A Validation Study of a Commercial Wearable Device to Automatically Detect and Estimate Sleep

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Laboratory Setting
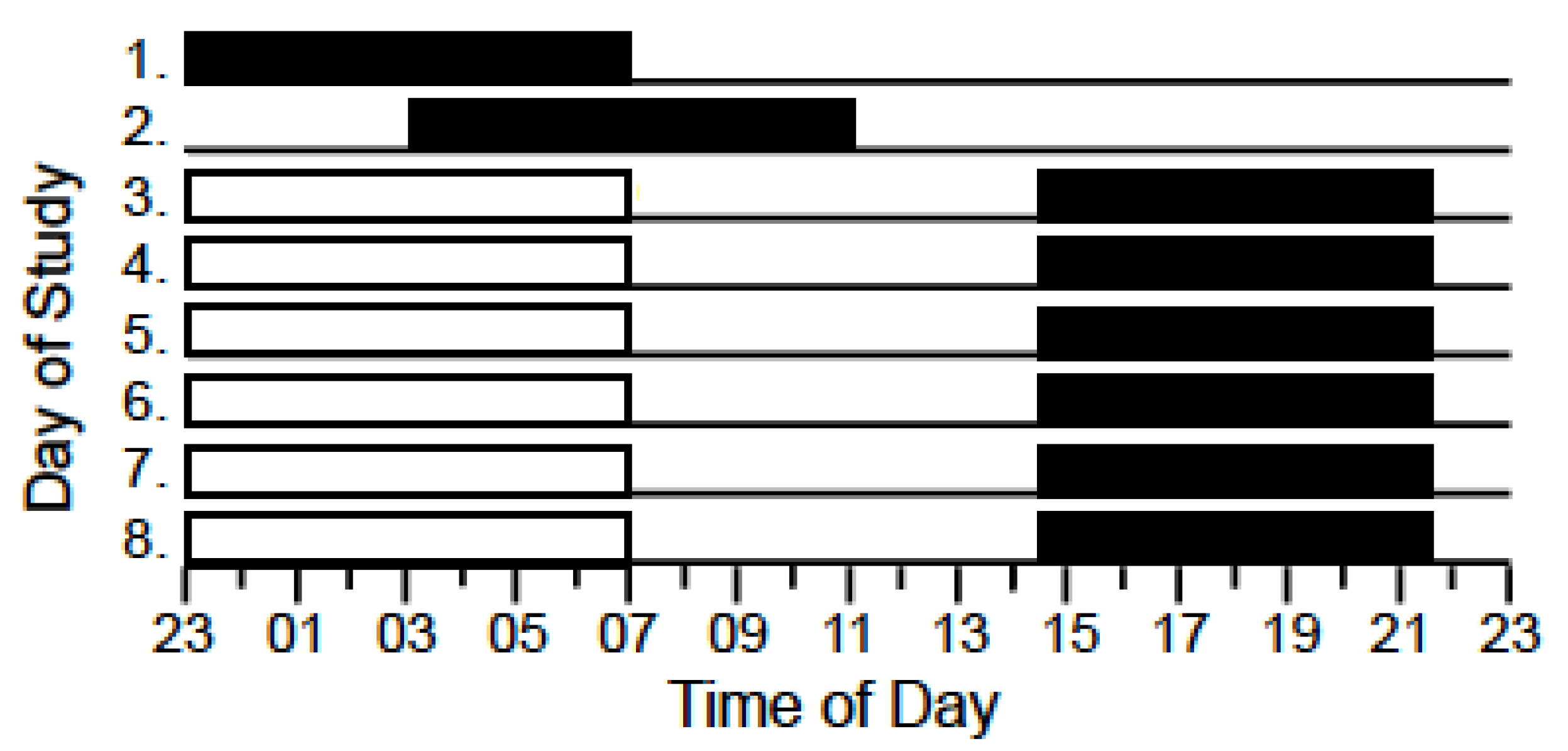
2.3. Design
2.4. Measures and Procedure
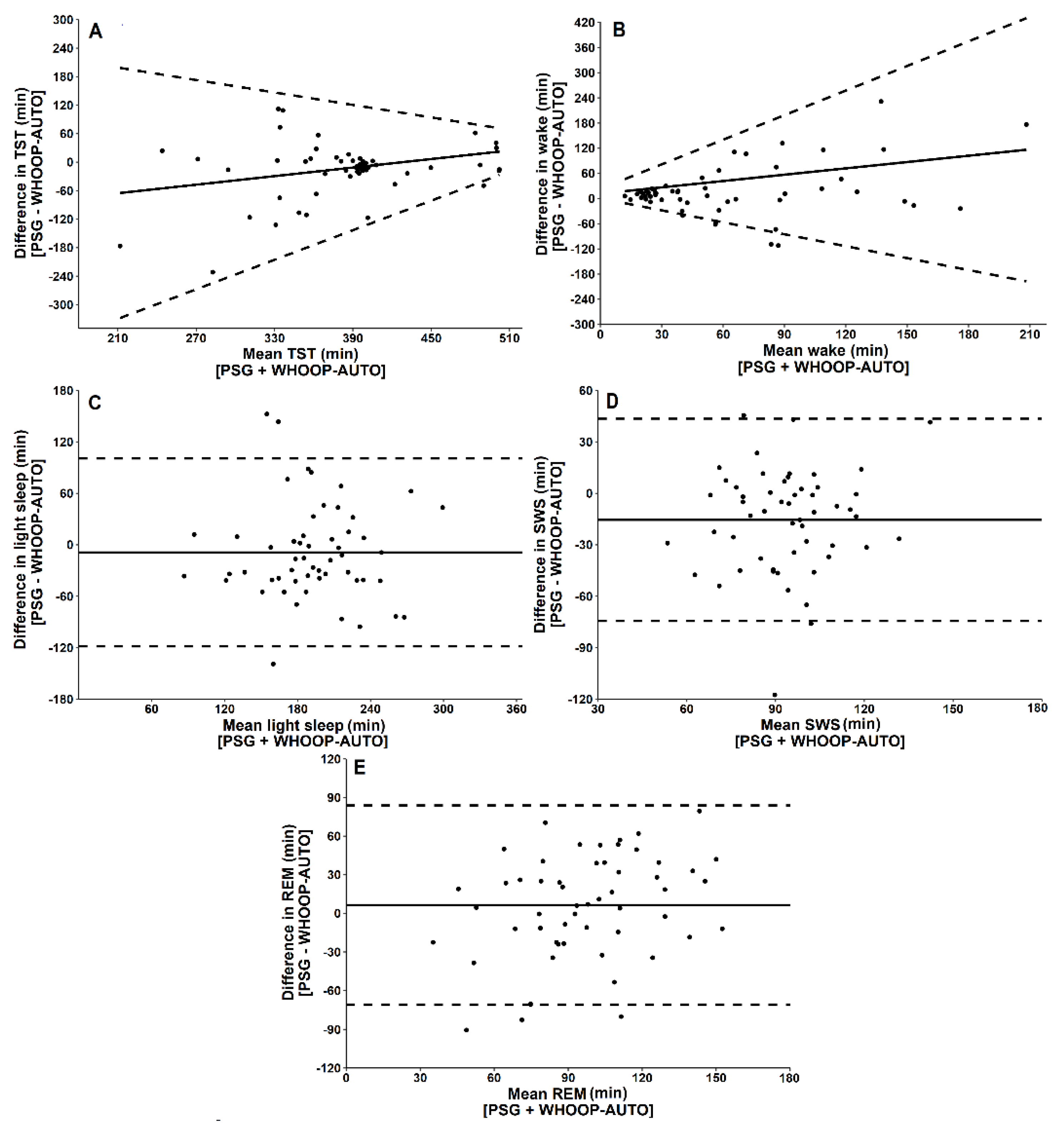
- Total sleep time (TST): the sum of minutes spent in any stage of sleep (N1, N2, N3, REM).
- Wake: the sum of minutes spent awake during the sleep opportunity.
- Light sleep: the sum of minutes spent in stage N1 or N2 sleep.
- Slow wave sleep (SWS): the sum of minutes spent in stage N3 sleep.
- Rapid eye movement sleep (REM): the sum of minutes spent in stage REM.
- Sleep onset latency (SOL): the duration of time from lights out to the first epoch of any stage of sleep.
3. Data Analysis
- Sensitivity: the percentage of PSG-determined sleep epochs correctly identified as sleep by each method;
- Specificity: the percentage of PSG-determined wake epochs correctly identified as wake by each method;
- Agreement: the percentage of PSG-determined sleep and wake epochs correctly identified as sleep or wake by each method.
- Sensitivity for wake: the percentage of PSG-determined wake epochs correctly identified as wake by each method;
- Sensitivity for light sleep: the percentage of PSG-determined N1 and N2 epochs correctly identified as light sleep by each method;
- Sensitivity for SWS: the percentage of PSG-determined N3 epochs correctly identified as SWS by each method;
- Sensitivity for REM: the percentage of PSG-determined REM epochs correctly identified as REM by each method;
- Agreement: the percentage of PSG-determined N1, N2, REM, and wake epochs correctly identified as light sleep, deep sleep, REM, or wake by each method.
4. Result
5. Discussion
5.1. Two-Stage Categorisation of Sleep
5.2. Four-Stage Categorisation of Sleep
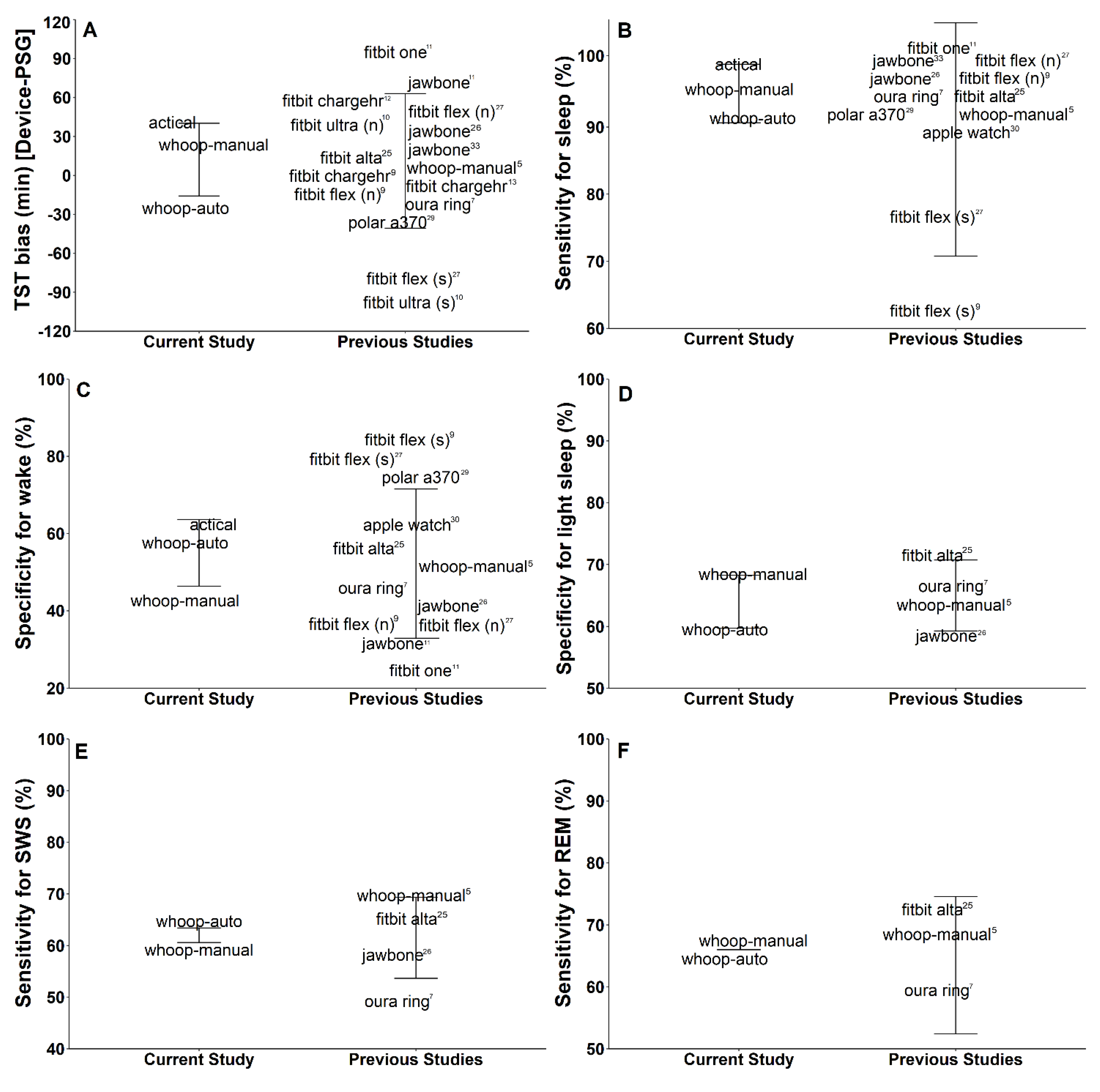
5.3. Comparison to Other Sleep Wearables
5.4. Boundary Conditions and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kushida, C.A.; Littner, M.R.; Morgenthaler, T.; Alessi, C.A.; Bailey, D.; Coleman, J.; Friedman, L.; Hirshkowitz, M.; Kapen, S.; Kramer, M.; et al. Practice parameters for the indications for polysomnography and related procedures: An update for 2005. Sleep 2005, 28, 499–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, H.; Shin, K.; Shin, C. ‘Development of the Sleep Quality Scale’: Erratum. J. Sleep Res. 2006, 15, 465. [Google Scholar] [CrossRef] [PubMed]
- Zambotti, M.; Cellini, N.; Goldstone, A.; Colrain, I.M.; Baker, F.C. Wearable Sleep Technology in Clinical and Research Settings. Med. Sci. Sports Exerc. 2019, 51, 1538–1557. [Google Scholar] [CrossRef] [PubMed]
- Pollak, C.P.; Tryon, W.W.; Nagaraja, H.; Dzwonczyk, R. How accurately does wrist actigraphy identify the states of sleep and wakefulness? Sleep 2001, 24, 957–965. [Google Scholar] [CrossRef]
- Miller, D.J.; Lastella, M.; Scanlan, A.T.; Bellenger, C.; Halson, S.L.; Roach, G.D.; Sargent, C. A validation study of the WHOOP strap against polysomnography to assess sleep. J. Sports Sci. 2020, 38, 2631–2636. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.K.; Pu, Y. Heart rate variability, sleep and sleep disorders. Sleep Med. Rev. 2012, 16, 47–66. [Google Scholar] [CrossRef]
- De Zambotti, M.; Rosas, L.; Colrain, I.M.; Baker, F.C. The Sleep of the Ring: Comparison of the OURA Sleep Tracker against Polysomnography. Behav. Sleep Med. 2019, 17, 124–136. [Google Scholar] [CrossRef]
- De Zambotti, M.; Baker, F.C.; Willoughby, A.R.; Godino, J.G.; Wing, D.; Patrick, K.; Colrain, I.M. Measures of sleep and cardiac functioning during sleep using a multi-sensory commercially-available wristband in adolescents. Physiol. Behav. 2016, 158, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.G.; Kang, J.M.; Ko, K.P.; Park, S.C.; Mariani, S.; Weng, J. Validity of a commercial wearable sleep tracker in adult insomnia disorder patients and good sleepers. J. Psychosom. Res. 2017, 97, 38–44. [Google Scholar] [CrossRef]
- Meltzer, L.J.; Hiruma, L.S.; Avis, K.; Montgomery-Downs, H.; Valentin, J. Comparison of a Commercial Accelerometer with Polysomnography and Actigraphy in Children and Adolescents. Sleep 2015, 38, 1323–1330. [Google Scholar] [CrossRef] [Green Version]
- Maskevich, S.; Jumabhoy, R.; Dao, P.D.M.; Stout, J.C.; Drummond, S.P.A. Pilot Validation of Ambulatory Activity Monitors for Sleep Measurement in Huntington’s Disease Gene Carriers. J. Huntingt. Dis. 2017, 6, 249–253. [Google Scholar] [CrossRef]
- Sargent, C.; Lastella, M.; Romyn, G.; Versey, N.; Miller, D.J.; Roach, G.D. How well does a commercially available wearable device measure sleep in young athletes? Chronobiol. Int. 2018, 35, 754–758. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.A. Patient non-compliance with paper diaries. BMJ 2002, 324, 1193–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saw, A.E.; Main, L.C.; Gastin, P.B. Monitoring athletes through self-report: Factors influencing implementation. J. Sports Sci. 2015, 14, 137–146. [Google Scholar]
- Miller, D.J.; Sargent, C.; Roach, G.D.; Scanlan, A.T.; Vincent, G.E.; Lastella, M. Moderate-intensity exercise performed in the evening does not impair sleep in healthy males. Eur. J. Sport Sci. 2019, 20, 80–89. [Google Scholar] [CrossRef]
- Iber, C.; Ancoli-Israel, S.; Chesson, A.; Quan, S. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology, and Technical Specifications; American Academy of Sleep Medicine: Westchester, IL, USA, 2007. [Google Scholar]
- Kosmadopoulos, A.; Sargent, C.; Darwent, D.; Zhou, X.; Roach, G.D. Alternatives to polysomnography (PSG): A validation of wrist actigraphy and a partial-PSG system. Behav. Res. Methods 2014, 46, 1032–1041. [Google Scholar] [CrossRef]
- Sargent, C.; Lastella, M.; Halson, S.L.; Roach, G.D. The validity of activity monitors for measuring sleep in elite athletes. J. Sci. Med. Sport 2016, 19, 848–853. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Agreement between methods of measurement with multiple observations per individual. J. Biopharm. Stat. 2007, 17, 571–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludbrook, J. Confidence in Altman-Bland plots: A critical review of the method of differences. Clin. Exp. Pharmacol. Physiol. 2010, 37, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.; Wright, C.C. The Kappa Statistic in Reliability Studies: Use, Interpretation, and Sample Size Requirements. Phys. Ther. 2005, 85, 257–268. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284. [Google Scholar] [CrossRef]
- Cook, J.D.; Eftekari, S.C.; Dallmann, E.; Sippy, M.; Plante, D.T. Ability of the Fitbit Alta HR to quantify and classify sleep in patients with suspected central disorders of hypersomnolence: A comparison against polysomnography. J. Sleep Res. 2019, 28, e12789. [Google Scholar] [CrossRef]
- Cook, J.D.; Prairie, M.L.; Plante, D.T. Ability of the Multisensory Jawbone UP3 to Quantify and Classify Sleep in Patients with Suspected Central Disorders of Hypersomnolence: A Comparison Against Polysomnography and Actigraphy. J. Clin. Sleep Med. 2018, 14, 841–848. [Google Scholar] [CrossRef]
- Cook, J.D.; Prairie, M.L.; Plante, D.T. Utility of the Fitbit Flex to evaluate sleep in major depressive disorder: A comparison against polysomnography and wrist-worn actigraphy. J. Affect Disord. 2017, 217, 299–305. [Google Scholar] [CrossRef]
- De Zambotti, M.; Goldstone, A.; Claudatos, S.; Colrain, I.M.; Baker, F.C. A validation study of Fitbit Charge 2™ compared with polysomnography in adults. Chronobiol. Int. 2018, 35, 465–476. [Google Scholar] [CrossRef]
- Pesonen, A.K.; Kuula, L. The Validity of a New Consumer-Targeted Wrist Device in Sleep Measurement: An Overnight Comparison against Polysomnography in Children and Adolescents. J. Clin. Sleep Med. 2018, 14, 585–591. [Google Scholar] [CrossRef] [Green Version]
- Walch, O.; Huang, Y.; Forger, D.; Goldstein, C. Sleep stage prediction with raw acceleration and photoplethysmography heart rate data derived from a consumer wearable device. Sleep 2019, 42, zsz180. [Google Scholar] [CrossRef]
- De Zambotti, M.; Baker, F.C.; Colrain, I.M. Validation of Sleep-Tracking Technology Compared with Polysomnography in Adolescents. Sleep 2015, 38, 1461–1468. [Google Scholar] [CrossRef]
- Halson, S.L. Sleep Monitoring in Athletes: Motivation, Methods, Miscalculations and Why it Matters. Sports Med. 2019, 49, 1487–1497. [Google Scholar] [CrossRef] [PubMed]
- Magalang, U.J.; Chen, N.H.; Cistulli, P.A.; Fedson, A.C.; Gíslason, T.; Hillman, D.; Penzel, T.; Tamisier, R.; Tufik, S.; Phillips, G.; et al. Agreement in the scoring of respiratory events and sleep among international sleep centers. Sleep 2013, 36, 591–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable (min) | PSG vs. WHOOP-AUTO | PSG vs. WHOOP-MANUAL | PSG vs. ACTICAL | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PSG | Bias | AE | F | Bias | AE | F | Bias | AE | F | |
| TST | 392.8 (60.7) | −17.8 (61.1) | 40.0 | 1.7 | 16.7 (35.6) | 25.4 | 2.4 | 37.6 * (85.6) | 38.1 | 12.2 |
| Wake | 53.9 (45.7) | 17.8 (61.1) | 40.0 | 2.8 | −16.7 * (35.6) | 25.4 | 6.3 | −37.6 * (85.6) | 38.1 | 35.1 |
| Light | 197.1 (50.8) | −8.9 * (55.9) | 43.8 | 0.8 | 13.9 (59.9) | 47.0 | 2.0 | |||
| SWS | 101.4 (21.6) | −15.5 ** (30.1) | 24.7 | 13.1 | −6.1 (25.4) | 20.7 | 2.8 | |||
| REM | 94.3 (28.9) | 6.5 (39.5) | 33.0 | 0.9 | 8.8 (42.0) | 33.0 | 1.9 | |||
| SOL | 5.3 (5.9) | −0.2 (4.8) | 2.8 | 0.01 | ||||||
| Measure | Value (%) |
|---|---|
| 2-stage comparison | |
| WHOOP-AUTO | |
| Sensitivity for sleep | 90 |
| Specificity for wake | 60 |
| Overall agreement | 86 |
| WHOOP-MANUAL | |
| Sensitivity for sleep | 97 |
| Specificity for wake | 45 |
| Overall agreement | 90 |
| ACTICAL | |
| Sensitivity for sleep | 98 |
| Specificity for wake | 60 |
| Overall agreement | 89 |
| 4-stage comparison | |
| WHOOP-AUTO | |
| Sensitivity for wake | 60 |
| Sensitivity for light sleep | 61 |
| Sensitivity for SWS | 63 |
| Sensitivity for REM | 66 |
| Overall agreement | 63 |
| WHOOP-MANUAL | |
| Sensitivity for wake | 45 |
| Sensitivity for light sleep | 67 |
| Sensitivity for SWS | 61 |
| Sensitivity for REM | 66 |
| Overall agreement | 62 |
| WHOOP-AUTO | |||||
|---|---|---|---|---|---|
| Stage | Wake | Light sleep | SWS | REM | |
| PSG | Wake | 60% | 26% | 1% | 12% |
| Light sleep | 14% | 61% | 10% | 15% | |
| SWS | 6% | 28% | 64% | 2% | |
| REM | 6% | 27% | 1% | 66% | |
| WHOOP-MANUAL | |||||
|---|---|---|---|---|---|
| Stage | Wake | Light sleep | SWS | REM | |
| PSG | Wake | 45% | 37% | 1% | 18% |
| Light sleep | 7% | 67% | 11% | 15% | |
| SWS | 1% | 38% | 61% | 1% | |
| REM | 1% | 31% | 2% | 66% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, D.J.; Roach, G.D.; Lastella, M.; Scanlan, A.T.; Bellenger, C.R.; Halson, S.L.; Sargent, C. A Validation Study of a Commercial Wearable Device to Automatically Detect and Estimate Sleep. Biosensors 2021, 11, 185. https://doi.org/10.3390/bios11060185
Miller DJ, Roach GD, Lastella M, Scanlan AT, Bellenger CR, Halson SL, Sargent C. A Validation Study of a Commercial Wearable Device to Automatically Detect and Estimate Sleep. Biosensors. 2021; 11(6):185. https://doi.org/10.3390/bios11060185
Chicago/Turabian StyleMiller, Dean J., Gregory D. Roach, Michele Lastella, Aaron T. Scanlan, Clint R. Bellenger, Shona L. Halson, and Charli Sargent. 2021. "A Validation Study of a Commercial Wearable Device to Automatically Detect and Estimate Sleep" Biosensors 11, no. 6: 185. https://doi.org/10.3390/bios11060185