





The Clinical Potential of 3D-Printed Crowns Reinforced with Zirconia and Glass Silica Microfillers

Abstract
:1. Introduction
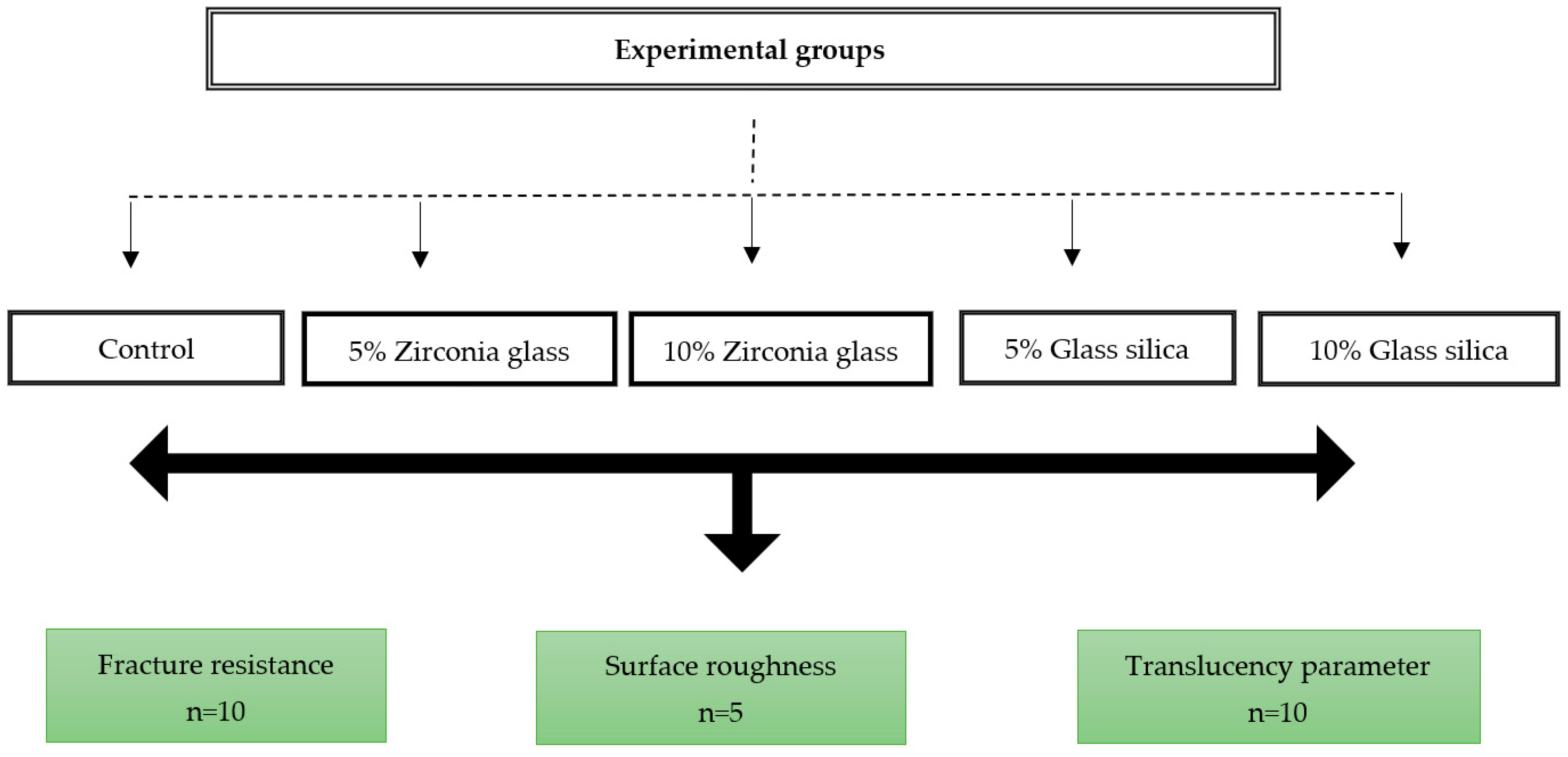
2. Materials and Methods
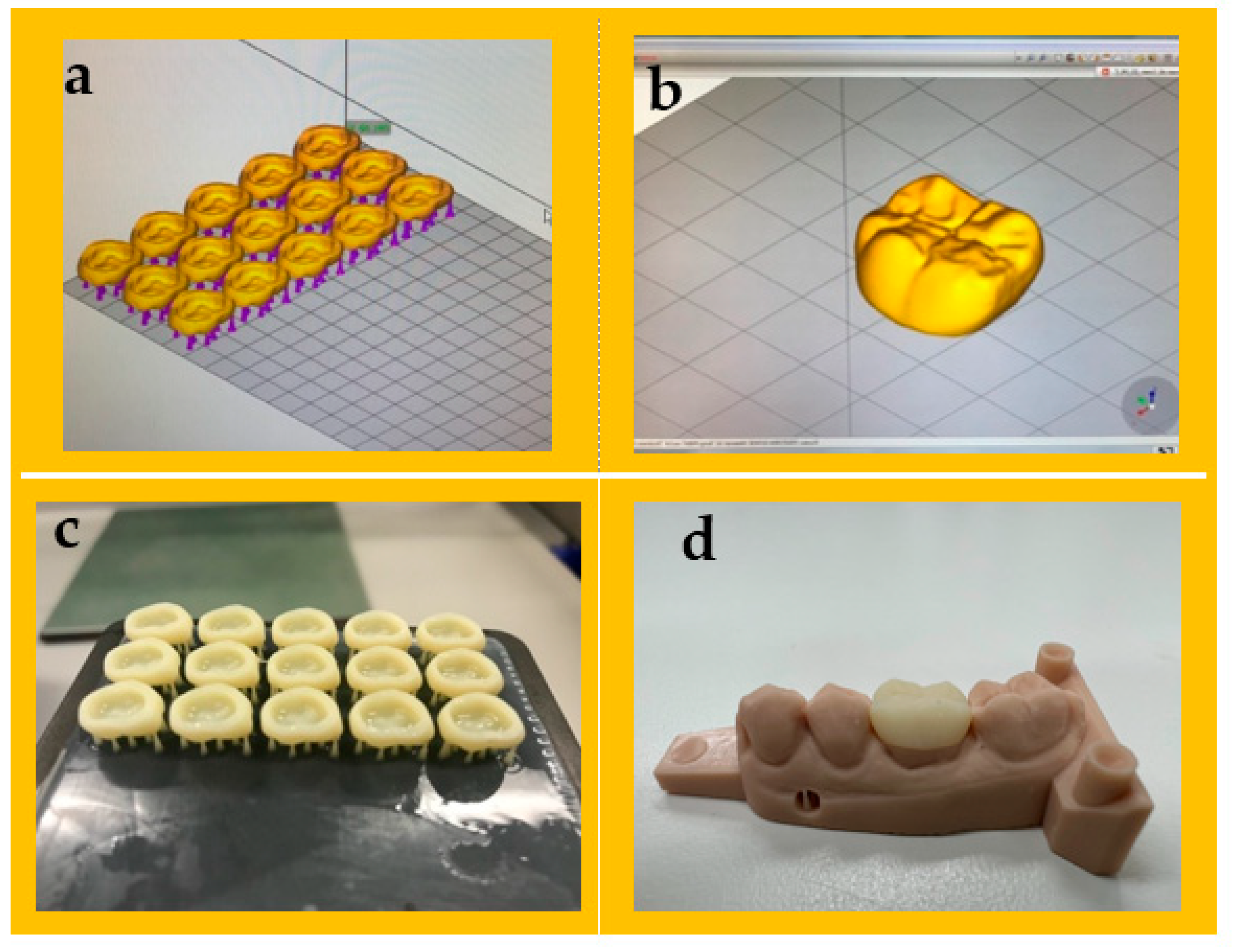
2.1. Sample Preparation
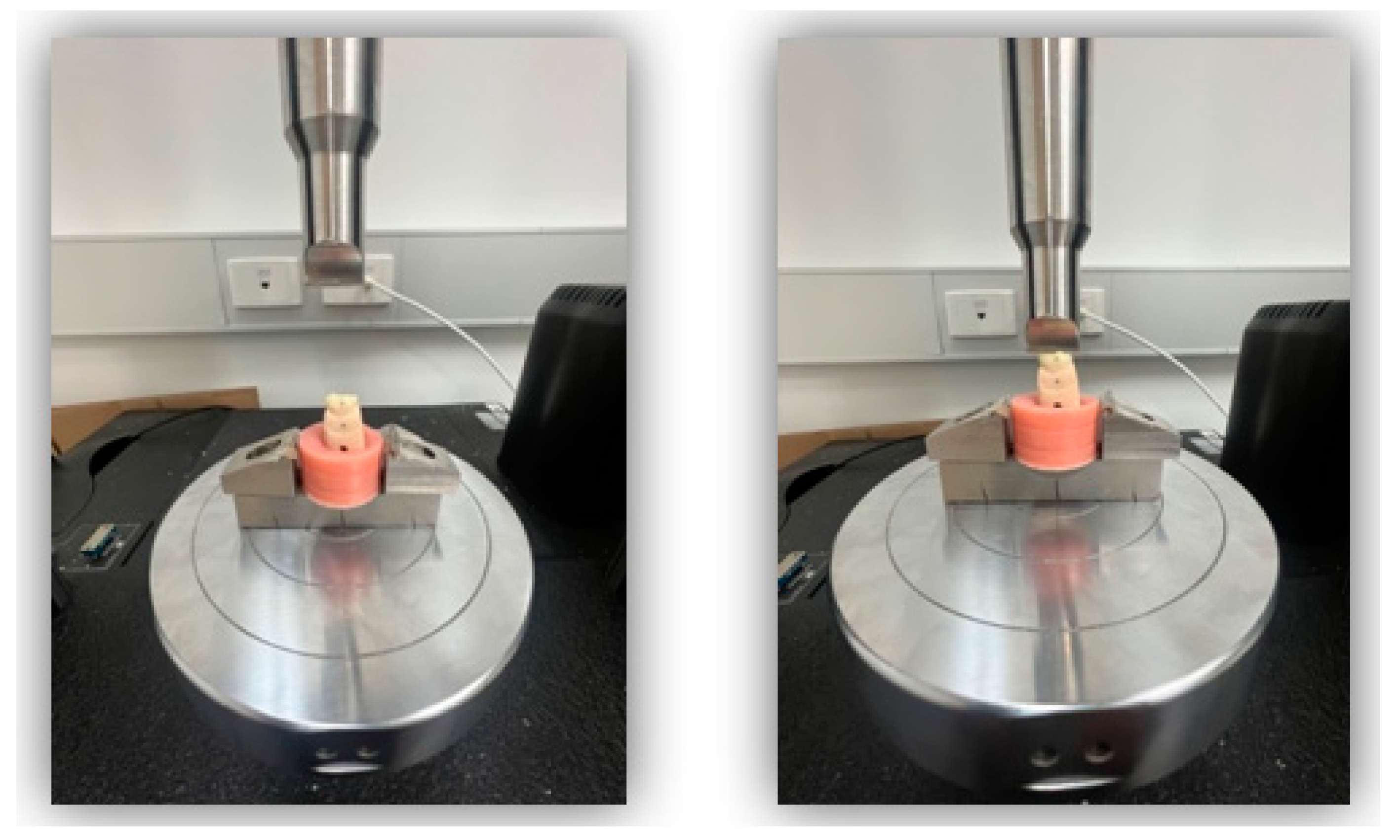
2.2. Fracture Resistance
2.3. Surface Roughness
2.4. Color Change Analysis (Translucency Parameters)
2.5. Fractographic Analysis
2.6. Statistical Analysis
3. Results
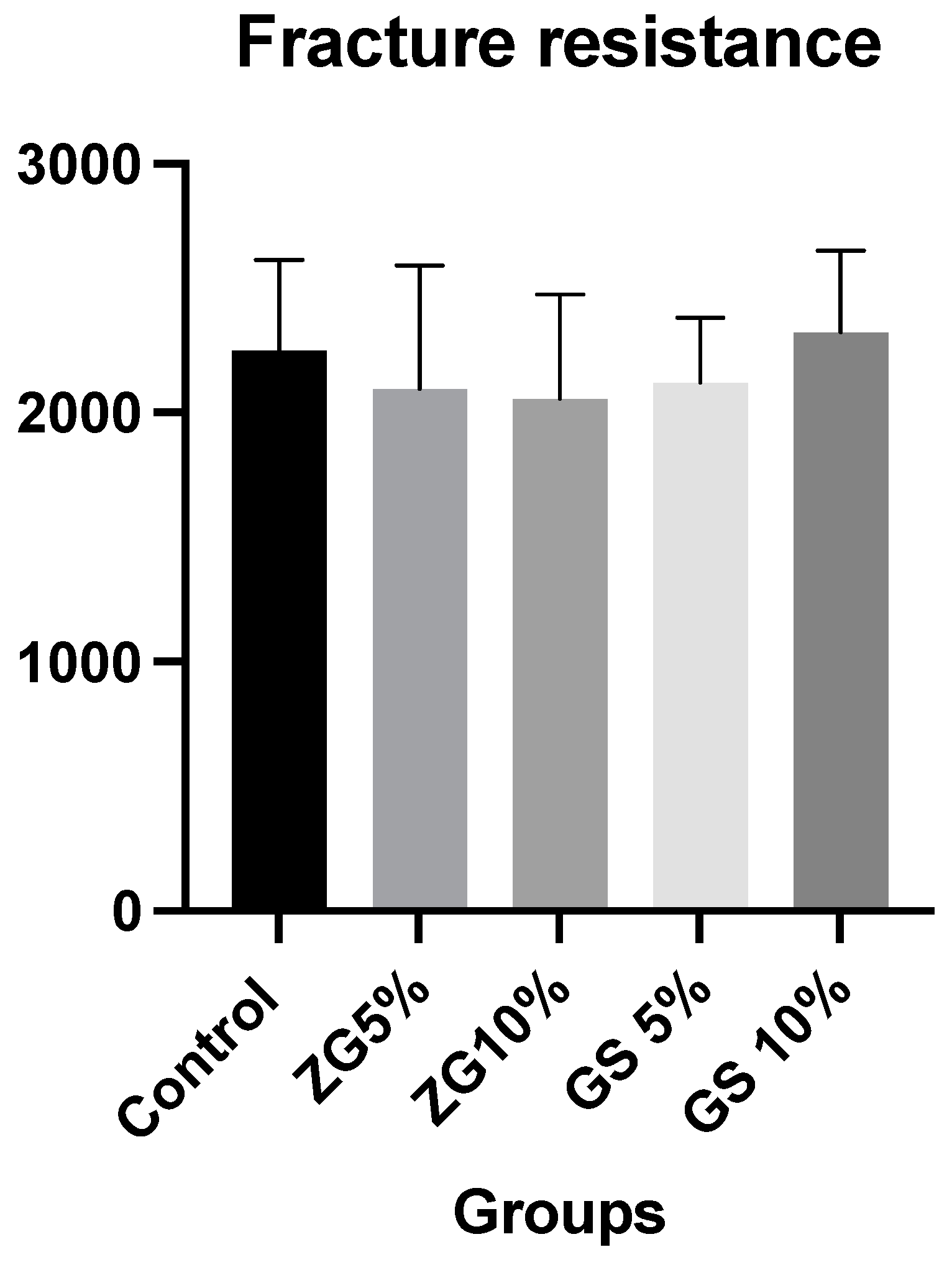
3.1. Fracture Resistance
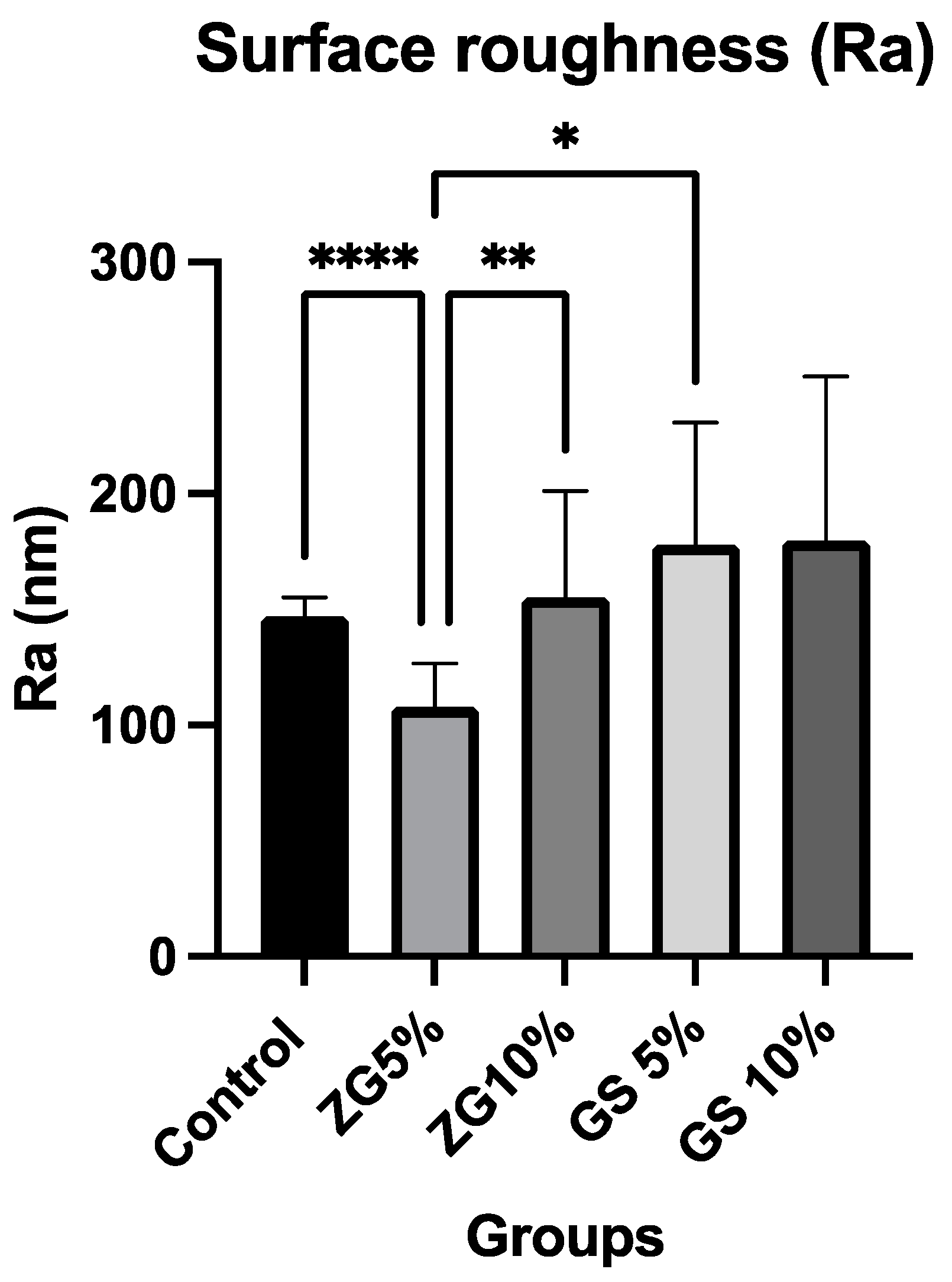
3.2. Surface Roughness
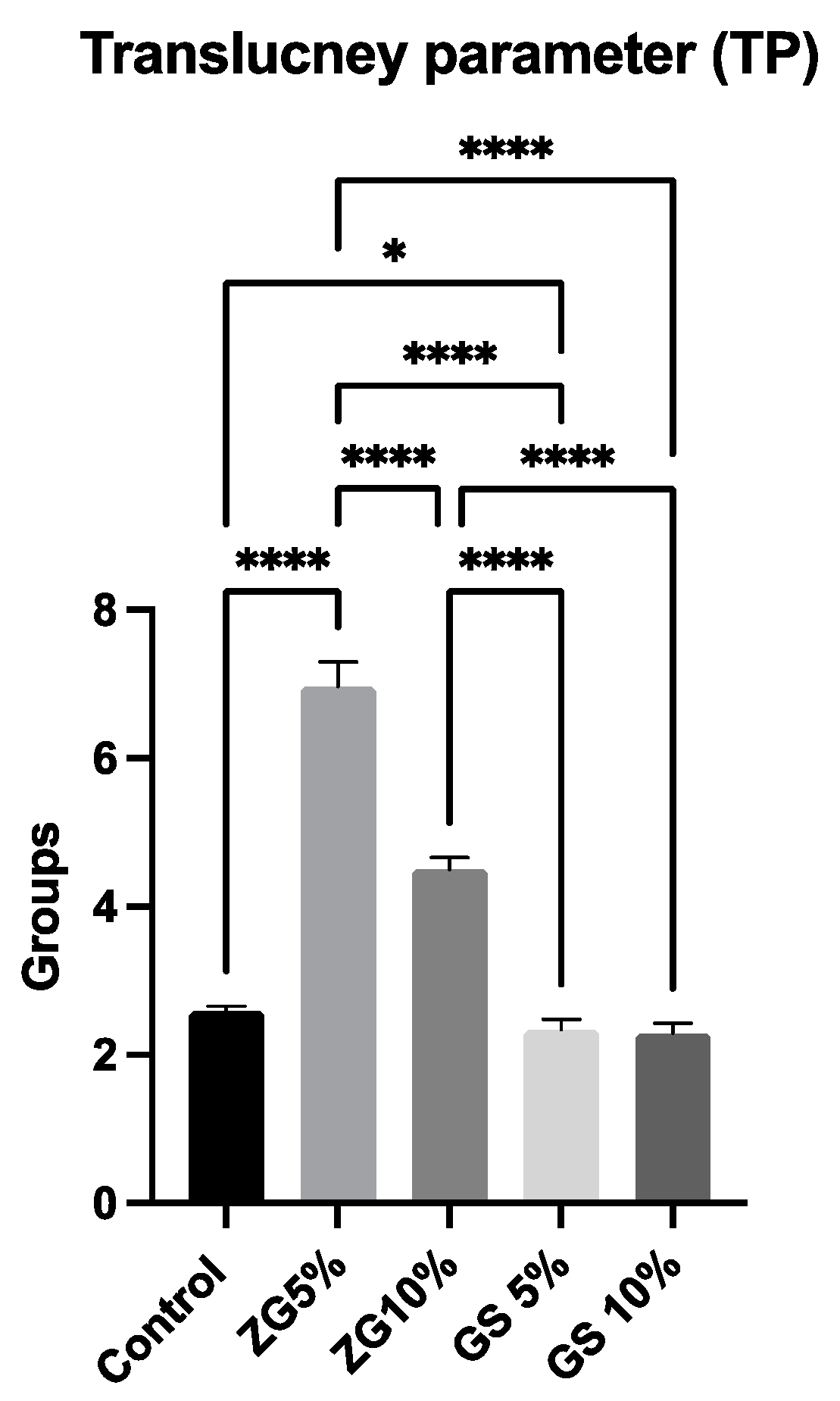
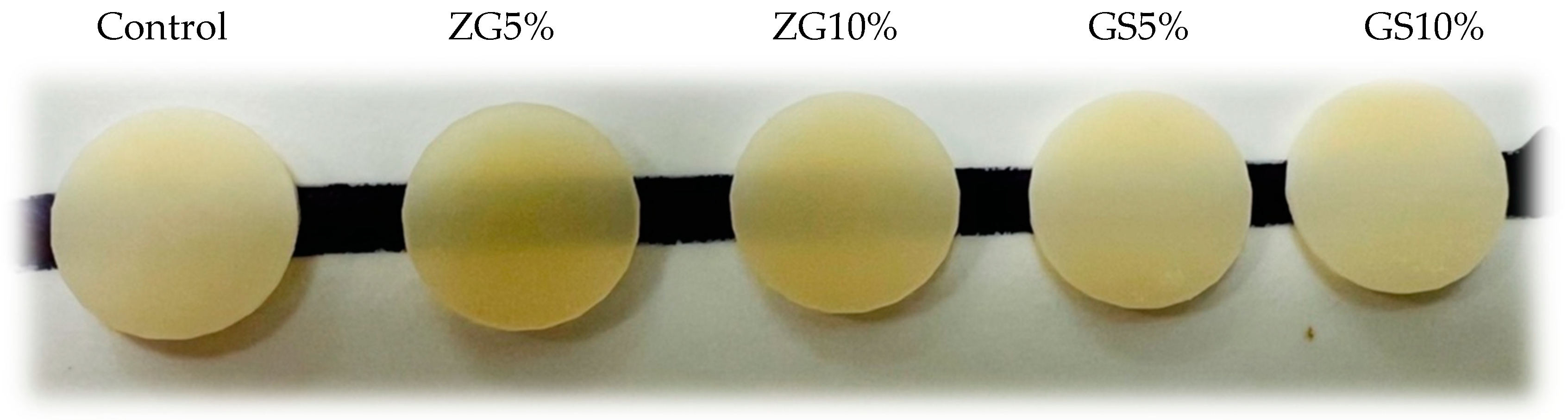
3.3. Translucency Parameter
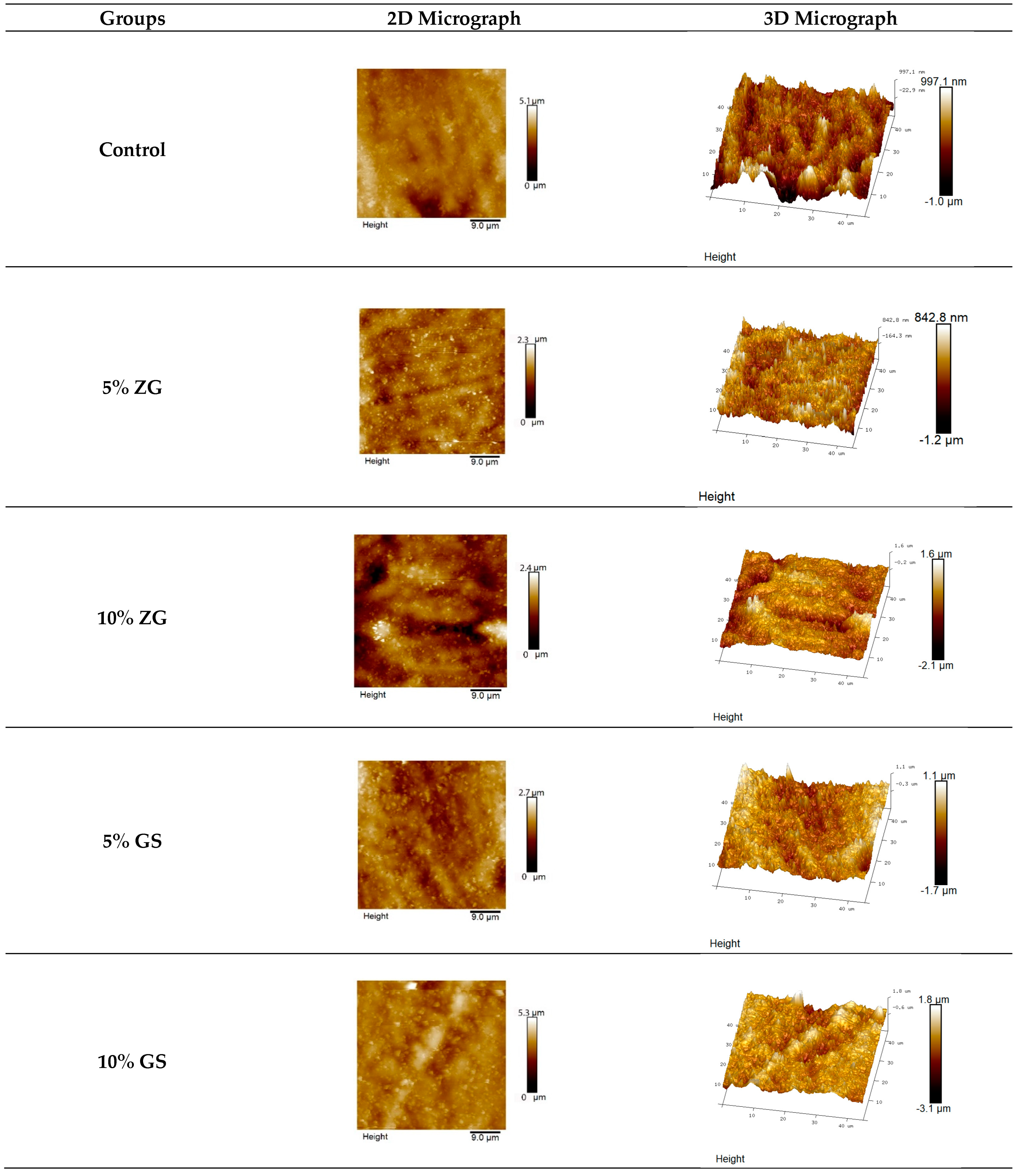
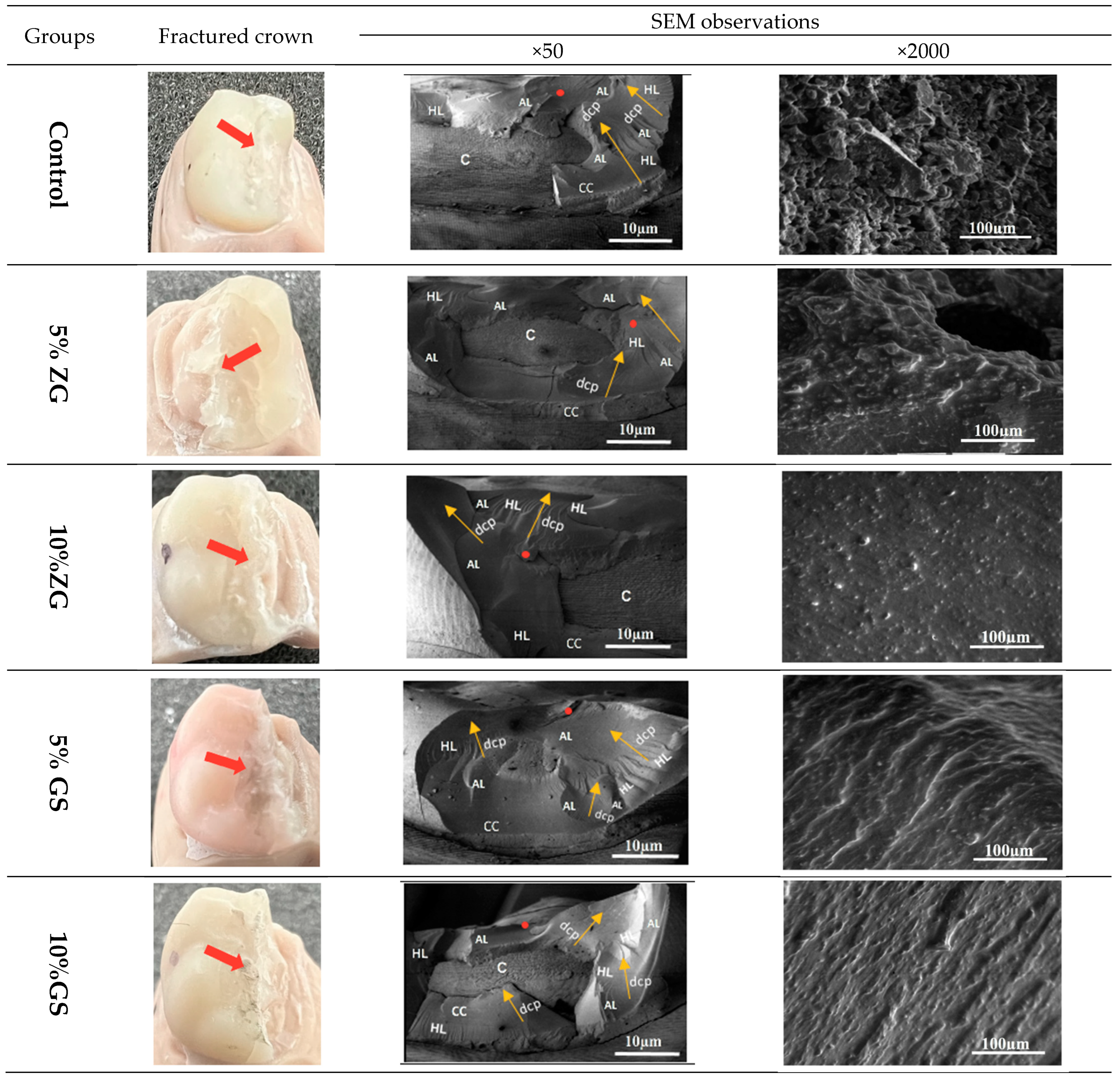
3.4. SEM Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Javaid, M.; Haleem, A. Current status and applications of additive manufacturing in dentistry: A literature-based review. J. Oral Biol. Craniofacial Res. 2019, 9, 179–185. [Google Scholar] [CrossRef]
- Masri, R.; Driscoll, C.F. Clinical Applications of Digital Dental Technology; Wiley Online Library: Hoboken, NJ, USA, 2015. [Google Scholar]
- Ahmadi, E.; Tabatabaei, M.H.; Sadr, S.M.; Atri, F. Comparison of the marginal discrepancy of PFM crowns in the CAD/CAM and lost-wax fabrication techniques by triple scanning. Dent. Med. Probl. 2020, 57, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Miura, S.; Fujisawa, M.; Komine, F.; Maseki, T.; Ogawa, T.; Takebe, J.; Nara, Y. Importance of interim restorations in the molar region. J. Oral Sci. 2019, 61, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Lorenz Holmer, A.O.; Lührs, A.-K.; von See, C. Comparison of the shear bond strength of 3D printed temporary bridges materials, on different types of resin cements and surface treatment. J. Clin. Exp. Dent. 2019, 11, e367. [Google Scholar]
- Raszewski, Z. Acrylic resins in the CAD/CAM technology: A systematic literature review. Dent. Med. Probl. 2020, 57, 449–454. [Google Scholar] [CrossRef]
- Kohorst, P.; Brinkmann, H.; Li, J.; Borchers, L.; Stiesch, M. Marginal accuracy of four-unit zirconia fixed dental prostheses fabricated using different computer-aided design/computer-aided manufacturing systems. Eur. J. Oral Sci. 2009, 117, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Anadioti, E.; Kane, B.; Soulas, E. Current and emerging applications of 3D printing in restorative dentistry. Curr. Oral Health Rep. 2018, 5, 133–139. [Google Scholar] [CrossRef]
- Paradowska-Stolarz, A.; Wezgowiec, J.; Mikulewicz, M. Comparison of Two Chosen 3D Printing Resins Designed for Orthodontic Use: An In Vitro Study. Materials 2023, 16, 2237. [Google Scholar] [CrossRef] [PubMed]
- Paradowska-Stolarz, A.; Wieckiewicz, M.; Kozakiewicz, M.; Jurczyszyn, K. Mechanical Properties, Fractal Dimension, and Texture Analysis of Selected 3D-Printed Resins Used in Dentistry That Underwent the Compression Test. Polymers 2023, 15, 1772. [Google Scholar] [CrossRef]
- Etajuri, E.A.; Suliman, E.; Mahmood, W.A.A.; Ibrahim, N.; Buzayan, M.; Mohd, N.R. Deviation of dental implants placed using a novel 3D-printed surgical guide: An in vitro study. Dent. Med. Probl. 2020, 57, 359–362. [Google Scholar] [CrossRef]
- Al-Halabi, M.N.; Bshara, N.; Comisi, J.C.; Abou Nassar, J. Evaluation of Fracture Resistance Force in Three Types of Primary Molar Crowns: Milled by CAD\CAM, 3D Dental Printed, and Composite Celluloid Crowns. Eur. Dent. Res. Biomater. J. 2020, 1, 33–39. [Google Scholar] [CrossRef]
- Al-Halabi, M.N.; Bshara, N.; Abou Nassar, J.; Comisi, J.C.; Alawa, L. Comparative assessment of novel 3d printed resin crowns versus direct celluloid crowns in restoring pulp treated primary molars. J. Evid.-Based Dent. Pract. 2022, 22, 101664. [Google Scholar] [CrossRef] [PubMed]
- Aati, S.; Akram, Z.; Ngo, H.; Fawzy, A.S. Development of 3D printed resin reinforced with modified ZrO2 nanoparticles for long-term provisional dental restorations. Dent. Mater. 2021, 37, e360–e374. [Google Scholar] [CrossRef] [PubMed]
- Wuersching, S.N.; Hickel, R.; Edelhoff, D.; Kollmuss, M. Initial biocompatibility of novel resins for 3D printed fixed dental prostheses. Dent. Mater. 2022, 38, 1587–1597. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Gironés, J.; López-García, S.; Pecci-Lloret, M.R.; Pecci-Lloret, M.P.; Lozano, F.J.R.; García-Bernal, D. In vitro biocompatibility testing of 3D printing and conventional resins for occlusal devices. J. Dent. 2022, 123, 104163. [Google Scholar] [CrossRef]
- Prpić, V.; Schauperl, Z.; Ćatić, A.; Dulčić, N.; Čimić, S. Comparison of mechanical properties of 3D-printed, CAD/CAM, and conventional denture base materials. J. Prosthodont. 2020, 29, 524–528. [Google Scholar] [CrossRef]
- Reymus, M.; Fabritius, R.; Keßler, A.; Hickel, R.; Edelhoff, D.; Stawarczyk, B. Fracture load of 3D-printed fixed dental prostheses compared with milled and conventionally fabricated ones: The impact of resin material, build direction, post-curing, and artificial aging—An In Vitro study. Clin. Oral Investig. 2020, 24, 701–710. [Google Scholar] [CrossRef]
- Asar, N.V.; Albayrak, H.; Korkmaz, T.; Turkyilmaz, I. Influence of various metal oxides on mechanical and physical properties of heat-cured polymethyl methacrylate denture base resins. J. Adv. Prosthodont. 2013, 5, 241–247. [Google Scholar] [CrossRef]
- Alshaikh, A.A.; Khattar, A.; Almindil, I.A.; Alsaif, M.H.; Akhtar, S.; Khan, S.Q.; Gad, M.M. 3D-printed nanocomposite denture-base resins: Effect of ZrO2 nanoparticles on the mechanical and surface properties In Vitro. Nanomaterials 2022, 12, 2451. [Google Scholar] [CrossRef]
- Miletic, V. Development of Dental Composites. In Dental Composite Materials for Direct Restorations; Springer: Berlin/Heidelberg, Germany, 2018; pp. 3–9. [Google Scholar]
- Ai, M.; Du, Z.; Zhu, S.; Geng, H.; Zhang, X.; Cai, Q.; Yang, X. Composite resin reinforced with silver nanoparticles–laden hydroxyapatite nanowires for dental application. Dent. Mater. 2017, 33, 12–22. [Google Scholar] [CrossRef]
- Bapat, R.A.; Parolia, A.; Chaubal, T.; Dharamadhikari, S.; Abdulla, A.M.; Sakkir, N.; Arora, S.; Bapat, P.; Sindi, A.M.; Kesharwani, P. Recent update on potential cytotoxicity, biocompatibility and preventive measures of biomaterials used in dentistry. Biomater. Sci. 2021, 9, 3244–3283. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-H.; Lin, Y.-M.; Lai, Y.-L.; Lee, S.-Y. Mechanical properties, accuracy, and cytotoxicity of UV-polymerized 3D printing resins composed of Bis-EMA, UDMA, and TEGDMA. J. Prosthet. Dent. 2020, 123, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Azmy, E.; Al-Kholy, M.R.Z.; Fattouh, M.; Kenawi, L.M.M.; Helal, M.A. Impact of nanoparticles additions on the strength of dental composite resin. Int. J. Biomater. 2022, 2022, 1165431. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Singh, S.; Sahu, J.; Srivastava, S.; Singh, M.R. Ceramic nanoparticles: Recompense, cellular uptake and toxicity concerns. Artif. Cells Nanomed. Biotechnol. 2016, 44, 401–409. [Google Scholar] [CrossRef]
- Moldovan, M.; Dudea, D.; Cuc, S.; Sarosi, C.; Prodan, D.; Petean, I.; Furtos, G.; Ionescu, A.; Ilie, N. Chemical and Structural Assessment of New Dental Composites with Graphene Exposed to Staining Agents. J. Funct. Biomater. 2023, 14, 163. [Google Scholar] [CrossRef] [PubMed]
- Aminoroaya, A.; Neisiany, R.E.; Khorasani, S.N.; Panahi, P.; Das, O.; Madry, H.; Cucchiarini, M.; Ramakrishna, S. A review of dental composites: Challenges, chemistry aspects, filler influences, and future insights. Compos. Part B Eng. 2021, 216, 108852. [Google Scholar] [CrossRef]
- Deng, J.; Ren, L.; Pan, Y.; Gao, H.; Meng, X. Antifungal property of acrylic denture soft liner containing silver nanoparticles synthesized in situ. J. Dent. 2021, 106, 103589. [Google Scholar] [CrossRef]
- Gowri, S.; Gandhi, R.R.; Sundrarajan, M. Structural, optical, antibacterial and antifungal properties of zirconia nanoparticles by biobased protocol. J. Mater. Sci. Technol. 2014, 30, 782–790. [Google Scholar] [CrossRef]
- Aati, S.; Shrestha, B.; Fawzy, A. Cytotoxicity and antimicrobial efficiency of ZrO2 nanoparticles reinforced 3D printed resins. Dent. Mater. 2022, 38, 1432–1442. [Google Scholar] [CrossRef]
- Schmalz, G.; Hickel, R.; van Landuyt, K.L.; Reichl, F.-X. Scientific update on nanoparticles in dentistry. Int. Dent. J. 2018, 68, 299–305. [Google Scholar] [CrossRef]
- Shahi, S.; Özcan, M.; Maleki Dizaj, S.; Sharifi, S.; Al-Haj Husain, N.; Eftekhari, A.; Ahmadian, E. A review on potential toxicity of dental material and screening their biocompatibility. Toxicol. Mech. Methods 2019, 29, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Ahlholm, P.; Sipilä, K.; Vallittu, P.; Jakonen, M.; Kotiranta, U. Digital versus conventional impressions in fixed prosthodontics: A review. J. Prosthodont. 2018, 27, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Chia, H.N.; Wu, B.M. Recent advances in 3D printing of biomaterials. J. Biol. Eng. 2015, 9, 4. [Google Scholar] [CrossRef]
- ISO 4049:2019; Dentistry—Polymer-Based Restorative Materials. ISO: Geneva, Switzerland, 2019.
- Shim, J.S.; Kim, J.-E.; Jeong, S.H.; Choi, Y.J.; Ryu, J.J. Printing accuracy, mechanical properties, surface characteristics, and microbial adhesion of 3D-printed resins with various printing orientations. J. Prosthet. Dent. 2020, 124, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Al-Dulaijan, Y.A.; Alsulaimi, L.; Alotaibi, R.; Alboainain, A.; Alalawi, H.; Alshehri, S.; Khan, S.Q.; Alsaloum, M.; AlRumaih, H.S.; Alhumaidan, A.A. Comparative Evaluation of Surface Roughness and Hardness of 3D Printed Resins. Materials 2022, 15, 6822. [Google Scholar] [CrossRef]
- Kul, E.; Abdulrahim, R.; Bayındır, F.; Matori, K.A.; Gül, P. Evaluation of the color stability of temporary materials produced with CAD/CAM. Dent. Med. Probl. 2021, 58, 187–191. [Google Scholar] [CrossRef]
- Ellakwa, A.; Thomas, G.D.; Shortall, A.C.; Marquis, P.M.; Burke, F.J. Fracture resistance of fiber-reinforced composite crown restorations. Am. J. Dent. 2003, 16, 375–380. [Google Scholar]
- Gadelmawla, E.S.; Koura, M.M.; Maksoud, T.M.A.; Elewa, I.M.; Soliman, H.H. Roughness parameters. J. Mater. Process. Technol. 2002, 123, 133–145. [Google Scholar] [CrossRef]
- Cie, C. Commission Internationale de l’Eclairage Proceedings, 1931; Cambridge University Press: Cambridge, UK, 1932. [Google Scholar]
- Scherrer, S.S.; Lohbauer, U.; Della Bona, A.; Vichi, A.; Tholey, M.J.; Kelly, J.R.; van Noort, R.; Cesar, P.F. ADM guidance—Ceramics: Guidance to the use of fractography in failure analysis of brittle materials. Dent. Mater. 2017, 33, 599–620. [Google Scholar] [CrossRef]
- Alrashdi, M.; Ardoin, J.; Liu, J.A. Zirconia crowns for children: A systematic review. Int. J. Paediatr. Dent. 2022, 32, 66–81. [Google Scholar] [CrossRef]
- Al-Zordk, W.; Elmisery, A.; Ghazy, M. Hybrid-abutment-restoration: Effect of material type on torque maintenance and fracture resistance after thermal aging. Int. J. Implant Dent. 2020, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.; Kim, H.; Kim, I.-H.; Lee, J.; Lee, K.E.; Lee, H.-S.; Kim, J.-H.; Song, J.S.; Shin, Y. Novel 3D Printed Resin Crowns for Primary Molars: In vitro study of fracture resistance, biaxial flexural strength, and dynamic mechanical analysis. Children 2022, 9, 1445. [Google Scholar] [CrossRef] [PubMed]
- Owais, A.I.; Shaweesh, M.; Abu Alhaija, E.S.J. Maximum occusal bite force for children in different dentition stages. Eur. J. Orthod. 2013, 35, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Guess, P.C.; Schultheis, S.; Wolkewitz, M.; Zhang, Y.; Strub, J.R. Influence of preparation design and ceramic thicknesses on fracture resistance and failure modes of premolar partial coverage restorations. J. Prosthet. Dent. 2013, 110, 264–273. [Google Scholar] [CrossRef]
- Albelasy, E.H.; Hamama, H.H.; Tsoi, J.K.H.; Mahmoud, S.H. Fracture resistance of CAD/CAM occlusal veneers: A systematic review of laboratory studies. J. Mech. Behav. Biomed. Mater. 2020, 110, 103948. [Google Scholar] [CrossRef]
- Ding, H.; Cui, Z.; Maghami, E.; Chen, Y.; Matinlinna, J.P.; Pow, E.H.N.; Fok, A.S.L.; Burrow, M.F.; Wang, W.; Tsoi, J.K.H. Morphology and mechanical performance of dental crown designed by 3D-DCGAN. Dent. Mater. 2023, 39, 320–332. [Google Scholar] [CrossRef]
- Campos, F.; Valandro, L.F.; Feitosa, S.A.; Kleverlaan, C.J.; Feilzer, A.J.; De Jager, N.; Bottino, M.A. Adhesive cementation promotes higher fatigue resistance to zirconia crowns. Oper. Dent. 2017, 42, 215–224. [Google Scholar] [CrossRef]
- May, L.G.; Kelly, J.R.; Bottino, M.A.; Hill, T. Effects of cement thickness and bonding on the failure loads of CAD/CAM ceramic crowns: Multi-physics FEA modeling and monotonic testing. Dent. Mater. 2012, 28, e99–e109. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dos Santos, A.F.C.; da Cruz Santos, G.; da Silva Leite, L.S.; Lozada, J.C.; Silva-Concílio, L.R.; Baroudi, K.; Amaral, M. Effect of cement layer thickness on the immediate and long-term bond strength and residual stress between lithium disilicate glass-ceramic and human dentin. Materials 2021, 14, 5153. [Google Scholar] [CrossRef]
- Zimmermann, M.; Ender, A.; Egli, G.; Özcan, M.; Mehl, A. Fracture load of CAD/CAM-fabricated and 3D-printed composite crowns as a function of material thickness. Clin. Oral Investig. 2019, 23, 2777–2784. [Google Scholar] [CrossRef]
- Soto-Montero, J.; de Castro, E.F.; Romano, B.D.C.; Nima, G.; Shimokawa, C.A.K.; Giannini, M. Color alterations, flexural strength, and microhardness of 3D printed resins for fixed provisional restoration using different post-curing times. Dent. Mater. 2022, 38, 1271–1282. [Google Scholar] [CrossRef] [PubMed]
- Soares, L.M.; Soares, C.; Miranda, M.E.; Basting, R.T. Influence of core-veneer thickness ratio on the fracture load and failure mode of zirconia crowns. J. Prosthodont. 2019, 28, 209–215. [Google Scholar] [CrossRef]
- Scherrer, S.S.; De Rijk, W.G. The fracture resistance of all-ceramic crowns on supporting structures with different elastic moduli. Int. J. Prosthodont. 1993, 6, 462–467. [Google Scholar] [PubMed]
- Kinney, J.H.; Marshall, S.J.; Marshall, G.W. The mechanical properties of human dentin: A critical review and re-evaluation of the dental literature. Crit. Rev. Oral Biol. Med. 2003, 14, 13–29. [Google Scholar] [CrossRef]
- Alkahtany, M.F.; Ali, S.; Khabeer, A.; Shah, S.A.; Almadi, K.H.; Abdulwahed, A.; Farooq, I.; Vohra, F.; Abduljabbar, T. A Microcomputed Tomographic Evaluation of Root Canal Morphology of Maxillary Second Premolars in a Pakistani Cohort. Appl. Sci. 2021, 11, 5086. [Google Scholar] [CrossRef]
- Ramezanzadeh, B.; Attar, M.M.; Farzam, M. Effect of ZnO nanoparticles on the thermal and mechanical properties of epoxy-based nanocomposite. J. Therm. Anal. Calorim. 2011, 103, 731–739. [Google Scholar] [CrossRef]
- Hiremath, A.; Thipperudrappa, S.; Bhat, R. Surface morphology analysis using atomic force microscopy and statistical method for glass fiber reinforced epoxy-zinc oxide nanocomposites. Eng. Sci. 2022, 18, 308–319. [Google Scholar] [CrossRef]
- Brandão, N.L.; Portela, M.B.; Maia, L.C.; Antônio, A.; Silva, V.L.M.; Silva, E.M.D. Model resin composites incorporating ZnO-NP: Activity against S. mutans and physicochemical properties characterization. J. Appl. Oral Sci. 2018, 26, e20170270. [Google Scholar] [CrossRef]
- Ionescu, A.C.; Cazzaniga, G.; Ottobelli, M.; Ferracane, J.L.; Paolone, G.; Brambilla, E. In vitro biofilm formation on resin-based composites cured under different surface conditions. J. Dent. 2018, 77, 78–86. [Google Scholar] [CrossRef]
- Sturz, C.R.C.; Faber, F.-J.; Scheer, M.; Rothamel, D.; Neugebauer, J. Effects of various chair-side surface treatment methods on dental restorative materials with respect to contact angles and surface roughness. Dent. Mater. J. 2015, 34, 796–813. [Google Scholar] [CrossRef]
- Karaokutan, I.; Sayin, G.; Kara, O. In vitro study of fracture strength of provisional crown materials. J. Adv. Prosthodont. 2015, 7, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Gantz, L.; Fauxpoint, G.; Arntz, Y.; Pelletier, H.; Etienne, O. In Vitro comparison of the surface roughness of polymethyl methacrylate and bis-acrylic resins for interim restorations before and after polishing. J. Prosthet. Dent. 2021, 125, 833.e1–833.e10. [Google Scholar] [CrossRef]
- Johnston, W.M. Review of translucency determinations and applications to dental materials. J. Esthet. Restor. Dent. 2014, 26, 217–223. [Google Scholar] [CrossRef]
- Haas, K.; Azhar, G.; Wood, D.J.; Moharamzadeh, K.; van Noort, R. The effects of different opacifiers on the translucency of experimental dental composite resins. Dent. Mater. 2017, 33, e310–e316. [Google Scholar] [CrossRef] [PubMed]
- Kolb, C.; Gumpert, K.; Wolter, H.; Sextl, G. Highly translucent dental resin composites through refractive index adaption using zirconium dioxide nanoparticles and organic functionalization. Dent. Mater. 2020, 36, 1332–1342. [Google Scholar] [CrossRef] [PubMed]
- Pop-Ciutrila, I.S.; Ghinea, R.; Colosi, H.A.; Dudea, D. Dentin translucency and color evaluation in human incisors, canines, and molars. J. Prosthet. Dent. 2016, 115, 475–481. [Google Scholar] [CrossRef]
- Almasabi, W.; Tichy, A.; Abdou, A.; Hosaka, K.; Nakajima, M.; Tagami, J. Effect of water storage and thermocycling on light transmission properties, translucency and refractive index of nanofilled flowable composites. Dent. Mater. J. 2021, 40, 599–605. [Google Scholar] [CrossRef]
- Ota, M.; Ando, S.; Endo, H.; Ogura, Y.; Miyazaki, M.; Hosoya, Y. Influence of refractive index on optical parameters of experimental resin composites. Acta Odontol. Scand. 2012, 70, 362–367. [Google Scholar] [CrossRef]
- Mubarak, S.; Dhamodharan, D.B.; Kale, M.; Divakaran, N.; Senthil, T.; Wu, L.; Wang, J. A novel approach to enhance mechanical and thermal properties of SLA 3D printed structure by incorporation of metal–metal oxide nanoparticles. Nanomaterials 2020, 10, 217. [Google Scholar] [CrossRef]
- Yang, Z.; Peng, S.; Wang, Z.; Miao, J.-T.; Zheng, L.; Wu, L.; Weng, Z. UV-curable, low-viscosity resin with a high silica filler content for preparing ultrastiff, 3D-printed molds. ACS Appl. Polym. Mater. 2022, 4, 2636–2647. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Type | Manufacturer |
|---|---|---|
| Everes Temporary (dental resin) | 3D-printed resin | Sisma, Italy |
| Glass fillers (ultrafine GM35429) | Additive particles | Shofu Inc., Kyoto, Japan |
| Zirconia glass (ultrafine GM018-307) | Additive particles | Shofu Inc., Kyoto, Japan |
| G-cement capsule A2 | Cement resin | GC corporation, Tokyo, Japan |
| Code# | Description |
|---|---|
| I | Minimal fracture capable of refinishing and rapier |
| II | Less than half of crown lost |
| III | Crown fracture through midline, half of crown displaced or lost |
| IV | More than half of crown lost |
| V | Sever fracture of the crown |
| Group | Fracture Resistance | Roughness Average (Ra) | Translucency Parameter (TP) |
|---|---|---|---|
| Control | 2250 (364.20) a | 147 (±9) a | 2.590 (0.06) a |
| 5% ZG | 2095(495.70) a | 108 (±20) b | 6.965 (0.33) b |
| 10% ZG | 2055 (420.0) a | 155 (±49) ac | 4.502 (0.15) c |
| 5% GS | 2121(260.10) a | 178 (±56) ac | 2.338 (0.13) d |
| 10% GS | 2325(325.8) a | 180 (±75) a | 2.293 (0.12) d |
| Groups | Mode of Failure | ||||
|---|---|---|---|---|---|
| I | II | III | IV | V | |
| Control | 1 | 1 | 8 | 0 | 0 |
| 5% ZG | 0 | 5 | 4 | 1 | 0 |
| 10% ZG | 0 | 3 | 3 | 4 | 0 |
| 5% GS | 0 | 5 | 5 | 0 | 0 |
| 10% GS | 0 | 5 | 4 | 1 | 0 |
| Total | 1 | 19 | 24 | 6 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshamrani, A.; Alhotan, A.; Owais, A.; Ellakwa, A. The Clinical Potential of 3D-Printed Crowns Reinforced with Zirconia and Glass Silica Microfillers. J. Funct. Biomater. 2023, 14, 267. https://doi.org/10.3390/jfb14050267
Alshamrani A, Alhotan A, Owais A, Ellakwa A. The Clinical Potential of 3D-Printed Crowns Reinforced with Zirconia and Glass Silica Microfillers. Journal of Functional Biomaterials. 2023; 14(5):267. https://doi.org/10.3390/jfb14050267
Chicago/Turabian StyleAlshamrani, Abdullah, Abdulaziz Alhotan, Ahmed Owais, and Ayman Ellakwa. 2023. "The Clinical Potential of 3D-Printed Crowns Reinforced with Zirconia and Glass Silica Microfillers" Journal of Functional Biomaterials 14, no. 5: 267. https://doi.org/10.3390/jfb14050267