
Reverse Torque Value of Angulated Screw Channel Abutment before and after Cyclic Loading: An In Vitro Study
Abstract
:1. Introduction
2. Materials and Methods
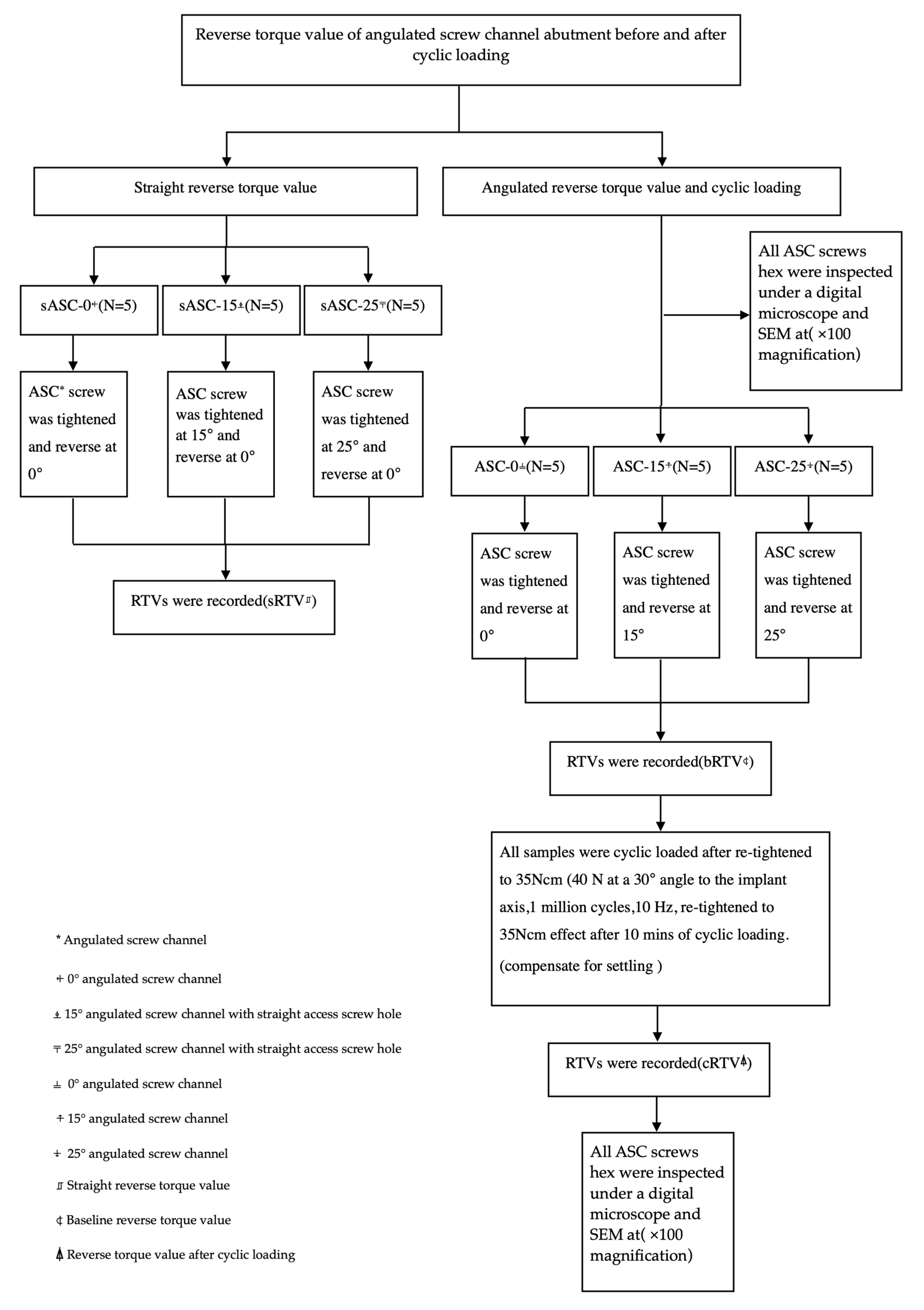
2.1. Straight Reverse Torque Value
2.2. Angulated Reverse Torque Value and Cyclic Loading
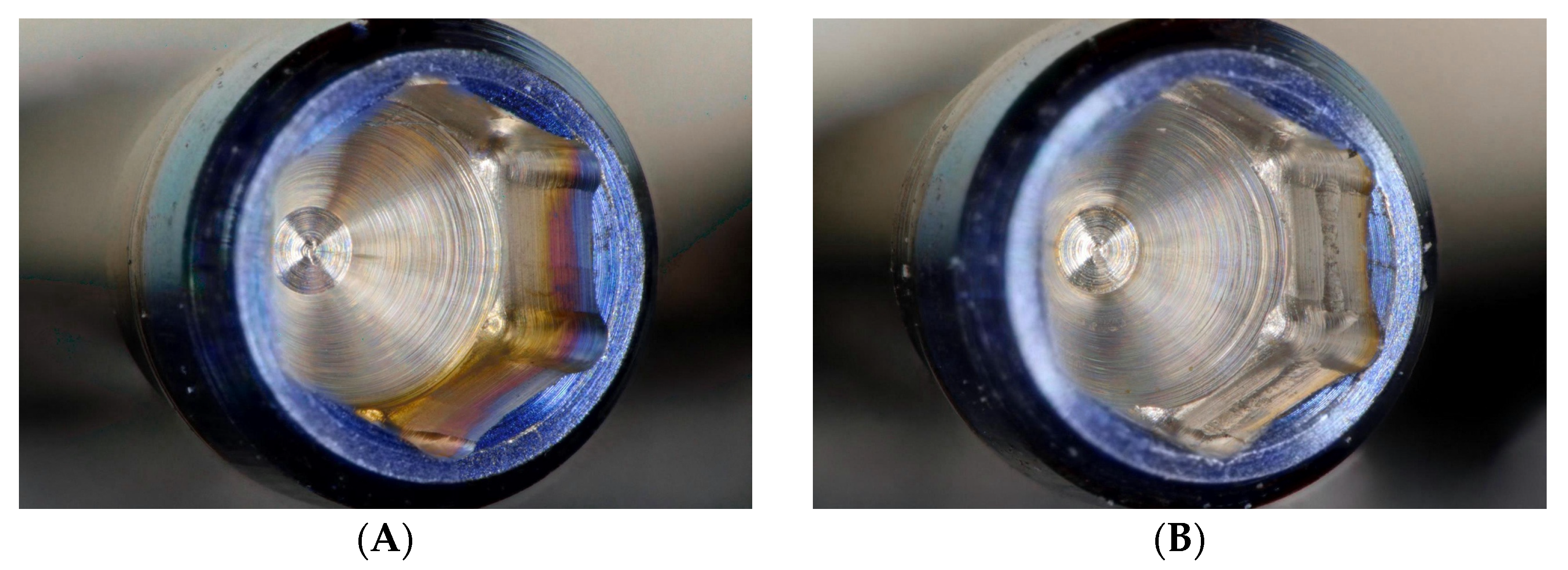
2.3. Microscope and SEM Examination
Statistical Analysis
3. Results
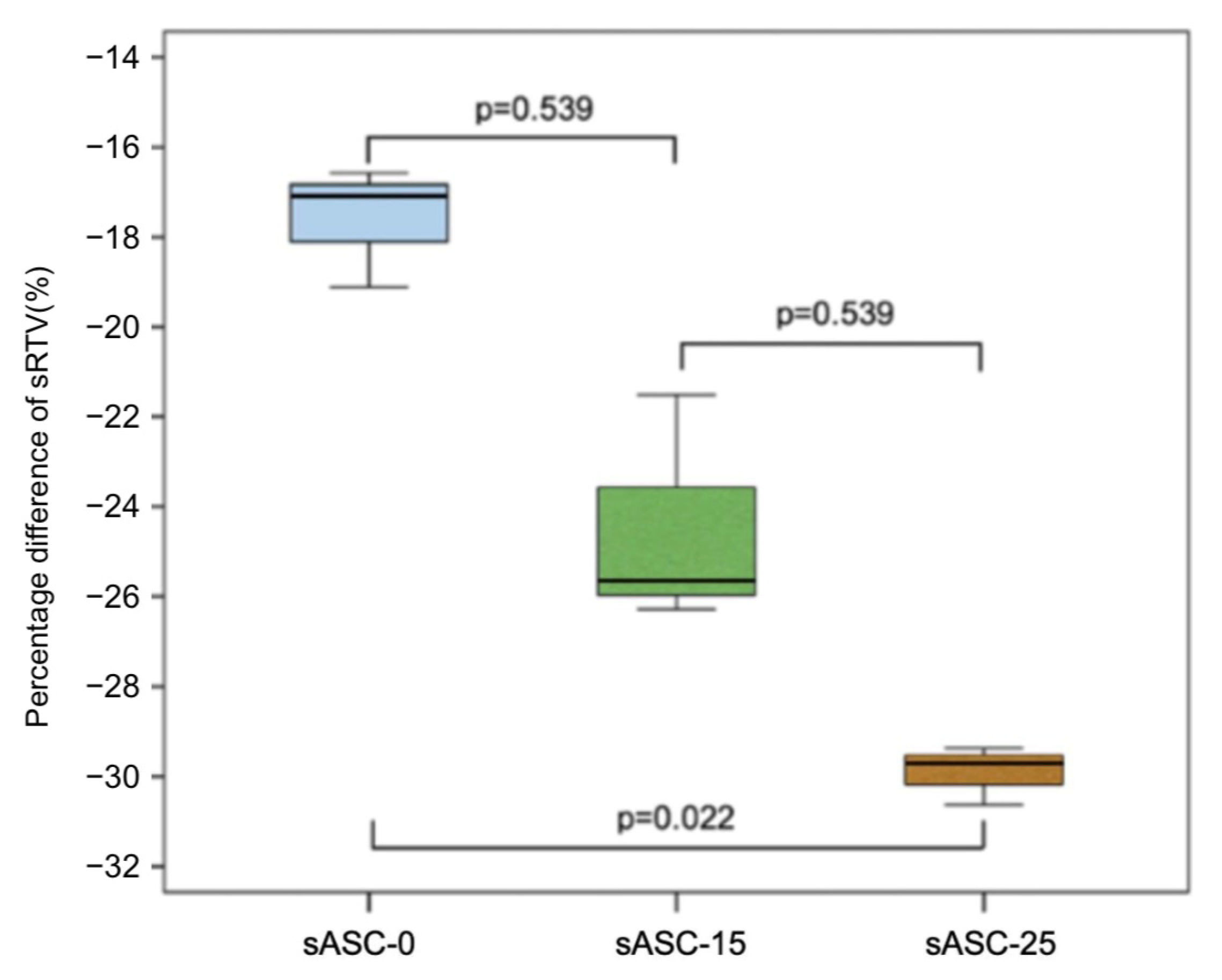
3.1. Straight Reverse Torque Value Percentage Difference
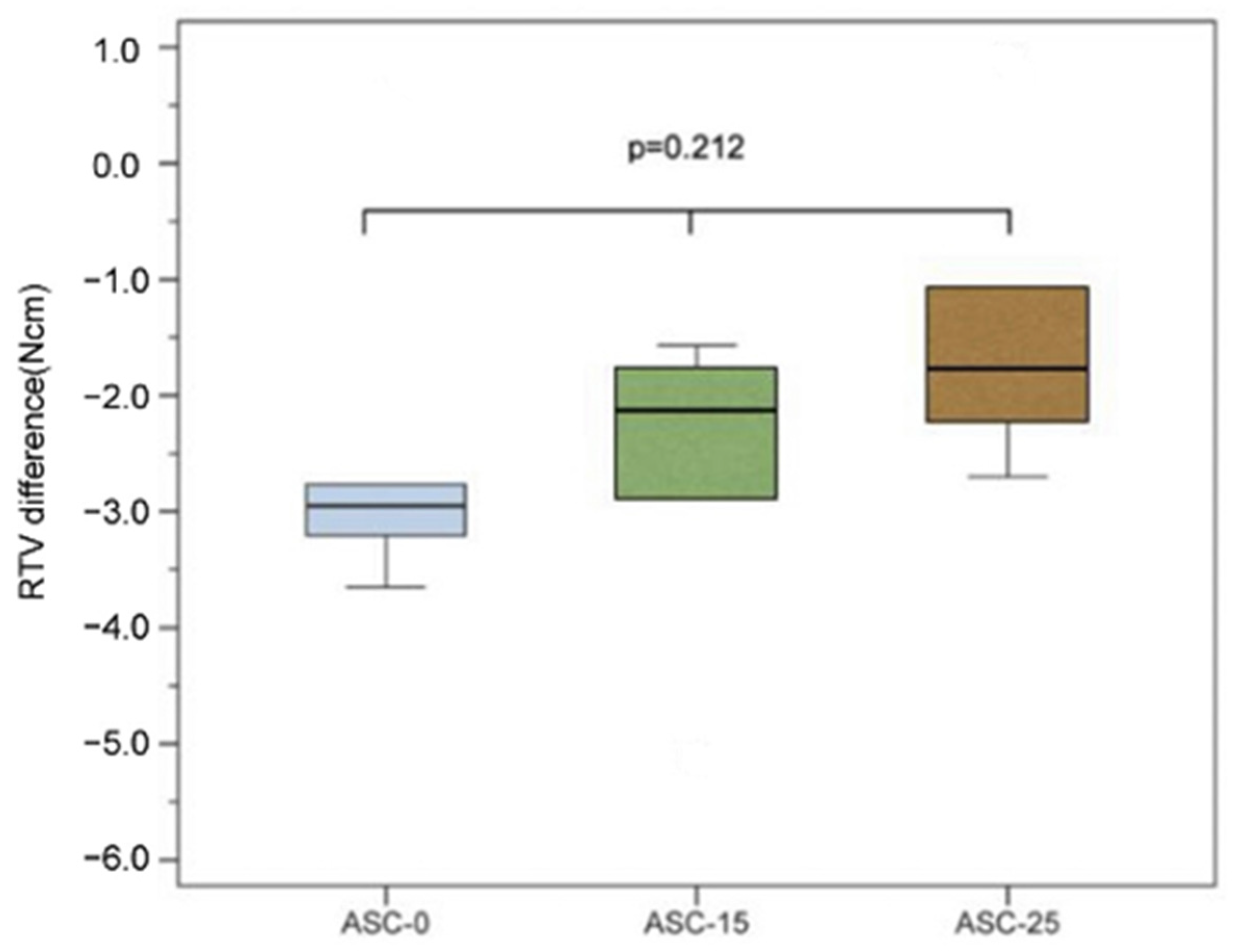
3.2. Angulated Reverse Torque Value and RTV Difference after Cyclic Loading
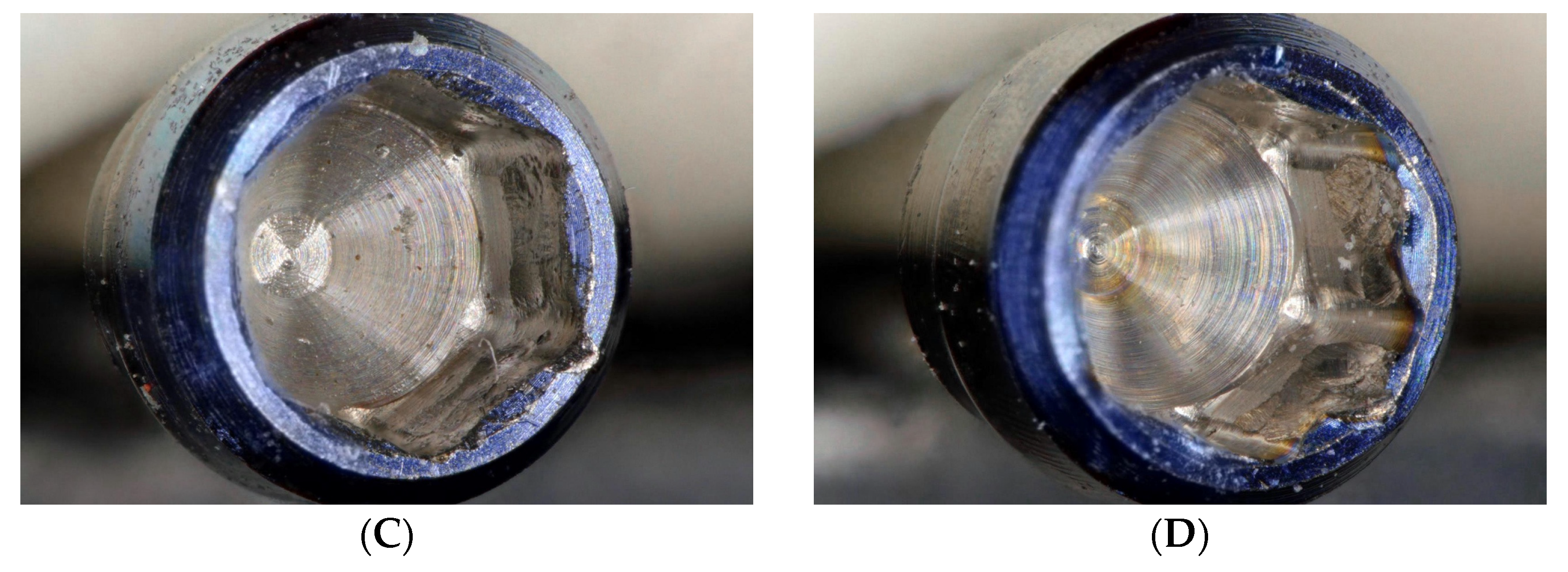
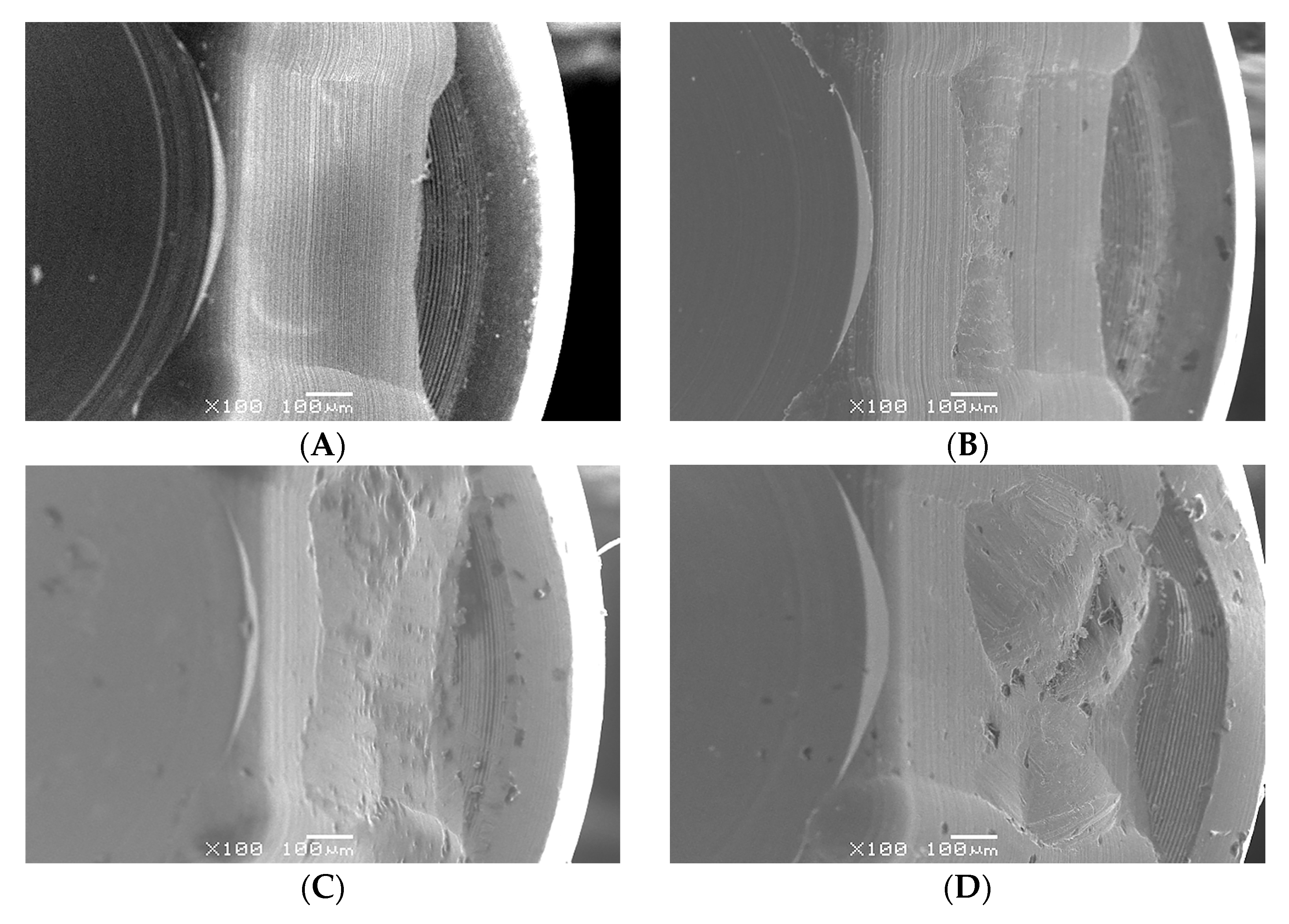
3.3. Microscope and SEM Examination
4. Discussion
5. Conclusions
- The ASC angle will affect the actual preload acting on the abutment screw and the larger the ASC angle, the lower the preload.
- The RTV of the ASC of all groups decreased after cyclic loading, and there was no significant difference between the 0° and angled groups. Thus, the performance of angled ASCs after cyclic loading was comparable to that of 0° ASC.
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Corbella, S.; Alberti, A.; Calciolari, E.; Francetti, L. Medium- and long-term survival rates of implant-supported single and partial restorations at a maximum follow-up of 12 years: A Retrospective Study. Int. J. Prosthodont. 2021, 34, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- French, D.; Ofec, R.; Levin, L. Long term clinical performance of 10871 dental implants with up to 22 years of follow-up: A cohort study in 4247 patients. Clin. Implant. Dent. Relat. Res. 2021, 23, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.C.; Cornacchia, T.M.; de Magalhães, C.S.; Bueno, A.C.; Moreira, A.N. Biomechanical evaluation of screw- and cement-retained implant-supported prostheses: A nonlinear finite element analysis. J. Prosthet. Dent. 2014, 112, 1479–1488. [Google Scholar] [CrossRef] [PubMed]
- Cosola, S.; Toti, P.; Babetto, E.; Covani, U.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. In-vitro fatigue and fracture performance of three different ferrulized implant connections used in fixed prosthesis. J. Dent. Sci. 2021, 16, 397–403. [Google Scholar] [CrossRef]
- Pellizzer, E.P.; Tonella, B.P.; Ferraço, R.; Falcón-Antenucci, R.M.; de Carvalho, P.S.; Alves-Rezende, M.C. Photoelastic stress analysis in screwed and cemented implant-supported dentures with external hexagon implants. J. Craniofac. Surg. 2010, 21, 1110–1113. [Google Scholar] [CrossRef]
- Linkevicius, T.; Puisys, A.; Vindasiute, E.; Linkeviciene, L.; Apse, P. Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis. Clin. Oral. Implant. Res. 2013, 24, 1179–1184. [Google Scholar] [CrossRef]
- Sailer, I.; Mühlemann, S.; Zwahlen, M.; Hämmerle, C.H.; Schneider, D. Cemented and screw-retained implant reconstructions: A systematic review of the survival and complication rates. Clin. Oral. Implant. Res. 2012, 23 (Suppl. 6), 163–201. [Google Scholar] [CrossRef]
- Berroeta, E.; Zabalegui, I.; Donovan, T.; Chee, W. Dynamic abutment: A method of redirecting screw access for implant-supported restorations: Technical details and a clinical report. J. Prosthet. Dent. 2015, 113, 516–519. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.; Lee, T.; Phark, J.H.; Chee, W. Removal torque and force to failure of non-axially tightened implant abutment screws. J. Prosthet. Dent. 2019, 121, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Swamidass, R.S.; Kan, J.Y.; Kattadiyil, M.T.; Goodacre, C.J.; Lozada, J. Abutment screw torque changes with straight and angled screw-access channels. J. Prosthet. Dent. 2021, 125, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Mulla, S.H.; Seghi, R.R.; Johnston, W.M.; Yilmaz, B. Effect of cyclic loading on reverse torque values of angled screw channel systems. J. Prosthet. Dent. 2022, 128, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Byrne, D.; Jacobs, S.; O’Connell, B.; Houston, F.; Claffey, N. Preloads generated with repeated tightening in three types of screws used in dental implant assemblies. J. Prosthodont. 2006, 15, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Jorge, J.R.P.; Barao, V.A.R.; Delben, J.A.; Assuncao, W.G. The role of implant/abutment system on torque maintenance of retention screws and vertical misfit of implant-supported crowns before and after mechanical cycling. Int. J. Oral. Maxillofac. Implant. 2013, 28, 415–422. [Google Scholar] [CrossRef]
- Siamos, G.; Winkler, S.; Boberick, K.G. Relationship between implant preload and screw loosening on implant-supported prostheses. J. Oral. Implantol. 2002, 28, 67–73. [Google Scholar] [CrossRef]
- Ha, C.Y.; Lim, Y.J.; Kim, M.J.; Choi, J.H. The influence of abutment angulation on screw loosening of implants in the anterior maxilla. Int. J. Oral. Maxillofac. Implant. 2011, 26, 45–55. [Google Scholar]
- Tsuge, T.; Hagiwara, Y. Influence of lateral-oblique cyclic loading on abutment screw loosening of internal and external hexagon implants. Dent. Mater. J. 2009, 28, 373–381. [Google Scholar] [CrossRef]
- Jung, R.E.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.; Thoma, D.S. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral. Implant. Res. 2012, 23 (Suppl. 6), 2–21. [Google Scholar] [CrossRef]
- Sherif, S.; Susarla, H.K.; Kapos, T.; Munoz, D.; Chang, B.M.; Wright, R.F. A systematic review of screw- versus cement-retained implant-supported fixed restorations. J. Prosthodont. 2014, 23, 1–9. [Google Scholar] [CrossRef]
- Hotinski, E.; Dudley, J. Abutment screw loosening in angulation-correcting implants: An in vitro study. J. Prosthet. Dent. 2019, 121, 151–155. [Google Scholar] [CrossRef]
- Vinhas, A.S.; Aroso, C.; Salazar, F.; Relvas, M.; Braga, A.C.; Ríos-Carrasco, B.; Gil, J.; Rios-Santos, J.V.; Fernández-Palacín, A.; Herrero-Climent, M. In Vitro Study of Preload Loss in Different Implant Abutment Connection Designs. Materials 2022, 15, 1392. [Google Scholar] [CrossRef]
- Butignon, L.E.; Basilio Mde, A.; Pereira Rde, P.; Arioli Filho, J.N. Influence of three types of abutments on preload values before and after cyclic loading with structural analysis by scanning electron microscopy. Int. J. Oral. Maxillofac. Implant. 2013, 28, e161–e170. [Google Scholar] [CrossRef] [PubMed]
- Winkler, S.; Ring, K.; Ring, J.D.; Boberick, K.G. Implant screw mechanics and the settling effect: Overview. J. Oral. Implantol. 2003, 29, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Pérez, R.; Bartolomé, J.F.; Ferreiroa, A.; Salido, M.P.; Pradíes, G. Original vs. non-original abutments for screw-retained single implant crowns: An in vitro evaluation of internal fit, mechanical behaviour and screw loosening. Clin. Oral. Implant. Res. 2018, 29, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Piermatti, J.; Yousef, H.; Luke, A.; Mahevich, R.; Weiner, S. An in vitro analysis of implant screw torque loss with external hex and internal connection implant systems. Implant. Dent. 2006, 15, 427–435. [Google Scholar] [CrossRef]
- Hu, E.; Petrich, A.; Imamura, G.; Hamlin, C. Effect of screw channel angulation on reverse torque values of dental implant abutment screws. J. Prosthodont. 2019, 28, 969–972. [Google Scholar] [CrossRef]
- Lang, L.A.; Kang, B.; Wang, R.F.; Lang, B.R. Finite element analysis to determine preload. J. Prosthet. Dent. 2003, 90, 539–546. [Google Scholar] [CrossRef]
- Kim, S.K.; Koak, J.Y.; Heo, S.J.; Taylor, T.D.; Ryoo, S.; Lee, S.Y. Screw loosening with interchangeable abutments in internally connected implants after cyclic loading. Int. J. Oral. Maxillofac. Implant. 2012, 27, 42–47. [Google Scholar]
- Sella, G.C.; Neto, A.R.L.P.; Volpato, C.Â.M.; de Vasconcellos, D.K.; Pekkan, G.; Özcan, M. Influence of different maintenance times of torque application on the removal torque values to loosen the prosthetic abutment screws of external hexagon implants. Implant. Dent. 2013, 22, 534–539. [Google Scholar] [CrossRef]
- Stüker, R.A.; Teixeira, E.R.; Beck, J.C.P.; Costa, N.P.D. Preload and torque removal evaluation of three different abutment screws for single standing implant restorations. J. Appl. Oral. Sci. 2008, 16, 55–58. [Google Scholar] [CrossRef]
- Park, J.K.; Choi, J.U.; Jeon, Y.C.; Choi, K.S.; Jeong, C.M. Effects of abutment screw coating on implant preload. J. Prosthodont. 2010, 19, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.B.; Nicholls, J.I. Implant-abutment screw joint preload of 7 hex-top abutment systems. Int. J. Oral. Maxillofac. Implant. 2001, 16, 367–377. [Google Scholar]
- Hess, D.P. Preload from Tightening and Removal Torque. J. Fail. Anal. Preven. 2019, 19, 1055–1066. [Google Scholar] [CrossRef]
- Al-Otaibi, H.N.; Almutairi, A.; Alfarraj, J.; Algesadi, W. The Effect of Torque Application Technique on Screw Preload of Implant-Supported Prostheses. Int. J. Oral. Maxillofac. Implant. 2017, 32, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Pournasiri, I.; Farid, F.; Jafari, H.Z.; Simdar, N.; Maleki, D. Screw loosening of original and non-original abutments in implant dentistry: An in vitro study. J. Osseointegr. 2022, 14, 155–158. [Google Scholar]
- Bulaqi, H.A.; Mashhadi, M.M.; Safari, H.; Samandari, M.M.; Geramipanah, F. Dynamic nature of abutment screw retightening: Finite element study of the effect of retightening on the settling effect. J. Prosthet. Dent. 2015, 113, 412–419. [Google Scholar] [CrossRef]
- Dixon, D.L.; Breeding, L.C.; Sadler, J.P.; McKay, M.L. Comparison of screw loosening, rotation, and deflection among three implant designs. J. Prosthet. Dent. 1995, 74, 270–278. [Google Scholar] [CrossRef]
- Bakaeen, L.G.; Winkler, S.; Neff, P.A. The effect of implant diameter, restoration design, and occlusal table variations on screw loosening of posterior single-tooth implant restorations. J. Oral. Implantol. 2001, 27, 63–72. [Google Scholar] [CrossRef]
- Opler, R.; Wadhwani, C.; Chung, K.H. The effect of screwdriver angle variation on the off-axis implant abutment system and hexalobular screw. J. Prosthet. Dent. 2020, 123, 524–528. [Google Scholar] [CrossRef]
- Cavallaro, J.; Greenstein, G. Angled implant abutments: A practical application of available knowledge. J. Am. Dent. Assoc. 2011, 142, 150–158. [Google Scholar] [CrossRef]
- Hsu, M.L.; Chen, F.C.; Kao, H.C.; Cheng, C.K. Influence of off-axis loading of an anterior maxillary implant: A 3-dimensional finite element analysis. Int. J. Oral. Maxillofac. Implant. 2007, 22, 301–309. [Google Scholar] [CrossRef]
- Hein, D.; Joly, J.C.; Napimoga, M.H.; Peruzzo, D.C.; Martinez, E.F. Influence of abutment angulation on loss of prosthetic abutment torque under mechanical cycling. J. Prosthet Dent. 2021, 125, 349.e1–349.e6. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Mean sRTV | Mean sRTV Percentage Difference | Median sRTV Percentage Difference |
|---|---|---|---|
| sASC-0 | 29.1 ± 0.43 | −17.6 ± 2.6 | −16.9 |
| sASC-15 | 26.4 ± 0.91 | −24.5 ± 2.6 | −25.6 |
| sASC-25 | 24.5 ± 0.23 | −29.9 ± 0.6 | −29.7 |
| Group | Mean bRTV | Mean RTV Difference after Cyclic Loading | Median RTV Difference after Cyclic Loading |
|---|---|---|---|
| ASC-0 | 28.84 ± 0.91 | −2.41 ± 1.68 | −2.95 |
| ASC-15 | 28.87 ± 1.43 | −2.70 ± 1.44 | −2.13 |
| ASC-25 | 27.14 ± 0.80 | −1.38 ± 1.40 | −1.78 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-H.; Wu, Y.-L.; Chen, H.-S.; Lin, C.-P.; Wu, A.Y.-J. Reverse Torque Value of Angulated Screw Channel Abutment before and after Cyclic Loading: An In Vitro Study. J. Funct. Biomater. 2023, 14, 124. https://doi.org/10.3390/jfb14030124
Chen Y-H, Wu Y-L, Chen H-S, Lin C-P, Wu AY-J. Reverse Torque Value of Angulated Screw Channel Abutment before and after Cyclic Loading: An In Vitro Study. Journal of Functional Biomaterials. 2023; 14(3):124. https://doi.org/10.3390/jfb14030124
Chicago/Turabian StyleChen, Yu-Hsuan, Yu-Ling Wu, Hung-Shyong Chen, Ching-Ping Lin, and Aaron Yu-Jen Wu. 2023. "Reverse Torque Value of Angulated Screw Channel Abutment before and after Cyclic Loading: An In Vitro Study" Journal of Functional Biomaterials 14, no. 3: 124. https://doi.org/10.3390/jfb14030124