
Dentin Sealing of Calcium Silicate-Based Sealers in Root Canal Retreatment: A Confocal Laser Microscopy Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Preparation
2.2. Root Canal Instrumentation
2.3. Root Canal Filling
2.4. Root Canal Re-Treatment Instrumentation
2.5. Root Canal Re-Treatment Filling
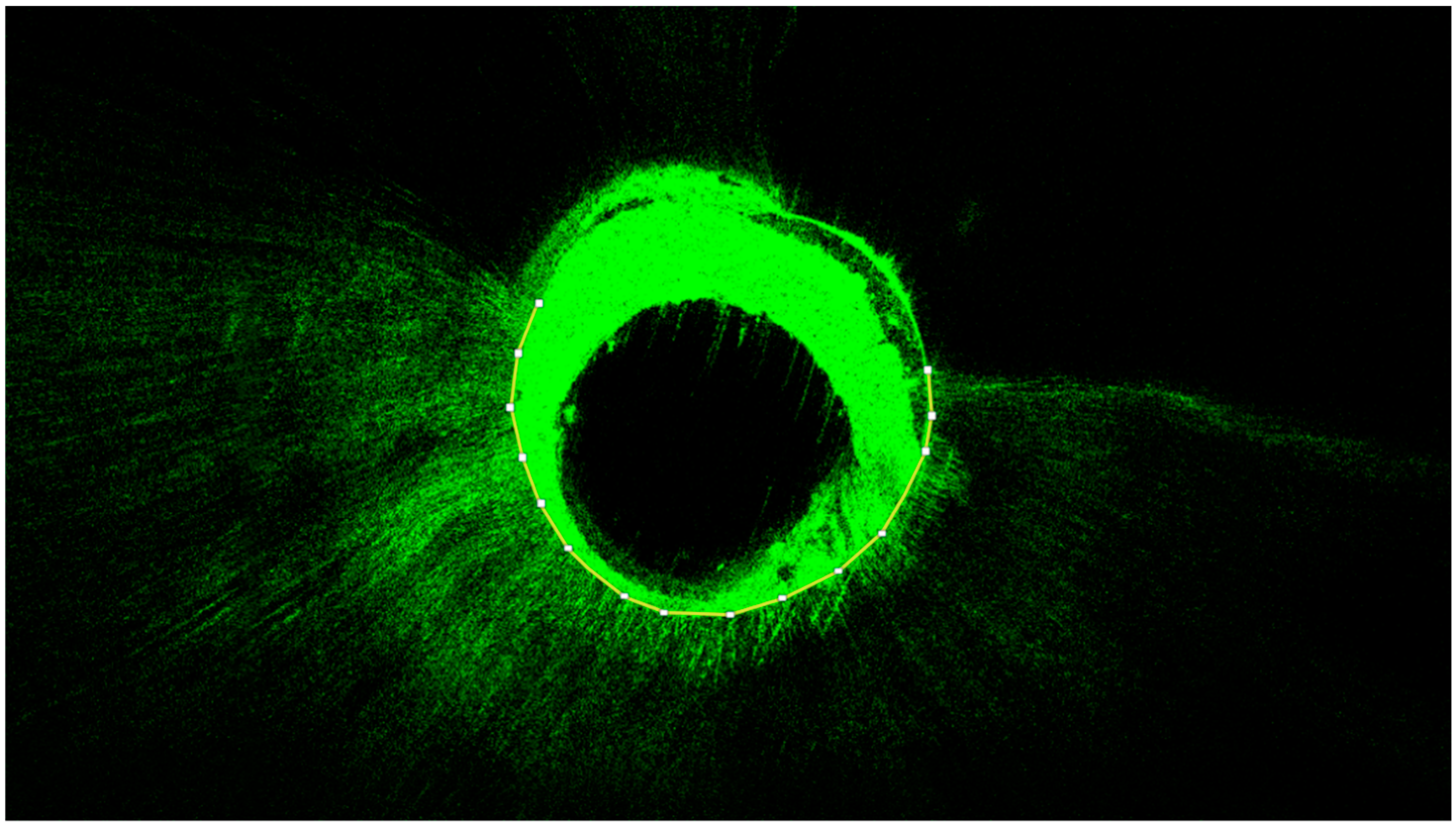
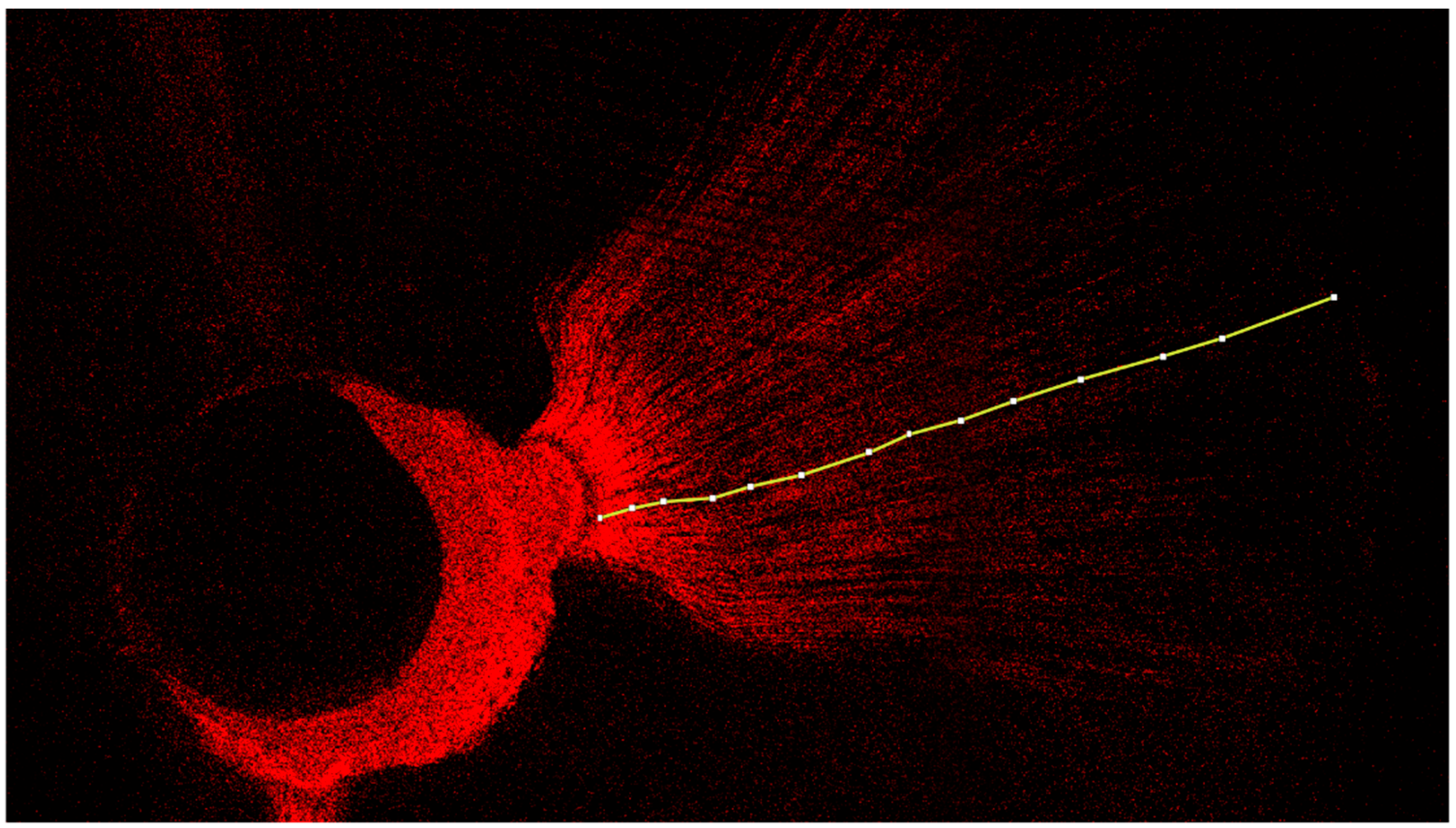
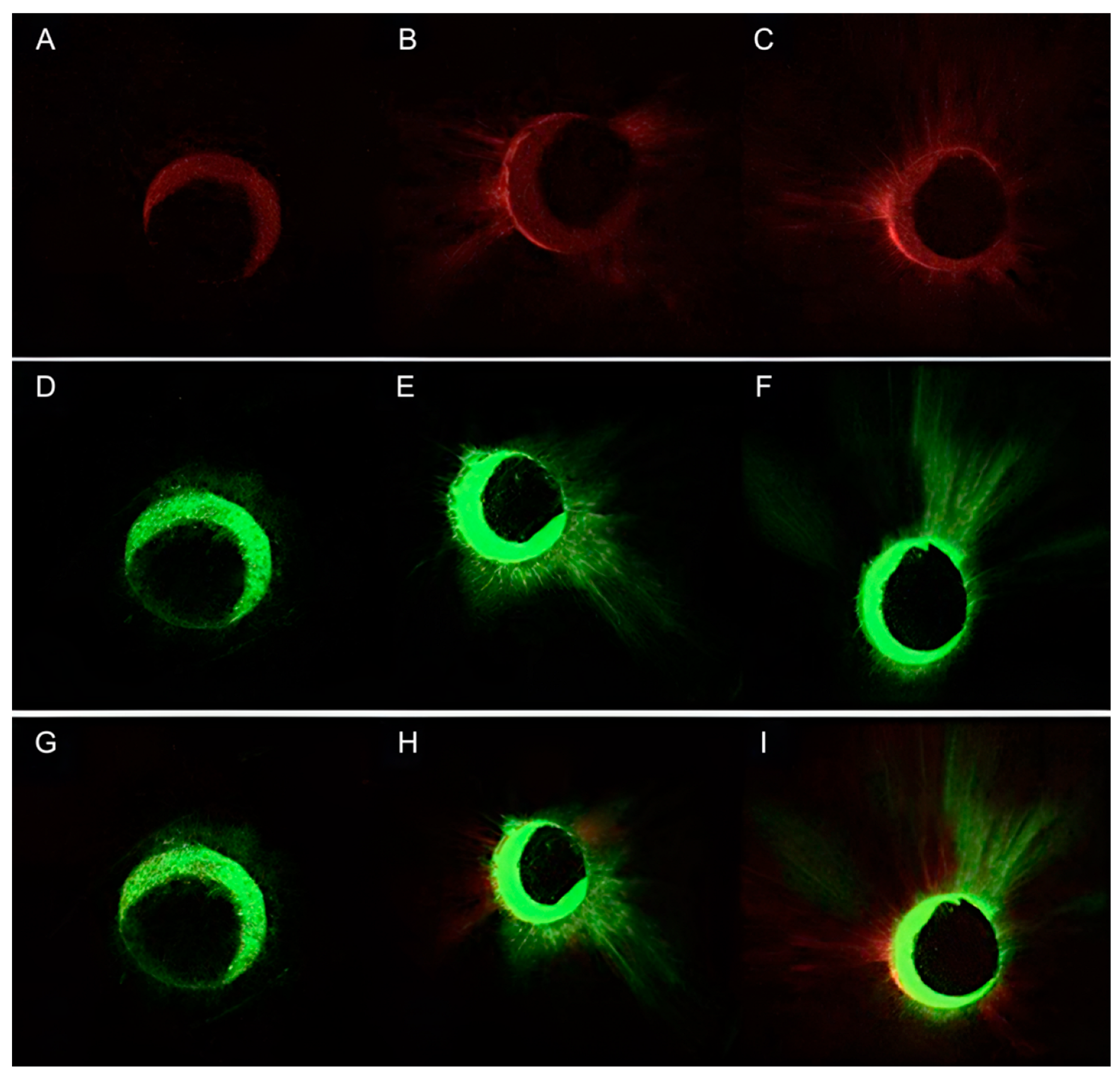
2.6. Confocal Laser Scanning Microscopy Assay (CLSM)
2.7. Statistical Analysis
3. Results
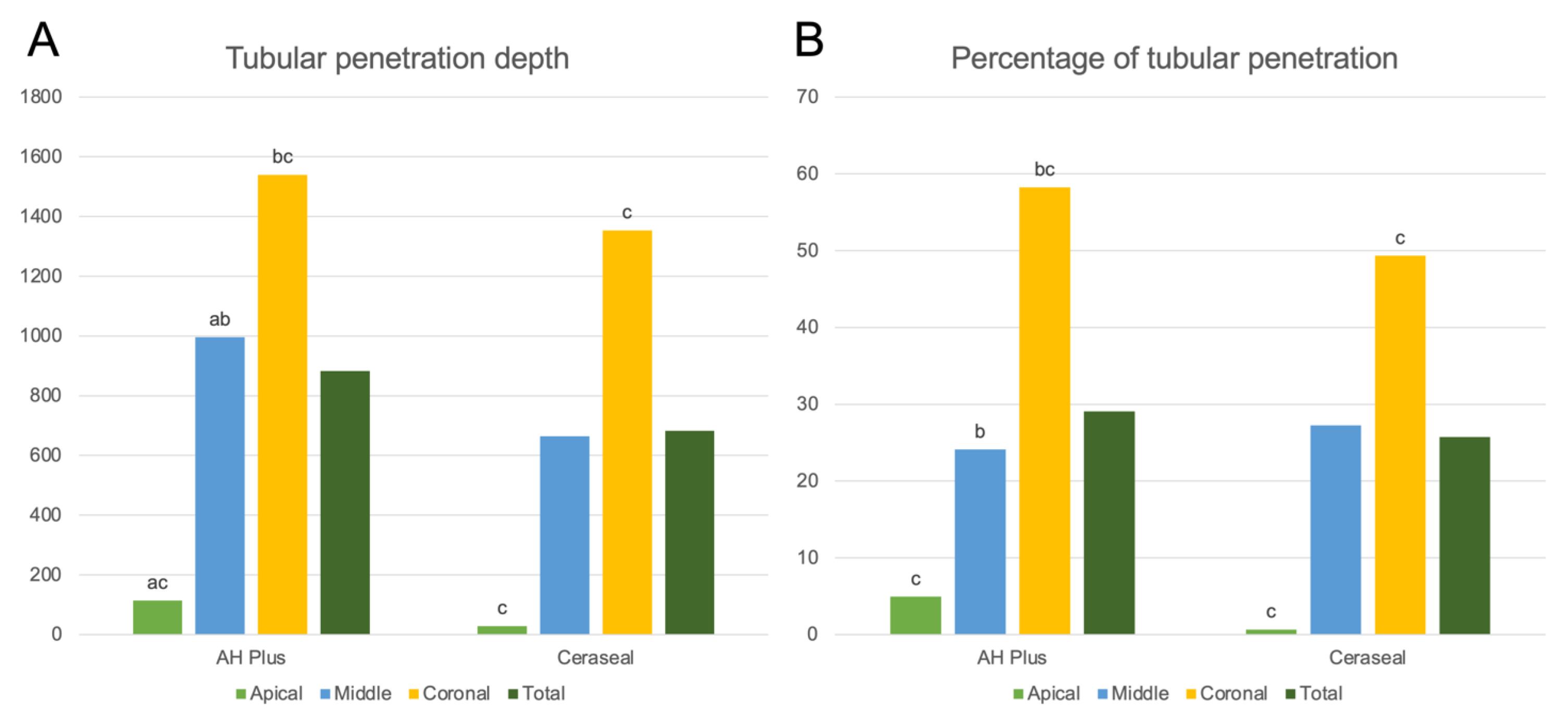
3.1. Results for CeraSeal
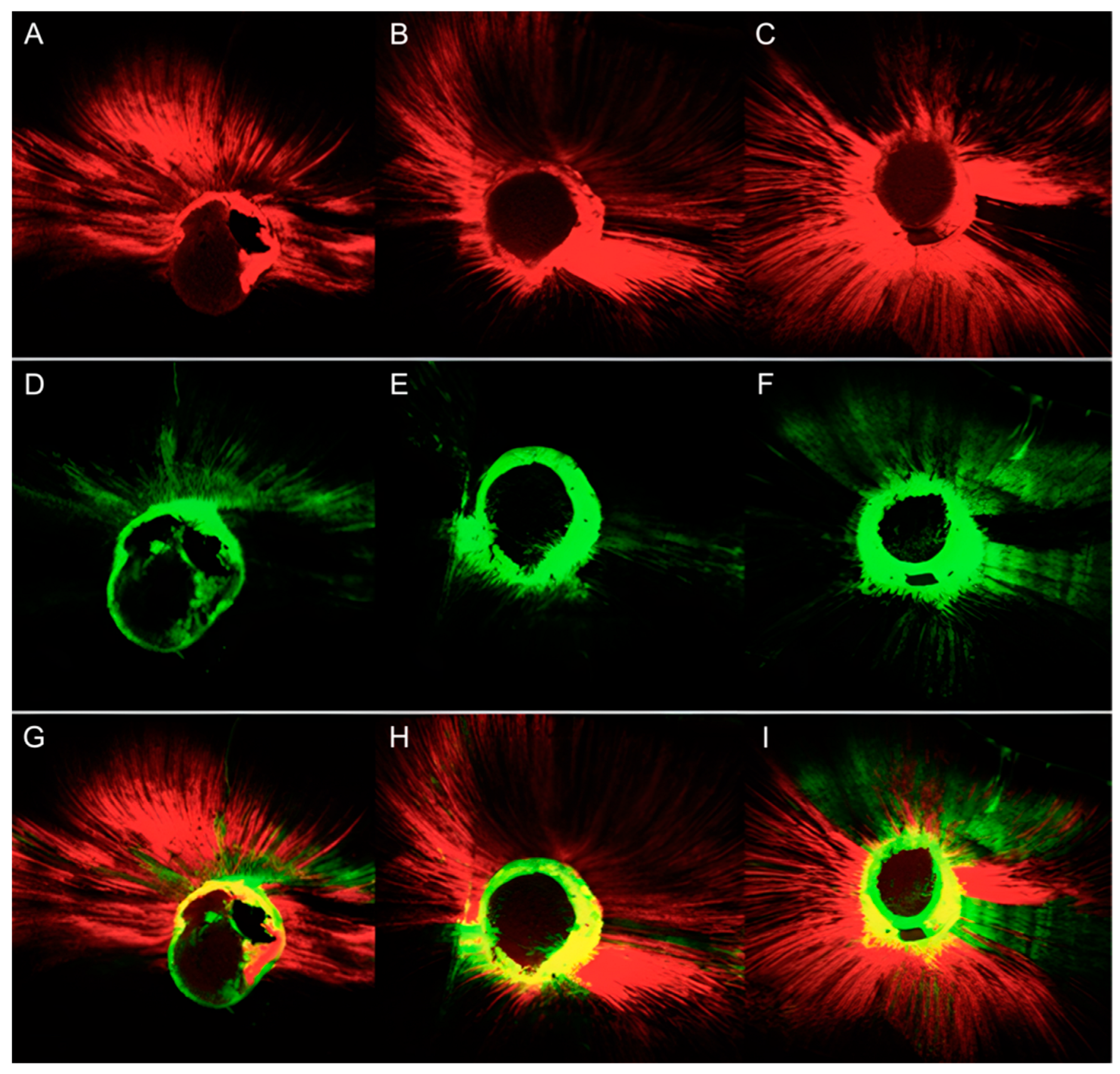
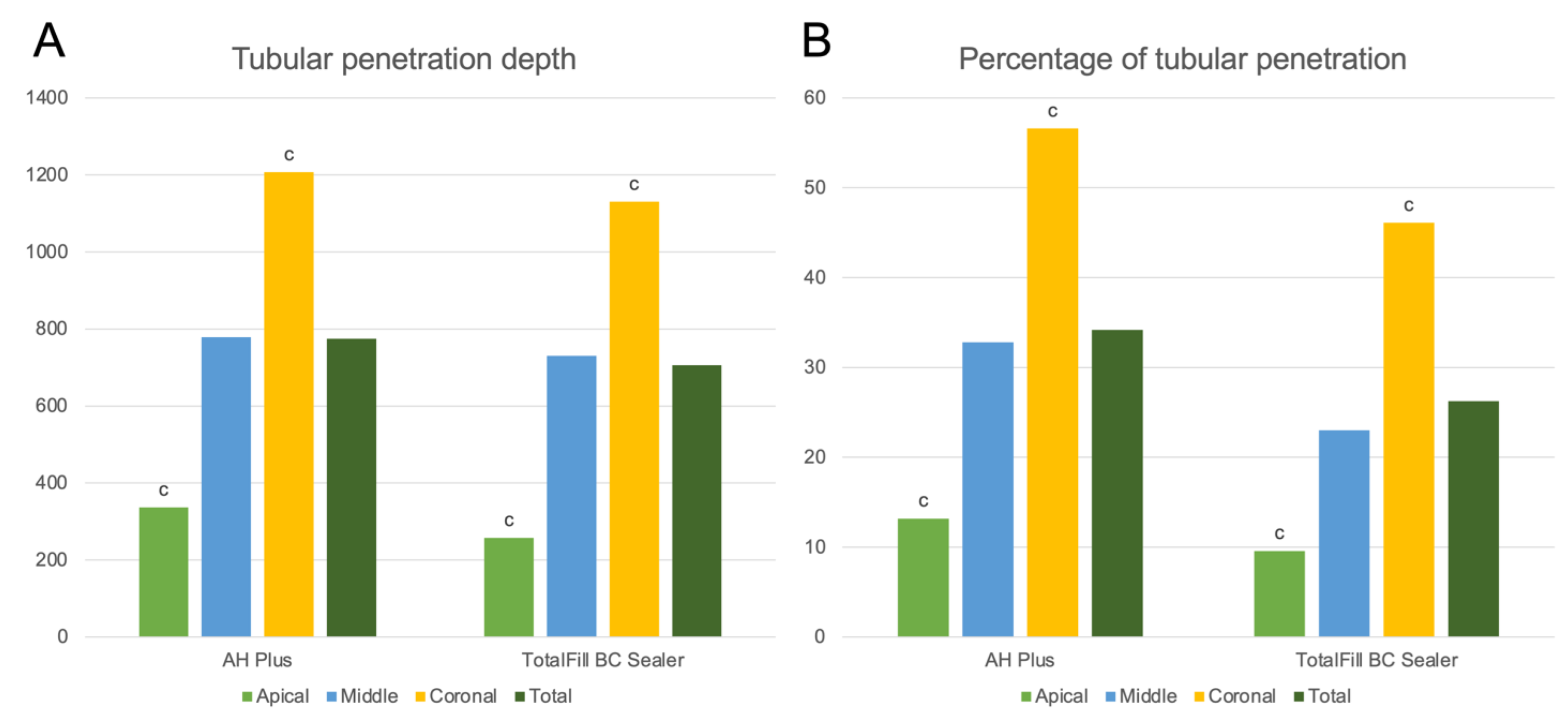
3.2. Results for TotalFill BC Sealer
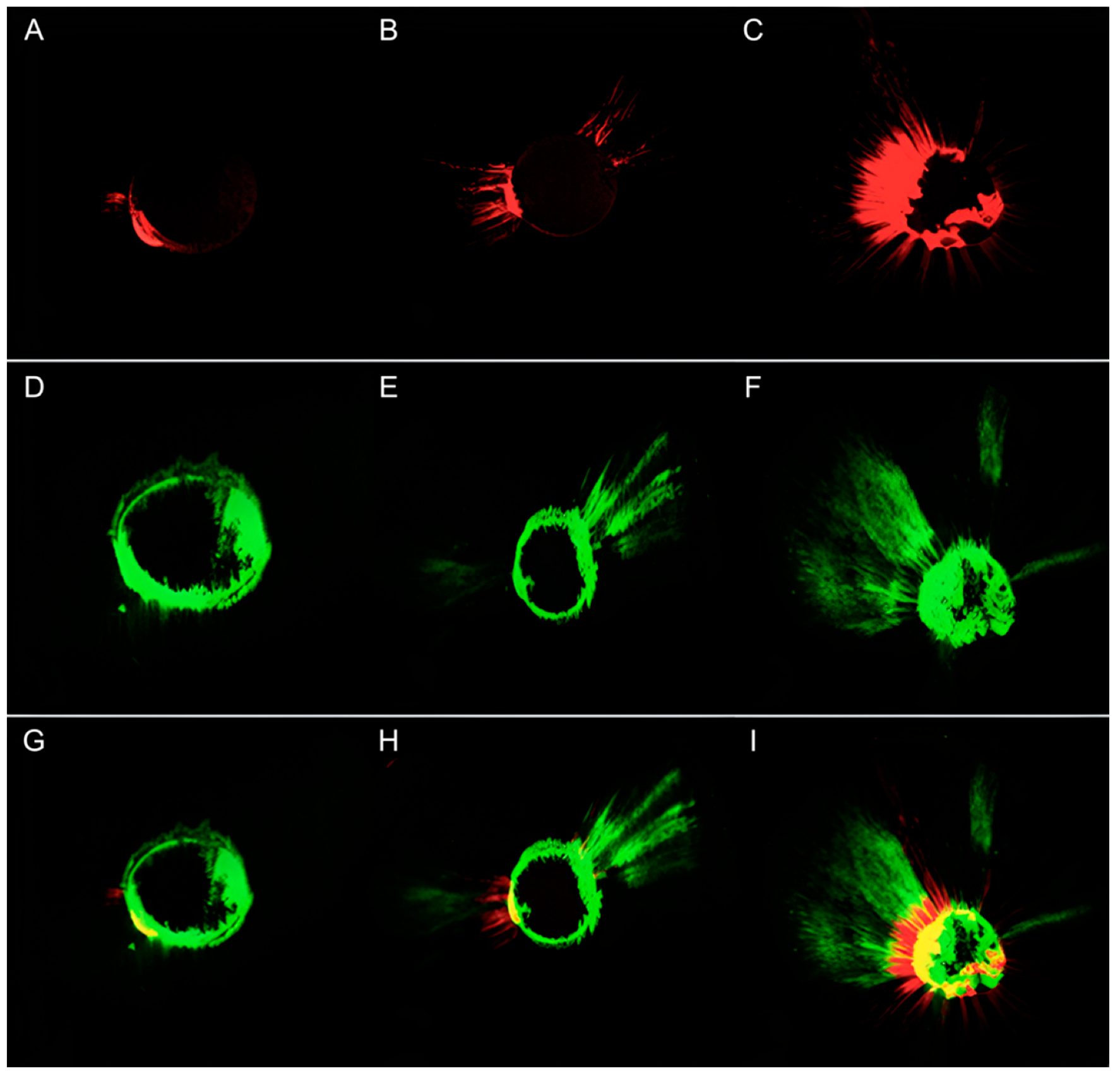
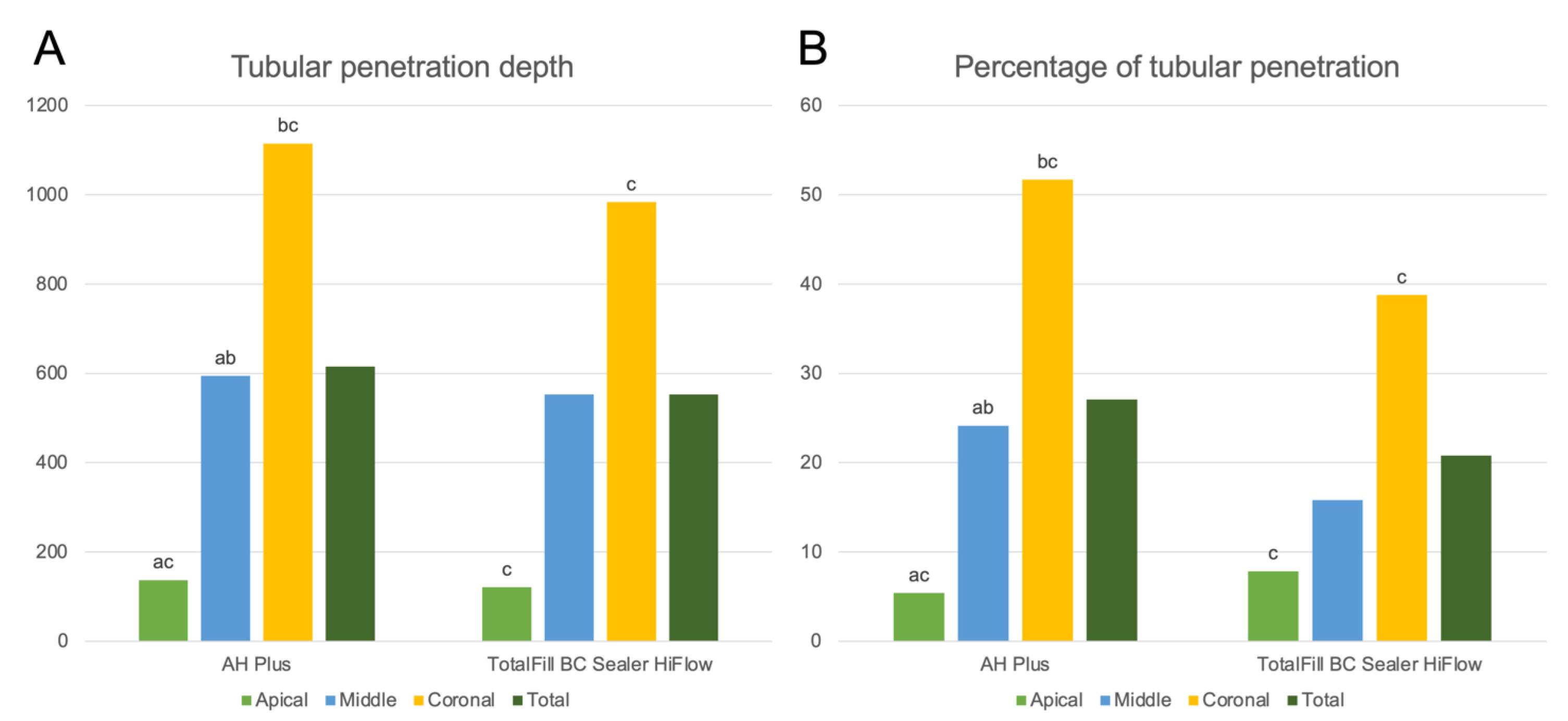
3.3. Results for TotalFill BC Sealer HiFlow
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kakoura, F.; Pantelidou, O. Retreatability of root canals filled with gutta percha and a novel bioceramic sealer: A scanning electron microscopy study. J. Conserv. Dent. 2018, 21, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Marinova-Takorova, M.; Radeva, E.; Kisyova, I.; Naseva, E. Retreatment of teeth filled with single cone technique and MTA based sealer-comparison of the effectiveness of different retreatment techniques (in vitro study). J. IMAB Annu. Proceeding Sci. Pap. 2019, 25, 2379–2383. [Google Scholar]
- Zhekov, K.; Stefanova, V. Retreatability of bioceramic endodontic sealers: A review. Folia Med. 2020, 622, 58–264. [Google Scholar] [CrossRef] [PubMed]
- Castagnola, R.; Miciacchi, I.; Marigo, L.; Cordaro, M.; Grande, N. Treatment of a root canal perforation using a calcium-silicatebased sealer: A case report with a 4 year follow-up. G. Ital. Di Endod. 2019, 33, 32–37. [Google Scholar]
- Marciano, M.A.; Guimaraes, B.M.; Ordinola-Zapata, R.; Bramante, C.M.; Cavenago, B.C.; Garcia, R.B.; Bernardineli, N.; Andrade, F.B.; Moraes, I.G.; Duarte, M.A. Physical properties and interfacial adaptation of three epoxy resin-based sealers. J. Endod. 2011, 37, 1417–1421. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, B.S.; Kim, Y.M.; Lee, D.; Kim, S.Y. The penetration ability of calcium silicate root canal sealers into dentinal tubules compared to conventional resin-based sealer: A confocal laser scanning microscopy study. Materials 2019, 12, 531. [Google Scholar] [CrossRef] [Green Version]
- Eymirly, A.; Sungur, D.D.; Uyanik, O.; Purali, N.; Nagas, E.; Cehreli, Z.C. Dentinal tubule penetration and retreatability of a calcium silicate-based sealer tested in bulk or with different main core material. J. Endod. 2019, 45, 1036–1040. [Google Scholar] [CrossRef]
- Qu, W.; Bai, W.; Liang, Y.H.; Gao, X.J. Influence of warm vertical compaction technique on physical properties of root canal sealer. J. Endod. 2016, 42, 1829–1833. [Google Scholar] [CrossRef]
- Chen, B.; Haapasalo, M.; Mobuchon, C.; Li, X.; Ma, J.; Shen, Y. Cytotoxicicty and the effect of temperature on physical properties and chemical composition of a new calcium silicate-based root canal sealer. J. Endod. 2020, 46, 531–538. [Google Scholar] [CrossRef]
- Rodríguez-Lozano, F.J.; López-García, S.; García-Bernal, D.; Tomás-Catalá, C.J.; Santos, J.M.; Llena, C.; Lozano, A.; Murcia, L.; Forner, L. Chemical composition and bioactivity potential of the new Endosequence BC Sealer formulation HiFlow. Int. Endod. J. 2020, 53, 1216–1228. [Google Scholar] [CrossRef]
- Santos, J.M.; Coelho, C.M.; Sequeira, D.B.; Marques, J.A.; Pereira, J.F.; Sousa, V.; Palma, P.J.; Santos, A.C. Subcutaneous implantation assessment of new calcium-silicate based sealer for warm obturation. Biomedicines 2021, 9, 24. [Google Scholar] [CrossRef]
- López-García, S.; Myong-Hyun, B.; Lozano, A.; García-Bernal, D.; Forner, L.; Llena, C.; Guerrero-Gironés, J.; Murcia, L.; Rodríguez-Lozano, F.J. Cytocompatibility, bioactivity potential, and ion release of three premixed calcium silicate-based sealers. Clin. Oral Investig. 2020, 24, 1749–1759. [Google Scholar] [CrossRef]
- Ordinola-Zapata, R.; Bramante, C.M.; Graeff, M.S.; del Carpio Perochena, A.; Vivan, R.R.; Camargo, E.J.; Garcia, R.B.; Bernardineli, N.; Gutmann, J.L.; de Moraes, I.G. Depth and percentage of penetration of endodontic sealers into dentinal tubules after root canal obturation using a lateral compaction technique: A confocal laser scanning microscopy study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 450–457. [Google Scholar] [CrossRef]
- Aktemur, T.S.; Uzunoglu, E.; Purali, N. Evaluation of dentinal tubule penetration depth and push-out bond strength of AH 26, BioRoot RCS, and MTA Plus root canal sealers in presence or absence of smear layer. J. Dent. Res. Dent. Clin. Dent. Prospect. 2018, 12, 294–298. [Google Scholar] [CrossRef]
- Chong, B.S.; Pitt Ford, T.R. Endodontic retreatment. 1: Indications and case selection. Dent Updat. 1996, 23, 320–328. [Google Scholar]
- Iandolo, A.; Simeone, M.; Orefice, S.; Rengo, S. 3D cleaning, a perfected technique: Thermal profile assessment of heated NaOCl. G. Ital. di Endod. 2017, 31, 58–61. [Google Scholar] [CrossRef]
- Barbosa-Ribeiro, M.; Arruda-Vasconcelos, R.; Louzada, L.M.; Dos Santos, D.G.; Andreote, F.D.; Gomes, B.P.F.A. Microbiological analysis of endodontically treated teeth with apical periodontitis before and after endodontic retreatment. Clin. Oral Investig. 2021, 25, 2017–2027. [Google Scholar] [CrossRef]
- Castro, R.F.; Melo, J.; Dias, L.; Silva, E.; Brandão, J. Evaluation of the efficacy of filling material removal and re-filling after different retreatment procedures. Braz. Oral Res. 2018, 32, e94. [Google Scholar] [CrossRef]
- Muedra, P.; Forner, L.; Lozano, A.; Sanz, J.L.; Rodriguez-Lozano, F.J.; Guerrero Gironés, J.; Riccitiello, F.; Spagnuolo, G.; Llena, C. Could the calcium silicate-based sealer presentation form influence dentinal sealing? An in vitro confocal laser study on tubular penetration. Materials 2021, 14, 659. [Google Scholar] [CrossRef]
- Eğemen, A.; Belli, S. The effect of primary root canal treatment on dentinal tubule penetration of calcium silicate-based sealers during endodontic retreatment. J. Endod. 2022. [Google Scholar] [CrossRef]
- Arikatla, S.K.; Chalasani, U.; Mandava, J.; Yelisela, R.K. Interfacial adaptation and penetration depth of bioceramic endodontic sealers. J. Conserv. Dent. 2018, 21, 373–377. [Google Scholar] [PubMed]
- Balguerie, E.; Van der Sluis, L.; Vallaeys, K.; Gurgel-Georgelin, M.; Diemer, F. Sealer penetration and adaptation in the dentinal tubules: A scanning electron microscopic study. J. Endod. 2011, 37, 1576–1579. [Google Scholar] [CrossRef] [PubMed]
- Kontogiannis, T.; Kerezoudis, N.; Kozyrakis, K.; Farmakis, E. Removal ability of MTA-, bioceramic- and resin-based sealers from obturated root canals, following XP-endo® Finisher R file: An ex vivo study. Saudi Endod. J. 2019, 9, 8–13. [Google Scholar]
- Kharouf, N.; Arntz, Y.; Eid, A.; Zghal, J.; Sauro, S.; Haikel, Y.; Mancino, D. Physicochemical and antibacterial properties of novel, premixed calcium silicate-based sealer compared to powder–liquid bioceramic sealer. J. Clin. Med. 2020, 9, 3096. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.; Romeiro, K.; Cassimiro, M.; Gominho, L.; Dantas, E.; Silva, S.; Albuquerque, D. Micro-CT analysis of dentinal microcracks on root canals filled with a bioceramic sealer and retreated with reciprocating instruments. Sci. Rep. 2020, 10, 15264. [Google Scholar] [CrossRef] [PubMed]
- Volponi, A.; Pelegrine, R.; Kato, A.; Stringueta, C.; Lopes, R.; de Sá Silva, A.; da Silveira, B.C. Micro-computed tomographic assesment of supplementary cleaning techniques for removing bioceramic sealer and gutta-percha in oval canals. J. Endod. 2020, 46, 1901–1906. [Google Scholar] [CrossRef]
- Sonntag, D.; Ritter, A.; Burkhart, A.; Fischer, J.; Mondrzyk, A.; Ritter, H. Experimental amine-epoxide sealer: A physicochemical study in comparison with AH Plus and EasySeal. Int. Endod. J. 2014, 48, 747–756. [Google Scholar] [CrossRef]
- Rajda, M.; Miletić, I.; Baršić, G.; Krmek, S.J.; Šnjarić, D.; Baraba, A. Efficacy of reciprocating instruments in the removal of bioceramic and epoxy resin-based sealers: Micro-CT analysis. Materials 2021, 14, 6670. [Google Scholar] [CrossRef]
- Chandra, S.S.; Shankar, P.; Indira, R. Depth of penetration of four resin sealers into radicular dentinal tubules: A confocal microscopic study. J. Endod. 2012, 38, 1412–1416. [Google Scholar] [CrossRef]
- DeLong, C.; He, J.; Woodmansey, K.F. The effect of obturation technique on the push-out bond strength of calcium silicate sealers. J. Endod. 2015, 41, 385–388. [Google Scholar] [CrossRef]
- Fernandez, R.; Restrepo, J.S.; Aristizabal, D.C.; Alvárez, L.G. Evaluation of the filling ability of artificial lateral canals using calcium silicate-based and epoxy resin-based endodontic sealers and two gutta-percha filling techniques. Int. Endod. J. 2015, 49, 365–373. [Google Scholar] [CrossRef]
- Abdellatif, D.; Amato, A.; Calapaj, M.; Pisano, M.; Iandolo, A. A novel modified obturation technique using biosealers: An ex vivo study. J. Conserv. Dent. 2021, 24, 369–373. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Composition |
|---|---|
| Ceraseal | 45–50% zirconium dioxide, 20–30% tricalcium silicate, 1–10% dicalcium silicate, 1–10% tricalcium aluminate |
| Totalfill BC Sealer | 35–45% Zirconium oxide, 20–35% tricalcium silicate, 7–15% dicalcium silicate, 1–4% calcium hydroxide, fillers |
| Totalfill BC Sealer HiFlow | 35–45% Zirconium oxide, 20–35% tricalcium silicate, 7–15% dicalcium silicate, 1–4% calcium hydroxide, fillers |
| AH Plus | Epoxy paste: diepoxy, calcium tungstate, zirconium oxide, aerosol, and dye Amine paste: 1-adamantane amine, N’dibenzyl-5 oxanonandiamine-1,9, TCD-diamine, calcium tungstate, zirconium oxide, aerosol, and silicone oil |
| Tubular Penetration Depth (μm) | Percentage of Penetrated Perimeter (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n = 10 | Apical | Middle | Coronal | Total | Apical | Middle | Coronal | Total | |
| AH Plus | Mean | 114.04 | 995.47 | 1539.83 | 883.11 | 4.94 | 24.11 | 58.23 | 29.09 |
| Median | 0.00 | 769.88 | 1255.66 | 706.73 | 0.00 | 15.66 | 63.15 | 14.73 | |
| IQR | 48.79 | 1386.31 | 1329.80 | 1523.15 | 1.20 | 32.04 | 71.08 | 50.25 | |
| CeraSeal | Mean | 28.94 | 663.87 | 1353.93 | 682.25 | 0.67 | 27.23 | 49.34 | 25.75 |
| Median | 0.00 | 569.08 | 1228.09 | 124.42 | 0.00 | 15.04 | 46.48 | 7.54 | |
| IQR | 0.00 | 1265.33 | 2237.41 | 1249.63 | 0.00 | 42.58 | 65.71 | 42.63 | |
| Tubular Penetration Depth (μm) | Percentage of Penetrated Perimeter (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n = 10 | Apical | Middle | Coronal | Total | Apical | Middle | Coronal | Total | |
| AH Plus | Mean | 336.74 | 778.23 | 1207.08 | 774.01 | 13.19 | 32.81 | 56.58 | 34.19 |
| Median | 153.67 | 839.67 | 1411.54 | 777.93 | 1.73 | 25.66 | 66.95 | 24.18 | |
| IQR | 604.97 | 1162.45 | 623.06 | 1383.86 | 21.58 | 41.14 | 55.55 | 64.50 | |
| TotalFill BC Sealer | Mean | 257.25 | 729.51 | 1130.60 | 705.79 | 9.59 | 23.02 | 46.11 | 26.24 |
| Median | 100.55 | 766.98 | 1218.06 | 683.17 | 9.81 | 19.71 | 49.20 | 16.41 | |
| IQR | 490.11 | 1134.02 | 915.81 | 1203.22 | 15.94 | 27.81 | 66.23 | 34.90 | |
| Tubular Penetration Depth (μm) | Percentage of Penetrated Perimeter (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n = 10 | Apical | Middle | Coronal | Total | Apical | Middle | Coronal | Total | |
| AH Plus | Mean | 137.26 | 594.11 | 1114.95 | 615.44 | 5.39 | 24.15 | 51.69 | 27.07 |
| Median | 0.00 | 622.22 | 1308.77 | 605.52 | 0.00 | 26.63 | 52.89 | 24.95 | |
| IQR | 283.69 | 679.61 | 742.33 | 1181.20 | 10.92 | 32.69 | 36.14 | 50.55 | |
| TotalFill BC Sealer HiFlow | Mean | 121.35 | 552.51 | 983.84 | 552.57 | 7.85 | 15.81 | 38.77 | 20.80 |
| Median | 0.00 | 293.62 | 1029.81 | 293.62 | 0.00 | 9.11 | 34.83 | 9.11 | |
| IQR | 104.68 | 1350.94 | 882.79 | 1202.03 | 9.50 | 29.33 | 54.77 | 40.86 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz-Blanco, B.; Sanz, J.L.; Llena, C.; Lozano, A.; Forner, L. Dentin Sealing of Calcium Silicate-Based Sealers in Root Canal Retreatment: A Confocal Laser Microscopy Study. J. Funct. Biomater. 2022, 13, 114. https://doi.org/10.3390/jfb13030114
Ortiz-Blanco B, Sanz JL, Llena C, Lozano A, Forner L. Dentin Sealing of Calcium Silicate-Based Sealers in Root Canal Retreatment: A Confocal Laser Microscopy Study. Journal of Functional Biomaterials. 2022; 13(3):114. https://doi.org/10.3390/jfb13030114
Chicago/Turabian StyleOrtiz-Blanco, Blanca, José Luis Sanz, Carmen Llena, Adrián Lozano, and Leopoldo Forner. 2022. "Dentin Sealing of Calcium Silicate-Based Sealers in Root Canal Retreatment: A Confocal Laser Microscopy Study" Journal of Functional Biomaterials 13, no. 3: 114. https://doi.org/10.3390/jfb13030114