
Long-Term Stability of Hydrothermally Aged and/or Dynamically Loaded One-Piece Diameter Reduced Zirconia Oral Implants

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
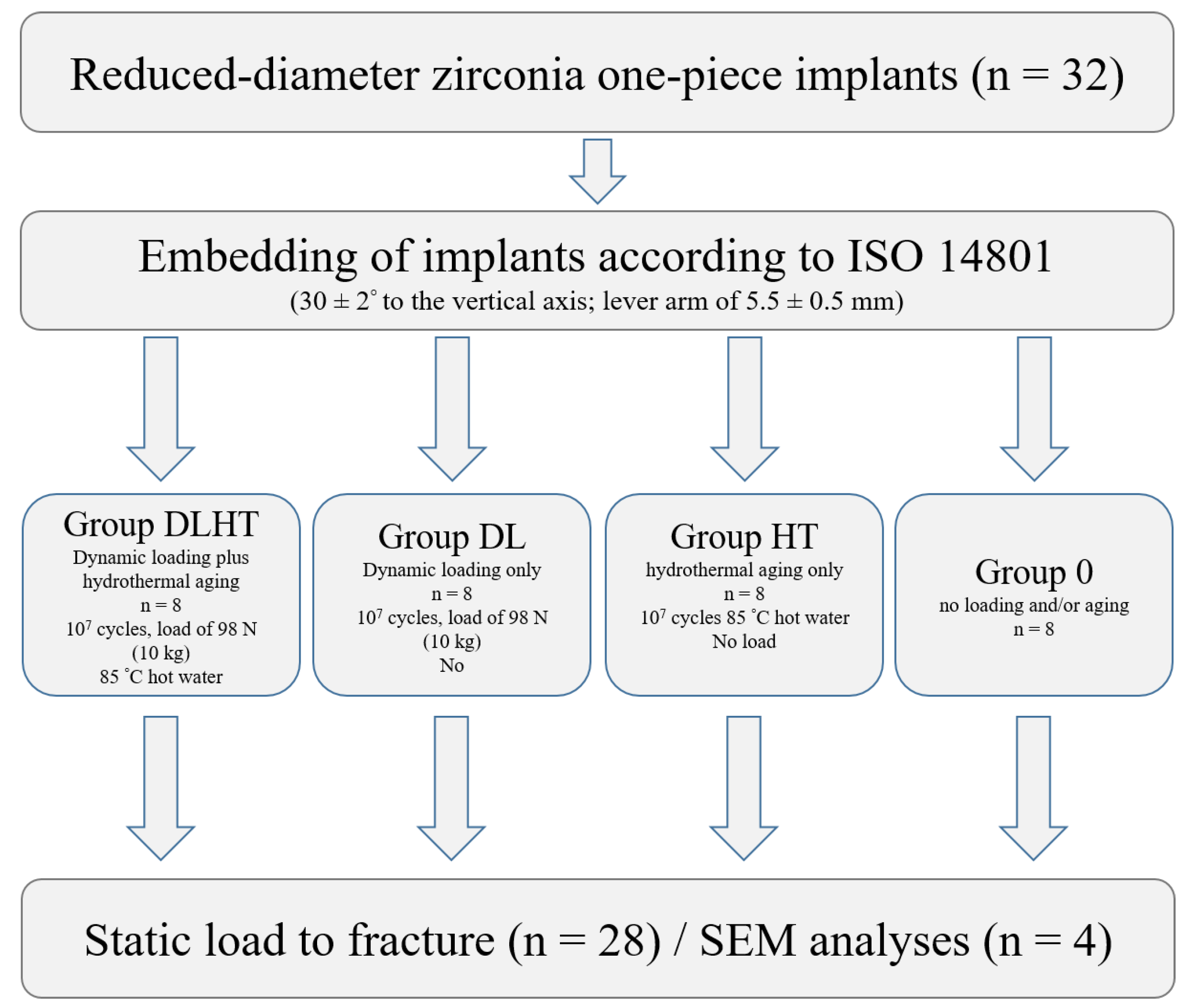
2.1. Study Implants and Experimental Setup
2.2. Preparation of the Test Specimens
2.3. Hydrothermal Aging and/or Dynamic Loading
2.4. Surface Microstructural Characterization
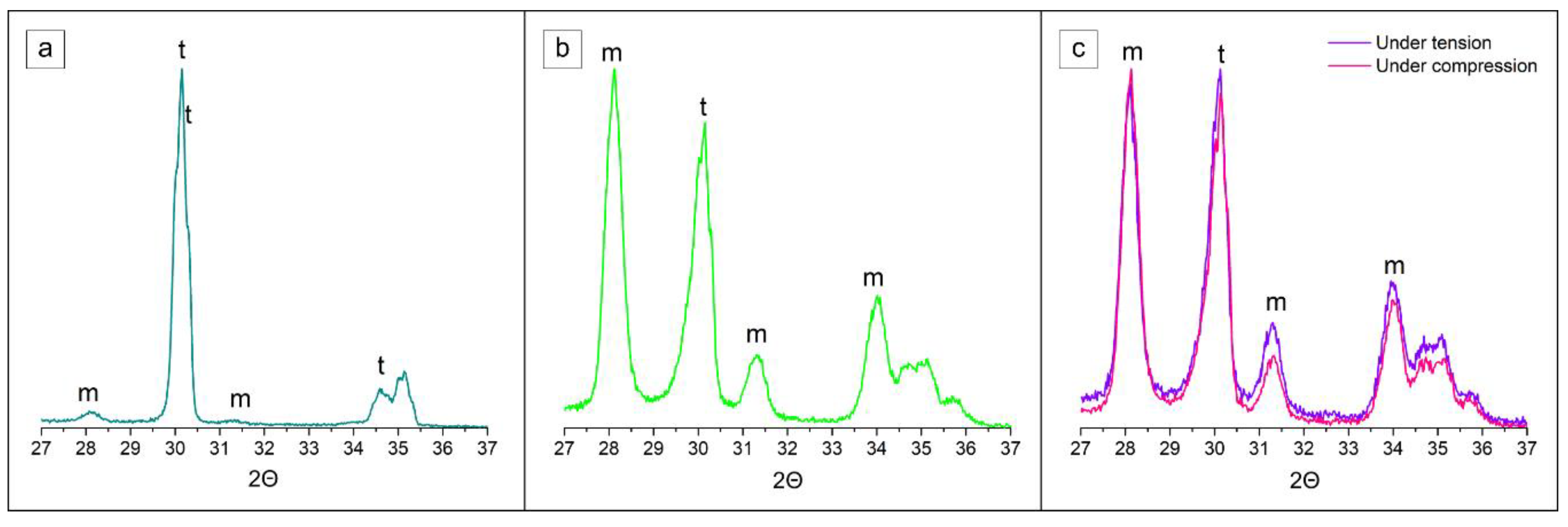
2.5. Subsurface Phase and Microstructural Composition
2.6. Static Loading Test in a Universal Testing Machine
2.7. Statistical Analysis
3. Results
3.1. Results of the Dynamic Loading Test
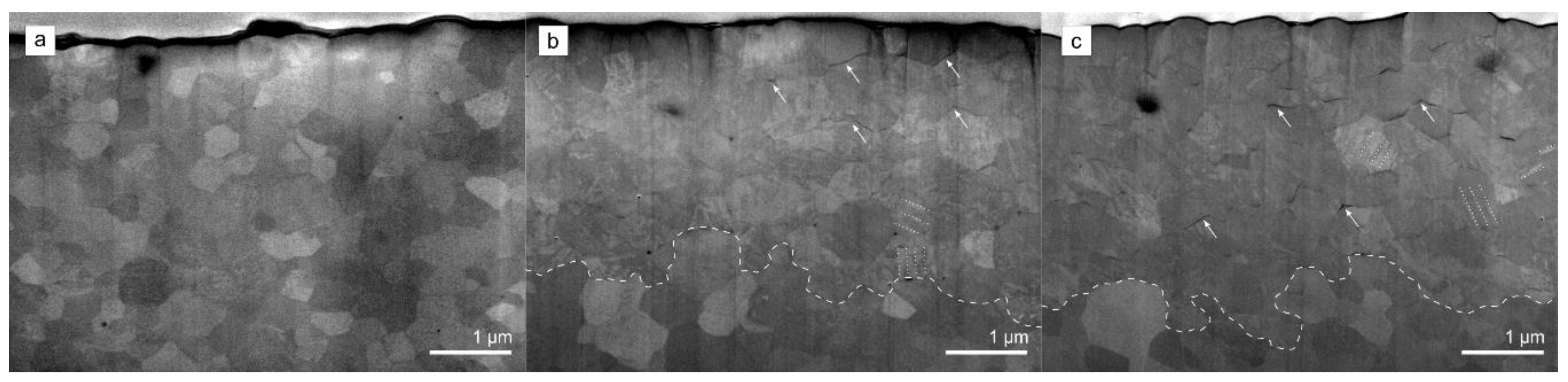
3.2. Scanning Electron Microscopy Analysis
3.3. Subsurface Phase and Microstructural Composition
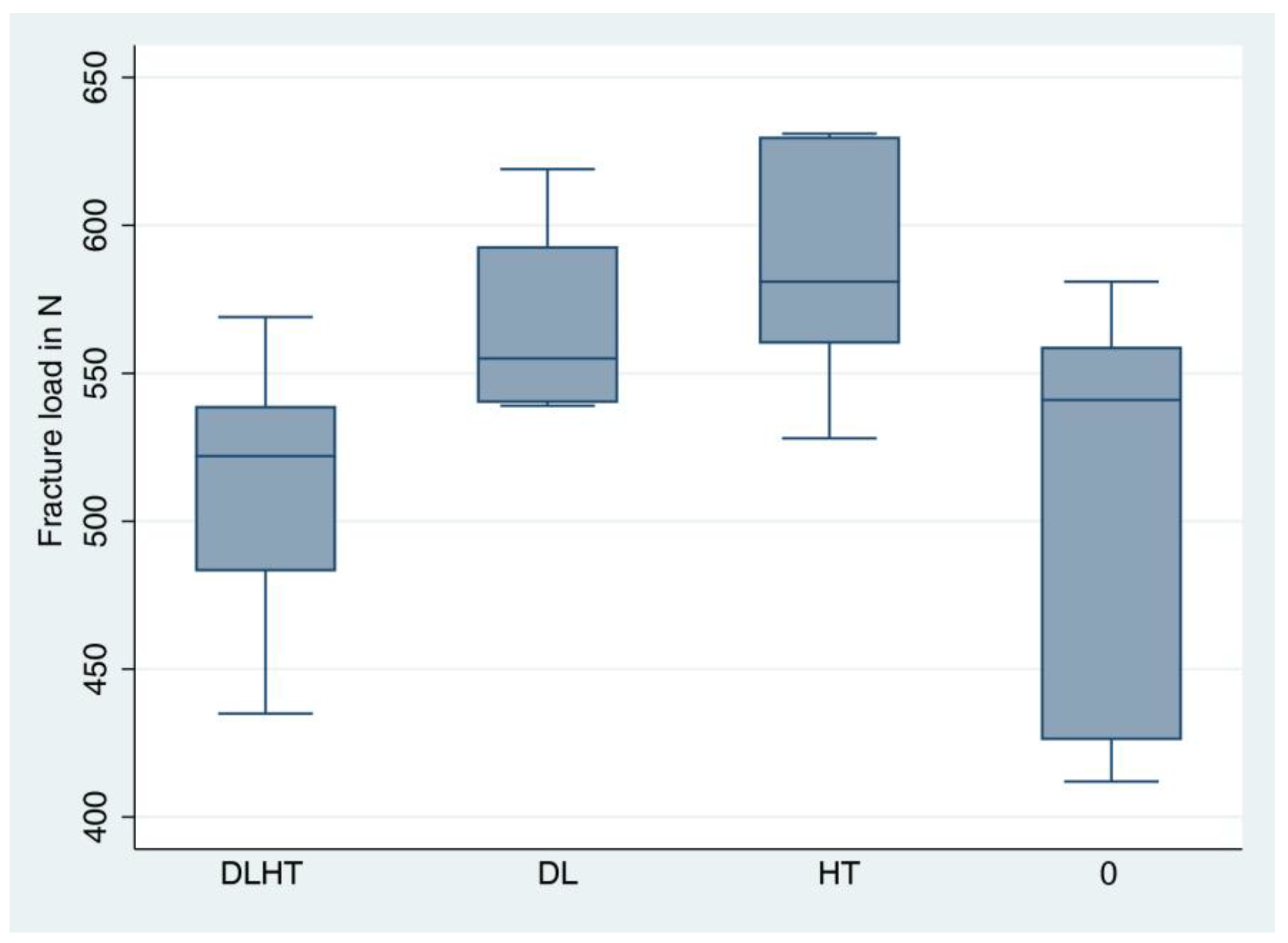
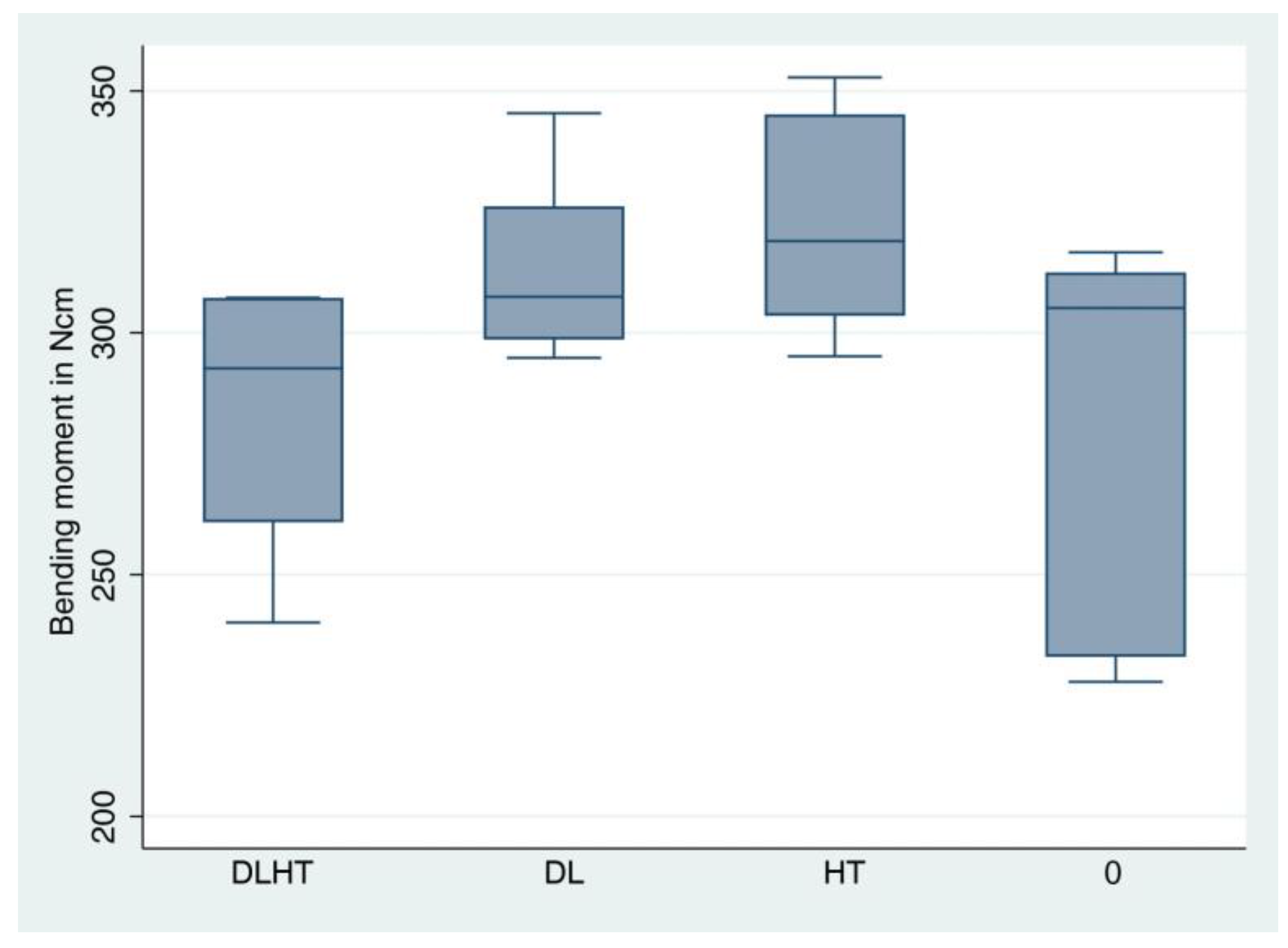
3.4. Static Loading Test until Fracture
3.5. Fracture Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ISO | International Organization for Standardization |
| DLHT | implants dynamically loaded and hydrothermally aged |
| DL | implants only dynamically loaded |
| HT | implants only hydrothermally aged |
| 3Y-TZP | 3 mol%-yttria stabilized tetragonal zirconia polycrystal |
| LTD | low temperature degradation |
| RDI | reduced diameter implants |
| FE-SEM | field-emission scanning electron microscopy |
| GI-XRD | grazing-incidence X-ray diffraction |
| FIB-SEM | focused Ion Beam Scanning Electron Microscopy |
References
- Goto, T. Osseointegration and dental implants. Clin. Calcium 2014, 24, 265–271. [Google Scholar]
- Adell, R.; Lekholm, U.; Rockler, B.; Brånemark, P.-I. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Brånemark, P.-I.; Hansson, H.-A.; Lindström, J. Osseointegrated Titanium Implants: Requirements for Ensuring a Long-Lasting, Direct Bone-to-Implant Anchorage in Man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef]
- Brånemark, P.-I. Osseointegration and its experimental background. J. Prosthet. Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Chappuis, V.; Belser, U.C.; Chen, S. Implant placement post extraction in esthetic single tooth sites: When immediate, when early, when late? Periodontol. 2000 2017, 73, 84–102. [Google Scholar] [CrossRef]
- Thoma, D.; Ioannidis, A.; Cathomen, E.; Hämmerle, C.H.F.; Hüsler, J.; Jung, R.E. Discoloration of the Peri-implant Mucosa Caused by Zirconia and Titanium Implants. Int. J. Periodontics Restor. Dent. 2016, 36, 39–45. [Google Scholar] [CrossRef]
- Mombelli, A.; Hashim, D.; Cionca, N. What is the impact of titanium particles and biocorrosion on implant survival and complications? A critical review. Clin. Oral Implant. Res. 2018, 29 (Suppl. 18), 37–53. [Google Scholar] [CrossRef] [PubMed]
- Andreiotelli, M.; Kohal, R.-J. Fracture Strength of Zirconia Implants after Artificial Aging. Clin. Implant. Dent. Relat. Res. 2009, 11, 158–166. [Google Scholar] [CrossRef]
- Cales, B. Zirconia as a sliding material: Histologic, laboratory, and clinical data. Clin. Orthop. Relat. Res. 2000, 379, 94–112. [Google Scholar] [CrossRef]
- Piconi, C.; Maccauro, G. Zirconia as a ceramic biomaterial. Biomaterials 1999, 20, 1–25. [Google Scholar] [CrossRef]
- Oliva, J.D.; Oliva, X.; Oliva, J.D. Five-year success rate of 831 consecutively placed Zirconia dental implants in humans: A comparison of three different rough surfaces. Int. J. Oral Maxillofac. Implant. 2010, 25, 336–344. [Google Scholar]
- Borgonovo, A.E.; Censi, R.; Vavassori, V.; Dolci, M.; Calvo-Guirado, J.L.; Ruiz, R.A.D.; Maiorana, C. Evaluation of the Success Criteria for Zirconia Dental Implants: A Four-Year Clinical and Radiological Study. Int. J. Dent. 2013, 2013, 463073. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.; Finke, H.C.; Klaus, G. Stability of Prototype Two-Piece Zirconia and Titanium Implants after Artificial Aging: An In Vitro Pilot Study. Clin. Implant. Dent. Relat. Res. 2009, 11, 323–329. [Google Scholar] [CrossRef]
- Dental Implants Market Size, Share & COVID-19 Impact Analysis, By Material (Titanium, Zirconium, and Others), By Design (Tapered Implants and Parallel Implants), By Type (Endosteal Implants, Subperiosteal Implants, and Transosteal Implants), By End-user (Hospitals, Dental Clinics, and Academic and Research Institutes) and Regional Forecast, 2022-2029; Fortune Business Insights. 2022. Available online: https://www.fortunebusinessinsights.com/industry-reports/dental-implants-market-100443 (accessed on 1 January 2023).
- Sanz, M.; Noguerol, B.; Sanz-Sanchez, I.; Hammerle, C.H.F.; Schliephake, H.; Renouard, F.; Sicilia, A.; Steering Committee; Cordaro, L.; Jung, R.; et al. European Association for Osseointegration Delphi study on the trends in Implant Dentistry in Europe for the year 2030. Clin. Oral Implant. Res. 2019, 30, 476–486. [Google Scholar] [CrossRef]
- Roehling, S.; Schlegel, K.A.; Woelfler, H.; Gahlert, M. Performance and outcome of zirconia dental implants in clinical studies: A meta-analysis. Clin. Oral Implant. Res. 2018, 29, 135–153. [Google Scholar] [CrossRef]
- Jung, R.E.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.; Thoma, D.S. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 2–21. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.-J.; Spies, B.C.; Vach, K.; Balmer, M.; Pieralli, S. A Prospective Clinical Cohort Investigation on Zirconia Implants: 5-Year Results. J. Clin. Med. 2020, 9, 2585. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.J.; Klaus, G. A zirconia implant-crown system: A case report. Int. J. Periodontics Restor. Dent. 2004, 24, 147–153. [Google Scholar]
- Kunrath, M.; Gupta, S.; Lorusso, F.; Scarano, A.; Noumbissi, S. Oral Tissue Interactions and Cellular Response to Zirconia Implant-Prosthetic Components: A Critical Review. Materials 2021, 14, 2825. [Google Scholar] [CrossRef]
- Okabe, E.; Ishihara, Y.; Kikuchi, T.; Izawa, A.; Kobayashi, S.; Goto, H.; Kamiya, Y.; Sasaki, K.; Ban, S.; Noguchi, T.; et al. Adhesion Properties of Human Oral Epithelial-Derived Cells to Zirconia. Clin. Implant. Dent. Relat. Res. 2016, 18, 906–916. [Google Scholar] [CrossRef]
- Hannink, R.H.J.; Kelly, P.M.; Muddle, B.C. Transformation Toughening in Zirconia-Containing Ceramics. J. Am. Ceram. Soc. 2004, 83, 461–487. [Google Scholar] [CrossRef]
- Sanon, C.; Chevalier, J.; Douillard, T.; Kohal, R.J.; Coelho, P.G.; Hjerppe, J.; Silva, N.R.F.A. Low temperature degradation and reliability of one-piece ceramic oral implants with a porous surface. Dent. Mater. 2013, 29, 389–397. [Google Scholar] [CrossRef]
- Chevalier, J.; Gremillard, L.; Deville, S. Low-Temperature Degradation of Zirconia and Implications for Biomedical Implants. Annu. Rev. Mater. Res. 2007, 37, 1–32. [Google Scholar] [CrossRef]
- Chevalier, J.; Loh, J.; Gremillard, L.; Meille, S.; Adolfson, E. Low-temperature degradation in zirconia with a porous surface. Acta Biomater. 2011, 7, 2986–2993. [Google Scholar] [CrossRef]
- Camposilvan, E.; Leone, R.; Gremillard, L.; Sorrentino, R.; Zarone, F.; Ferrari, M.; Chevalier, J. Aging resistance, mechanical properties and translucency of different yttria-stabilized zirconia ceramics for monolithic dental crown applications. Dent. Mater. 2018, 34, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Cotič, J.; Jevnikar, P.; Kocjan, A. Ageing kinetics and strength of airborne-particle abraded 3Y-TZP ceramics. Dent. Mater. 2017, 33, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Monzavi, M.; Zhang, F.; Meille, S.; Douillard, T.; Adrien, J.; Noumbissi, S.; Nowzari, H.; Chevalier, J. Influence of artificial aging on mechanical properties of commercially and non-commercially available zirconia dental implants. J. Mech. Behav. Biomed. Mater. 2020, 101, 103423. [Google Scholar] [CrossRef]
- Burkhardt, F.; Spies, B.C.; Riemer, L.; Adolfsson, E.; Doerken, S.; Kohal, R. Fracture resistance and crystal phase transformation of a one- and a two-piece zirconia implant with and without simultaneous loading and aging—An in vitro study. Clin. Oral Implant. Res. 2021, 32, 1288–1298. [Google Scholar] [CrossRef] [PubMed]
- Schiegnitz, E.; Al-Nawas, B. Narrow-diameter implants: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 21–40. [Google Scholar] [CrossRef]
- Parize, H.; Bohner, L.O.L.; Gama, L.T.; Porporatti, A.L.; Mezzomo, L.A.M.; Martin, W.C.; Gonçalves, T.M.S.V. Narrow-Diameter Implants in the Anterior Region: A Meta-analysis. Int. J. Oral Maxillofac. Implant. 2019, 34, 1347–1358. [Google Scholar] [CrossRef]
- King, P.; Maiorana, C.; Luthardt, R.G.; Sondell, K.; Øland, J.; Galindo-Moreno, P.; Nilsson, P. Clinical and Radiographic Evaluation of a Small-Diameter Dental Implant Used for the Restoration of Patients with Permanent Tooth Agenesis (Hypodontia) in the Maxillary Lateral Incisor and Mandibular Incisor Regions: A 36-Month Follow-Up. Int. J. Prosthodont. 2016, 29, 147–153. [Google Scholar] [CrossRef]
- Sohrabi, K.; Mushantat, A.; Esfandiari, S.; Feine, J. How successful are small-diameter implants? A literature review. Clin. Oral Implants Res. 2012, 23, 515–525. [Google Scholar] [CrossRef]
- Pieri, F.; Siroli, L.; Forlivesi, C.; Corinaldesi, G. Clinical, Esthetic, and Radiographic Evaluation of Small-Diameter (3.0-mm) Implants Supporting Single Crowns in the Anterior Region: A 3-Year Prospective Study. Int. J. Periodontics Restor. Dent. 2014, 34, 825–832. [Google Scholar] [CrossRef]
- De Souza, A.B.; Sukekava, F.; Tolentino, L.; Neto, J.B.C.; Garcez-Filho, J.; Araújo, M.G. Narrow- and regular-diameter implants in the posterior region of the jaws to support single crowns: A 3-year split-mouth randomized clinical trial. Clin. Oral Implant. Res. 2018, 29, 100–107. [Google Scholar] [CrossRef]
- Kohal, R.-J.; Spies, B.C.; Bauer, A.; Butz, F. One-piece zirconia oral implants for single-tooth replacement: Three-year results from a long-term prospective cohort study. J. Clin. Periodontol. 2018, 45, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Grassi, F.R.; Capogreco, M.; Consonni, D.; Bilardi, G.; Buti, J.; Kalemaj, Z. Immediate occlusal loading of one-piece zirconia implants: Five-year radiographic and clinical evaluation. Int. J. Oral Maxillofac. Implant. 2015, 30, 671–680. [Google Scholar] [CrossRef]
- Spies, B.C.; Nold, J.; Vach, K.; Kohal, R.-J. Two-piece zirconia oral implants withstand masticatory loads: An investigation in the artificial mouth. J. Mech. Behav. Biomed. Mater. 2016, 53, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Saini, B.S.; Kaur, R. X-Ray Diffraction. In Handbook of Modern Coating Technologies; Elsevier: Amsterdam, The Netherlands, 2021; pp. 85–141. ISBN 978-0-444-63239-5. [Google Scholar]
- Samodurova, A.; Vengust, D.; Kocjan, A.; Kosmač, T. The sintering-temperature-related microstructure and phase assemblage of alumina-doped and alumina–silica-co-doped 3-mol%-yttria-stabilized tetragonal zirconia. Scr. Mater. 2015, 105, 50–53. [Google Scholar] [CrossRef]
- Kosmač, T.; Kocjan, A. Ageing of dental zirconia ceramics. J. Eur. Ceram. Soc. 2012, 32, 2613–2622. [Google Scholar] [CrossRef]
- Kocjan, A.; Cotič, J.; Kosmač, T.; Jevnikar, P. In vivo aging of zirconia dental ceramics—Part I: Biomedical grade 3Y-TZP. Dent. Mater. 2021, 37, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Cionca, N.; Hashim, D.; Mombelli, A. Zirconia dental implants: Where are we now, and where are we heading? Periodontology 2000 2017, 73, 241–258. [Google Scholar] [CrossRef]
- Kohorst, P.; Borchers, L.; Strempel, J.; Stiesch, M.; Hassel, T.; Bach, F.-W.; Hübsch, C. Low-temperature degradation of different zirconia ceramics for dental applications. Acta Biomater. 2012, 8, 1213–1220. [Google Scholar] [CrossRef]
- Muñoz-Tabares, J.; Jiménez-Piqué, E.; Reyes-Gasga, J.; Anglada, M. Microstructural changes in ground 3Y-TZP and their effect on mechanical properties. Acta Mater. 2011, 59, 6670–6683. [Google Scholar] [CrossRef]
- Spies, B.C.; Spies, B.C.; Maass, M.E.; Maass, M.E.; Adolfsson, E.; Adolfsson, E.; Sergo, V.; Sergo, V.; Kiemle, T.; Kiemle, T.; et al. Long-term stability of an injection-molded zirconia bone-level implant: A testing protocol considering aging kinetics and dynamic fatigue. Dent. Mater. 2017, 33, 954–965. [Google Scholar] [CrossRef] [PubMed]
- Tinschert, J.; Natt, G.; Mohrbotter, N.; Spiekermann, H.; Schulze, K.A. Lifetime of alumina- and zirconia ceramics used for crown and bridge restorations. J. Biomed. Mater. Res. B Appl. Biomater. 2006, 80, 317–321. [Google Scholar] [CrossRef]
- Bethke, A.; Pieralli, S.; Kohal, R.-J.; Burkhardt, F.; Von Stein-Lausnitz, M.; Vach, K.; Spies, B.C. Fracture Resistance of Zirconia Oral Implants In Vitro: A Systematic Review and Meta-Analysis. Materials 2020, 13, 562. [Google Scholar] [CrossRef] [PubMed]
- Kammermeier, A.; Rosentritt, M.; Behr, M.; Schneider-Feyrer, S.; Preis, V. In vitro performance of one- and two-piece zirconia implant systems for anterior application. J. Dent. 2016, 53, 94–101. [Google Scholar] [CrossRef]
- Burkhardt, F.; Harlass, M.; Adolfsson, E.; Vach, K.; Spies, B.; Kohal, R.-J. A Novel Zirconia-Based Composite Presents an Aging Resistant Material for Narrow-Diameter Ceramic Implants. Materials 2021, 14, 2151. [Google Scholar] [CrossRef]
- Morneburg, T.R.; Pröschel, P.A. In vivo forces on implants influenced by occlusal scheme and food consistency. Int. J. Prosthodont. 2003, 16, 481–486. [Google Scholar]
- Richter, E.J. In vivo horizontal bending moments on implants. Int. J. Oral Maxillofac. Implant. 1998, 13, 232–244. [Google Scholar]
- Roehling, S.; Woelfler, H.; Hicklin, S.; Kniha, H.; Gahlert, M. A Retrospective Clinical Study with Regard to Survival and Success Rates of Zirconia Implants up to and after 7 Years of Loading: Long-Term Performance of Zirconia Implants. Clin. Implant. Dent. Relat. Res. 2016, 18, 545–558. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Fracture Load [N] | Bending Moment | |
|---|---|---|---|
| DLHT (dynamic loading & hydrothermal aging) | Median | 522 | 292.7 |
| Mean | 512 | 283.5 | |
| SD | 47 | 279 | |
| Minimum | 435 | 240.1 | |
| Maximum | 569 | 307.3 | |
| DL (dynamic loading & no hydrothermal aging) | Median | 555 | 307.4 |
| Mean | 569 | 313.7 | |
| SD | 30 | 178 | |
| Minimum | 539 | 294.8 | |
| Maximum | 619 | 345.4 | |
| HT (no dynamic loading & hydrothermal aging) | Median | 581 | 319.0 |
| Mean | 588 | 324.4 | |
| SD | 39 | 222 | |
| Minimum | 528 | 295.1 | |
| Maximum | 631 | 352.8 | |
| 0 (no dynamic loading & no hdydrothermal aging) | Median | 541 | 305.1 |
| Mean | 516 | 284.5 | |
| SD | 67 | 378 | |
| Minimum | 412 | 227.8 | |
| Maximum | 581 | 316.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kohal, R.-J.; Trinkner, A.; Burkhardt, F.; Patzelt, S.B.M.; Vach, K.; Kušter, M.; Abram, A.; Kocjan, A.; Nold, J. Long-Term Stability of Hydrothermally Aged and/or Dynamically Loaded One-Piece Diameter Reduced Zirconia Oral Implants. J. Funct. Biomater. 2023, 14, 123. https://doi.org/10.3390/jfb14030123
Kohal R-J, Trinkner A, Burkhardt F, Patzelt SBM, Vach K, Kušter M, Abram A, Kocjan A, Nold J. Long-Term Stability of Hydrothermally Aged and/or Dynamically Loaded One-Piece Diameter Reduced Zirconia Oral Implants. Journal of Functional Biomaterials. 2023; 14(3):123. https://doi.org/10.3390/jfb14030123
Chicago/Turabian StyleKohal, Ralf-Joachim, Anja Trinkner, Felix Burkhardt, Sebastian Berthold Maximilian Patzelt, Kirstin Vach, Monika Kušter, Anže Abram, Andraž Kocjan, and Julian Nold. 2023. "Long-Term Stability of Hydrothermally Aged and/or Dynamically Loaded One-Piece Diameter Reduced Zirconia Oral Implants" Journal of Functional Biomaterials 14, no. 3: 123. https://doi.org/10.3390/jfb14030123