
Current Status of Peri-Implant Diseases: A Clinical Review for Evidence-Based Decision Making
 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Peri-Implant Diseases and Conditions
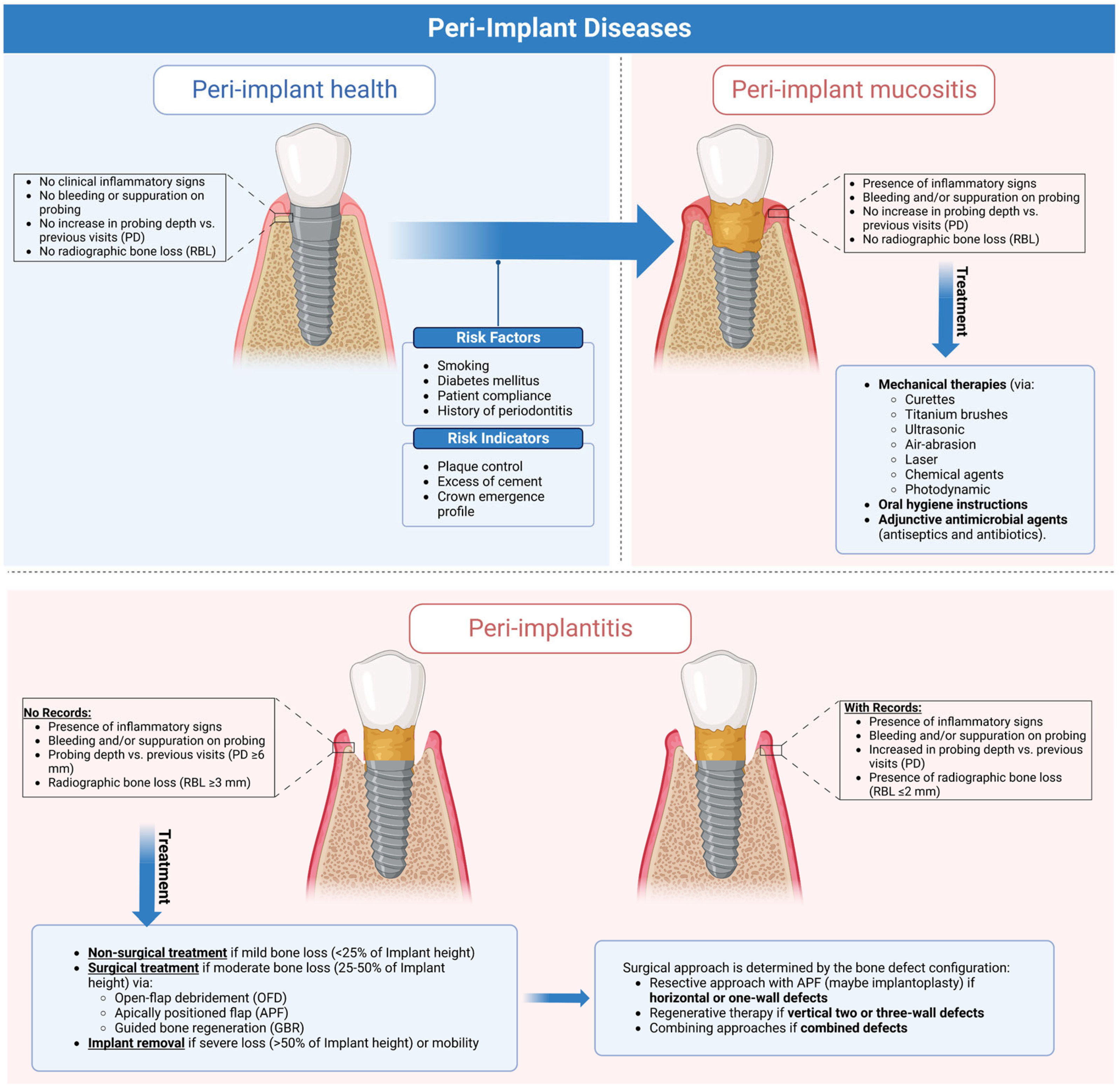
2.1. Peri-Implant Health
- Absence of clinical inflammatory signs;
- No bleeding and suppuration on mild probing (0.25 N);
- Stable probing depth compared to previous visits;
- Absence of radiographic bone loss (excluding physiological crestal bone loss one year after the prosthetic load of 0.5–2 mm) [3].
2.2. Peri-Implant Mucositis
2.3. Peri-Implantitis
3. Epidemiology of Peri-Implant Diseases
4. Risk Factors and Indicators
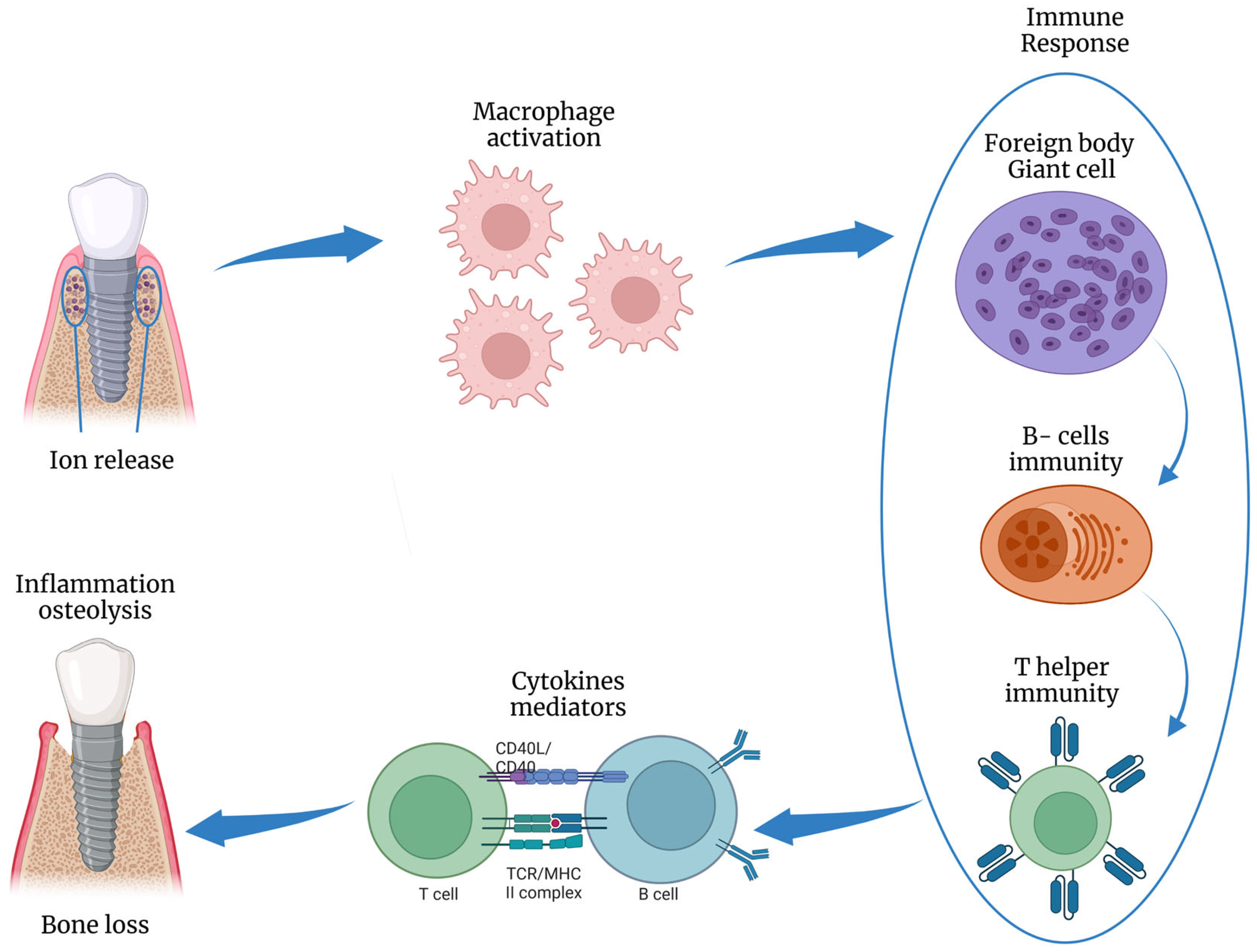
5. Microbiological Profile
6. Prevention of Peri-Implant Diseases
7. Treatment Strategies
7.1. Nonsurgical Treatment
- Curettes plastic or carbon-fiber curettes are softer since they can mechanically debride the implant surface without damaging it. However, they cannot clean the spaces between the threads. Stainless steel curette is contraindicated since its hardness is greater than titanium, resulting in substantial damage to the implant surface [52,54];
- Ultrasonic Instruments: specialized ultrasonic tips that are implant compatible (a steel tip, Teflon tip, and tip covered with either polyether ketone PEEK or carbon fiber), vibrating at high frequencies (>20 kHz), can effectively debride the implant surface and remove subgingival tartar faster than manual instruments [54,55,56];
- Titanium Brush: these brushes are often used during open flap debridement. However, they are fragile and break easily;
- Air Powder Abrasion: granules of glycine, hydroxyapatite, sodium bicarbonate, titanium dioxide, erythritol, or tricalcium phosphate can be used to debride the implant surface without damaging it. However, these devices must be used cautiously (especially subgingivally) to avoid soft tissue injury or emphysema [57,58];
- Laser: many lasers can decontaminate the implant surface at high doses, and their capacity is dose dependent. It can irreversibly alter the implant surface; it is critical to consider proper time and emission power to avoid the possibility of thermal osteonecrosis of the bone. There is no clear evidence in the literature distinguishing between laser, mechanical treatment alone, combined with mechanical debridement, and air powder abrasion [59,60,61]. As such, Cosgarea et al. found insufficient evidence of the clinical efficacy and patient-reported benefits of mechanical/physical decontamination in nonsurgical submarginal instrumentation [19]. In all cases, inflammatory indices were reduced for a limited follow-up period (3–6 months), while longer periods were associated with reinfection phenomena [59];
- Photodynamic Therapy: a low-power laser light (usually diode) or a nonlaser infrared light stimulates the production of reactive oxygen species (ROS) from a photosensitive molecule (methylene blue and toluidine blue, porphyrins, chlorines, and phthalocyanines). Photodynamic therapy destroys bacteria directly and speeds tissue healing; it should be used as an adjunct to mechanical debridement or surgery. However, Ramanauskaite et al., in a systematic review, revealed limited data with inconclusive evidence on the clinical effectiveness of photo/mechanical and physical implant surface decontamination in conjunction with surgical peri-implantitis treatment [62]. Therefore, the literature has yet to prove that this treatment is superior to conventional decontamination procedures, and there is no consensus on the factors making this therapy more successful (type of light source, wavelength, and time of therapy), so additional research is needed [63];
- Chemical methods: chemical agents with antimicrobial effects (e.g., hydrogen peroxide, phosphoric acid, EDTA, and NaOCl) can efficiently debride the implant surface. However, these agents could alter the titanium surface’s integrity and produce chemical residues having a cytotoxic effect. Therefore, they should be used at a moderate concentration (citric acid 20%, EDTA 24%, NaOCl 1.5%) [64]. Yet, Dommisch et al., in a systematic review, concluded limited evidence that the adjunctive use of aPDT, 0.95% NaOCl, and 0.12% CHX had no additional efficacy in improving bleeding on probing or pocket depth as compared to submarginal instrumentation during peri-implant mucositis treatment [65]. Also, Wilensky et al., in a meta-analysis, found a low quality of evidence supporting not employing chemicals (PDT, CHX, and LAbs) for surface decontamination during peri-implantitis surgery since mechanical debridement (either with or without saline) was superior [66];
- Adjunctive Measures: such measures have been employed in response to the necessity to eliminate dental biofilm to maintain peri-implant tissues healthy regularly [53,66]; thus, adjunctive patient usage of some chemical agents (e.g., antimicrobials, anti-inflammatory, or probiotic drugs) after mechanical treatment of peri-implant diseases could aid in resolving inflammation around implants [67,68,69]. Antibiotics (systemic and local) have been shown to reduce bleeding on probing and pocket depth [67,68], and systematic antibiotics significantly improved the modified implant surface treatment when combined with mechanical debridement with no effect on nonmodified surfaces [69]. Gennai et al., concluded the current evidence as the systemic application of probiotics, antiseptics, and antibiotics for three months at least have clinical improvements by reducing gingival and plaque indices when combined with submarginal instrumentation for peri-implant mucositis patients [70]. However, Teughels et al. revealed insufficient evidence to support systemic and local antimicrobials as adjuncts during surgical treatment of peri-implantitis since they did not improve clinical outcomes (e.g., pocket depth, bleeding on probing, etc.) [71]. Given the inconclusive evidence on their efficacy and concerns about increasing antibiotics resistance or superinfection by opportunistic microorganisms [72], further randomized clinical trials are needed to validate their adjunctive usage;
- Electrochemical Disinfection: the main principles regarding this technique involve the surface disinfection of biofilm-contaminated implant surfaces that could take advantage of the application of low direct currents [73]. Recent studies reported that the current charge is effective for organic component removal of the oral biofilms and could reduce the adhesion capabilities and the oral environment survival [74,75]. For this purpose, Koch et al., evaluated boron-doped diamond (BDD) electrodes (>2.5 V) to determine an electrochemical implant surface treatment against biofilms producing a water electrolytic property with hydrogen release from the cathode and oxygen from the anode [73].
7.2. Surgical Treatment
7.2.1. Open-Flap Debridement (OFD)
7.2.2. Resective Technique and Apically Positioned Flap (APF)
7.2.3. Regenerative Technique and Guided Bone Regeneration (GBR)
- 2.38 ± 0.53 mm (37.9%) for OFD;
- 2.04 ± 0.15 mm (33.4%) for the resective surgery;
- 2.32 ± 1.29 mm (37.1%) for the use of bone substitutes;
- 3.16 ± 0.62 mm (48.2%) for regenerative procedures.
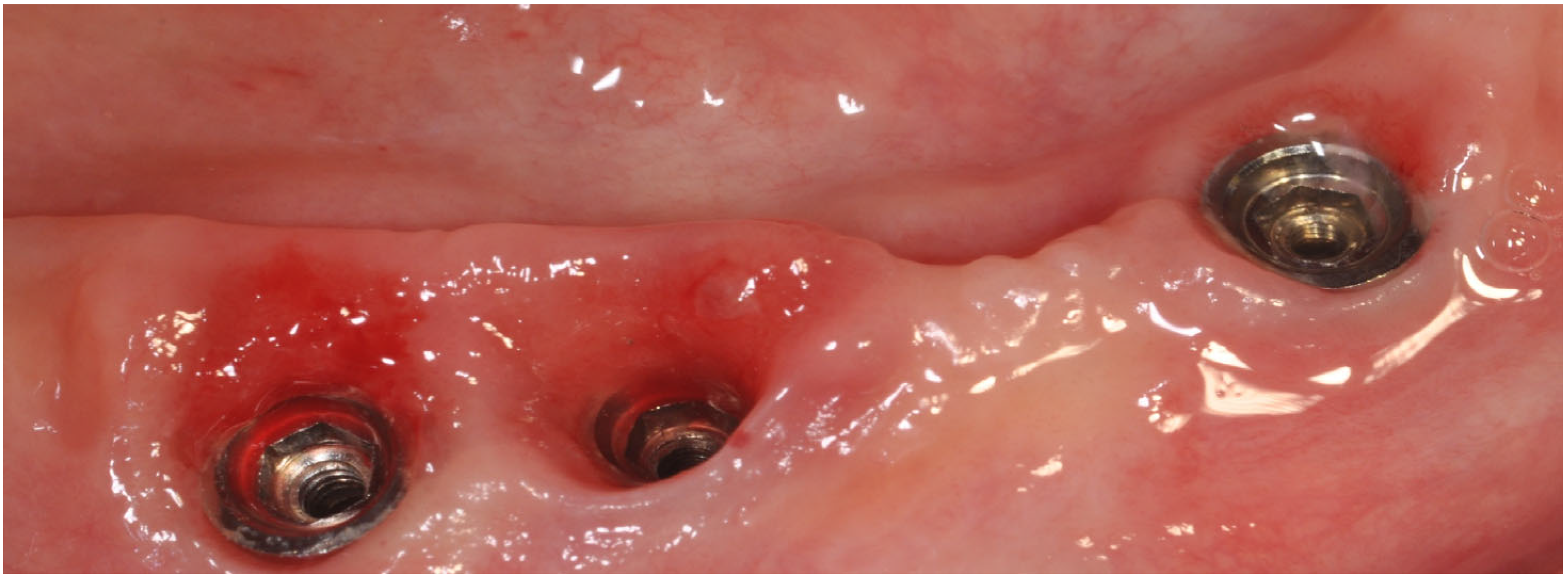
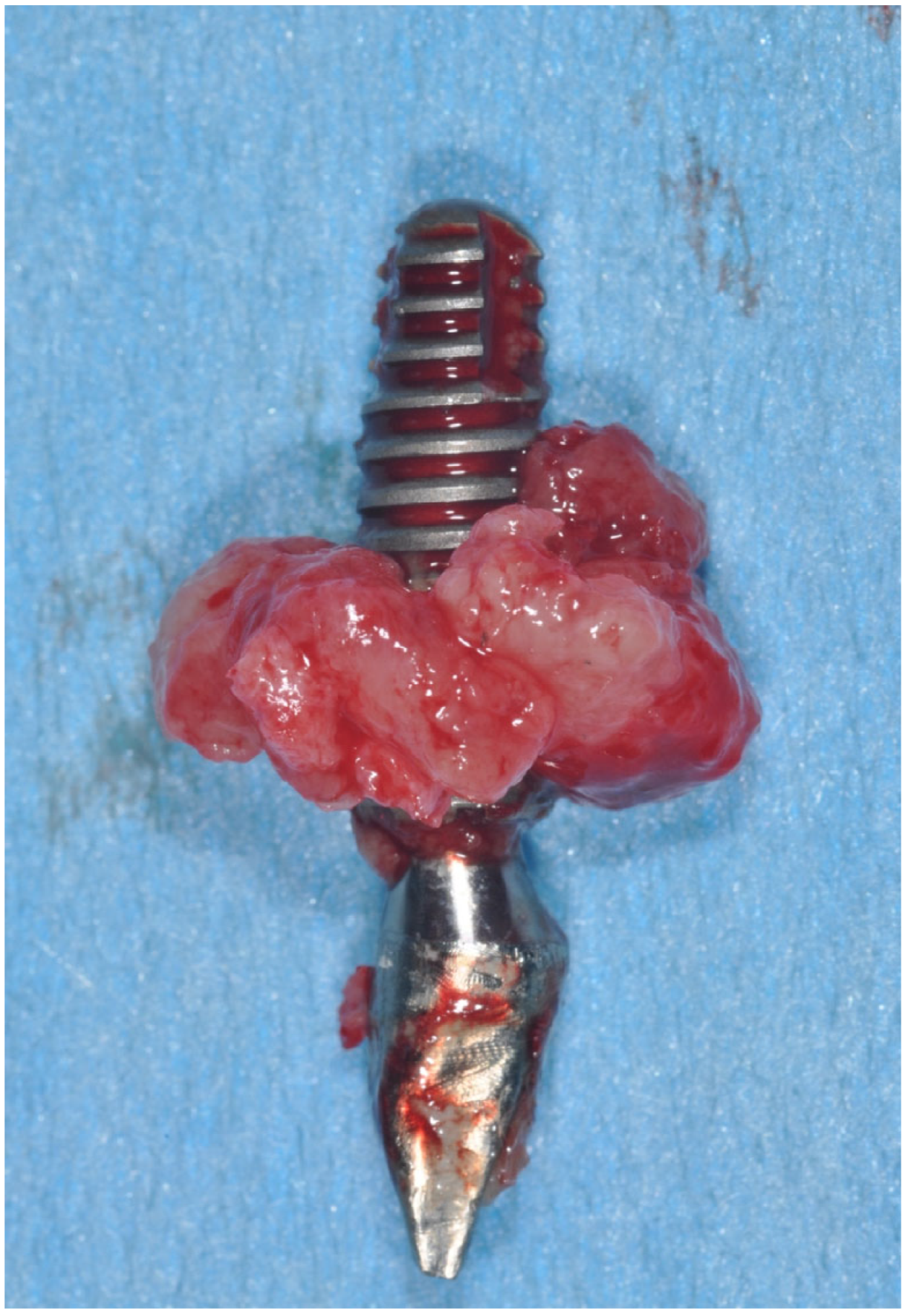
7.3. Implant Removal
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Berglundh, T.; Persson, L.; Klinge, B. A Systematic Review of the Incidence of Biological and Technical Complications in Implant Dentistry Reported in Prospective Longitudinal Studies of at Least 5 Years: Systematic Review of Implant Complications. J. Clin. Periodontol. 2002, 29, 197–212. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-Implant Diseases and Conditions: Consensus Report of Workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S313–S318. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Lindhe, J. Peri-Implant Health. J. Periodontol. 2018, 89 (Suppl. 1), S249–S256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-Implant Health, Peri-Implant Mucositis, and Peri-Implantitis: Case Definitions and Diagnostic Considerations. J. Clin. Periodontol. 2018, 45, S278–S285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomasi, C.; Tessarolo, F.; Caola, I.; Piccoli, F.; Wennström, J.L.; Nollo, G.; Berglundh, T. Early Healing of Peri-implant Mucosa in Man. J. Clin. Periodontol. 2016, 43, 816–824. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-Implant Mucositis. J. Clin. Periodontol. 2018, 45, S237–S245. [Google Scholar] [CrossRef] [Green Version]
- Pontoriero, R.; Tonelli, M.P.; Carnevale, G.; Mombelli, A.; Nyman, S.R.; Lang, N.P. Experimentally Induced Peri-Implant Mucositis. A Clinical Study in Humans: Experimental Peri-Implant Mucositis. Clin. Oral Implant. Res. 1994, 5, 254–259. [Google Scholar] [CrossRef]
- Meyer, S.; Giannopoulou, C.; Courvoisier, D.; Schimmel, M.; Müller, F.; Mombelli, A. Experimental Mucositis and Experimental Gingivitis in Persons Aged 70 or over. Clinical and Biological Responses. Clin. Oral Implant. Res. 2017, 28, 1005–1012. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-Implantitis. J. Periodontol. 2018, 89, S267–S290. [Google Scholar] [CrossRef]
- Berglundh, T.; Zitzmann, N.U.; Donati, M. Are Peri-Implantitis Lesions Different from Periodontitis Lesions?: Peri-Implantitis and Periodontitis Lesions. J. Clin. Periodontol. 2011, 38, 188–202. [Google Scholar] [CrossRef]
- Berglundh, T.; Gislason, O.; Lekholm, U.; Sennerby, L.; Lindhe, J. Histopathological Observations of Human Periimplantitis Lesions. J. Clin. Periodontol. 2004, 31, 341–347. [Google Scholar] [CrossRef]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Peri-Implantitis—Onset and Pattern of Progression. J. Clin. Periodontol. 2016, 43, 383–388. [Google Scholar] [CrossRef]
- Fransson, C.; Tomasi, C.; Pikner, S.S.; Gröndahl, K.; Wennström, J.L.; Leyland, A.H.; Berglundh, T. Severity and Pattern of Peri-Implantitis-Associated Bone Loss. J. Clin. Periodontol. 2010, 37, 442–448. [Google Scholar] [CrossRef]
- Fowkes, F.G.; Dobson, A.J.; Hensley, M.J.; Leeder, S.R. The Role of Clinical Epidemiology in Medical Practice. Eff. Health Care 1984, 1, 259–265. [Google Scholar]
- Derks, J.; Tomasi, C. Peri-Implant Health and Disease. A Systematic Review of Current Epidemiology. J. Clin. Periodontol. 2015, 42, S158–S171. [Google Scholar] [CrossRef]
- Lee, C.-T.; Huang, Y.-W.; Zhu, L.; Weltman, R. Prevalences of Peri-Implantitis and Peri-Implant Mucositis: Systematic Review and Meta-Analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Rakic, M.; Galindo-Moreno, P.; Monje, A.; Radovanovic, S.; Wang, H.-L.; Cochran, D.; Sculean, A.; Canullo, L. How Frequent Does Peri-Implantitis Occur? A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2018, 22, 1805–1816. [Google Scholar] [CrossRef]
- Dreyer, H.; Grischke, J.; Tiede, C.; Eberhard, J.; Schweitzer, A.; Toikkanen, S.E.; Glöckner, S.; Krause, G.; Stiesch, M. Epidemiology and Risk Factors of Peri-Implantitis: A Systematic Review. J. Periodontal Res. 2018, 53, 657–681. [Google Scholar] [CrossRef]
- Cosgarea, R.; Sculean, A.; Shibli, J.A.; Salvi, G.E. Prevalence of Peri-Implant Diseases—A Critical Review on the Current Evidence. Braz. Oral Res. 2019, 33, e063. [Google Scholar] [CrossRef] [Green Version]
- Renvert, S.; Polyzois, I.; Claffey, N. Surgical Therapy for the Control of Peri-Implantitis. Clin. Oral Implant. Res. 2012, 23, 84–94. [Google Scholar] [CrossRef]
- Rinke, S.; Ohl, S.; Ziebolz, D.; Lange, K.; Eickholz, P. Prevalence of Periimplant Disease in Partially Edentulous Patients: A Practice-Based Cross-Sectional Study. Clin. Oral Implant. Res. 2011, 22, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Roos-Jansåker, A.M.; Lindahl, C.; Renvert, H.; Renvert, S. Nine- to Fourteen-Year Follow-up of Implant Treatment. Part I: Implant Loss and Associations to Various Factors. J. Clin. Periodontol. 2006, 33, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Catena, A.; Borgnakke, W.S. Association between Diabetes Mellitus/Hyperglycaemia and Peri-Implant Diseases: Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2017, 44, 636–648. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, M.; De Angelis, N.; Bonino, L.; Aglietta, M. Ten-Year Results of a Three-Arm Prospective Cohort Study on Implants in Periodontally Compromised Patients. Part 1: Implant Loss and Radiographic Bone Loss. Clin. Oral Implant. Res. 2010, 21, 490–496. [Google Scholar] [CrossRef]
- Serino, G.; Ström, C. Peri-Implantitis in Partially Edentulous Patients: Association with Inadequate Plaque Control. Clin. Oral Implant. Res. 2009, 20, 169–174. [Google Scholar] [CrossRef]
- Staubli, N.; Walter, C.; Schmidt, J.C.; Weiger, R.; Zitzmann, N.U. Excess Cement and the Risk of Peri-Implant Disease—A Systematic Review. Clin. Oral Impl. Res. 2017, 28, 1278–1290. [Google Scholar] [CrossRef]
- Scarano, A.; Inchingolo, F.; Scogna, S.; Leo, L.; Greco Lucchina, A.; Mavriqi, L. Peri-Implant Disease Caused by Residual Cement around Implant-Supported Restorations: A Clinical Report. J. Biol. Regul. Homeost. Agents 2021, 35, 211–216. [Google Scholar] [CrossRef]
- Costa, F.O.; Takenaka-Martinez, S.; Cota, L.O.M.; Ferreira, S.D.; Silva, G.L.M.; Costa, J.E. Peri-Implant Disease in Subjects with and without Preventive Maintenance: A 5-Year Follow-Up. J. Clin. Periodontol. 2012, 39, 173–181. [Google Scholar] [CrossRef]
- Lin, G.-H.; Chan, H.-L.; Wang, H.-L. The Significance of Keratinized Mucosa on Implant Health: A Systematic Review. J. Periodontol. 2013, 84, 1755–1767. [Google Scholar] [CrossRef]
- Gobbato, L.; Avila-Ortiz, G.; Sohrabi, K.; Wang, C.-W.; Karimbux, N. The Effect of Keratinized Mucosa Width on Peri-Implant Health: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2013, 28, 1536–1545. [Google Scholar] [CrossRef] [Green Version]
- Wilson, T.G.; Valderrama, P.; Burbano, M.; Blansett, J.; Levine, R.; Kessler, H.; Rodrigues, D.C. Foreign Bodies Associated with Peri-Implantitis Human Biopsies. J. Periodontol. 2015, 86, 9–15. [Google Scholar] [CrossRef]
- Noumbissi, S.; Scarano, A.; Gupta, S. A Literature Review Study on Atomic Ions Dissolution of Titanium and Its Alloys in Implant Dentistry. Materials 2019, 12, 368. [Google Scholar] [CrossRef] [Green Version]
- Daubert, D.; Pozhitkov, A.; McLean, J.; Kotsakis, G. Titanium as a Modifier of the Peri-Implant Microbiome Structure. Clin. Implant Dent. Relat. Res. 2018, 20, 945–953. [Google Scholar] [CrossRef]
- Hashim, D.; Cionca, N. A Comprehensive Review of Peri-Implantitis Risk Factors. Curr. Oral Health Rep. 2020, 7, 262–273. [Google Scholar] [CrossRef]
- Sasada, Y.; Cochran, D.L. Implant-Abutment Connections: A Review of Biologic Consequences and Peri-Implantitis Implications. Int. J. Oral Maxillofac. Implant. 2017, 32, 1296–1307. [Google Scholar] [CrossRef] [Green Version]
- Carinci, F.; Lauritano, D.; Bignozzi, C.A.; Pazzi, D.; Candotto, V.; Santos de Oliveira, P.; Scarano, A. A New Strategy Against Peri-Implantitis: Antibacterial Internal Coating. Int. J. Mol. Sci. 2019, 20, 3897. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; de Oliveira, P.S.; Leo, L.; Festa, F.; Carinci, F.; Lorusso, F. Evaluation of a New Antibacterial Coating of the Internal Chamber of an Implant via Real Time Measurement of Volatile Organic Compounds (VOCs). Front. Biosci. 2021, 13, 216–225. [Google Scholar] [CrossRef]
- Sanz, M.; Chapple, I.L.; on behalf of Working Group 4 of the VIII European Workshop on Periodontology. Clinical Research on Peri-Implant Diseases: Consensus Report of Working Group 4. J. Clin. Periodontol. 2012, 39, 202–206. [Google Scholar] [CrossRef]
- Shibli, J.A.; Melo, L.; Ferrari, D.S.; Figueiredo, L.C.; Faveri, M.; Feres, M. Composition of Supra- and Subgingival Biofilm of Subjects with Healthy and Diseased Implants. Clin. Oral Implant. Res. 2008, 19, 975–982. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D. Periodontal Microbial Ecology. Periodontol. 2000 2005, 38, 135–187. [Google Scholar] [CrossRef]
- Albertini, M.; López-Cerero, L.; O’Sullivan, M.G.; Chereguini, C.F.; Ballesta, S.; Ríos, V.; Herrero-Climent, M.; Bullón, P. Assessment of Periodontal and Opportunistic Flora in Patients with Peri-Implantitis. Clin. Oral Implant. Res. 2015, 26, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Ahn, D.-H.; Yu, Y.; Han, H.; Kim, S.Y.; Joo, J.-Y.; Chung, J.; Na, H.S.; Lee, J.-Y. Microbial Profiling of Peri-Implantitis Compared to the Periodontal Microbiota in Health and Disease Using 16S RRNA Sequencing. J. Periodontal Implant Sci. 2023, 53, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Kensara, A.; Saito, H.; Mongodin, E.F.; Masri, R. Microbiological Profile of Peri-implantitis: Analyses of Microbiome within Dental Implants. J. Prosthodont. 2023. [Google Scholar] [CrossRef] [PubMed]
- Lafaurie, G.I.; Sabogal, M.A.; Castillo, D.M.; Rincón, M.V.; Gómez, L.A.; Lesmes, Y.A.; Chambrone, L. Microbiome and Microbial Biofilm Profiles of Peri-Implantitis: A Systematic Review. J. Periodontol. 2017, 88, 1066–1089. [Google Scholar] [CrossRef]
- Persson, G.R.; Renvert, S. Cluster of Bacteria Associated with Peri-Implantitis: Pathogens in Peri-Implantitis. Clin. Implant Dent. Relat. Res. 2014, 16, 783–793. [Google Scholar] [CrossRef]
- Schwarz, F.; Becker, K.; Rahn, S.; Hegewald, A.; Pfeffer, K.; Henrich, B. Real-Time PCR Analysis of Fungal Organisms and Bacterial Species at Peri-Implantitis Sites. Int. J. Implant Dent. 2015, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Jankovic, S.; Aleksic, Z.; Dimitrijevic, B.; Lekovic, V.; Camargo, P.; Kenney, B. Prevalence of Human Cytomegalovirus and Epstein-Barr Virus in Subgingival Plaque at Peri-Implantitis, Mucositis and Healthy Sites. A Pilot Study. Int. J. Oral Maxillofac. Surg. 2011, 40, 271–276. [Google Scholar] [CrossRef]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Primary Prevention of Peri-Implantitis: Managing Peri-Implant Mucositis. J. Clin. Periodontol. 2015, 42, S152–S157. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Chapple, I.L.C.; Jepsen, S.; Sanz, M. Primary and Secondary Prevention of Periodontal and Peri-Implant Diseases: Introduction to, and Objectives of the 11 th European Workshop on Periodontology Consensus Conference. J. Clin. Periodontol. 2015, 42, S1–S4. [Google Scholar] [CrossRef]
- Sinjab, K.; Garaicoa-Pazmino, C.; Wang, H.-L. Decision Making for Management of Periimplant Diseases. Implant Dent. 2018, 27, 276–281. [Google Scholar] [CrossRef]
- Kormas, I.; Pedercini, C.; Pedercini, A.; Raptopoulos, M.; Alassy, H.; Wolff, L.F. Peri-Implant Diseases: Diagnosis, Clinical, Histological, Microbiological Characteristics and Treatment Strategies. A Narrative Review. Antibiotics 2020, 9, 835. [Google Scholar] [CrossRef]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of Peri-Implant Mucositis and Peri-Implantitis. Periodontol. 2000 2014, 66, 255–273. [Google Scholar] [CrossRef]
- Wilson, T.G.; Valderrama, P.; Rodrigues, D.B.C. Commentary: The Case for Routine Maintenance of Dental Implants. J. Periodontol. 2014, 85, 657–660. [Google Scholar] [CrossRef]
- Schmidt, K.E.; Auschill, T.M.; Heumann, C.; Frankenberger, R.; Eick, S.; Sculean, A.; Arweiler, N.B. Influence of Different Instrumentation Modalities on the Surface Characteristics and Biofilm Formation on Dental Implant Neck, In Vitro. Clin. Oral Implant. Res. 2017, 28, 483–490. [Google Scholar] [CrossRef]
- Renvert, S.; Samuelsson, E.; Lindahl, C.; Persson, G.R. Mechanical Non-Surgical Treatment of Peri-Implantitis: A Double-Blind Randomized Longitudinal Clinical Study. I: Clinical Results. J. Clin. Periodontol. 2009, 36, 604–609. [Google Scholar] [CrossRef]
- Sirinirund, B.; Garaicoa-Pazmino, C.; Wang, H.-L. Effects of Mechanical Instrumentation with Commercially Available Instruments Used in Supportive Peri-Implant Therapy: An In Vitro Study. Int. J. Oral Maxillofac. Implant. 2019, 34, 1370–1378. [Google Scholar] [CrossRef]
- Tastepe, C.S.; van Waas, R.; Liu, Y.; Wismeijer, D. Air Powder Abrasive Treatment as an Implant Surface Cleaning Method: A Literature Review. Int. J. Oral Maxillofac. Implant. 2012, 27, 1461–1473. [Google Scholar]
- Schwarz, F.; Becker, K.; Renvert, S. Efficacy of Air Polishing for the Non-Surgical Treatment of Peri-Implant Diseases: A Systematic Review. J. Clin. Periodontol. 2015, 42, 951–959. [Google Scholar] [CrossRef]
- Pisano, M.; Amato, A.; Sammartino, P.; Iandolo, A.; Martina, S.; Caggiano, M. Laser Therapy in the Treatment of Peri-Implantitis: State-of-the-Art, Literature Review and Meta-Analysis. Appl. Sci. 2021, 11, 5290. [Google Scholar] [CrossRef]
- Renvert, S.; Lindahl, C.; Roos Jansåker, A.-M.; Persson, G.R. Treatment of Peri-Implantitis Using an Er:YAG Laser or an Air-Abrasive Device: A Randomized Clinical Trial: Non-Surgical Treatment of Peri-Implantitis. J. Clin. Periodontol. 2011, 38, 65–73. [Google Scholar] [CrossRef]
- Schwarz, F.; Bieling, K.; Bonsmann, M.; Latz, T.; Becker, J. Nonsurgical Treatment of Moderate and Advanced Periimplantitis Lesions: A Controlled Clinical Study. Clin. Oral Investig. 2006, 10, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Ramanauskaite, A.; Schwarz, F.; Cafferata, E.A.; Sahrmann, P. Photo/Mechanical and Physical Implant Surface Decontamination Approaches in Conjunction with Surgical Peri-Implantitis Treatment: A Systematic Review. J. Clin. Periodontol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Sivaramakrishnan, G.; Sridharan, K. Photodynamic Therapy for the Treatment of Peri-Implant Diseases: A Network Meta-Analysis of Randomized Controlled Trials. Photodiagn. Photodyn. Ther. 2018, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Garaicoa-Pazmino, C.; Sinjab, K.; Wang, H.-L. Current Protocols for the Treatment of Peri-Implantitis. Curr. Oral Health Rep. 2019, 6, 209–217. [Google Scholar] [CrossRef]
- Dommisch, H.; Hoedke, D.; Valles, C.; Vilarrasa, J.; Jepsen, S.; Pascual La Rocca, A. Efficacy of Professionally Administered Chemical Agents as an Adjunctive Treatment to Sub-marginal Instrumentation during the Therapy of Peri-implant Mucositis. J. Clin. Periodontol. 2022. [Google Scholar] [CrossRef]
- Wilensky, A.; Shapira, L.; Limones, A.; Martin, C. The Efficacy of Implant Surface Decontamination Using Chemicals during Surgical Treatment of Peri-Implantitis: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2023. [Google Scholar] [CrossRef]
- Galofré, M.; Palao, D.; Vicario, M.; Nart, J.; Violant, D. Clinical and Microbiological Evaluation of the Effect of Lactobacillus Reuteri in the Treatment of Mucositis and Peri-Implantitis: A Triple-Blind Randomized Clinical Trial. J. Periodont. Res. 2018, 53, 378–390. [Google Scholar] [CrossRef]
- Hallström, H.; Persson, G.R.; Lindgren, S.; Olofsson, M.; Renvert, S. Systemic Antibiotics and Debridement of Peri-Implant Mucositis. A Randomized Clinical Trial. J. Clin. Periodontol. 2012, 39, 574–581. [Google Scholar] [CrossRef]
- Pulcini, A.; Bollaín, J.; Sanz-Sánchez, I.; Figuero, E.; Alonso, B.; Sanz, M.; Herrera, D. Clinical Effects of the Adjunctive Use of a 0.03% Chlorhexidine and 0.05% Cetylpyridinium Chloride Mouth Rinse in the Management of Peri-Implant Diseases: A Randomized Clinical Trial. J. Clin. Periodontol. 2019, 46, 342–353. [Google Scholar] [CrossRef]
- Gennai, S.; Bollain, J.; Ambrosio, N.; Marruganti, C.; Graziani, F.; Figuero, E. Efficacy of Adjunctive Measures in Peri-implant Mucositis. A Systematic Review and Meta-analysis. J. Clin. Periodontol. 2023. [Google Scholar] [CrossRef]
- Teughels, W.; Seyssens, L.; Christiaens, V.; Temmerman, A.; Castro, A.B.; Cosyn, J. Adjunctive Locally and Systemically Delivered Antimicrobials during Surgical Treatment of Peri-implantitis: A Systematic Review. J. Clin. Periodontol. 2023. [Google Scholar] [CrossRef]
- Verdugo, F. Risk of Superinfection in Peri-Implantitis After Systemic Broad Spectrum Antibiotics. Int. J. Periodont. Restor. Dent. 2018, 38, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Koch, F.P.; Kaemmerer, P.W.; Biesterfeld, S.; Kunkel, M.; Wagner, W. Effectiveness of Autofluorescence to Identify Suspicious Oral Lesions—A Prospective, Blinded Clinical Trial. Clin. Oral Investig. 2011, 15, 975–982. [Google Scholar] [CrossRef]
- Schneider, S.; Rudolph, M.; Bause, V.; Terfort, A. Electrochemical Removal of Biofilms from Titanium Dental Implant Surfaces. Bioelectrochemistry 2018, 121, 84–94. [Google Scholar] [CrossRef]
- Dhaliwal, J.S.; Abd Rahman, N.A.; Ming, L.C.; Dhaliwal, S.K.S.; Knights, J.; Albuquerque Junior, R.F. Microbial Biofilm Decontamination on Dental Implant Surfaces: A Mini Review. Front. Cell. Infect. Microbiol. 2021, 11, 736186. [Google Scholar] [CrossRef]
- Roccuzzo, A.; De Ry, S.P.; Sculean, A.; Roccuzzo, M.; Salvi, G.E. Current Approaches for the Non-Surgical Management of Peri-Implant Diseases. Curr. Oral Health Rep. 2020, 7, 274–282. [Google Scholar] [CrossRef]
- Subramani, K.; Wismeijer, D. Decontamination of Titanium Implant Surface and Re-Osseointegration to Treat Peri-Implantitis: A Literature Review. Int. J. Oral Maxillofac. Implant. 2012, 27, 1043–1054. [Google Scholar]
- Lindhe, J.; Meyle, J.; on behalf of Group D of the European Workshop on Periodontology. Peri-Implant Diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [Green Version]
- Ramanauskaite, A.; Fretwurst, T.; Schwarz, F. Efficacy of Alternative or Adjunctive Measures to Conventional Non-Surgical and Surgical Treatment of Peri-Implant Mucositis and Peri-Implantitis: A Systematic Review and Meta-Analysis. Int. J. Implant Dent. 2021, 7, 112. [Google Scholar] [CrossRef]
- Suárez-López del Amo, F.; Yu, S.-H.; Wang, H.-L. Non-Surgical Therapy for Peri-Implant Diseases: A Systematic Review. J. Oral Maxillofac. Res. 2016, 7, e13. [Google Scholar] [CrossRef] [Green Version]
- Renvert, S.; Polyzois, I.; Maguire, R. Re-Osseointegration on Previously Contaminated Surfaces: A Systematic Review. Clin. Oral Implant. Res. 2009, 20, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A.; Salvi, G.E.; Mombelli, A.; Faddy, M.; Lang, N.P.; On behalf of the Implant Complication Research Group Anti-Infective Surgical Therapy of Peri-Implantitis. A 12-Month Prospective Clinical Study. Clin. Oral Implant. Res. 2012, 23, 205–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carcuac, O.; Derks, J.; Abrahamsson, I.; Wennström, J.L.; Berglundh, T. Risk for Recurrence of Disease Following Surgical Therapy of Peri-Implantitis—A Prospective Longitudinal Study. Clin. Oral Implant. Res. 2020, 31, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Serino, G.; Turri, A. Outcome of Surgical Treatment of Peri-Implantitis: Results from a 2-Year Prospective Clinical Study in Humans: Outcome of Surgical Treatment of Peri-Implantitis. Clin. Oral Implant. Res. 2011, 22, 1214–1220. [Google Scholar] [CrossRef]
- Romeo, E.; Lops, D.; Chiapasco, M.; Ghisolfi, M.; Vogel, G. Therapy of Peri-Implantitis with Resective Surgery. A 3-Year Clinical Trial on Rough Screw-Shaped Oral Implants. Part II: Radiographic Outcome. Clin. Oral Implant. Res. 2007, 18, 179–187. [Google Scholar] [CrossRef]
- Aljohani, M.; Yong, S.L.; Bin Rahmah, A. The Effect of Surgical Regenerative Treatment for Peri-Implantitis: A Systematic Review. Saudi Dent. J. 2020, 32, 109–119. [Google Scholar] [CrossRef]
- Koo, K.-T.; Khoury, F.; Keeve, P.L.; Schwarz, F.; Ramanauskaite, A.; Sculean, A.; Romanos, G. Implant Surface Decontamination by Surgical Treatment of Periimplantitis: A Literature Review. Implant Dent. 2019, 28, 173–176. [Google Scholar] [CrossRef]
- Jepsen, K.; Jepsen, S.; Laine, M.L.; Anssari Moin, D.; Pilloni, A.; Zeza, B.; Sanz, M.; Ortiz-Vigon, A.; Roos-Jansåker, A.M.; Renvert, S. Reconstruction of Peri-Implant Osseous Defects: A Multicenter Randomized Trial. J. Dent. Res. 2016, 95, 58–66. [Google Scholar] [CrossRef]
- Aghazadeh, A.; Persson, R.G.; Renvert, S. Impact of Bone Defect Morphology on the Outcome of Reconstructive Treatment of Peri-Implantitis. Int. J. Implant Dent. 2020, 6, 33. [Google Scholar] [CrossRef]
- Chan, H.-L.; Lin, G.-H.; Suarez, F.; MacEachern, M.; Wang, H.-L. Surgical Management of Peri-Implantitis: A Systematic Review and Meta-Analysis of Treatment Outcomes. J. Periodontol. 2014, 85, 1027–1041. [Google Scholar] [CrossRef]
- Toma, S.; Brecx, M.C.; Lasserre, J.F. Clinical Evaluation of Three Surgical Modalities in the Treatment of Peri-Implantitis: A Randomized Controlled Clinical Trial. J. Clin. Med. 2019, 8, 966. [Google Scholar] [CrossRef] [Green Version]
- Tomasi, C.; Regidor, E.; Ortiz-Vigón, A.; Derks, J. Efficacy of Reconstructive Surgical Therapy at Peri-Implantitis-Related Bone Defects. A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2019, 46, 340–356. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; Ramanauskaite, A. It Is All about Peri-implant Tissue Health. Periodontol. 2000 2022, 88, 9–12. [Google Scholar] [CrossRef]
- Scarano, A.; Barros, R.R.M.; Iezzi, G.; Piattelli, A.; Novaes, A.B. Acellular Dermal Matrix Graft for Gingival Augmentation: A Preliminary Clinical, Histologic, and Ultrastructural Evaluation. J. Periodontol. 2009, 80, 253–259. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, A.; Polimeni, A.; Di Iorio, D.; Carinci, F. Bacterial Adhesion on Commercially Pure Titanium and Anatase-Coated Titanium Healing Screws: An In Vivo Human Study. J. Periodontol. 2010, 81, 1466–1471. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Peri-Implant Health | Peri-Implant Mucositis | Peri-Implantitis (With rx and Clinical Records) | Peri-Implantitis (No rx and Clinical Records | |
|---|---|---|---|---|
| Clinical signs of inflammation | − | + | + | + |
| BOP +/− suppuration | − | + | + | + |
| Increase in PD vs. previous visits | − | − | + | ≥6 mm |
| Radiographic bone loss (except physiological remodeling) | − | − | + physiological remodeling < 2 mm | ≥3 mm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarano, A.; Khater, A.G.A.; Gehrke, S.A.; Serra, P.; Francesco, I.; Di Carmine, M.; Tari, S.R.; Leo, L.; Lorusso, F. Current Status of Peri-Implant Diseases: A Clinical Review for Evidence-Based Decision Making. J. Funct. Biomater. 2023, 14, 210. https://doi.org/10.3390/jfb14040210
Scarano A, Khater AGA, Gehrke SA, Serra P, Francesco I, Di Carmine M, Tari SR, Leo L, Lorusso F. Current Status of Peri-Implant Diseases: A Clinical Review for Evidence-Based Decision Making. Journal of Functional Biomaterials. 2023; 14(4):210. https://doi.org/10.3390/jfb14040210
Chicago/Turabian StyleScarano, Antonio, Ahmad G. A. Khater, Sergio Alexandre Gehrke, Paola Serra, Inchingolo Francesco, Mariastella Di Carmine, Sergio Rexhep Tari, Lucia Leo, and Felice Lorusso. 2023. "Current Status of Peri-Implant Diseases: A Clinical Review for Evidence-Based Decision Making" Journal of Functional Biomaterials 14, no. 4: 210. https://doi.org/10.3390/jfb14040210