef]
- Lin, J.; Chen, R.; Feng, S.; Pan, J.; Li, Y.; Chen, G.; Cheng, M.; Huang, Z.; Yu, Y.; Zeng, H. A novel blood plasma analysis technique combining membrane electrophoresis with silver nanoparticle-based SERS spectroscopy for potential applications in noninvasive cancer detection. Nanomed. Nanotechnol. Biol. Med. 2011, 7, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Pan, J.; Wu, Y.; Lin, D.; Chen, Y.; Xi, G.; Lin, J.; Chen, R. Study on gastric cancer blood plasma based surface-enhanced Raman spectroscopy combined with multivariate analysis. Sci. China Life Sci. 2011, 54, 828–834. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.; Lin, Y.; Zhao, X.; Gao, J.; Xie, S.; Gong, W.; Yu, Y.; Lin, J. Label-free surface enhanced Raman spectroscopy analysis of blood serum via coffee ring effect for accurate diagnosis of cancers. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2022, 267, 120605. [Google Scholar] [CrossRef]
- Fornasaro, S.; Gurian, E.; Pagarin, S.; Genova, E.; Stocco, G.; Decorti, G.; Sergo, V.; Bonifacio, A. Ergothioneine, a dietary amino acid with a high relevance for the interpretation of label-free surface enhanced Raman scattering (SERS) spectra of many biological samples. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2021, 246, 119024. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.; Lu, D.; Zhang, B.; You, R.; Chen, J.; Xu, H.; Lu, Y. Machine learning–assisted internal standard calibration label-free SERS strategy for colon cancer detection. Anal. Bioanal. Chem. 2023, 415, 1699–1707. [Google Scholar] [CrossRef]
- Lin, D.; Pan, J.; Huang, H.; Chen, G.; Qiu, S.; Shi, H.; Chen, W.; Yu, Y.; Feng, S.; Chen, R. Label-free blood plasma test based on surface-enhanced Raman scattering for tumor stages detection in nasopharyngeal cancer. Sci. Rep. 2014, 4, 4751. [Google Scholar] [CrossRef] [Green Version]
- González-Solís, J.; Luévano-Colmenero, G.; Vargas-Mancilla, J. Surface enhanced Raman spectroscopy in breast cancer cells. Laser Ther. 2013, 22, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Li, L.; Zeng, Q.; Zhang, Y.; Guo, Z.; Liu, Z.; Jin, M.; Su, C.; Lin, L.; Xu, J.; et al. Characterization and noninvasive diagnosis of bladder cancer with serum surface-enhanced Raman spectroscopy and genetic algorithms. Sci. Rep. 2015, 5, 9582. [Google Scholar] [CrossRef] [PubMed]
- Bonifacio, A.; Cervo, S.; Sergo, V. Label-free surface-enhanced Raman spectroscopy of biofluids: Fundamental aspects and diagnostic applications. Anal. Bioanal. Chem. 2015, 407, 8265–8277. [Google Scholar] [CrossRef] [PubMed]
- Cervo, S.; Mansutti, E.; Del Mistro, G.; Spizzo, R.; Colombatti, A.; Steffan, A.; Servo, V.; Bonifacio, A. SERS analysis of serum for detection of early and locally advanced breast cancer. Anal. Bioanal. Chem. 2015, 407, 7503–7509. [Google Scholar] [CrossRef]
- Munteanu, V.C.; Munteanu, R.A.; Gulei, D.; Mărginean, R.; Schițcu, V.H.; Onaciu, A.; Toma, V.; Știufiuc, G.F.; Coman, I.; Știufiuc, R.I. New Insights into the Multivariate Analysis of SER Spectra Collected on Blood Samples for Prostate Cancer Detection: Towards a Better Understanding of the Role Played by Different Biomolecules on Cancer Screening: A Preliminary Study. Cancers 2022, 14, 3227. [Google Scholar] [CrossRef]
- Wu, L.; Wang, Z.; Zong, S.; Cui, Y. Rapid and reproducible analysis of thiocyanate in real human serum and saliva using a droplet SERS-microfluidic chip. Biosens. Bioelectron. 2014, 62, 13–18. [Google Scholar] [CrossRef]
- Stewart, A.; Murray, S.; Bell, S.E.J. Simple preparation of positively charged silver nanoparticles for detection of anions by surface-enhanced Raman spectroscopy. Analyst 2015, 140, 2988–2994. [Google Scholar] [CrossRef]
- Fornasaro, S.; Sergo, V.; Bonifacio, A. The key role of ergothioneine in label-free surface-enhanced Raman scattering spectra of biofluids: A retrospective re-assessment of the literature. FEBS Lett. 2022, 596, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Pucetaite, M.; Velicka, M.; Pilipavicius, J.; Beganskiene, A.; Ceponkus, J.; Sablinskas, V. Uric acid detection by means of SERS spectroscopy on dried Ag colloidal drops. J. Raman Spectrosc. 2016, 47, 681–686. [Google Scholar] [CrossRef]
- Huang, W.; Jiang, J.-Z.; Chen, L.; Zhang, B.-Q.; Deng, S.-F.; Sun, J.J.; Chen, W.-K. Density functional theory and surface enhanced Raman spectroscopy studies of tautomeric hypoxanthine and its adsorption behaviors in electrochemical processes. Electrochim. Acta 2015, 164, 132–138. [Google Scholar] [CrossRef]
- Colceriu-Șimon, I.M.; Hedeșiu, M.; Toma, V.; Armencea, G.; Moldovan, A.; Știufiuc, G.; Culic, B.; Țărmure, V.; Dinu, C.; Berindan-Neagoe, I.; et al. The effects of low-dose irradiation on human saliva: A surface-enhanced Raman spectroscopy study. Diagnostics 2019, 9, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allegrini, S.; Garcia-Gil, M.; Pesi, R.; Camici, M.; Tozzi, M.G. The Good, the Bad and the New about Uric Acid in Cancer. Cancers 2022, 14, 4959. [Google Scholar] [CrossRef]
- Aurilio, G.; Piva, F.; Santoni, M.; Cimadamore, A.; Sorgentoni, G.; Lopez-Beltran, A.; Cheng, L.; Battelli, N.; Nolè, F.; Montironi, R. The Role of Obesity in Renal Cell Carcinoma Patients: Clinical-Pathological Implications. Int. J. Mol. Sci. 2019, 20, 5683. [Google Scholar] [CrossRef] [Green Version]
- Battelli, M.G.; Polito, L.; Bortolotti, M.; Bolognesi, A. Xanthine oxidoreductase in cancer: More than a differentiation marker. Cancer Med. 2016, 5, 546–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.-M.; Meng, L.-H. The double faced role of xanthine oxidoreductase in cancer. Acta Pharmacol. Sin. 2021, 43, 1623–1632. [Google Scholar] [CrossRef]
- Dai, X.; He, Q.; Jing, Z.; Yuan, J. Serum uric acid levels and risk of kidney cancer incidence and mortality: A prospective cohort study. Cancer Med. 2020, 9, 5655–5661. [Google Scholar] [CrossRef]
- LIBSVM—A Library for Support Vector Machines. Available online: https://www.csie.ntu.edu.tw/~cjlin/libsvm/index.html (accessed on 25 May 2023).
- dos Santos, D.P.; Sena, M.M.; Almeida, M.R.; Mazali, I.O.; Olivieri, A.C.; Villa, J.E.L. Unraveling surface-enhanced Raman spectroscopy results through chemometrics and machine learning: Principles, progress, and trends. Anal. Bioanal. Chem. 2023, 415, 3945–3966. [Google Scholar] [CrossRef] [PubMed]
- Zong, M.; Zhou, L.; Guan, Q.; Lin, D.; Zhao, J.; Qi, H.; Harriman, D.; Fan, L.; Zeng, H.; Du, C. Comparison of Sur-face-Enhanced Raman Scattering Properties of Serum and Urine for the Detection of Chronic Kidney Disease in Patients. Appl. Spectrosc. 2021, 75, 412–421. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Raman Shift Measured [cm−1] | Raman Shift Range Reported [cm−1] | Assignments in Literature | Tentative Assignments in this Study |
|---|---|---|---|
| 390 | 382 | Uric acid [22] | Uric acid |
| 496 | 482–496 | ν(S–S) [28] and ring vibration of L-arginine [29,30], guanine [30,31], ergothioneine [32], DNA [33] | 480 Ergothioneine 496 Uric acid |
| 593 | 589–592 | amide-VI [30], glycerol [31] uric acid [20] | Uric acid |
| 640 | 637–650 | ν(C–S) of tyrosine [28,30,31,33,34,35] τ(C–C) of tyrosine [29] and phenylalanine [36], uric acid [20,22] | Uric acid |
| 727 | 720–725 | Hypoxanthine [20,22,29,31,37,38], δ(CH) of adenine [30,36] | Hypoxanthine |
| 765 | 755–757 | Tryptophan [34,35] | Uric Acid |
| 812 | 813–818 | ν(C–C–O) of L-serine [28,30,31], ν(C–C) of collagen [34], gluthatione [30], uric acid [20,22] | Uric acid |
| 889 | 885–890 | ν(C–O–H) of D-galactosamine [28,29,31,33,34,37], glutathione [30,34], uric acid [20,22] | Uric acid |
| 1008 | 1002–1003 | ν(C–C) in ring breathing of phenylalanine [20,29,31,34,35,37] uric acid [22] | Phenylalanine |
| 1070 | 1068–1074 | ν(C–C) of lipids [29,31], ν(C–N) [30] of collagen | |
| 1135 | 1131–1135 | ν(C–N) of D-mannose [28,29,31,36], tyrosine [20], uric acid [22] | Uric acid |
| 1205 | 1205–1219 | ν(C–C6H5) of tryptophan and phenylalanine rings [29,31,34,36], uric acid [22], ergothioneine [32] | Ergothioneine/Uric acid |
| 1260 | 1250–1257 | Amid III [34,37] | Amid III |
| 1331 | 1324–1338 | Adenine [28], δ(CH2) [34], hypoxanthine [38], ν(CH) of nucleic acid bases [30,31] | |
| 1396 | 1400–1402 | δ(CH2) of collagen [28], phospholipids [28,29], citrate [37] | |
| 1445 | 1444–1450 | Collagen [34,36], phospholipids [34,36], hypoxanthine [33,38], δ(CH2/CH3) [20,22,35,38] ergothioneine [32] | |
| 1575 | 1576–1585 | δ(C=C) of phenylalanine [28,30,33,34,36], acetoacetate [34,36,38], riboflavin [30,34,35], DNA/RNA bases [29], uric acid [20], amide II [20] hypoxanthine [22] ergothioneine [32] | Amide II |
| 1657 | 1640–1680 | ν(C=O) of amide I with the α-helix conformation [20,28,29,34,35,36,39] or collagen [30,31] | Amid I α helix |
| 2107 | 2108 | Thiocyanate [40] | Thiocyanate |
| Wavenumber (cm−1) | Coefficient of Determination for the Linear Regression with 640 cm−1 (R2) | Wavenumber (cm−1) | Coefficient of Determination for the Linear Regression with 727 cm−1 (R2) |
|---|---|---|---|
| 496 | R2 = 0.93 | 496 | R2 = 0.11 |
| 390 | R2 = 0.84 | 390 | R2 = 0.26 |
| 531 | R2 = 0.80 | 531 | R2 = 0.01 |
| 590 | R2 = 0.98 | 590 | R2 = 0.11 |
| 640 | 1 | 640 | R2 = 0.15 |
| 727 | R2 = 0.15 | 727 | 1 |
| 765 | R2 = 0.94 | 765 | R2 = 0.00 |
| 812 | R2 = 0.91 | 812 | R2 = 0.20 |
| 889 | R2 = 0.93 | 889 | R2 = 0.21 |
| 1008 | R2 = 0.82 | 1008 | R2 = 0.13 |
| 1031 | R2 = 0.55 | 1031 | R2 = 0.01 |
| 1070 | R2 = 0.79 | 1070 | R2 = 0.06 |
| 1135 | R2 = 0.93 | 1135 | R2 = 0.20 |
| 1170 | R2 = 0.00 | 1170 | R2 = 0.02 |
| 1260 | R2 = 0.40 | 1260 | R2 = 0.13 |
| 1331 | R2 = 0.45 | 1331 | R2 = 0.44 |
| 1390 | R2 = 0.60 | 1390 | R2 = 0.29 |
| 1445 | R2 = 0.02 | 1445 | R2 = 0.25 |
| 1503 | R2 = 0.83 | 1503 | R2 = 0.22 |
| 1575 | R2 = 0.72 | 1575 | R2 = 0.23 |
| 1657 | R2 = 0.89 | 1657 | R2 = 0.12 |
| Wavenumber [cm−1] | p | Interpretation |
|---|---|---|
| 390 | p < 0.001 | Highly significant |
| 496 | p < 0.001 | Highly significant |
| 590 | p < 0.001 | Highly significant |
| 640 | p < 0.001 | Highly significant |
| 727 | p = 0.111 | Statistically insignificant |
| 812 | p = 0.022 | Significant |
| 889 | p = 0.015 | Significant |
| 1008 | p < 0.001 | Highly significant |
| 1070 | p = 0.0012 | Significant |
| 1135 | p = 0.039 | Significant |
| 1205 | p < 0.001 | Highly significant |
| 1331 | p < 0.001 | Highly significant |
| 1445 | p = 0.016 | Significant |
| 1575 | p < 0.001 | Highly significant |
| 1657 | p < 0.001 | Highly significant |
| Actual/Predicted | CTRL | Stage 1 | Stages 2 and 3 | Total Predicted |
|---|---|---|---|---|
| CTRL | 42 | 2 | 1 | 45 |
| Stage 1 | 2 | 26 | 1 | 29 |
| Stages 2 and 3 | 1 | 4 | 16 | 21 |
| Total Actual | 45 | 32 | 18 |
| Actual/Predicted | CTRL | Stage 1 | Stage 2 | Stage 3 | Total Predicted |
|---|---|---|---|---|---|
| CTRL | 45 | 0 | 0 | 1 | 46 |
| Stage 1 | 0 | 32 | 11 | 5 | 48 |
| Stage 2 | 0 | 0 | 0 | 1 | 1 |
| Stage 3 | 0 | 0 | 0 | 0 | 0 |
| Total Actual | 45 | 32 | 11 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buhas, B.A.; Toma, V.; Crisan, N.; Ploussard, G.; Maghiar, T.A.; Știufiuc, R.-I.; Lucaciu, C.M. High-Accuracy Renal Cell Carcinoma Discrimination through Label-Free SERS of Blood Serum and Multivariate Analysis. Biosensors 2023, 13, 813. https://doi.org/10.3390/bios13080813
Buhas BA, Toma V, Crisan N, Ploussard G, Maghiar TA, Știufiuc R-I, Lucaciu CM. High-Accuracy Renal Cell Carcinoma Discrimination through Label-Free SERS of Blood Serum and Multivariate Analysis. Biosensors. 2023; 13(8):813. https://doi.org/10.3390/bios13080813
Chicago/Turabian StyleBuhas, Bogdan Adrian, Valentin Toma, Nicolae Crisan, Guillaume Ploussard, Teodor Andrei Maghiar, Rareș-Ionuț Știufiuc, and Constantin Mihai Lucaciu. 2023. "High-Accuracy Renal Cell Carcinoma Discrimination through Label-Free SERS of Blood Serum and Multivariate Analysis" Biosensors 13, no. 8: 813. https://doi.org/10.3390/bios13080813