Label-Free Analysis of Urine Samples with In-Flow Digital Holographic Microscopy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
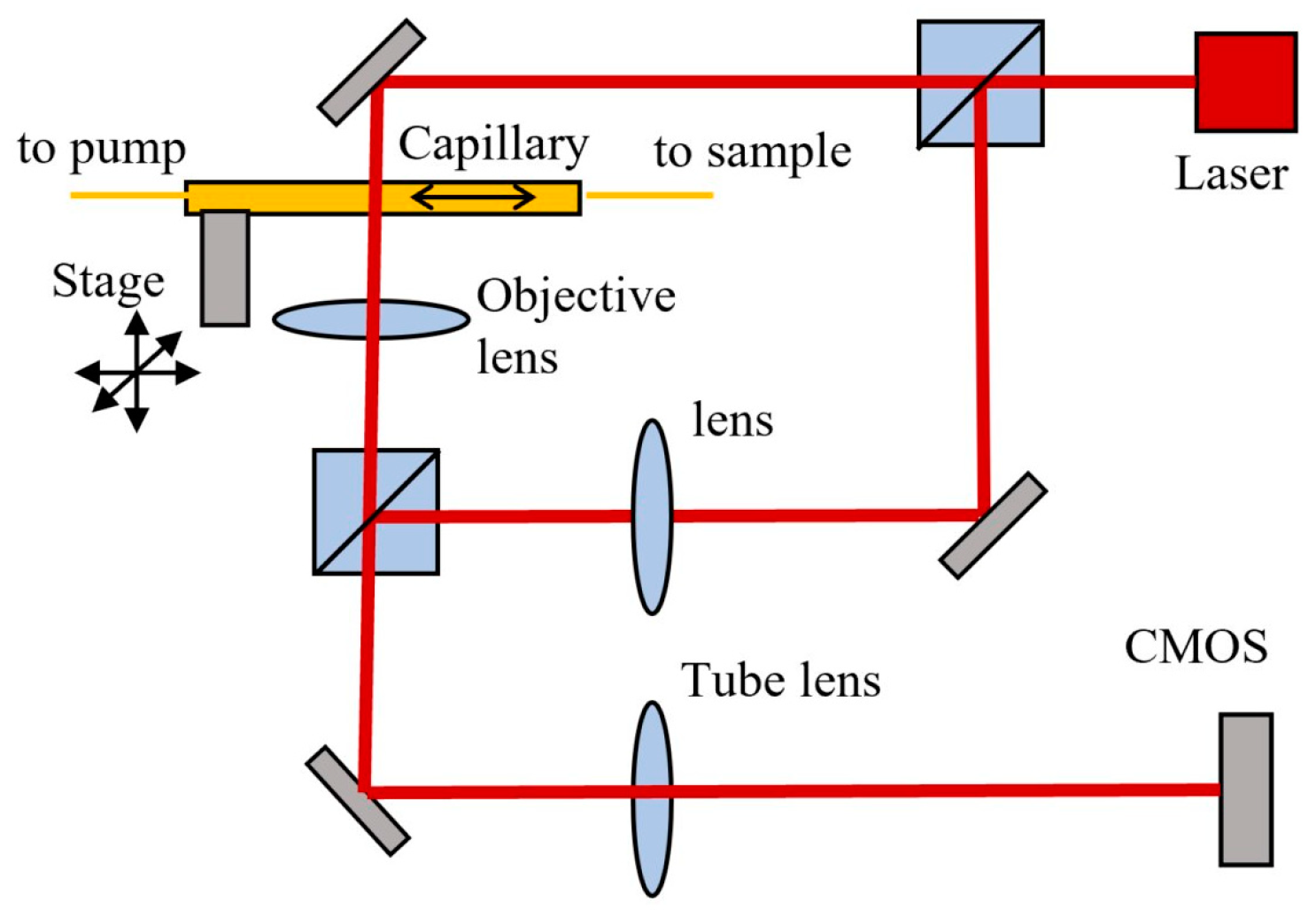
2.1. In-Flow DHM
2.2. Sample Handling
2.3. Culture Plate Test (CPT)
2.4. Measured Parameters and Evaluation Criteria
3. Results and Discussion
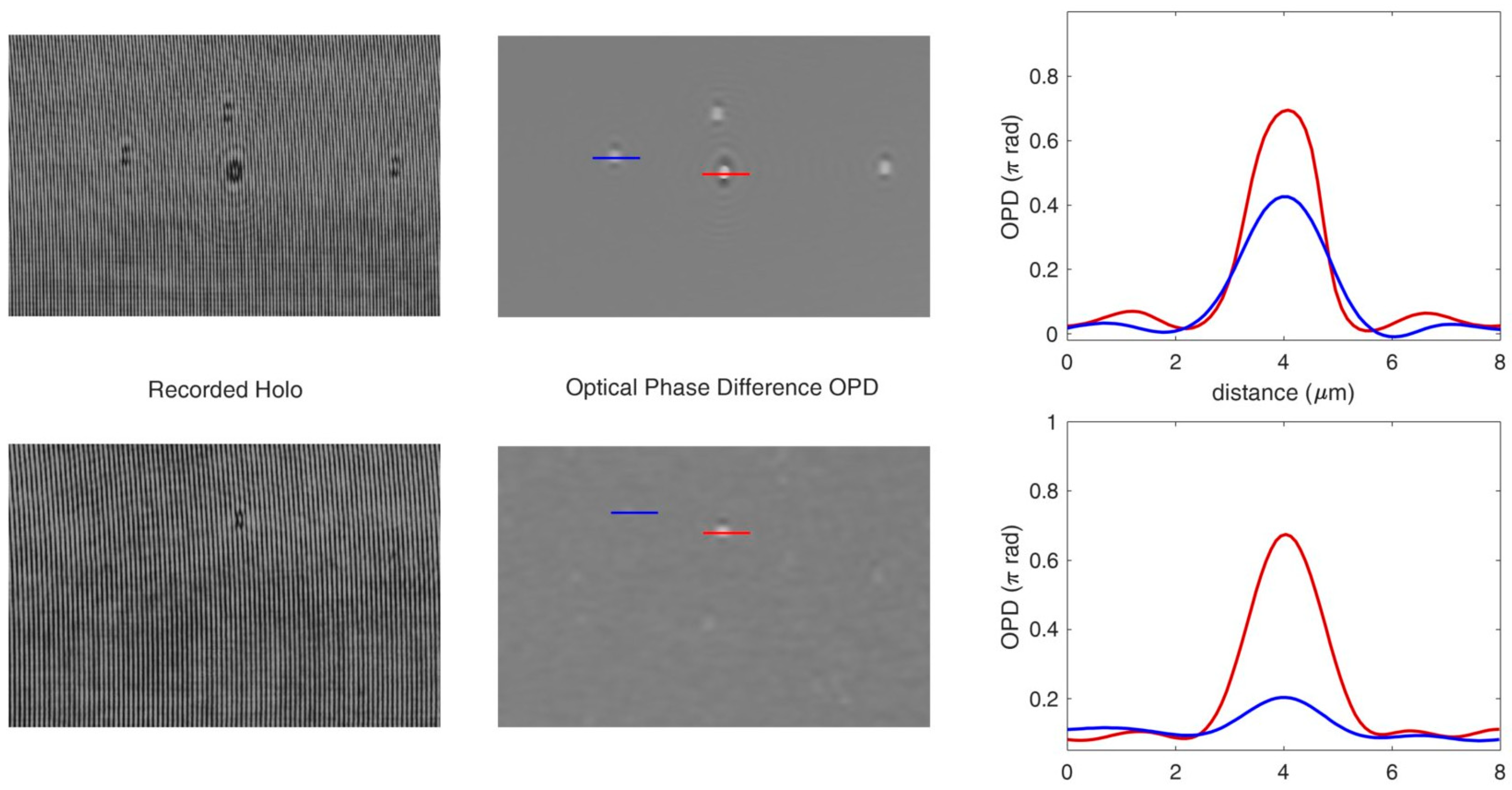
3.1. In-Flow DHM of Microbeads in a Glass Capillary
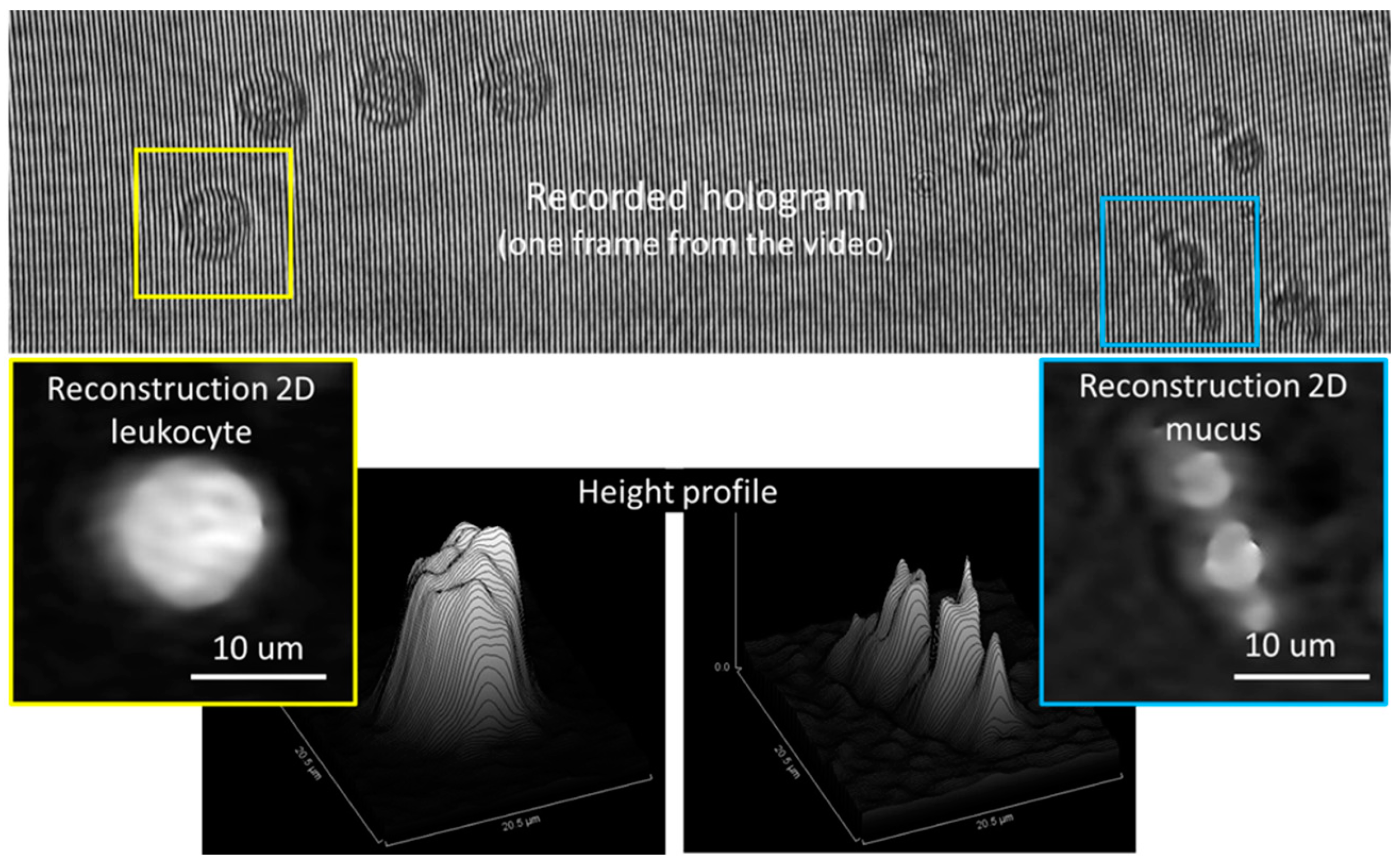
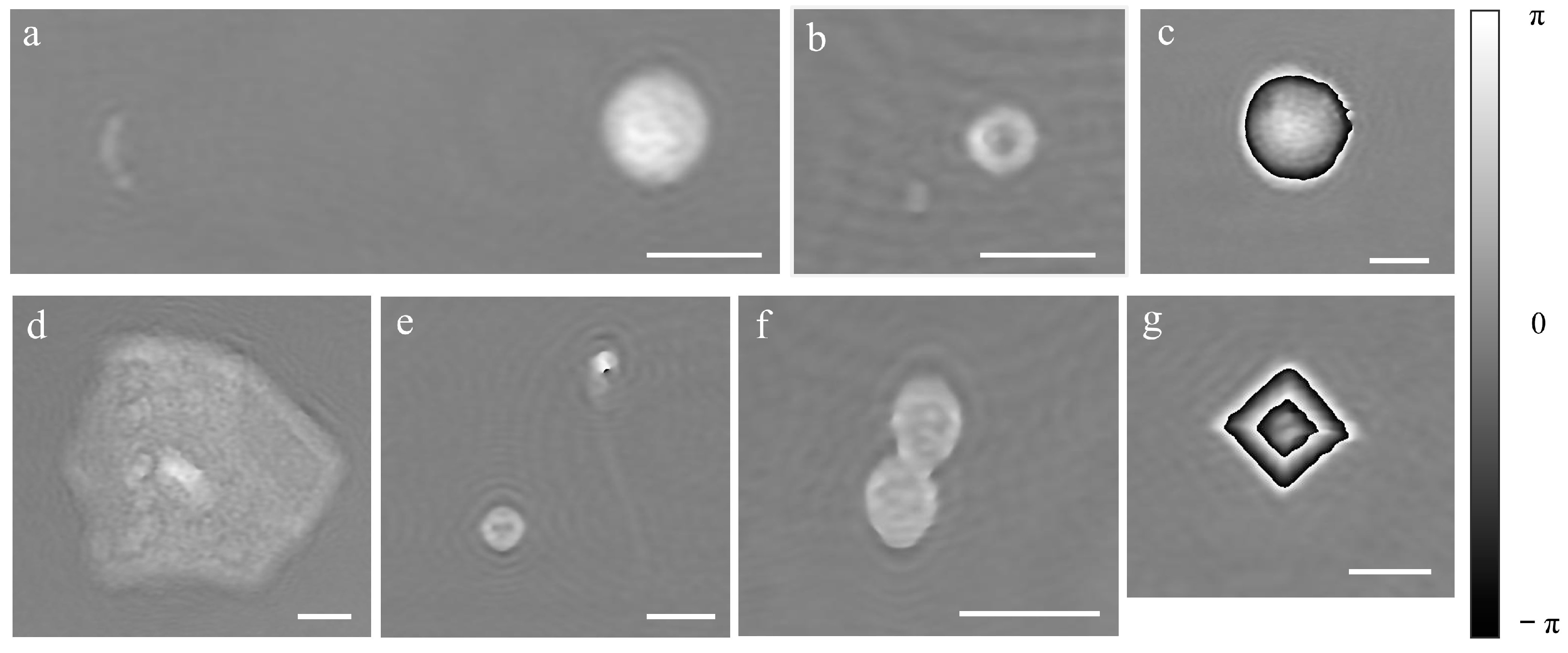
3.2. In-Flow DHM of Urine Sample in a Glass Capillary
3.3. Bacteriuria Detection and Samples Classification into Positives or Negatives
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gehringer, C.; Regeniter, A.; Rentsch, K.; Tschudin-Sutter, S.; Bassetti, S.; Egli, A. Accuracy of urine flow cytometry and urine test strip in predicting relevant bacteriuria in different patient populations. BMC Infect. Dis. 2021, 21, 209. [Google Scholar] [CrossRef]
- Cao, Y.; Gao, F.; Chen, W. Comparison of different urine culture methods in urinary tract infection. Transl. Androl. Urol. 2022, 11, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Xie, R.; Li, X.; Li, G.; Fu, R. Diagnostic value of different urine tests for urinary tract infection: A systematic review and meta-analysis. Transl. Androl. Urol. 2022, 11, 325. [Google Scholar] [PubMed]
- Boonen, K.J.M.; Koldewijn, E.L.; Arents, N.L.A.; Raaymakers, P.A.M.; Scharnhorst, V. Urine flow cytometry as a primary screening method to exclude urinary tract infections. World J. Urol. 2013, 31, 547–551. [Google Scholar] [CrossRef]
- Mejuto, P.; Luengo, M.; Díaz-Gigante, J. Automated Flow Cytometry: An Alternative to Urine Culture in a Routine Clinical Microbiology Laboratory? Int. J. Microbiol. 2017, 2017, 8532736. [Google Scholar] [CrossRef] [Green Version]
- Robinson, J.P. Flow cytometry: Past and future. BioTechniques 2022, 72, 159–169. [Google Scholar] [CrossRef]
- Jolkkonen, S.; Paattiniemi, E.-L.; Kärpänoja, P.; Sarkkinen, H. Screening of Urine Samples by Flow Cytometry Reduces the Need for Culture. J. Clin. Microbiol. 2010, 48, 3117–3121. [Google Scholar] [CrossRef] [Green Version]
- van der Zwet, W.C.; Hessels, J.; Canbolat, F.; Deckers, M.M.L. Evaluation of the Sysmex UF-1000i® urine flow cytometer in the diagnostic work-up of suspected urinary tract infection in a Dutch general hospital. Clin. Chem. Lab. Med. 2010, 48, 1765–1771. [Google Scholar] [CrossRef]
- Okada, H.; Horie, S.; Inoue, J.; Kawashima, Y. The basic performance of bacteria counting for diagnosis of urinary tract infection using the fully automated urine particle analyzer UF-1000i. Sysmex J. Int. 2007, 17, 95–101. [Google Scholar]
- De Rosa, R.; Grosso, S.; Lorenzi, G.; Bruschetta, G.; Camporese, A. Evaluation of the new Sysmex UF-5000 fluorescence flow cytometry analyser for ruling out bacterial urinary tract infection and for prediction of Gram negative bacteria in urine cultures. Clin. Chim. Acta 2018, 484, 171–178. [Google Scholar] [CrossRef]
- Marquet, P.; Rappaz, B.; Magistretti, P.J.; Cuche, E.; Emery, Y.; Colomb, T.; Depeursinge, C. Digital holographic microscopy: A noninvasive contrast imaging technique allowing quantitative visualization of living cells with subwavelength axial accuracy. Opt. Lett. 2005, 30, 468–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemper, B.; Daniel, D.C.; Jürgen, S.; Ilona, B.; Marcus, S.; Wolfram, D.; von Bally, G. Investigation of living pancreas tumor cells by digital holographic microscopy. J. Biomed. Opt. 2006, 11, 034005. [Google Scholar] [CrossRef]
- Bernecker, C.; Lima, M.A.R.B.F.; Ciubotaru, C.D.; Schlenke, P.; Dorn, I.; Cojoc, D. Biomechanics of Ex Vivo-Generated Red Blood Cells Investigated by Optical Tweezers and Digital Holographic Microscopy. Cells 2021, 10, 552. [Google Scholar] [CrossRef] [PubMed]
- Braidotti, N.; do R. B. F. Lima, M.A.; Zanetti, M.; Rubert, A.; Ciubotaru, C.; Lazzarino, M.; Sbaizero, O.; Cojoc, D. The Role of Cytoskeleton Revealed by Quartz Crystal Microbalance and Digital Holographic Microscopy. Int. J. Mol. Sci. 2022, 23, 4108. [Google Scholar] [CrossRef] [PubMed]
- do R. B. F. Lima, M.A.; Cojoc, D. Monitoring Human Neutrophil Differentiation by Digital Holographic Microscopy. Front. Phys. 2021, 9, 653353. [Google Scholar] [CrossRef]
- Uttam, S.; Pham, H.V.; LaFace, J.; Leibowitz, B.; Yu, J.; Brand, R.E.; Hartman, D.J.; Liu, Y. Early Prediction of Cancer Progression by Depth-Resolved Nanoscale Mapping of Nuclear Architecture from Unstained Tissue Specimens. Cancer Res. 2015, 75, 4718–4727. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.; Diez-Silva, M.; Popescu, G.; Lykotrafitis, G.; Choi, W.; Feld, M.S.; Suresh, S. Refractive index maps and membrane dynamics of human red blood cells parasitized by Plasmodium falciparum. Proc. Natl. Acad. Sci. USA 2008, 105, 13730–13735. [Google Scholar] [CrossRef]
- Natan, T.S.; Lisa, L.S.; George, A.T.; Adam, P.W.; Marilyn, J.T. Quantitative microscopy and nanoscopy of sickle red blood cells performed by wide field digital interferometry. J. Biomed. Opt. 2011, 16, 030506. [Google Scholar] [CrossRef] [Green Version]
- Majeed, H.; Nguyen, T.H.; Kandel, M.E.; Kajdacsy-Balla, A.; Popescu, G. Label-free quantitative evaluation of breast tissue using Spatial Light Interference Microscopy (SLIM). Sci. Rep. 2018, 8, 6875. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.; Depeursinge, C.; Popescu, G. Quantitative phase imaging in biomedicine. Nat. Photonics 2018, 12, 578–589. [Google Scholar] [CrossRef]
- Ugele, M.; Weniger, M.; Stanzel, M.; Bassler, M.; Krause, S.W.; Friedrich, O.; Hayden, O.; Richter, L. Label-Free High-Throughput Leukemia Detection by Holographic Microscopy. Adv. Sci. 2018, 5, 1800761. [Google Scholar] [CrossRef] [PubMed]
- Rappaz, B.; Barbul, A.; Emery, Y.; Korenstein, R.; Depeursinge, C.D.; Magistretti, P.J.; Marquet, P. Comparative study of human erythrocytes by digital holographic microscopy, confocal microscopy, and impedance volume analyzer. Cytom. Part A 2008, 73, 895–903. [Google Scholar] [CrossRef] [PubMed]
- McNeal, A.S.; Belote, R.L.; Zeng, H.; Urquijo, M.; Barker, K.; Torres, R.; Curtin, M.; Shain, A.H.; Andtbacka, R.H.I.; Holmen, S.; et al. BRAFV600E induces reversible mitotic arrest in human melanocytes via microRNA-mediated suppression of AURKB. eLife 2021, 10, e70385. [Google Scholar] [CrossRef] [PubMed]
- Roitshtain, D.; Wolbromsky, L.; Bal, E.; Greenspan, H.; Satterwhite, L.L.; Shaked, N.T. Quantitative phase microscopy spatial signatures of cancer cells. Cytom. Part A 2017, 91, 482–493. [Google Scholar] [CrossRef] [Green Version]
- Pham, H.V.; Pantanowitz, L.; Liu, Y. Quantitative phase imaging to improve the diagnostic accuracy of urine cytology. Cancer Cytopathol. 2016, 124, 641–650. [Google Scholar] [CrossRef] [Green Version]
- Rasband, W.S. ImageJ. Available online: https://imagej.nih.gov/ij/ (accessed on 10 January 2020).
- Xiang, D.-J.; Cong, Y.; Wang, C.; Yue, J.; Ma, X.; Lu, Y.; Liu, P.; Ma, J. Development of microscopic review criteria by comparison urine flow cytometer, strip and manual microscopic examination. Clin. Lab. 2012, 58, 979–985. [Google Scholar]
- Christelle, F.; Jacques, D.; Jean-Philippe, R. Évaluation des performances de l’automate d’analyse urinaire UF-1000i®. Ann. Biol. Clin. 2011, 69, 431–439. [Google Scholar] [CrossRef]
- Kadkhoda, K.; Manickam, K.; DeGagne, P.; Sokolowski, P.; Pang, P.; Kontzie, N.; Alfa, M. UF-1000i™ flow cytometry is an effective screening method for urine specimens. Diagn. Microbiol. Infect. Dis. 2011, 69, 130–136. [Google Scholar] [CrossRef]
- Jiang, T.; Chen, P.; Ouyang, J.; Zhang, S.; Cai, D. Urine particles analysis: Performance evaluation of Sysmex UF-1000i and comparison among urine flow cytometer, dipstick, and visual microscopic examination. Scand. J. Clin. Lab. Investig. 2011, 71, 30–37. [Google Scholar] [CrossRef]
- Manoni, F.; Tinello, A.; Fornasiero, L.; Hoffer, P.; Temporin, V.; Valverde, S.; Gessoni, G. Urine particle evaluation: A comparison between the UF-1000i and quantitative microscopy. Clin. Chem. Lab. Med. 2010, 48, 1107–1111. [Google Scholar] [CrossRef]
- Mosby, C.V. Mosby’s Medical Dictionary, 8th ed.; Elsevier: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Cornaglia, G.; Courcol, R.; Herrmann, J.L.; Kahlmeter, G. European Manual of Clinical Microbiology. European Society for Clinical Microbiology and Infections Diseases: Basel, Switzerland, 2012. [Google Scholar]
- Sharp, S.E. Cumitech 2c: Laboratory Diagnosis of Urinary Tract Infections; ASM Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Trevethan, R. Sensitivity, Specificity, and Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Health 2017, 5, 307. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.Y.; Chin, L.K.; Ser, W.; Ayi, T.C.; Yap, P.H.; Bourouina, T.; Leprince-Wang, Y. Real-time Measurement of Single Bacterium’s Refractive Index Using Optofluidic Immersion Refractometry. Procedia Eng. 2014, 87, 356–359. [Google Scholar] [CrossRef]
- Godin, M.; Bryan, A.K.; Burg, T.P.; Babcock, K.; Manalis, S.R. Measuring the mass, density, and size of particles and cells using a suspended microchannel resonator. Appl. Phys. Lett. 2007, 91, 123121. [Google Scholar] [CrossRef] [Green Version]
- Carl, D.; Kemper, B.; Wernicke, G.; von Bally, G. Parameter-optimized digital holographic microscope for high-resolution living-cell analysis. Appl. Opt. 2004, 43, 6536–6544. [Google Scholar] [CrossRef]
- Howard, J. Mechanics of Motor Proteins and the Cytoskeleton; Sinauer Associates: Sunderland, UK, 2001. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensitivity % | TP/(TP + FN) × 100 |
| Specificity % | TN/(TN + FP) × 100 |
| Positive predictive value % | TP/(TP + FN) × 100 |
| Negative predictive value % | TN/(TN + FN) × 100 |
| True positive ratio % | TP/Pos Ref × 100 |
| False positive ratio % | FP/Neg Ref × 100 |
| Accuracy % | (TP + TN)/Tot × 100 |
| (a) | |||||||||||
| |||||||||||
| Number of samples | DHM | UF-1000i * | CPT | ||||||||
| POS | NEG | TOT | POS | NEG | TOT | POS | NEG | TOT | |||
| 133 | 47 | 180 | 114 | 61 | 175 * | 91 | 89 | 180 | |||
| 122 | 47 | 169 | 103 | 61 | 164 | 91 | 78 | 169 | |||
| 110 | 59 | 169 | |||||||||
| (b) | |||||||||||
| Number of samples | DHM vs. CPT | UF-1000i vs. CPT | |||||||||
| TP | TN | FP | FN | TP | TN | FP | FN | ||||
| 82 | 38 | 51 | 9 | 79 | 52 | 35 | 9 | ||||
| 82 | 38 | 40 | 9 | 79 | 52 | 24 | 9 | ||||
| 80 | 48 | 30 | 11 | ||||||||
| (c) | |||||||||||
| % | DHM vs. CPT | UF-1000i vs. CPT | |||||||||
| Sensitivity | 90.11 | 90.00 | 87.91 | 89.77 | 89.66 | ||||||
| Specificity | 42.70 | 48.10 | 61.54 | 59.77 | 67.53 | ||||||
| Positive Predictive Value | 61.65 | 66.39 | 72.73 | 69.30 | 75.73 | ||||||
| Negative Predictive Value | 80.85 | 80.85 | 81.36 | 85.25 | 85.25 | ||||||
| True Positive Ratio | 90.11 | 90.00 | 87.91 | 86.81 | 86.67 | ||||||
| False Positive Ratio | 57.30 | 51.90 | 38.46 | 39.33 | 31.65 | ||||||
| Accuracy | 66.67 | 70.41 | 75.74 | 74.86 | 78.78 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gigli, L.; Braidotti, N.; Lima, M.A.d.R.B.F.; Ciubotaru, C.D.; Cojoc, D. Label-Free Analysis of Urine Samples with In-Flow Digital Holographic Microscopy. Biosensors 2023, 13, 789. https://doi.org/10.3390/bios13080789
Gigli L, Braidotti N, Lima MAdRBF, Ciubotaru CD, Cojoc D. Label-Free Analysis of Urine Samples with In-Flow Digital Holographic Microscopy. Biosensors. 2023; 13(8):789. https://doi.org/10.3390/bios13080789
Chicago/Turabian StyleGigli, Lucia, Nicoletta Braidotti, Maria Augusta do R. B. F. Lima, Catalin Dacian Ciubotaru, and Dan Cojoc. 2023. "Label-Free Analysis of Urine Samples with In-Flow Digital Holographic Microscopy" Biosensors 13, no. 8: 789. https://doi.org/10.3390/bios13080789