





Evaluation of the Hemostatic Effect of an Innovative Tissue Adhesive during Extraction Therapy under Rivaroxaban in a Rodent Model
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
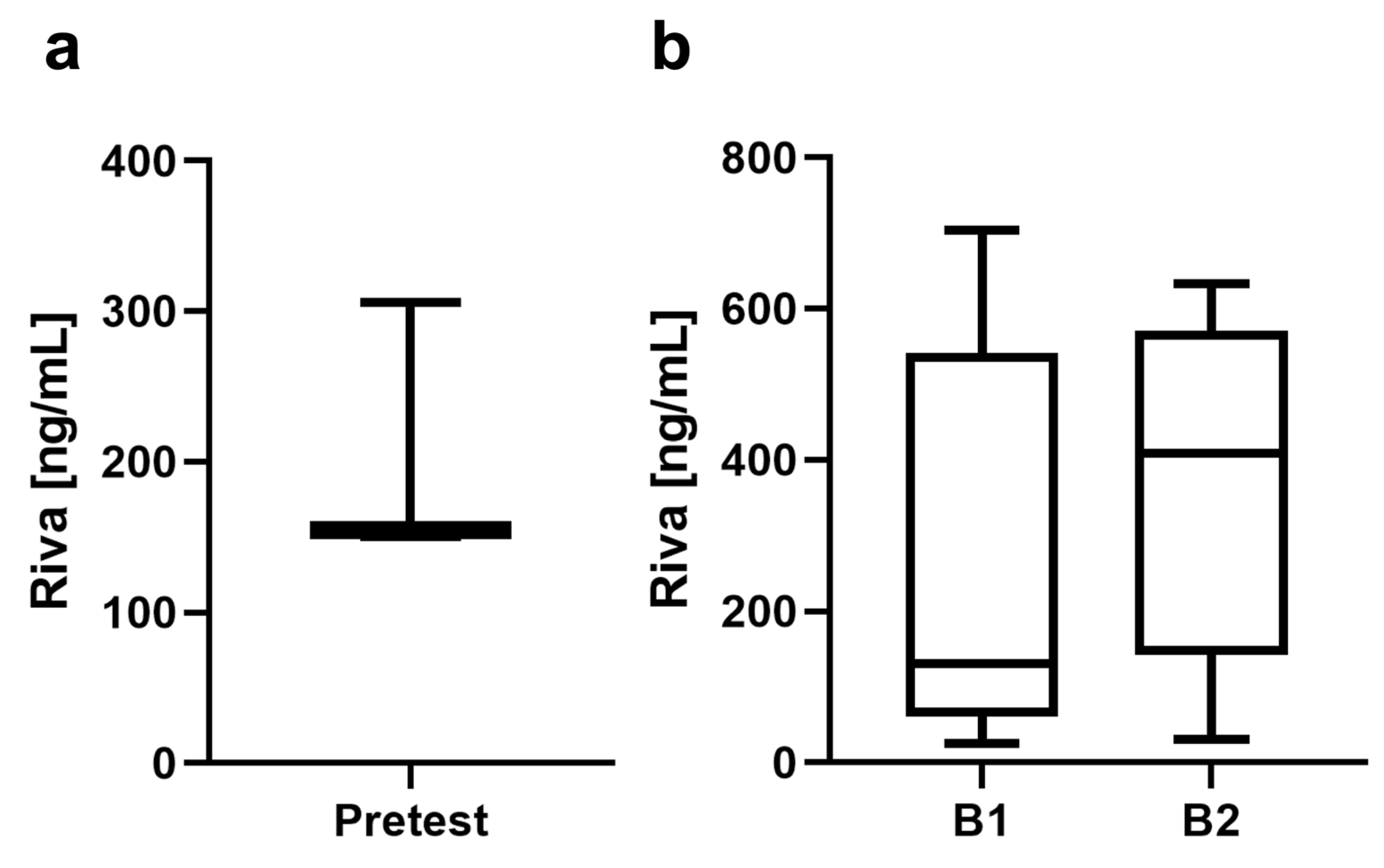
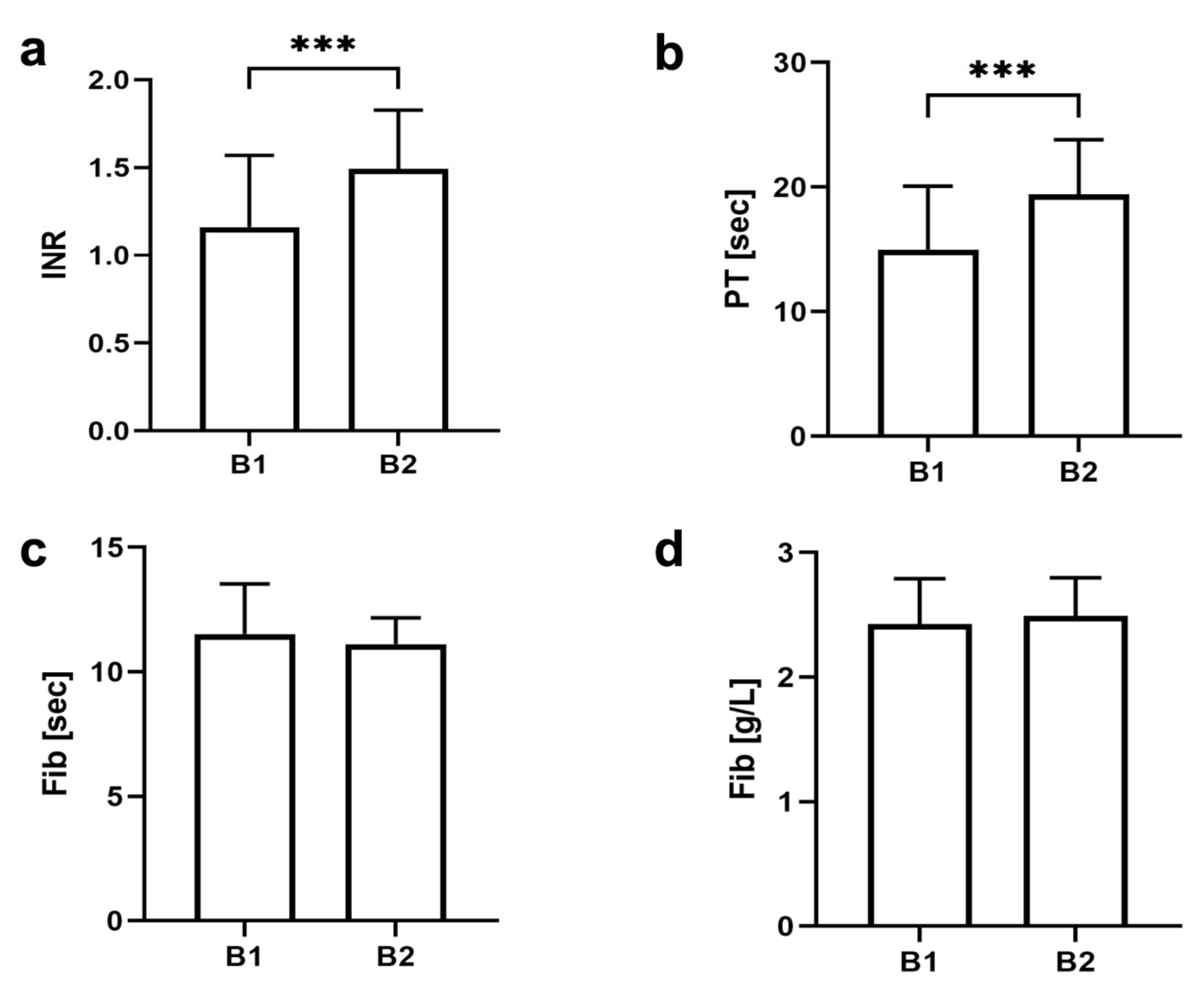
2.1. Blood Sample Determination
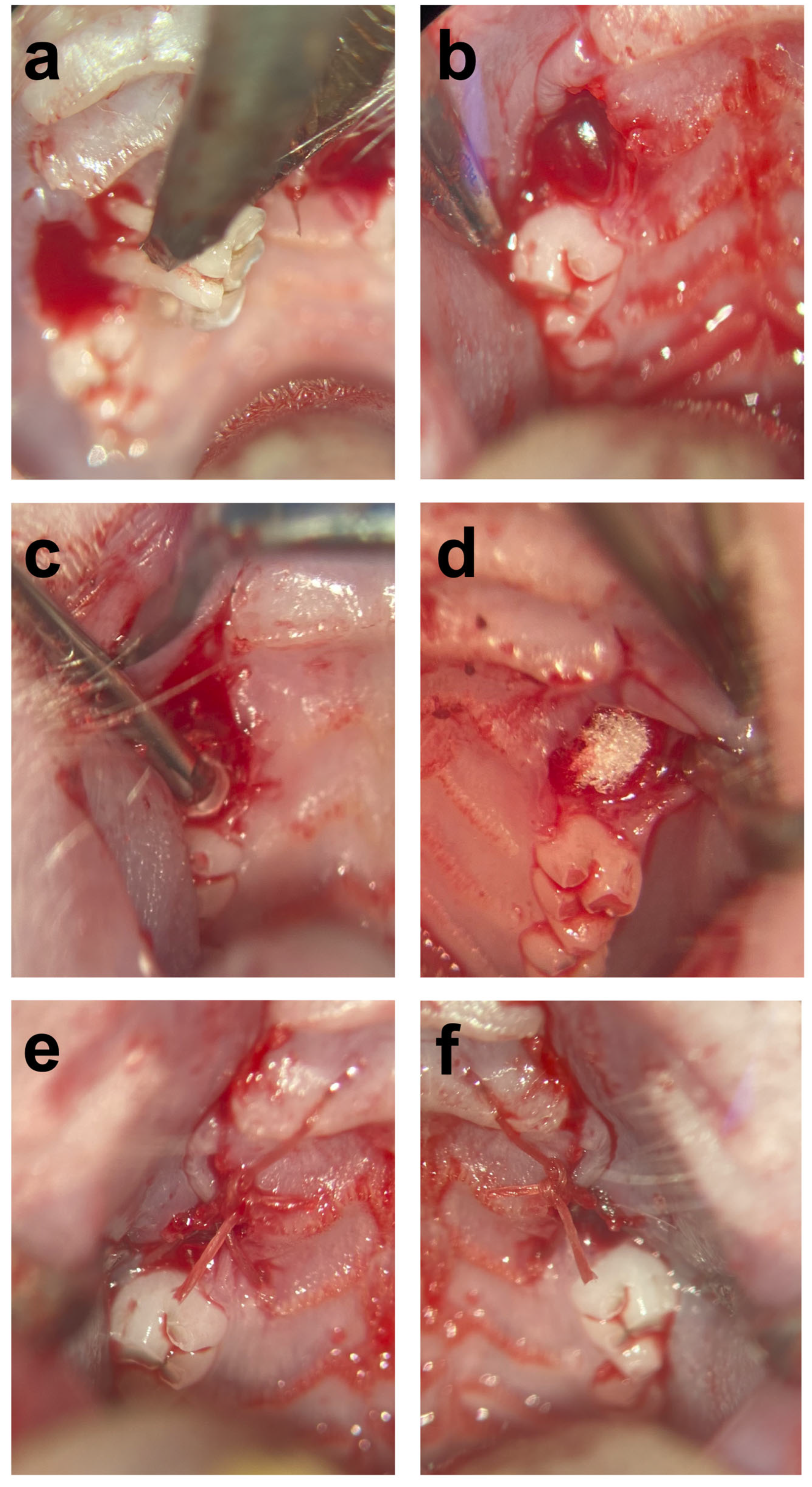
2.2. Surgical Procedures
2.3. Clinical Examination
2.4. Histomorphometric Analysis
2.5. Statistical Analysis
3. Results
3.1. Blood Sample Determination
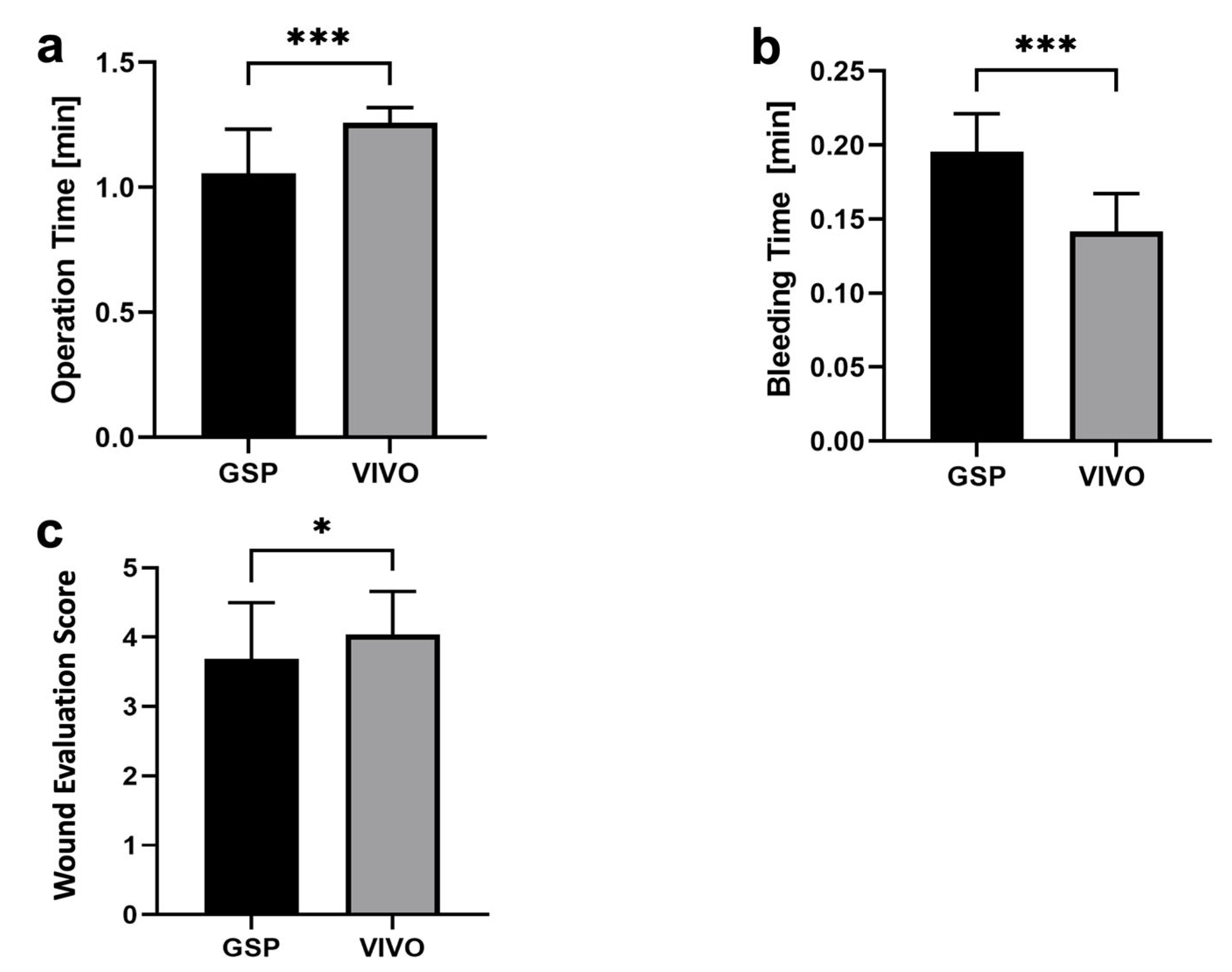
3.2. Surgical Procedures
3.3. Clinical Examination
3.4. Histomorphometric Analysis
4. Discussion
5. Conclusions
- The use of the polyurethane-based biodegradable tissue adhesive VIVO offers promising results in reducing postoperative bleeding risk in oral surgery;
- After 5 days, VIVO showed better wound healing regarding extraction sockets;
- Future studies with a higher number of extraction alveoli are essential for the further evaluation of the incidence of rebleeding with OATs and therapy with VIVO or GSP before transferring to human clinical use;
- Additionally, the degradation of the adhesive and the interaction of its degradation products on bone healing over the long term should be determined;
- Further research is needed to fully assess the efficacy and long-term safety of VIVO as a hemostatic agent in extraction sockets.
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boccatonda, A.; Frisone, A.; Lorusso, F.; Bugea, C.; Di Carmine, M.; Schiavone, C.; Cocco, G.; D’Ardes, D.; Scarano, A.; Guagnano, M.T. Perioperative Management of Antithrombotic Therapy in Patients Who Undergo Dental Procedures: A Systematic Review of the Literature and Network Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 5293. [Google Scholar] [CrossRef] [PubMed]
- Shaer, F.E.; Raslan, I.; Osaimi, N.A.; Bawazeer, G.; Alayobi, F.; Alhogbani, T.; Kharabsheh, S.; Habeeb, W.A. Documentation of various approaches and outcomes in patients on warfarin undergoing dental procedures: A review article. Am. J. Cardiovasc. Dis. 2016, 6, 109–117. [Google Scholar] [PubMed]
- Chaushu, L.P.N.; Botticelli, D.; Porfirio Xavier, S.; Kolerman, R.; Masri, D. The Effect of Anticoagulants on Early Implant Failure: A Retrospective Cohort Study. J. Funct. Biomater. 2023, 14, 186. [Google Scholar] [CrossRef]
- Miclotte, I.; Vanhaverbeke, M.; Agbaje, J.O.; Legrand, P.; Vanassche, T.; Verhamme, P.; Politis, C. Pragmatic approach to manage new oral anticoagulants in patients undergoing dental extractions: A prospective case-control study. Clin. Oral Investig. 2017, 21, 2183–2188. [Google Scholar] [CrossRef]
- Riess, H.; Ay, C.; Bauersachs, R.; Becattini, C.; Beyer-Westendorf, J.; Cajfinger, F.; Chau, I.; Cohen, A.T.; Khorana, A.A.; Maraveyas, A.; et al. Use of Direct Oral Anticoagulants in Patients with Cancer: Practical Considerations for the Management of Patients with Nausea or Vomiting. Oncologist 2018, 23, 822–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marzec, L.N.; Wang, J.; Shah, N.D.; Chan, P.S.; Ting, H.H.; Gosch, K.L.; Hsu, J.C.; Maddox, T.M. Influence of Direct Oral Anticoagulants on Rates of Oral Anticoagulation for Atrial Fibrillation. J. Am. Coll. Cardiol. 2017, 69, 2475–2484. [Google Scholar] [CrossRef]
- Galliazzo, S.; Donadini, M.P.; Ageno, W. Antidotes for the direct oral anticoagulants: What news? Thromb. Res. 2018, 164 (Suppl. S1), S119–S123. [Google Scholar] [CrossRef]
- Ballestri, S.; Romagnoli, E.; Arioli, D.; Coluccio, V.; Marrazzo, A.; Athanasiou, A.; Di Girolamo, M.; Cappi, C.; Marietta, M.; Capitelli, M. Risk and Management of Bleeding Complications with Direct Oral Anticoagulants in Patients with Atrial Fibrillation and Venous Thromboembolism: A Narrative Review. Adv. Ther. 2023, 40, 41–66. [Google Scholar] [CrossRef]
- Connors, J.M. Testing and monitoring direct oral anticoagulants. Blood 2018, 132, 2009–2015. [Google Scholar] [CrossRef] [Green Version]
- Halvorsen, S.; Ghanima, W.; Fride Tvete, I.; Hoxmark, C.; Falck, P.; Solli, O.; Jonasson, C. A nationwide registry study to compare bleeding rates in patients with atrial fibrillation being prescribed oral anticoagulants. Eur. Heart J. Cardiovasc. Pharmacother. 2017, 3, 28–36. [Google Scholar] [CrossRef]
- Nathwani, S.; Wanis, C. Novel oral anticoagulants and exodontia: The evidence. Br. Dent. J. 2017, 222, 623–628. [Google Scholar] [CrossRef]
- Inokoshi, M.; Kubota, K.; Yamaga, E.; Ueda, K.; Minakuchi, S. Postoperative bleeding after dental extraction among elderly patients under anticoagulant therapy. Clin. Oral Investig. 2021, 25, 2363–2371. [Google Scholar] [CrossRef]
- Berton, F.; Costantinides, F.; Stacchi, C.; Corradini, A.; Di Lenarda, A.; Di Lenarda, R. Is L-PRF an effective hemostatic agent in single tooth extractions? A cohort study on VKA and DOAC patients. Clin. Oral Investig. 2023, 27, 2865–2874. [Google Scholar] [CrossRef]
- Galletti, G.; Alfonsi, F.; Raffaele, A.; Valente, N.A.; Chatelain, S.; Kolerman, R.; Cinquini, C.; Romeggio, S.; Iezzi, G.; Barone, A. Implant Placement in Patients under Treatment with Rivaroxaban: A Retrospective Clinical Study. Int. J. Environ. Res. Public Health 2020, 17, 4607. [Google Scholar] [CrossRef]
- Manfredini, M.; Poli, P.P.; Creminelli, L.; Porro, A.; Maiorana, C.; Beretta, M. Comparative Risk of Bleeding of Anticoagulant Therapy with Vitamin K Antagonists (VKAs) and with Non-Vitamin K Antagonists in Patients Undergoing Dental Surgery. J. Clin. Med. 2021, 10, 5526. [Google Scholar] [CrossRef]
- Pippi, R.; Santoro, M.; Cafolla, A. The effectiveness of a new method using an extra-alveolar hemostatic agent after dental extractions in older patients on oral anticoagulation treatment: An intrapatient study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 15–21. [Google Scholar] [CrossRef]
- Kumbargere Nagraj, S.; Prashanti, E.; Aggarwal, H.; Lingappa, A.; Muthu, M.S.; Kiran Kumar Krishanappa, S.; Hassan, H. Interventions for treating post-extraction bleeding. Cochrane Database Syst. Rev. 2018, 3, CD011930. [Google Scholar] [CrossRef]
- Aldridge, E.; Cunningham, L.L., Jr. Current thoughts on treatment of patients receiving anticoagulation therapy. J. Oral Maxillofac. Surg. 2010, 68, 2879–2887. [Google Scholar] [CrossRef]
- Hamzah, N.A.; Graf, H.L.; Kaluderovic, M.R.; Meyer, A.L.; Dieterlen, M.T.; Hemprich, A. Haemostasis in oral surgical procedures involving patients with a ventricular assist device. Int. J. Oral Maxillofac. Surg. 2020, 49, 1355–1359. [Google Scholar] [CrossRef]
- Heitzer, M.; Ooms, M.; Katz, M.S.; Peters, F.; Kilic, K.; Tolba, R.; Jockenhoevel, S.; Hermanns-Sachweh, B.; Holzle, F.; Modabber, A. Evaluation of the long-term results of vascular anastomosis using polyurethane adhesive and shape-memory stent in the rat carotid artery model. Microsurgery 2022, 42, 480–489. [Google Scholar] [CrossRef]
- Fukushima, K.; Tanaka, H.; Kadaba Srinivasan, P.; Pawlowsky, K.; Kogel, B.; Uemoto, S.; Ku, Y.; Tolba, R.H. Hemostatic Efficacy and Safety of the Novel Medical Adhesive, MAR VIVO-107, in a Rabbit Liver Resection Model. Eur. Surg. Res. 2018, 59, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Schulten, L.; Spillner, J.; Kanzler, S.; Teubner, A.; Jockenhoevel, S.; Apel, C. A polyurethane-based surgical adhesive for sealing blood vessel anastomoses-A feasibility study in pigs. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 1922–1931. [Google Scholar] [CrossRef] [PubMed]
- Bremer, L.; Hagemeister, K.; Moss, M.; Ernst, L.; Tolba, R.H.; Jockenhoevel, S.; Apel, C. Long-Term Degradation Assessment of a Polyurethane-Based Surgical Adhesive-Assessment and Critical Consideration of Preclinical In Vitro and In Vivo Testing. J. Funct. Biomater. 2023, 14, 168. [Google Scholar] [CrossRef] [PubMed]
- Modabber, A.; Winnand, P.; Goloborodko, E.; Mohlhenrich, S.C.; Kniha, K.; Tolba, R.; Jockenhoevel, S.; Hermanns-Sachweh, B.; Holzle, F.; Heitzer, M. Biodegradation and Immunological Parameters of Polyurethane-Based Tissue Adhesive in Arterial Microvascular Anastomoses-A Long-Term In Vivo Study. Macromol. Biosci. 2022, 22, e2100451. [Google Scholar] [CrossRef] [PubMed]
- Ockerman, A.; Vanhaverbeke, M.; Miclotte, I.; Belmans, A.; Vanassche, T.; Politis, C.; Jacobs, R.; Verhamme, P. Tranexamic acid to reduce bleeding after dental extraction in patients treated with non-vitamin K oral anticoagulants: Design and rationale of the EXTRACT-NOAC trial. Br. J. Oral Maxillofac. Surg. 2019, 57, 1107–1112. [Google Scholar] [CrossRef]
- Hamzani, Y.; Chaushu, G. Evaluation of early wound healing scales/indexes in oral surgery: A literature review. Clin. Implant Dent. Relat. Res. 2018, 20, 1030–1035. [Google Scholar] [CrossRef]
- Quinn, J.V.; Wells, G.A. An assessment of clinical wound evaluation scales. Acad. Emerg. Med. 1998, 5, 583–586. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Moreno, G.; Aguilar-Salvatierra, A.; Fernandez-Cejas, E.; Delgado-Ruiz, R.A.; Markovic, A.; Calvo-Guirado, J.L. Dental implant surgery in patients in treatment with the anticoagulant oral rivaroxaban. Clin. Oral Implants Res. 2016, 27, 730–733. [Google Scholar] [CrossRef]
- Hiroshi, I.; Natsuko, S.Y.; Yutaka, I.; Masayori, S.; Hiroyuki, N.; Hirohisa, I. Frequency of hemorrhage after tooth extraction in patients treated with a direct oral anticoagulant: A multicenter cross-sectional study. PLoS ONE 2022, 17, e0266011. [Google Scholar] [CrossRef]
- Huang, J.; Liu, J.; Shi, H.; Wu, J.; Liu, J.; Pan, J. Risk factors for bleeding after dental extractions in patients receiving antithrombotic drugs—A case control study. J. Dent. Sci. 2022, 17, 780–786. [Google Scholar] [CrossRef]
- Yan, W.; Yang, F.; Liu, Z.; Wen, Q.; Gao, Y.; Niu, X.; Zhao, Y. Anti-Inflammatory and Mineralization Effects of an ASP/PLGA-ASP/ACP/PLLA-PLGA Composite Membrane as a Dental Pulp Capping Agent. J. Funct. Biomater. 2022, 13, 106. [Google Scholar] [CrossRef]
- Edanami, N.; Takenaka, S.; Ibn Belal, R.S.; Yoshiba, K.; Takahara, S.; Yoshiba, N.; Ohkura, N.; Noiri, Y. In Vivo Assessment of the Apatite-Forming Ability of New-Generation Hydraulic Calcium Silicate Cements Using a Rat Subcutaneous Implantation Model. J. Funct. Biomater. 2023, 14, 213. [Google Scholar] [CrossRef]
- Parry, T.J.; Huang, Z.; Chen, C.; Connelly, M.A.; Perzborn, E.; Andrade-Gordon, P.; Damiano, B.P. Arterial antithrombotic activity of rivaroxaban, an orally active factor Xa inhibitor, in a rat electrolytic carotid artery injury model of thrombosis. Blood Coagul. Fibrinolysis 2011, 22, 720–726. [Google Scholar] [CrossRef]
- Gu, J.T.; Jiao, K.; Li, J.; Yan, J.F.; Wang, K.Y.; Wang, F.; Liu, Y.; Tay, F.R.; Chen, J.H.; Niu, L.N. Polyphosphate-crosslinked collagen scaffolds for hemostasis and alveolar bone regeneration after tooth extraction. Bioact. Mater. 2022, 15, 68–81. [Google Scholar] [CrossRef]
- Liu, F.D.; Zhao, R.; Feng, X.Y.; Shi, Y.H.; Wu, Y.L.; Shen, X.L.; Li, G.F.; Liu, Y.S.; Zhao, Y.; He, X.W.; et al. Rivaroxaban does not influence hemorrhagic transformation in a diabetes ischemic stroke and endovascular thrombectomy model. Sci. Rep. 2018, 8, 7408. [Google Scholar] [CrossRef] [Green Version]
- Weinz, C.; Schwarz, T.; Kubitza, D.; Mueck, W.; Lang, D. Metabolism and excretion of rivaroxaban, an oral, direct factor Xa inhibitor, in rats, dogs, and humans. Drug Metab. Dispos. 2009, 37, 1056–1064. [Google Scholar] [CrossRef]
- Guillou, S.; Beaumont, J.; Tamareille, S.; Giraud, S.; Mirebeau-Prunier, D.; Prunier, F.; Macchi, L. Direct Rivaroxaban-Induced Factor XA Inhibition Proves to be Cardioprotective in Rats. Shock 2020, 53, 730–736. [Google Scholar] [CrossRef]
- Yoshikawa, H.; Yoshida, M.; Yasaka, M.; Yoshida, H.; Murasato, Y.; Fukunaga, D.; Shintani, A.; Okada, Y. Safety of tooth extraction in patients receiving direct oral anticoagulant treatment versus warfarin: A prospective observation study. Int. J. Oral Maxillofac. Surg. 2019, 48, 1102–1108. [Google Scholar] [CrossRef]
- Shigeishi, H.; Ohta, K.; Takechi, M. Risk factors for postoperative complications following oral surgery. J. Appl. Oral Sci. 2015, 23, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Jin, H. Rivaroxaban for treatment of livedoid vasculopathy: A systematic review. Dermatol. Ther. 2021, 34, e15051. [Google Scholar] [CrossRef] [PubMed]
- Schastlivtsev, I.; Lobastov, K.; Tsaplin, S.; Kanzafarova, I.; Barinov, V.; Laberko, L.; Rodoman, G.; Zhuravlev, S. Rivaroxaban in the treatment of upper extremity deep vein thrombosis: A single-center experience and review of the literature. Thromb. Res. 2019, 181, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Kniha, K.; Rink, L.; Wolf, J.; Mohlhenrich, S.C.; Peters, F.; Heitzer, M.; Holzle, F.; Modabber, A. Host inflammatory response and clinical parameters around implants in a rat model using systemic alendronate and zoledronate acid drug administrations. Sci. Rep. 2022, 12, 4431. [Google Scholar] [CrossRef]
- Cle-Ovejero, A.; Valmaseda-Castellon, E. Haemostatic agents in apical surgery. A systematic review. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e652–e657. [Google Scholar] [CrossRef] [Green Version]
- Zirk, M.; Fienitz, T.; Edel, R.; Kreppel, M.; Dreiseidler, T.; Rothamel, D. Prevention of post-operative bleeding in hemostatic compromised patients using native porcine collagen fleeces-retrospective study of a consecutive case series. Oral Maxillofac. Surg. 2016, 20, 249–254. [Google Scholar] [CrossRef]
- Lied, G.A.; Lund, K.B.; Storaas, T. Intraoperative anaphylaxis to gelatin-based hemostatic agents: A case report. J. Asthma Allergy 2019, 12, 163–167. [Google Scholar] [CrossRef] [Green Version]
- Heitzer, M.; Brockhaus, J.; Kniha, K.; Merkord, F.; Peters, F.; Holzle, F.; Goloborodko, E.; Modabber, A. Mechanical strength and hydrostatic testing of VIVO adhesive in sutureless microsurgical anastomoses: An ex vivo study. Sci. Rep. 2021, 11, 13598. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Absent/Present | |
|---|---|
| Protruding wound edges | 1/0 |
| Contour irregularities (wrinkling) | 1/0 |
| Distance between wound edges > 2 mm | 1/0 |
| Edge inversion (sinking, curling) | 1/0 |
| Inflammation (redness, discharge) | 1/0 |
| Overall cosmetic appearance (good/not good) | 1/0 |
| Group | Degree of Bleeding Mean ± SD | |||||
|---|---|---|---|---|---|---|
| Minor | Relevant | Major | ||||
| GSP (n = 31) | 2/31 (p = 0.56) | 0.07 ± 0.26 | 0/31 | 0.00 | 0/31 | 0.00 |
| VIVO (n = 31) | 1/31 (p = 0.56) | 0.03 ± 0.19 | 0/31 | 0.00 | 0/31 | 0.00 |
| Group | Early Bleeding Mean ± SD | Delayed Bleeding Mean ± SD | ||
|---|---|---|---|---|
| GSP (n = 31) | 2/31 (p = 0.56) | 0.07 ± 0.26 | 0/31 | 0.00 |
| VIVO (n = 31) | 1/31 (p = 0.56) | 0.03 ± 0.19 | 0/31 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heitzer, M.; Winnand, P.; Bock, A.; Ooms, M.; Katz, M.S.; Kniha, K.; Grottke, O.; Hölzle, F.; Modabber, A. Evaluation of the Hemostatic Effect of an Innovative Tissue Adhesive during Extraction Therapy under Rivaroxaban in a Rodent Model. J. Funct. Biomater. 2023, 14, 333. https://doi.org/10.3390/jfb14070333
Heitzer M, Winnand P, Bock A, Ooms M, Katz MS, Kniha K, Grottke O, Hölzle F, Modabber A. Evaluation of the Hemostatic Effect of an Innovative Tissue Adhesive during Extraction Therapy under Rivaroxaban in a Rodent Model. Journal of Functional Biomaterials. 2023; 14(7):333. https://doi.org/10.3390/jfb14070333
Chicago/Turabian StyleHeitzer, Marius, Philipp Winnand, Anna Bock, Mark Ooms, Marie Sophie Katz, Kristian Kniha, Oliver Grottke, Frank Hölzle, and Ali Modabber. 2023. "Evaluation of the Hemostatic Effect of an Innovative Tissue Adhesive during Extraction Therapy under Rivaroxaban in a Rodent Model" Journal of Functional Biomaterials 14, no. 7: 333. https://doi.org/10.3390/jfb14070333