Wearable Sensor-Based Monitoring of Environmental Exposures and the Associated Health Effects: A Review


Abstract
:1. Introduction
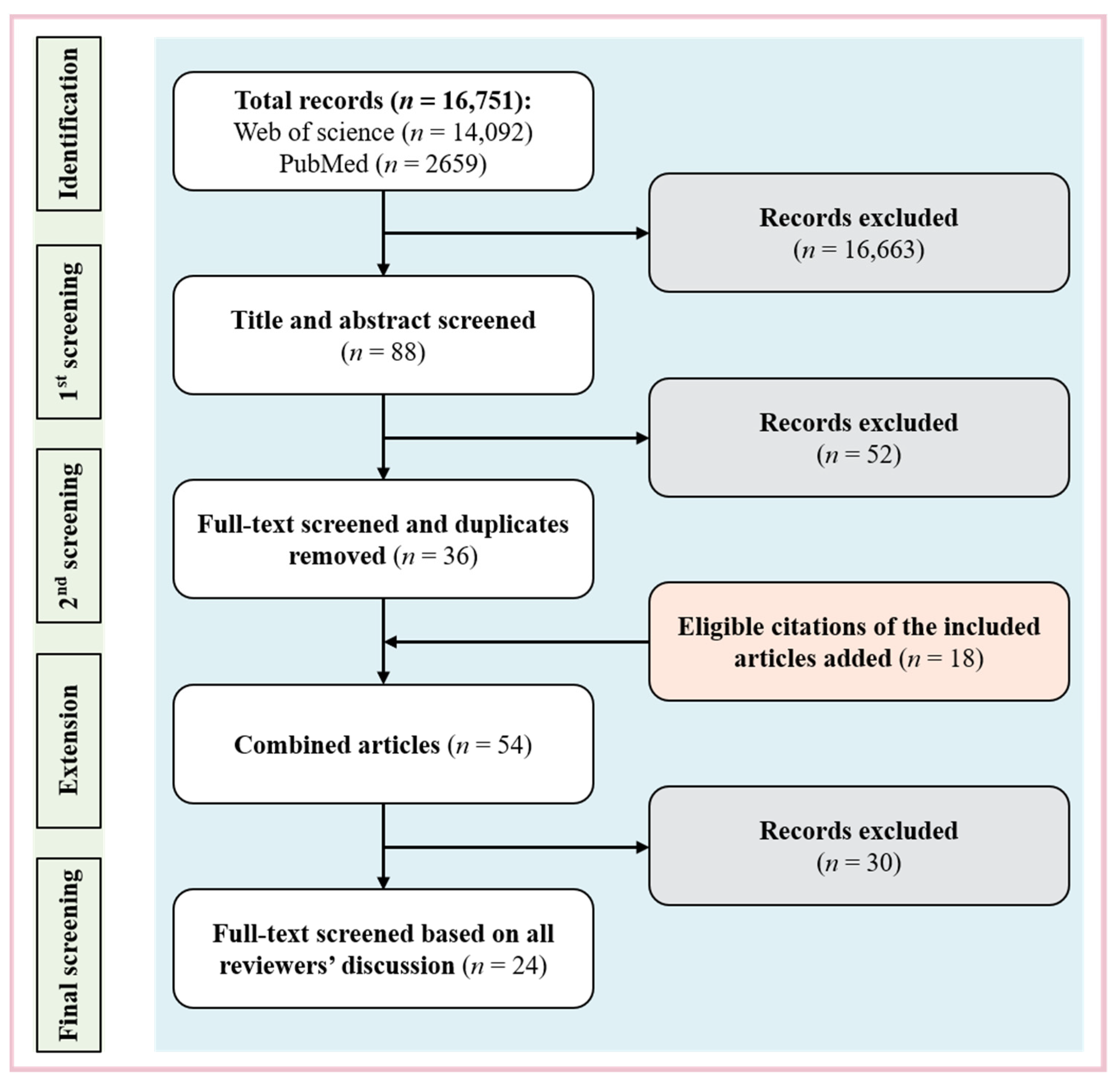
2. Methods
2.1. Data Source and Search Strategy
2.2. Eligibility Criteria
2.3. Study Inclusion
2.4. Analysis Strategy
3. Results
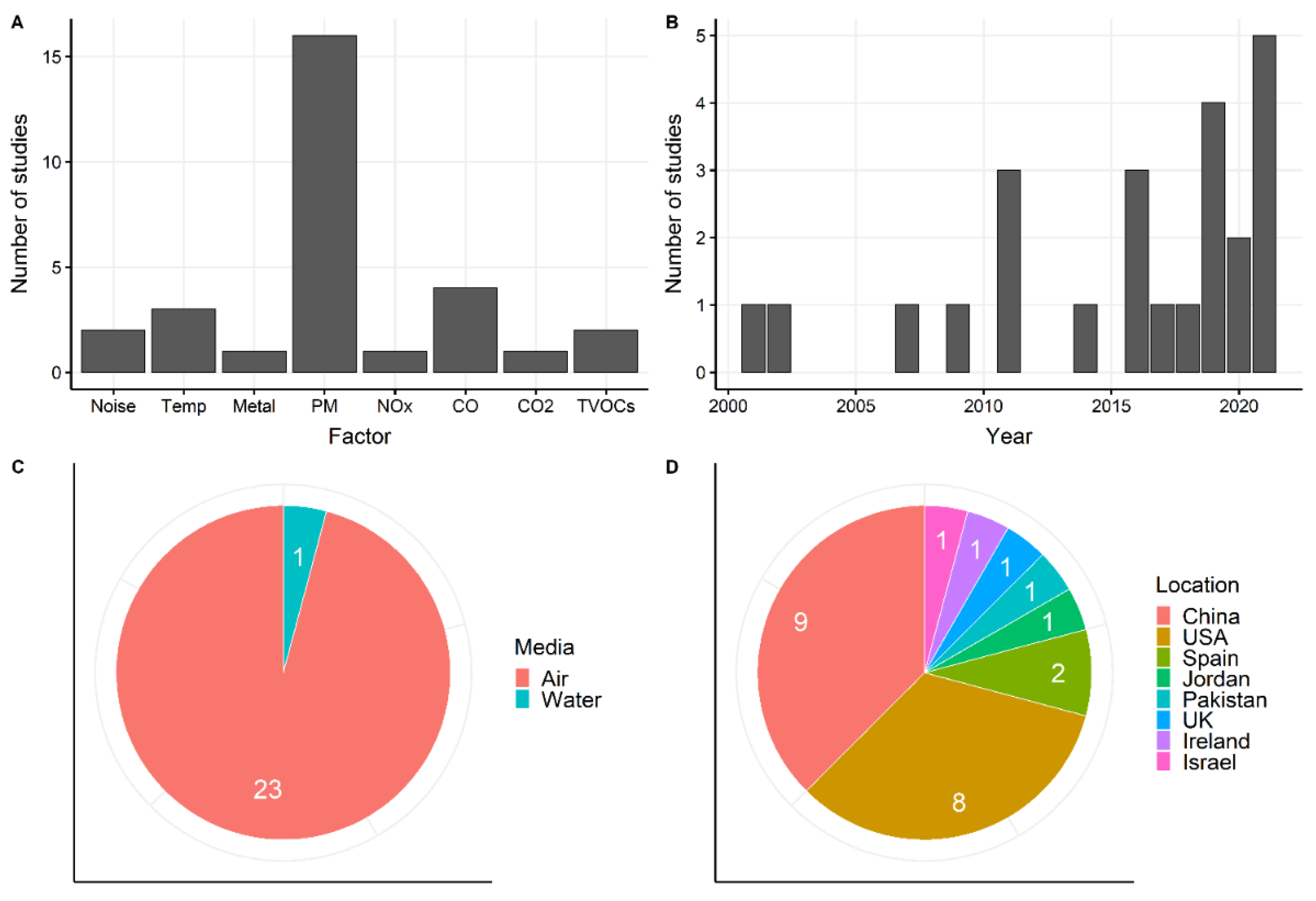
3.1. Overview
3.2. Physical Factors
3.2.1. Noise
3.2.2. Temperature
3.3. Chemical Factors
3.3.1. Gaseous Pollutants
- NOx.
- Carbon monoxide (CO) and carbon dioxide (CO2)
- Volatile Organic Compounds (VOCs)
3.3.2. Particles
3.3.3. Heavy Metals
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Institute for Health Metrics and Evaluation. Global Disease Burden (GBD) Compare. Available online: http://vizhub.healthdata.org/gbd-compare/ (accessed on 22 July 2022).
- Neira, M.; Prüss-Ustün, A. Preventing disease through healthy environments: A global assessment of the environmental burden of disease. Toxicol. Lett. 2016, 259, S1. [Google Scholar] [CrossRef]
- Pope III, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Shi, L.; Wu, X.; Yazdi, M.D.; Braun, D.; Awad, Y.A.; Wei, Y.; Liu, P.; Di, Q.; Wang, Y.; Schwartz, J. Long-term effects of PM2.5 on neurological disorders in the american medicare population: A longitudinal cohort study. Lancet Planet. Health 2020, 4, e557–e565. [Google Scholar] [CrossRef]
- Shi, L.; Steenland, K.; Li, H.; Liu, P.; Zhang, Y.; Lyles, R.H.; Requia, W.J.; Ilango, S.D.; Chang, H.H.; Wingo, T. A national cohort study (2000–2018) of long-term air pollution exposure and incident dementia in older adults in the United States. Nat. Commun. 2021, 12, 6754. [Google Scholar] [CrossRef]
- Kim, K.N.; Lim, Y.H.; Bae, H.J.; Kim, M.; Jung, K.; Hong, Y.C. Long-term fine particulate matter exposure and major depressive disorder in a community-based urban cohort. Environ. Health Perspect. 2016, 124, 1547–1553. [Google Scholar] [CrossRef] [Green Version]
- Power, M.C.; Kioumourtzoglou, M.-A.; Hart, J.E.; Okereke, O.I.; Laden, F.; Weisskopf, M.G. The relation between past exposure to fine particulate air pollution and prevalent anxiety: Observational cohort study. BMJ 2015, 350, h1111. [Google Scholar] [CrossRef] [Green Version]
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef] [Green Version]
- Pleban, F.T.; Oketope, O.; Shrestha, L. Occupational Styrene Exposure on Auditory Function among Adults: A Systematic Review of Selected Workers. Saf. Health Work 2017, 8, 329–336. [Google Scholar] [CrossRef]
- Khan, A.M.; Finlay, J.M.; Clarke, P.; Sol, K.; Melendez, R.; Judd, S.; Gronlund, C.J. Association between temperature exposure and cognition: A cross-sectional analysis of 20,687 aging adults in the United States. BMC Public Health 2021, 21, 1484. [Google Scholar] [CrossRef]
- Chen, N.-T.; Lin, P.-H.; Guo, Y.-L.L. Long-term exposure to high temperature associated with the incidence of major depressive disorder. Sci. Total Environ. 2019, 659, 1016–1020. [Google Scholar] [CrossRef]
- Zhang, S.; Yang, Y.; Xie, X.; Li, H.; Han, R.; Hou, J.; Sun, J.; Qian, Z.; Wu, S.; Huang, C.; et al. The effect of temperature on cause-specific mental disorders in three subtropical cities: A case-crossover study in China. Environ. Int. 2020, 143, 105938. [Google Scholar] [CrossRef]
- Riemersma-van der Lek, R.F.; Swaab, D.F.; Twisk, J.; Hol, E.M.; Hoogendijk, W.J.G.; Van Someren, E.J.W. Effect of bright light and melatonin on cognitive and noncognitive function in elderly residents of group care facilities—A randomized controlled trial. Jama-J. Am. Med. Assoc. 2008, 299, 2642–2655. [Google Scholar] [CrossRef]
- Xiang, J.; Weschler, C.J.; Wang, Q.; Zhang, L.; Mo, J.; Ma, R.; Zhang, J.; Zhang, Y. Reducing indoor levels of "outdoor PM2.5" in urban China: Impact on mortalities. Environ. Sci. Technol. 2019, 53, 3119–3127. [Google Scholar] [CrossRef]
- Xiang, J.; Weschler, C.J.; Zhang, J.; Zhang, L.; Sun, Z.; Duan, X.; Zhang, Y. Ozone in urban China: Impact on mortalities and approaches for establishing indoor guideline concentrations. Indoor Air 2019, 29, 604–615. [Google Scholar] [CrossRef]
- Xiang, J.; Seto, E.; Mo, J.; Zhang, J.; Zhang, Y. Impacts of implementing Healthy Building guidelines for daily PM2.5 limit on premature deaths and economic losses in urban China: A population-based modeling study. Environ. Int. 2021, 147, 106342. [Google Scholar] [CrossRef]
- Day, D.B.; Xiang, J.; Mo, J.; Li, F.; Chung, M.; Gong, J.; Weschler, C.J.; Ohman-Strickland, P.A.; Sundell, J.; Weng, W.; et al. Association of ozone exposure with cardiorespiratory pathophysiologic mechanisms in healthy adults. JAMA Intern. Med. 2017, 177, 1344–1353. [Google Scholar] [CrossRef]
- Day, D.; Xiang, J.; Mo, J.; Clyde, M.; Weschler, C.; Li, F.; Gong, J.; Chung, M.; Zhang, Y.; Zhang, J. Combined use of an electrostatic precipitator and a high-efficiency particulate air filter in building ventilation systems: Effects on cardiorespiratory health indicators in healthy adults. Indoor Air 2018, 28, 360–372. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, B.; Huang, C.; Yang, X.; Qian, H.; Deng, Q.; Zhao, Z.; Li, A.; Zhao, J.; Zhang, X. Ten cities cross-sectional questionnaire survey of children asthma and other allergies in China. Chin. Sci. Bull. 2013, 58, 4182–4189. [Google Scholar] [CrossRef] [Green Version]
- Lin, Z.; Chen, R.; Norback, D.; Liu, C.; Kan, H.; Deng, Q.; Huang, C.; Hu, Y.; Zou, Z.; Liu, W. The effects of PM2. 5 on asthmatic and allergic diseases or symptoms in preschool children of six Chinese cities, based on China, Children, Homes and Health (CCHH) project. Environ. Pollut. 2018, 232, 329–337. [Google Scholar]
- Vrijheid, M.; Casas, M.; Bergström, A.; Carmichael, A.; Cordier, S.; Eggesbø, M.; Eller, E.; Fantini, M.P.; Fernández, M.F.; Fernández-Somoano, A. European birth cohorts for environmental health research. Environ. Health Perspect. 2012, 120, 29–37. [Google Scholar] [CrossRef]
- Cui, X.; Li, F.; Xiang, J.; Fang, L.; Chung, M.K.; Day, D.B.; Mo, J.; Weschler, C.J.; Gong, J.; He, L.; et al. Cardiopulmonary effects of overnight indoor air filtration in healthy non-smoking adults: A double-blind randomized crossover study. Environ. Int. 2018, 114, 27–36. [Google Scholar] [CrossRef]
- Snyder, E.G.; Watkins, T.H.; Solomon, P.A.; Thoma, E.D.; Williams, R.W.; Hagler, G.S.W.; Shelow, D.; Hindin, D.A.; Kilaru, V.J.; Preuss, P.W. The changing paradigm of air pollution monitoring. Environ. Sci. Technol. 2013, 47, 11369–11377. [Google Scholar] [CrossRef]
- Hernandez-Gordillo, A.; Ruiz-Correa, S.; Robledo-Valero, V.; Hernandez-Rosales, C.; Arriaga, S. Recent advancements in low-cost portable sensors for urban and indoor air quality monitoring. Air Qual. Atmos. Health 2021, 14, 1931–1951. [Google Scholar] [CrossRef]
- Transparency Market Research. Smart/intelligent Sensors Market. Available online: https://www.transparencymarketresearch.com/smart-intelligent-sensor-market.html (accessed on 1 November 2022).
- Runkle, J.D.; Cui, C.; Fuhrmann, C.; Stevens, S.; Del Pinal, J.; Sugg, M.M. Evaluation of wearable sensors for physiologic monitoring of individually experienced temperatures in outdoor workers in southeastern US. Environ. Int. 2019, 129, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Sisto, R.; Cerini, L.; Gatto, M.P.; Gherardi, M.; Gordiani, A.; Sanjust, F.; Paci, E.; Tranfo, G.; Moleti, A. Otoacoustic emission sensitivity to exposure to styrene and noise. J. Acoust. Soc. Am. 2013, 134, 3739–3748. [Google Scholar] [CrossRef]
- Tang, C.-S.; Chuang, K.-J.; Chang, T.-Y.; Chuang, H.-C.; Chen, L.-H.; Lung, S.-C.C.; Chang, L.-T. Effects of personal exposures to micro- and nano-particulate matter, black carbon, particle-bound polycyclic aromatic hydrocarbons, and carbon monoxide on heart rate variability in a panel of healthy older subjects. Int. J. Env. Res. Public Health 2019, 16, 4672. [Google Scholar] [CrossRef] [Green Version]
- Borghi, F.; Spinazze, A.; Rovelli, S.; Campagnolo, D.; Del Buono, L.; Cattaneo, A.; Cavallo, D.M. Miniaturized monitors for assessment of exposure to air pollutants: A Review. Int. J. Environ. Res. Public Health 2017, 14, 909. [Google Scholar] [CrossRef] [Green Version]
- Morawska, L.; Thai, P.K.; Liu, X.T.; Asumadu-Sakyi, A.; Ayoko, G.; Bartonova, A.; Bedini, A.; Chai, F.H.; Christensen, B.; Dunbabin, M.; et al. Applications of low-cost sensing technologies for air quality monitoring and exposure assessment: How far have they gone? Environ. Int. 2018, 116, 286–299. [Google Scholar] [CrossRef]
- Longo, V.; Forleo, A.; Giampetruzzi, L.; Siciliano, P.; Capone, S. Human biomonitoring of environmental and occupational exposures by gc-ms and gas sensor systems: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 10236. [Google Scholar] [CrossRef] [PubMed]
- Ullo, S.L.; Sinha, G.R. Advances in smart environment monitoring systems using iot and sensors. Sensors 2020, 20, 3113. [Google Scholar] [CrossRef]
- Willner, M.R.; Vikesland, P.J. Nanomaterial enabled sensors for environmental contaminants. J. Nanobiotechnol. 2018, 16, 95. [Google Scholar] [CrossRef]
- Zhang, Z.; Amegbor, P.M.; Sabel, C.E. Assessing the current integration of multiple personalised wearable sensors for environment and health monitoring. Sensors 2021, 21, 7693. [Google Scholar] [CrossRef]
- Al Mamun, M.A.; Yuce, M.R. Sensors and systems for wearable environmental monitoring toward IoT-enabled applications: A review. IEEE Sens. J. 2019, 19, 7771–7788. [Google Scholar] [CrossRef]
- Meng, K.; Xiao, X.; Wei, W.; Chen, G.; Nashalian, A.; Shen, S.; Xiao, X.; Chen, J. Wearable pressure sensors for pulse wave monitoring. Adv. Mater. 2022, 34, e2109357. [Google Scholar] [CrossRef]
- Oh, H.S.; Lee, C.H.; Kim, N.K.; An, T.; Kim, G.H. Review: Sensors for biosignal/health monitoring in electronic skin. Polymers 2021, 13, 2478. [Google Scholar] [CrossRef]
- Chen, S.; Qi, J.; Fan, S.; Qiao, Z.; Yeo, J.C.; Lim, C.T. Flexible wearable sensors for cardiovascular health monitoring. Adv. Healthc. Mater. 2021, 10, e2100116. [Google Scholar] [CrossRef]
- Li, G.; Wen, D. Wearable biochemical sensors for human health monitoring: Sensing materials and manufacturing technologies. J. Mater. Chem. B 2020, 8, 3423–3436. [Google Scholar] [CrossRef] [PubMed]
- Nserat, S.; Al-Musa, A.; Khader, Y.S.; Abu Slaih, A.; Iblan, I. Blood pressure of jordanian workers chronically exposed to noise in industrial plants. Int. J. Occup. Environ. Med. 2017, 8, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Cole-Hunter, T.; Weichenthal, S.; Kubesch, N.; Foraster, M.; Carrasco-Turigas, G.; Bouso, L.; Martinez, D.; Westerdahl, D.; de Nazelle, A.; Nieuwenhuijsen, M. Impact of traffic-related air pollution on acute changes in cardiac autonomic modulation during rest and physical activity: A cross-over study. J. Expo. Sci. Environ. Epidemiol. 2016, 26, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Sugg, M.M.; Stevens, S.; Runkle, J.D. Estimating personal ambient temperature in moderately cold environments for occupationally exposed populations. Environ. Res. 2019, 173, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Samet, J.M. An exposure assessment study of ambient heat exposure in an elderly population in Baltimore, Maryland. Environ. Health Perspect. 2002, 110, 1219–1224. [Google Scholar] [CrossRef]
- WHO. Burden of Disease from Environmental Noise. In Quantification of Healthy Life Years Lost in Europe; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Abraham, Z.; Massawe, E.; Ntunaguzi, D.; Kahinga, A.; Mawala, S. Prevalence of noise-induced hearing loss among textile industry workers in Dar es Salaam, Tanzania. Ann. Glob. Health 2019, 85, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almaayeh, M.; Al-Musa, A.; Khader, Y.S. Prevalence of noise induced hearing loss among Jordanian industrial workers and its associated factors. Work 2018, 61, 267–271. [Google Scholar] [CrossRef]
- Watts, N.; Amann, M.; Ayeb-Karlsson, S.; Belesova, K.; Bouley, T.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; Chambers, J.; et al. The Lancet Countdown on health and climate change: From 25 years of inaction to a global transformation for public health. Lancet 2018, 391, 581–630. [Google Scholar] [CrossRef]
- O’Neill, M.S.; Ebi, K.L. Temperature extremes and health: Impacts of climate variability and change in the united states. J. Occup. Environ. Med. 2009, 51, 13–25. [Google Scholar] [CrossRef]
- Matt, F.; Cole-Hunter, T.; Donaire-Gonzalez, D.; Kubesch, N.; Martinez, D.; Carrasco-Turigas, G.; Nieuwenhuijsen, M. Acute respiratory response to traffic-related air pollution during physical activity performance. Environ. Int. 2016, 97, 45–55. [Google Scholar] [CrossRef]
- Tang, C.S.; Wu, T.Y.; Chuang, K.J.; Chang, T.Y.; Chuang, H.C.; Lung, S.C.C.; Chang, L.T. Impacts of in-cabin exposure to size-fractionated particulate matters and carbon monoxide on changes in heart rate variability for healthy public transit commuters. Atmosphere 2019, 10, 409. [Google Scholar] [CrossRef] [Green Version]
- Saadi, D.; Tirosh, E.; Schnell, I. The relationship between city size and carbon monoxide (CO) concentration and their effect on heart rate variability (HRV). Int. J. Environ. Res. Public Health 2021, 18, 788. [Google Scholar] [CrossRef]
- Deng, Y.; Liu, N.Y.; Tsow, F.; Xian, X.J.; Krajmalnik-Brown, R.; Tao, N.J.; Forzani, E. Tracking personal health-environment interaction with novel mobile sensing devices. Sensors 2018, 18, 2670. [Google Scholar] [CrossRef] [Green Version]
- Wong, T.W.; Wong, A.H.S.; Lee, F.S.C.; Qiu, H. Respiratory health and lung function in Chinese restaurant kitchen workers. Occup. Environ. Med. 2011, 68, 746–752. [Google Scholar] [CrossRef]
- Chen, R.; Yin, P.; Meng, X.; Wang, L.; Liu, C.; Niu, Y.; Lin, Z.; Liu, Y.; Liu, J.; Qi, J. Associations between ambient nitrogen dioxide and daily cause-specific mortality: Evidence from 272 Chinese cities. Epidemiology 2018, 29, 482–489. [Google Scholar] [CrossRef]
- Lu, P.; Zhang, Y.; Lin, J.; Xia, G.; Zhang, W.; Knibbs, L.D.; Morgan, G.G.; Jalaludin, B.; Marks, G.; Abramson, M. Multi-city study on air pollution and hospital outpatient visits for asthma in China. Environ. Pollut. 2020, 257, 113638. [Google Scholar] [CrossRef]
- Azuma, K.; Kagi, N.; Yanagi, U.; Osawa, H. Effects of low-level inhalation exposure to carbon dioxide in indoor environments: A short review on human health and psychomotor performance. Environ. Int. 2018, 121, 51–56. [Google Scholar] [CrossRef]
- Bourbeau, J.; Brisson, C.; Allaire, S. Prevalence of the sick building syndrome symptoms in office workers before and six months and three years after being exposed to a building with an improved ventilation system. Occup. Environ. Med. 1997, 54, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Zhou, C.S.; Li, S.J.; Wang, S.J. Examining the impacts of urban form on air pollution in developing countries: A case study of China’s megacities. Int. J. Environ. Res. Public Health 2018, 15, 1565. [Google Scholar] [CrossRef] [Green Version]
- Barn, P.; Giles, L.; Heroux, M.E.; Kosatsky, T. A review of the experimental evidence on the toxicokinetics of carbon monoxide: The potential role of pathophysiology among susceptible groups. Environ. Health 2018, 17, 13. [Google Scholar] [CrossRef] [Green Version]
- Tucciarone, M.; Dileo, P.A.; Castro, E.R.; Guerrero, M. Myocardial infarction secondary to carbon monoxide poisoning: An uncommon presentation of a common condition. Case report and review of the literature. Am. J. Ther. 2009, 16, 462–465. [Google Scholar] [CrossRef]
- WHO. The Cost of a Polluted Environment: 1.7 Million Child Deaths a Year. Available online: https://www.who.int/news/item/06-03-2017-the-cost-of-a-polluted-environment-1-7-million-child-deaths-a-year-says-who (accessed on 1 November 2022).
- Liu, N.; Bu, Z.; Liu, W.; Kan, H.; Zhao, Z.; Deng, F.; Huang, C.; Zhao, B.; Zeng, X.; Sun, Y.; et al. Health effects of exposure to indoor volatile organic compounds from 1980 to 2017: A systematic review and meta-analysis. Indoor Air 2022, 32, e13038. [Google Scholar] [CrossRef]
- Lee, D.H.; Kim, S.H.; Kang, S.H.; Kwon, O.K.; Park, J.J.; Yoon, C.H.; Cho, Y.S.; Heo, J.; Yi, S.M.; Youn, T.J.; et al. Personal exposure to fine particulate air pollutants impacts blood pressure and heart rate variability. Sci. Rep. 2020, 10, 16538. [Google Scholar] [CrossRef]
- Arvind, D.K.; Maiya, S.; Sedeno, P.A. Identifying causal relationships in time-series data from a pair of wearable sensors. In Proceedings of the 2021 IEEE 17th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Athens, Greece, 27–30 July 2021. [Google Scholar] [CrossRef]
- Tsou, M.C.M.; Lung, S.C.C.; Shen, Y.S.; Liu, C.H.; Hsieh, Y.H.; Chen, N.; Hwang, J.S. A community-based study on associations between PM2.5 and PM1 exposure and heart rate variability using wearable low-cost sensing devices. Environ. Pollut. 2021, 277, 116761. [Google Scholar] [CrossRef] [PubMed]
- Lung, S.C.C.; Chen, N.; Hwang, J.S.; Hu, S.C.; Wang, W.C.V.; Wen, T.Y.J.; Liu, C.H. Panel study using novel sensing devices to assess associations of PM(2.5) with heart rate variability and exposure sources. J. Expo. Sci. Environ. Epidemiol. 2020, 30, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Xing, X.L.; Liu, F.C.; Yang, X.L.; Liu, Q.; Wang, X.Y.; Lin, Z.N.; Huang, K.Y.; Cao, J.; Li, J.X.; Fan, M.; et al. Declines in heart rate variability associated with short-term PM2.5 exposure were modified by blood pressure control and treatment: A multi-city panel study in China. Environ. Pollut. 2021, 287, 117572. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Eum, K.D.; Rodrigues, E.G.; Magari, S.R.; Fang, S.C.; Modest, G.A.; Christiani, D.C. Effects of personal exposure to ambient fine particulate matter on acute change in nocturnal heart rate variability in subjects without overt heart disease. Am. J. Cardiol. 2016, 117, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, F.; Shaffer, M.L.; Li, X.A.; Rodriguez-Colon, S.; Wolbrette, D.L.; Williams, R.; Cascio, W.E.; Liao, D.P. Individual-level PM2.5 exposure and the time course of impaired heart rate variability: The APACR Study. J. Expo. Sci. Environ. Epidemiol. 2011, 21, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Li, L.Y.; Hu, D.Y.; Zhang, W.L.; Cui, L.Y.; Jia, X.; Yang, D.; Liu, S.; Deng, F.R.; Liu, J.X.; Guo, X.B. Effect of short-term exposure to particulate air pollution on heart rate variability in normal-weight and obese adults. Environ. Health 2021, 20, 29. [Google Scholar] [CrossRef]
- Magari, S.R.; Hauser, R.; Schwartz, J.; Williams, P.L.; Smith, T.J.; Christiani, D.C. Association of heart rate variability with occupational and environmental exposure to particulate air pollution. Circulation 2001, 104, 986–991. [Google Scholar] [CrossRef] [Green Version]
- Langrish, J.P.; Mills, N.L.; Chan, J.K.K.; Leseman, D.; Aitken, R.J.; Fokkens, P.H.B.; Cassee, F.R.; Li, J.; Donaldson, K.; Newby, D.E.; et al. Beneficial cardiovascular effects of reducing exposure to particulate air pollution with a simple facemask. Part Fibre Toxicol. 2009, 6, 8. [Google Scholar] [CrossRef] [Green Version]
- Tang, C.S.; Chang, L.T.; Lee, H.C.; Chan, C.C. Effects of personal particulate matter on peak expiratory flow rate of asthmatic children. Sci. Total Environ. 2007, 382, 43–51. [Google Scholar] [CrossRef]
- Nyhan, M.; McNabola, A.; Misstear, B. Comparison of particulate matter dose and acute heart rate variability response in cyclists, pedestrians, bus and train passengers. Sci. Total Environ. 2014, 468, 821–831. [Google Scholar] [CrossRef]
- Nafees, A.A.; Kazi, A.; Fatmi, Z.; Irfan, M.; Ali, A.; Kayama, F. Lung function decrement with arsenic exposure to drinking groundwater along River Indus: A comparative cross-sectional study. Environ. Geochem. Health 2011, 33, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Zahra, N.; Kalim, I.; Mahmood, M.; Naeem, N. Perilous effects of heavy metals contamination on human health. Pak. J. Anal. Environ. Chem. 2017, 18, 1–17. [Google Scholar] [CrossRef]
- Fu, Z.S.; Xi, S.H. The effects of heavy metals on human metabolism. Toxicol. Mech. Methods 2020, 30, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Bolte, J.F.B.; Clahsen, S.; Vercruijsse, W.; Houtveen, J.H.; Schipper, C.M.A.; van Kamp, I.; Bogers, R. Ecological momentary assessment study of exposure to radiofrequency electromagnetic fields and non-specific physical symptoms with self-declared electrosensitives. Environ. Int. 2019, 131, 104948. [Google Scholar] [CrossRef] [PubMed]
- Laeremans, M.; Dons, E.; Avila-Palencia, I.; Carrasco-Turigas, G.; Orjuela, J.P.; Anaya, E.; Cole-Hunter, T.; de Nazelle, A.; Nieuwenhuijsen, M.; Standaert, A.; et al. Short-term effects of physical activity, air pollution and their interaction on the cardiovascular and respiratory system. Environ. Int. 2018, 117, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Arlien-Soborg, M.C.; Schmedes, A.S.; Stokholm, Z.A.; Grynderup, M.B.; Bonde, J.P.; Jensen, C.S.; Hansen, A.M.; Frederiksen, T.W.; Kristiansen, J.; Christensen, K.L.; et al. Ambient and at-the-ear occupational noise exposure and serum lipid levels. Int. Arch. Occup. Environ. Health 2016, 89, 1087–1093. [Google Scholar] [CrossRef]
- Sinharay, R.; Gong, J.; Barratt, B.; Ohman-Strickland, P.; Ernst, S.; Kelly, F.J.; Zhang, J.J.; Collins, P.; Cullinan, P.; Chung, K.F. Respiratory and cardiovascular responses to walking down a traffic-polluted road compared with walking in a traffic-free area in participants aged 60 years and older with chronic lung or heart disease and age-matched healthy controls: A randomised, crossover study. Lancet 2018, 391, 339–349. [Google Scholar]
- Krewski, D.; Byus, C.V.; Glickman, B.W.; Lotz, W.C.; Mandeville, R.; Prato, F.S.; Weaver, D.F. Recent advances in research on radiofrequency fields and health. J. Toxicol. Environ. Health-Part B-Crit. Rev. 2001, 4, 145–159. [Google Scholar] [CrossRef]
- Modenese, A.; Korpinen, L.; Gobba, F. Solar radiation exposure and outdoor work: An underestimated occupational risk. Int. J. Environ. Res. Public Health 2018, 15, 2063. [Google Scholar] [CrossRef] [Green Version]
- Anenberg, S.C.; Haines, S.; Wang, E.; Nassikas, N.; Kinney, P.L. Synergistic health effects of air pollution, temperature, and pollen exposure: A systematic review of epidemiological evidence. Environ. Health 2020, 19, 130. [Google Scholar] [CrossRef]
- Mallires, K.R.; Wang, D.; Tipparaju, V.V.; Tao, N.J. Developing a low-cost wearable personal exposure monitor for studying respiratory diseases using metal-oxide sensors. IEEE Sens. J. 2019, 19, 8252–8261. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Chen, Z.; Song, Z.; Wang, C.; Wan, Z.a.; Chan, C.L.J.; Chen, Z.; Ye, W.; Fan, Z. Microheater integrated nanotube array gas sensor for parts-per-trillion level gas detection and single sensor-based gas discrimination. ACS Nano 2022, 16, 10968–10978. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Ye, W.; Chen, Z.; Chen, Z.; Li, M.; Tang, W.; Wang, C.; Wan, Z.a.; Poddar, S.; Wen, X. Wireless self-powered high-performance integrated nanostructured-gas-sensor network for future smart homes. ACS Nano 2021, 15, 7659–7667. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Sikarwar, S.; Verma, A.; Yadav, B.C. The recent development of metal oxide heterostructures based gas sensor, their future opportunities and challenges: A review. Sens. Actuators A Phys. 2021, 332, 113127. [Google Scholar] [CrossRef]
- Menger, R.F.; Funk, E.; Henry, C.S.; Borch, T. Sensors for detecting per-and polyfluoroalkyl substances (PFAS): A critical review of development challenges, current sensors, and commercialization obstacles. Chem. Eng. J. 2021, 417, 129133. [Google Scholar] [CrossRef]
- Shen, Y.; Wei, Y.; Zhu, C.; Cao, J.; Han, D.-M. Ratiometric fluorescent signals-driven smartphone-based portable sensors for onsite visual detection of food contaminants. Coord. Chem. Rev. 2022, 458, 214442. [Google Scholar] [CrossRef]
- Umapathi, R.; Raju, C.V.; Ghoreishian, S.M.; Rani, G.M.; Kumar, K.; Oh, M.-H.; Park, J.P.; Huh, Y.S. Recent advances in the use of graphitic carbon nitride-based composites for the electrochemical detection of hazardous contaminants. Coord. Chem. Rev. 2022, 470, 214708. [Google Scholar] [CrossRef]
- Umapathi, R.; Ghoreishian, S.M.; Sonwal, S.; Rani, G.M.; Huh, Y.S. Portable electrochemical sensing methodologies for on-site detection of pesticide residues in fruits and vegetables. Coord. Chem. Rev. 2022, 453, 214305. [Google Scholar] [CrossRef]
- Byrom, B.; McCarthy, M.; Schueler, P.; Muehlhausen, W. Brain monitoring devices in neuroscience clinical research: The potential of remote monitoring using sensors, wearables, and mobile devices. Clin. Pharmacol. Ther. 2018, 104, 59–71. [Google Scholar] [CrossRef] [Green Version]
- Cappon, G.; Vettoretti, M.; Sparacino, G.; Facchinetti, A. Continuous glucose monitoring sensors for diabetes management: A review of technologies and applications. Diabetes Metab. J. 2019, 43, 383–397. [Google Scholar] [CrossRef]
- Comini, E. Metal oxide nanowire chemical sensors: Innovation and quality of life. Mater. Today 2016, 19, 559–567. [Google Scholar] [CrossRef]
- Demanega, I.; Mujan, I.; Singer, B.C.; Anđelković, A.S.; Babich, F.; Licina, D. Performance assessment of low-cost environmental monitors and single sensors under variable indoor air quality and thermal conditions. Build. Environ. 2020, 187, 107415. [Google Scholar] [CrossRef]
- Levy Zamora, M.; Xiong, F.; Gentner, D.; Kerkez, B.; Kohrman-Glaser, J.; Koehler, K. Field and laboratory evaluations of the low-cost Plantower particulate matter sensor. Environ. Sci. Technol. 2019, 53, 838–849. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Chen, F.; Cai, Y.; Fan, S.; Cai, J.; Chen, R.; Kan, H.; Lu, Y.; Zhao, Z. Validation of a light-scattering PM2.5 sensor monitor based on the long-term gravimetric measurements in field tests. PLoS ONE 2017, 12, e0185700. [Google Scholar] [CrossRef]
- Wang, Z.; Delp, W.W.; Singer, B.C. Performance of low-cost indoor air quality monitors for PM2.5 and PM10 from residential sources. Build. Environ. 2020, 171, 106654. [Google Scholar] [CrossRef]
- Zusman, M.; Shappard, L.; Larson, T.; Seto, E.; Spalt, E.; Gassett, A.; Schumacher, C.; Carvlin, G.; Austin, E.; Kaufman, J. Calibration of low-cost particulate matter sensors: Model development for a multi-city epidemiological study. Environ. Int. 2019, 134, 105329. [Google Scholar] [CrossRef]
- Maag, B.; Zhou, Z.M.; Thiele, L. A survey on sensor calibration in air pollution monitoring deployments. IEEE Internet Things J. 2018, 5, 4857–4870. [Google Scholar] [CrossRef] [Green Version]
- Honicky Jr, R. Understanding and using rendezvous to enhance mobile crowdsourcing applications. Computer 2011, 44, 22–28. [Google Scholar] [CrossRef]
- Xiang, J.; Austin, E.; Gould, T.; Larson, T.V.; Yost, M.; Shirai, J.H.; Liu, Y.; Yun, S.; Seto, E. Using vehicles’ rendezvous for in-situ calibration of instruments in fleet vehicle-based air pollution mobile monitoring. Environ. Sci. Technol. 2020, 54, 4286–4294. [Google Scholar] [CrossRef]
- Dons, E.; Laeremans, M.; Orjuela, J.P.; Avila-Palencia, I.; Carrasco-Turigas, G.; Cole-Hunter, T.; Anaya-Boig, E.; Standaert, A.; De Boever, P.; Nawrot, T.; et al. Wearable sensors for personal monitoring and estimation of inhaled traffic-related air pollution: Evaluation of methods. Environ. Sci. Technol. 2017, 51, 1859–1867. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Location | Scenario | Period | Subject | Exposure Measurement | Health Measurement | Number of Records | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Nserat et al. [41] | Jordan | Industrial plants | 2017 | 191 male workers | Noise level: Casella sound level meter CEL-450A, ~USD 4000 | Blood pressure (BP): KaWe Mastermed A2 Aneroid BP Monitor, ~USD 43 | One time for each subject | Exposure to a high level of noise was associated with elevated blood pressure. |
| Cole-Hunter et al. [42] | Spain | Traffic | 2011 | 28 healthy non-smoking adults | Noise level (LAeq): CESVA sound level meter SC160 | Heart rate (HR), heart rate variability (HRV): Gem-Med Holter monitor CardioLight | 8 h for each subject | Not presented. |
| Runkle et al. [27] | USA | Occupational | 2016 | 35 outdoors workers | Ambient temperature: Thermochron iButton DS 1921G, ~USD 50 | HR: Garmin vivoActive HR watches, ~USD 1500 | 5 days for each subject | The association between increasing temperature and heat strain was nonlinear and exhibited a U-shaped relationship. |
| Sugg et al. [43] | USA | Occupational | 2018 | 54 outdoors workers | Ambient temperature, solar radiation intensity: Thermochron iButton DS 1921G, ~USD 50 | HR: Garmin vivoActive HR watches, ~USD 1500 | 1 week for each subject | A weak significant relationship was observed between personal ambient temperatures and weather station measurements. |
| Basu and Samet [44] | USA | Daily routine | 2000 | 42 elderly residents | Ambient temperature: unknown temperature sensor probes | HR, body temperature: unknown polar chest strap, temperature sensor probes, mercury detectors | 48 h for each subject | Body temperature was not associated with ground station temperature. |
| Study | Location | Scenario | Period | Subject | Exposure Measurement | Health Measurement | Number of Records | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Matt et al. [50] | Spain | Traffic | 2013–2014 | 30 healthy adults | NOx: 2B Tech. Model 410 Nitric Oxide Monitor, ~USD 8000 | Respiratory function: Ndd Medical EasyOne spirometer, ~USD 1900 | 8 h for each subject | Associations between NOx exposure and respiratory measures were modified by participants’ physical activity levels. |
| Tang et al. [29] | China | Daily life | 2012–2013 | 7 healthy older people | CO: TSI Q-TRAK model 7575, ~USD 4300 | HRV: MSI ECG recorder and analyzer model E3-8010 | 144 h for each subject | Exposure to CO had a lagged effect of 0–7 h on HRV for elders. |
| Tang et al. [51] | China | Traffic | 2009–2010 | 20 college students | CO: Dräger PAC III CO detection instrument, ~USD 900 | HRV: MSI ECG recorder and analyzer model E3-8010 | 48 h for each subject | Exposure to CO had a > 4 h lagged effect on HRV for young people. |
| Saadi et al. [52] | Israel | Daily life | Not mentioned | 44 healthy women | CO: Dräger PAC III CO detection instrument, ~USD 900 | HRV: Polar 810i monitor | 48 h for each subject | Short-term exposure to CO below 7 ppm was related to declined HRV. |
| Deng et al. [53] | USA | Working and resting | 2016 | 17 workers | TVOC: Self-made portable wireless VOC monitoring device | Individual resting metabolic rate (RMR): Breezing Indirect Calorimeter, ~USD 550 | 2 h for each subject | No obvious correlation between VOCs exposure and RMR was found. |
| Wong et al. [54] | China | Chinese restaurant kitchens | Not mentioned | 393 kitchen workers | CO, CO2: TSI Q-Trak Model 8554, TVOC: RAE Systems PGM-7240, ~USD 1200 | Respiratory function: Vitalograph 2160 | 2 h for each subject | Exposure to toxic air pollutants in kitchens led to worse lung functions and higher prevalence of respiratory symptoms. |
| Study | Location | Scenario | Period | Subject | Exposure Measurement | Health Measurement | Number of Records | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Lee et al. [64] | Korea | Daily life | 2018–2019 | 22 healthy adults | PM2.5: Dylos DC1700 | BP: IEM Mobil-O Graph Ambulatory BP monitor HR and HRV: Aria Del Mar Reynolds Medical ECG monitor | 24 h for each subject | Short-term exposure to PM2.5 was associated with decreased HRV. |
| Tang et al. [29] | China | Daily life | 2012–2013 | 7 healthy older adults | UFPs: DiSCmini PM2.5 and PM10: Grimm PAS Model 1.109 BC: MicroAeth model AE51 p-PAHs: EcoChem Photoelectric sensor PAS2000CE | HRV: MSI ECG Model E3-8010 | 144 h for each subject | Different pollutants showed different lagged effects on HRV. |
| Tsou et al. [66] | China | Daily life | 2018–2019 | 35 healthy adults | PM1 and PM2.5: Self-made box with PlanTower PMS sensor | HRV: RootiRx | 48 h for each subject | Short-term exposure to PM2.5 had 6–18 h lagged effects on overweight people’s HRV. |
| Cole-Hunter et al. [42] | Spain | Traffic | 2011 | 28 healthy non-smoking adults | UFPs: TSI CPC Model 3007 PM2.5: TSI DusTrak Model 8532 BC: MicroAeth model AE51 | HR and HRV: Gem-Med Holter monitor CardioLight | 8 h for each subject | Exposure to TRAP shows a rapid but nonlinear impact on HRV in healthy adults. |
| He et al. [70] | USA | Daily life | 2007–2009 | 106 healthy non-smoking elders | PM2.5: Thermo Scientific Personal DataRam pDR model 1200 | HR: Mortara 12-lead HScribe Holter System | 24 h for each subject | PM2.5 exposure was related to HRV, with the largest effects occurring about 4–6 h lagged. |
| Lee et al. [69] | USA | Daily life | 2004 | 21 healthy adults | PM2.5: TSI SidePak AM510 | HR and HRV: Raytel Cardiac Services ECG Holter | 48 h for each subject | Short-term exposure to PM2.5 showed a lag effect on people’s HRV up to 2.5 h. |
| Li et al. [71] | China | Daily life | 2017–2018 | 97 young adults | PM2.5: RTI MicroPEM BC: MicroAeth model AE51 | HR and HRV: DM Software Inc. 12-channel Holter recorder MGY-H12 | 24 h for each subject | PM2.5/BC exposure showed lag effects on obese people’s HRV and HR at least within 3 h. |
| Lung et al. [67] | China | Daily life | Not mentioned | 36 healthy non-smoking adults | PM2.5: Self-made box with PlanTower PMS sensor | HRV: RootiRx | 48–96 h for each subject | Short-term exposure to low-level PM2.5 (<10 µg/m3) was related to HRV. |
| Magari et al. [72] | USA | Industrial plants | Not mentioned | 40 male workers | PM2.5: TSI DustTrak 8534 | HRV: Dynacord 3-channel device 423 | up to 24 h for each subject | Occupational and environmental PM2.5 exposure within minutes to hours was related to HRV. |
| Langrish et al. [73] | China | Daily life | 2008 | 15 healthy non-smoking volunteers | PM2.5: Thermo Scientific DataRAM monitor pDR-1500 | HRV: Spacelabs Holter monitor Lifecard | 24 h for each subject | Wearing a mask for 2 h tended to eliminate the adverse effects of air pollution on blood pressure and HRV. |
| Matt et al. [50] | Spain | Traffic | 2013–2014 | 30 healthy non-smoking adults | UFPs: TSI CPC 3007 PM2.5 and PM10: TSI DustTrack 8534 | HR: Gem-Med Holter monitor CardioLight Respiratory function: Ndd Medical EasyOne spirometer | 8 h for each subject | Associations between various pollutant exposures and respiratory measures were modified by participants’ physical activity levels. |
| Tang et al. [51] | China | Traffic | 2009–2010 | 20 healthy college students | PM1, PM2.5, and PM10: GRIMM PAS Model 1.108 | HRV: MSI ECG Model E3-8010 | 48 h for each subject | Exposure to PM2.5–10, among all size-fractional particles, led to the largest variations in HRV. |
| Tang et al. [74] | China | Daily life | 2003–2005 | 30 children with asthma | PM1, PM2.5, and PM10: GRIMM PAS Model 1.108 | Peak expiratory flow rate (PEFR): Microlife Electronic PEFR monitor PF-100 | 14 h for each subject | PM exposure showed lagged and cumulative effects on the decrements in morning PEFR. |
| Arvind et al. [65] | Greece | Daily life | Not mentioned | 44 asthmatic subjects | PM2.5: Airpseck sensor (self-made) | Respiratory rate: Respeck sensor (self-made) | 48 h for each subject | Short-term exposure to PM2.5 showed lagged effects on respiratory rates of asthmatic adolescents |
| Xing et al. [68] | China | Daily life | 2017–2019 | 282 hypertension patients | PM2.5: RTI MicroPEM and TSI SidePak AM520 | HRV: 12-lead Holter device. JincoMed | 3 days for each subject | Short-term exposure to PM2.5 was related to HRV; BP control and ARB treatment alleviated the adverse effects. |
| Nyhan et al. [75] | Ireland | Traffic | Not mentioned | 32 young, healthy subjects | PM1, PM2.5, PM7, PM10, and TSP: Met One Aerocet 531 | HRV: CamNtech Actiheart units | 8–10 h for each subject | Short-term exposure to PM2.5 was related to HRV decline for commuters. |
| Nafees et al. [76] | Pakistan | Drinking groundwater | 2009 | 100 subjects ≥15 yrs | Water Arsenic: Industrial Test Systems, Inc. Arsenic Quick Kit | Lung function: Vitalograph New Alpha 6000 spirometer | One time for each subject | Chronic exposure to arsenic in drinking groundwater was associated with a decrement in lung function. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, X.; Luo, J.; Liao, M.; Su, Y.; Lv, M.; Li, Q.; Xiao, S.; Xiang, J. Wearable Sensor-Based Monitoring of Environmental Exposures and the Associated Health Effects: A Review. Biosensors 2022, 12, 1131. https://doi.org/10.3390/bios12121131
Lin X, Luo J, Liao M, Su Y, Lv M, Li Q, Xiao S, Xiang J. Wearable Sensor-Based Monitoring of Environmental Exposures and the Associated Health Effects: A Review. Biosensors. 2022; 12(12):1131. https://doi.org/10.3390/bios12121131
Chicago/Turabian StyleLin, Xueer, Jiaying Luo, Minyan Liao, Yalan Su, Mo Lv, Qing Li, Shenglan Xiao, and Jianbang Xiang. 2022. "Wearable Sensor-Based Monitoring of Environmental Exposures and the Associated Health Effects: A Review" Biosensors 12, no. 12: 1131. https://doi.org/10.3390/bios12121131