Effect of Androgen-Deprivation Therapy on Bone Mineral Density in Patients with Prostate Cancer: A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Trial Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Study Quality Assessments and Quality of Evidence
2.5. Statistical Analysis
3. Results
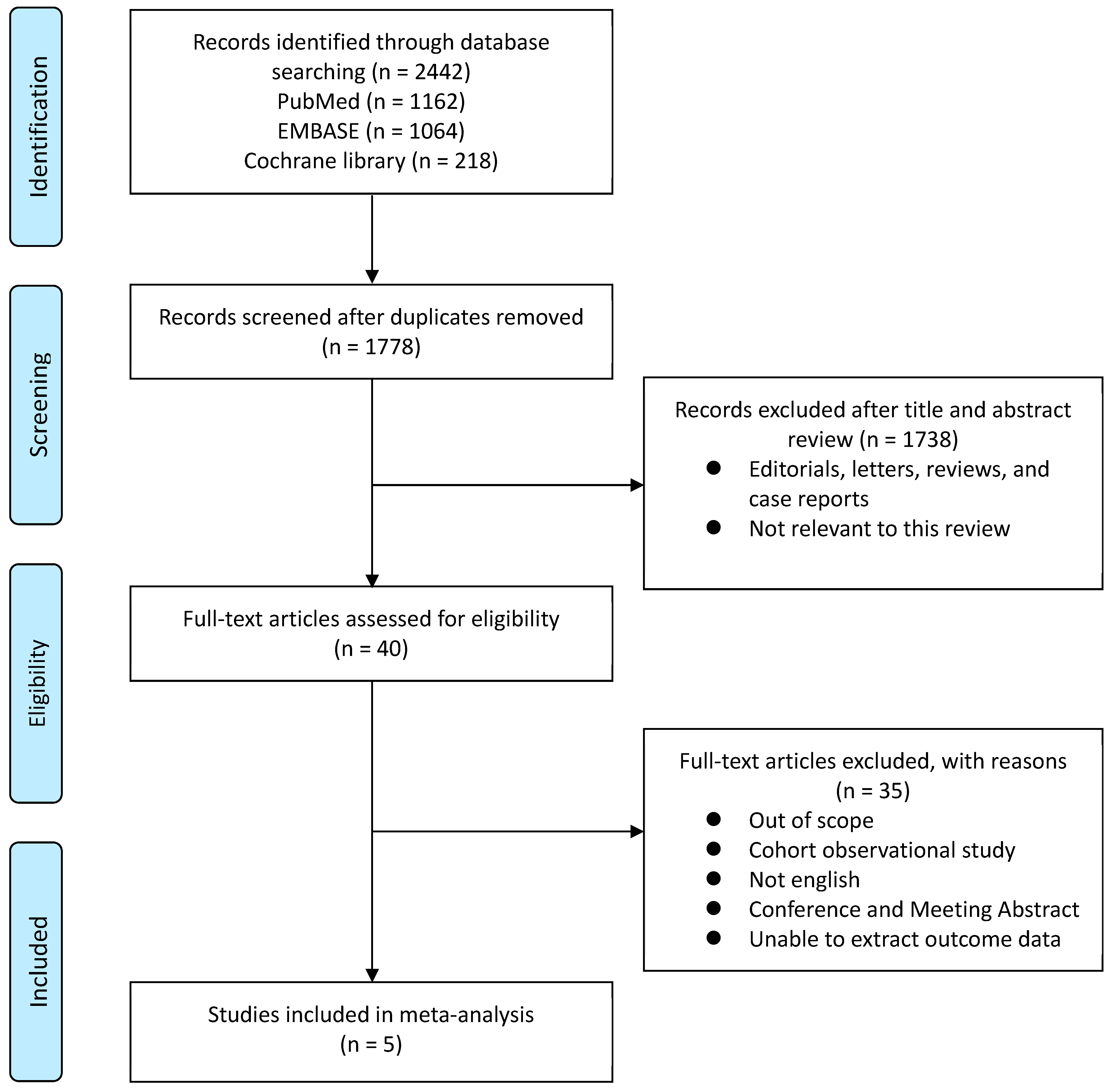
3.1. Systematic Review Process
3.2. Outcome Comparisons between ADT and Control Groups
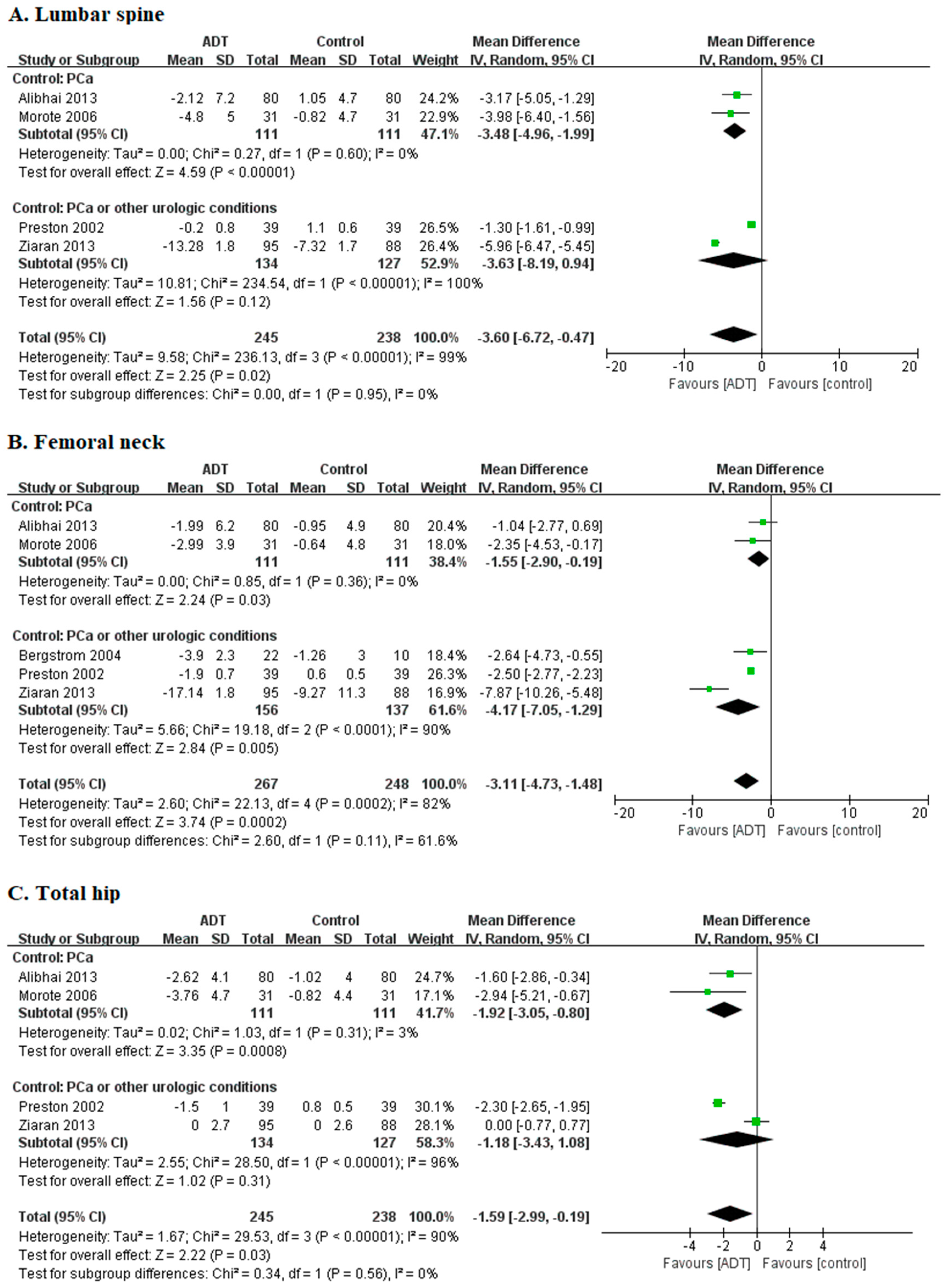
3.2.1. Lumbar Spine: Percent Change of BMD
3.2.2. Femoral Neck: Percent Change of BMD
3.2.3. Total Hip: Percent Change of BMD
3.3. Quality Assessment and Qualitative Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jemal, A.; Siegel, R.; Xu, J.; Ward, E. Cancer statistics, 2010. CA Cancer J. Clin. 2010, 60, 277–300. [Google Scholar] [CrossRef] [PubMed]
- Bienz, M.; Saad, F. Androgen-deprivation therapy and bone loss in prostate cancer patients: A clinical review. Bonekey Rep. 2015, 4, 716. [Google Scholar] [CrossRef] [PubMed]
- So, A.; Chin, J.; Fleshner, N.; Saad, F. Management of skeletal-related events in patients with advanced prostate cancer and bone metastases: Incorporating new agents into clinical practice. Can. Urol. Assoc. J. 2012, 6, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Koo, K.C.; Dasgupta, P. Treatment of oligometastatic hormone-sensitive prostate cancer: A comprehensive review. Yonsei Med. J. 2018, 59, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Mohler, J.L.; Armstrong, A.J.; Bahnson, R.R.; D’Amico, A.V.; Davis, B.J.; Eastham, J.A.; Enke, C.A.; Farrington, T.A.; Higano, C.S.; Horwitz, E.M.; et al. Prostate cancer, version 1.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 19–30. [Google Scholar] [CrossRef]
- Eastham, J.A. Bone health in men receiving androgen deprivation therapy for prostate cancer. J. Urol. 2007, 177, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Jang, W.S.; Koh, D.H.; Ham, W.S.; Rha, K.H.; Hong, S.J.; Choi, Y.D. Impact of early salvage androgen deprivation therapy in localized prostate cancer after radical prostatectomy: A propensity score matched analysis. Yonsei Med. J. 2018, 59, 580–587. [Google Scholar] [CrossRef]
- Sharifi, N.; Gulley, J.L.; Dahut, W.L. Androgen deprivation therapy for prostate cancer. JAMA 2005, 294, 238–244. [Google Scholar] [CrossRef]
- Bergstrom, I.; Gustafsson, H.; Sjoberg, K.; Arver, S. Changes in bone mineral density differ between gonadotrophin-releasing hormone analogue- and surgically castrated men with prostate cancer—A prospective, controlled, parallel-group study. Scand. J. Urol. Nephrol. 2004, 38, 148–152. [Google Scholar] [CrossRef]
- Berruti, A.; Dogliotti, L.; Terrone, C.; Cerutti, S.; Isaia, G.; Tarabuzzi, R.; Reimondo, G.; Mari, M.; Ardissone, P.; De Luca, S.; et al. Changes in bone mineral density, lean body mass and fat content as measured by dual energy x-ray absorptiometry in patients with prostate cancer without apparent bone metastases given androgen deprivation therapy. J. Urol. 2002, 167, 2361–2367. [Google Scholar] [CrossRef]
- Daniell, H.W.; Dunn, S.R.; Ferguson, D.W.; Lomas, G.; Niazi, Z.; Stratte, P.T. Progressive osteoporosis during androgen deprivation therapy for prostate cancer. J. Urol. 2000, 163, 181–186. [Google Scholar] [CrossRef]
- Smith, M.R.; McGovern, F.J.; Zietman, A.L.; Fallon, M.A.; Hayden, D.L.; Schoenfeld, D.A.; Kantoff, P.W.; Finkelstein, J.S. Pamidronate to prevent bone loss during androgen-deprivation therapy for prostate cancer. N. Engl. J. Med. 2001, 345, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.A.; Weston, R.; Stephenson, R.N.; George, E.; Parr, N.J. Immediate dual energy x-ray absorptiometry reveals a high incidence of osteoporosis in patients with advanced prostate cancer before hormonal manipulation. BJU Int. 2003, 92, 690–694. [Google Scholar] [CrossRef] [PubMed]
- Shahinian, V.B.; Kuo, Y.F.; Freeman, J.L.; Goodwin, J.S. Risk of fracture after androgen deprivation for prostate cancer. N. Engl. J. Med. 2005, 352, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Oefelein, M.G.; Ricchiuti, V.; Conrad, W.; Resnick, M.I. Skeletal fractures negatively correlate with overall survival in men with prostate cancer. J. Urol. 2002, 168, 1005–1007. [Google Scholar] [CrossRef]
- Mittan, D.; Lee, S.; Miller, E.; Perez, R.C.; Basler, J.W.; Bruder, J.M. Bone loss following hypogonadism in men with prostate cancer treated with gnrh analogs. J. Clin. Endocrinol. Metab. 2002, 87, 3656–3661. [Google Scholar] [CrossRef]
- Maillefert, J.F.; Sibilia, J.; Michel, F.; Saussine, C.; Javier, R.M.; Tavernier, C. Bone mineral density in men treated with synthetic gonadotropin-releasing hormone agonists for prostatic carcinoma. J. Urol. 1999, 161, 1219–1222. [Google Scholar] [CrossRef]
- Eriksson, S.; Eriksson, A.; Stege, R.; Carlstrom, K. Bone mineral density in patients with prostatic cancer treated with orchidectomy and with estrogens. Calcif. Tissue Int. 1995, 57, 97–99. [Google Scholar] [CrossRef]
- Alibhai, S.M.; Mohamedali, H.Z.; Gulamhusein, H.; Panju, A.H.; Breunis, H.; Timilshina, N.; Fleshner, N.; Krahn, M.D.; Naglie, G.; Tannock, I.F.; et al. Changes in bone mineral density in men starting androgen deprivation therapy and the protective role of vitamin d. Osteoporos Int. 2013, 24, 2571–2579. [Google Scholar] [CrossRef]
- Morote, J.; Orsola, A.; Abascal, J.M.; Planas, J.; Trilla, E.; Raventos, C.X.; Cecchini, L.; Encabo, G.; Reventos, J. Bone mineral density changes in patients with prostate cancer during the first 2 years of androgen suppression. J. Urol. 2006, 175, 1679–1683. [Google Scholar] [CrossRef]
- Preston, D.M.; Torrens, J.I.; Harding, P.; Howard, R.S.; Duncan, W.E.; McLeod, D.G. Androgen deprivation in men with prostate cancer is associated with an increased rate of bone loss. Prostate Cancer Prostatic Dis. 2002, 5, 304–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziaran, S.; Goncalves, F.M.; Sn, J.B. Complex metabolic and skeletal changes in men taking long-term androgen deprivation therapy. Clin. Genitourin. Cancer 2013, 11, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef]
- Leder, B.Z.; LeBlanc, K.M.; Schoenfeld, D.A.; Eastell, R.; Finkelstein, J.S. Differential effects of androgens and estrogens on bone turnover in normal men. J. Clin. Endocrinol. Metab. 2003, 88, 204–210. [Google Scholar] [CrossRef]
- Benito, M.; Gomberg, B.; Wehrli, F.W.; Weening, R.H.; Zemel, B.; Wright, A.C.; Song, H.K.; Cucchiara, A.; Snyder, P.J. Deterioration of trabecular architecture in hypogonadal men. J. Clin. Endocrinol. Metab. 2003, 88, 1497–1502. [Google Scholar] [CrossRef]
- Hamilton, E.J.; Ghasem-Zadeh, A.; Gianatti, E.; Lim-Joon, D.; Bolton, D.; Zebaze, R.; Seeman, E.; Zajac, J.D.; Grossmann, M. Structural decay of bone microarchitecture in men with prostate cancer treated with androgen deprivation therapy. J. Clin. Endocrinol. Metab. 2010, 95, E456–E463. [Google Scholar] [CrossRef]
- Cheung, A.S.; Zajac, J.D.; Grossmann, M. Muscle and bone effects of androgen deprivation therapy: Current and emerging therapies. Endocr. Relat. Cancer 2014, 21, R371–R394. [Google Scholar] [CrossRef]
- Greenspan, S.L.; Coates, P.; Sereika, S.M.; Nelson, J.B.; Trump, D.L.; Resnick, N.M. Bone loss after initiation of androgen deprivation therapy in patients with prostate cancer. J. Clin. Endocrinol. Metab. 2005, 90, 6410–6417. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.W.; Huo, D.; Stallings, J.W.; Davis, R.L.; Beer, T.M.; McWhorter, L.T. Lifestyle factors and duration of androgen deprivation affect bone mineral density of patients with prostate cancer during first year of therapy. Urology 2007, 70, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Watts, N.B.; Adler, R.A.; Bilezikian, J.P.; Drake, M.T.; Eastell, R.; Orwoll, E.S.; Finkelstein, J.S. Osteoporosis in men: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2012, 97, 1802–1822. [Google Scholar] [CrossRef] [PubMed]
- Alibhai, S.M.; Duong-Hua, M.; Cheung, A.M.; Sutradhar, R.; Warde, P.; Fleshner, N.E.; Paszat, L. Fracture types and risk factors in men with prostate cancer on androgen deprivation therapy: A matched cohort study of 19,079 men. J. Urol. 2010, 184, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.E.; Leslie, W.D.; Czaykowski, P.; Gingerich, J.; Geirnaert, M.; Lau, Y.K. A comprehensive bone-health management approach for men with prostate cancer receiving androgen deprivation therapy. Curr. Oncol. 2011, 18, e163–e172. [Google Scholar] [CrossRef] [PubMed]
- Diamond, T.H.; Higano, C.S.; Smith, M.R.; Guise, T.A.; Singer, F.R. Osteoporosis in men with prostate carcinoma receiving androgen-deprivation therapy: Recommendations for diagnosis and therapies. Cancer 2004, 100, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Gralow, J.R.; Biermann, J.S.; Farooki, A.; Fornier, M.N.; Gagel, R.F.; Kumar, R.; Litsas, G.; McKay, R.; Podoloff, D.A.; Srinivas, S.; et al. Nccn task force report: Bone health in cancer care. J. Natl. Compr. Cancar Netw. 2013, 11 (Suppl. 3), S1–S50; quiz S51. [Google Scholar] [CrossRef]
- Nguyen, P.L.; Alibhai, S.M.; Basaria, S.; D’Amico, A.V.; Kantoff, P.W.; Keating, N.L.; Penson, D.F.; Rosario, D.J.; Tombal, B.; Smith, M.R. Adverse effects of androgen deprivation therapy and strategies to mitigate them. Eur. Urol. 2015, 67, 825–836. [Google Scholar] [CrossRef]
- Poon, Y.; Pechlivanoglou, P.; Alibhai, S.M.H.; Naimark, D.; Hoch, J.S.; Papadimitropoulos, E.; Hogan, M.E.; Krahn, M. Systematic review and network meta-analysis on the relative efficacy of osteoporotic medications: Men with prostate cancer on continuous androgen-deprivation therapy to reduce risk of fragility fractures. BJU Int. 2018, 121, 17–28. [Google Scholar] [CrossRef]
- Hertel, K.L.; Trahiotis, M.G. Exercise in the prevention and treatment of osteoporosis: The role of physical therapy and nursing. Nurs. Clin. N. Am. 2001, 36, 441–453. [Google Scholar]
- Bosco, C.; Bosnyak, Z.; Malmberg, A.; Adolfsson, J.; Keating, N.L.; Van Hemelrijck, M. Quantifying observational evidence for risk of fatal and nonfatal cardiovascular disease following androgen deprivation therapy for prostate cancer: A meta-analysis. Eur. Urol. 2015, 68, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Huang, Y.; Gong, L.; Gan, S.; Chan, F.L.; Gu, C.; Xiang, S.; Wang, S. Association of androgen deprivation therapy with thromboembolic events in patients with prostate cancer: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2018. [Google Scholar] [CrossRef] [PubMed]
- McGinty, H.L.; Phillips, K.M.; Jim, H.S.; Cessna, J.M.; Asvat, Y.; Cases, M.G.; Small, B.J.; Jacobsen, P.B. Cognitive functioning in men receiving androgen deprivation therapy for prostate cancer: A systematic review and meta-analysis. Support Care Cancer 2014, 22, 2271–2280. [Google Scholar] [CrossRef] [PubMed]
- Meng, F.; Zhu, S.; Zhao, J.; Vados, L.; Wang, L.; Zhao, Y.; Zhao, D.; Niu, Y. Stroke related to androgen deprivation therapy for prostate cancer: A meta-analysis and systematic review. BMC Cancer 2016, 16, 180. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.L.; Je, Y.; Schutz, F.A.; Hoffman, K.E.; Hu, J.C.; Parekh, A.; Beckman, J.A.; Choueiri, T.K. Association of androgen deprivation therapy with cardiovascular death in patients with prostate cancer: A meta-analysis of randomized trials. JAMA 2011, 306, 2359–2366. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Sultan, S.; Glasziou, P.; Akl, E.A.; Alonso-Coello, P.; Atkins, D.; Kunz, R.; Brozek, J.; Montori, V.; et al. Grade guidelines: 9. Rating up the quality of evidence. J. Clin. Epidemiol. 2011, 64, 1311–1316. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Design | Group Characteristics (Total Number) | Tumor Stage (Total Number) | Duration of ADT | Follow-Up Period | BMD Check Site | BMD Change Outcome (SD) | Conflict of Interest | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Alibhai et al. [19] | prospective cohort study | ADT | Patients with PCa who underwent continuous ADT for at least 1 year (80) | cT1c N0 M0 (22) cT2 N0 M0 (41) cT3 N0 M0 (17) | 12–36 months | 3 years | 1. Lumbar spine 2. Femoral neck 3. Total hip | Lumbar spine | ADT: −2.12% (7.2) | None |
| Control: −1.05% (4.7) | ||||||||||
| Femoral neck | ADT: −1.99% (6.2) | |||||||||
| Control | Patients with PCa who were not on ADT (80) | cT1c N0 M0 (35) cT2 N0 M0 (43) cT3 N0 M0 (2) | Control: −0.95% (4.9) | |||||||
| Total hip | ADT: −2.62% (4.1) | |||||||||
| Control: 1.02% (4.0) | ||||||||||
| Bergstrom et al. [9] | prospective cohort study | ADT | Patients with either advanced PCa or recurrent disease following primary, local therapy who were treated with bilateral orchidectomy and GnRH analogues continuously (22) | NA | 12 months | 1 year | Femoral neck | ADT | −3.9% (2.3) | Stiftelsen Johanna Hagstrand och Sigfrid Linne’rs Minne and Karolinska Institutet Research funds |
| Control | Patients with other urologic conditions such as BPH, stones (40) | NA | Control | −1.26% (3) | ||||||
| Morote et al. [20] | prospective cohort study | ADT | Patients with PCa who underwent continuous ADT with 3 months of depot LH-RH agonist (31) | cT3a N0 M0 (14) cT3b-4 N0 M0 (7) cT2-4 N1 M0 (10) | 12 months | 1 year | 1. Lumbar spine 2. Femoral neck 3. Total hip | Lumbar spine | ADT: −4.8% (5) | None |
| Control: −0.82% (4.7) | ||||||||||
| Femoral neck | ADT: −2.99% (3.9) | |||||||||
| Control | Patients with PCa free of BCR after RP (31) | cT1c N0 M0 (20) cT2a N0 M0 (11) | Control: −0.64% (4.8) | |||||||
| Total hip | ADT: −3.76% (4.7) | |||||||||
| Control: −0.82% (4.4) | ||||||||||
| Preston et al. [21] | prospective cohort study | ADT | Patients with PCa who had received continuous ADT for a minimum of 6 months for either advanced PCa on presentation or for recurrent disease following primary local therapy (RP or RT) (39) | NA | ≥6 months | 2 years | 1. Lumbar spine 2. Femoral neck 3. Total hip | Lumbar spine | ADT: −0.2% (0.8) | U.S. Army Medical Research and Development Command |
| Control: 1.1% (0.6) | ||||||||||
| Femoral neck | ADT: −1.9% (0.7) | |||||||||
| Control | Patients with other urologic conditions, such as ED or BPH, and those with PCa who had completed primary therapy (RP or RT) with no evidence of disease (39) | NA | Control: 0.6% (0.5) | |||||||
| Total hip | ADT: −1.5% (1) | |||||||||
| Control: −0.8% (0.5) | ||||||||||
| Ziaran et al. [22] | prospective cohort study | ADT | Patients with locally advanced PCa (95) | cT3a N0 M0 (89) pT3b N0 M0 (6) | 24 months | 2 years | 1. Lumbar spine 2. Femoral neck 3. Total hip | Lumbar spine | ADT: −13.28% (1.8) | None |
| Control: −7.32% (1.7) | ||||||||||
| Femoral neck | ADT: −17.14% (1.8) | |||||||||
| Control | Patients with other urologic conditions such as LUTS, stones, etc. (88) | NA | Control: −9.27% (11.3) | |||||||
| Total hip | ADT: 0% (2.7) | |||||||||
| Control: 0% (2.6) | ||||||||||
| Reporting | External Validity | Internal Validity | Power | Total | ||
|---|---|---|---|---|---|---|
| Bias | Confounding (Selection Bias) | |||||
| Alibhai et al. [19] | 7 | 1 | 3 | 3 | 1 | 15 |
| Bergstrom et al. [9] | 6 | 1 | 3 | 2 | 1 | 13 |
| Morote et al. [20] | 7 | 1 | 3 | 3 | 1 | 15 |
| Preston et al. [21] | 7 | 1 | 3 | 4 | 1 | 15 |
| Ziaran et al. [22] | 6 | 1 | 3 | 4 | 1 | 14 |
| Certainty Assessment | Number of Patients | Effect | Certainty | Importance | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | ADT | Control | Absolute (95% CI) | ||
| Lumbar spine | |||||||||||
| 4 | Prospective, cohort studies | Not serious | Serious a | Not serious | Not serious | Dose–response gradient | 245 | 238 | MD 3.6 lower (6.72 lower to 0.47 lower) | ●●◯◯ LOW | CRITICAL |
| Femoral neck | |||||||||||
| 5 | Prospective, cohort studies | Not serious | Serious a | Not serious | Not serious | Dose–response gradient | 267 | 248 | MD 3.11 lower (4.73 lower to 1.48 lower) | ●●◯◯ LOW | CRITICAL |
| Total hip | |||||||||||
| 4 | Prospective, cohort studies | Not serious | Serious a | Not serious | Not serious | Dose–response gradient | 245 | 238 | MD 1.59 lower (2.99 lower to 0.19 lower) | ●●◯◯ LOW | CRITICAL |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.K.; Lee, J.Y.; Kim, K.J.; Hong, N.; Kim, J.W.; Hah, Y.S.; Koo, K.C.; Kim, J.H.; Cho, K.S. Effect of Androgen-Deprivation Therapy on Bone Mineral Density in Patients with Prostate Cancer: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 113. https://doi.org/10.3390/jcm8010113
Kim DK, Lee JY, Kim KJ, Hong N, Kim JW, Hah YS, Koo KC, Kim JH, Cho KS. Effect of Androgen-Deprivation Therapy on Bone Mineral Density in Patients with Prostate Cancer: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(1):113. https://doi.org/10.3390/jcm8010113
Chicago/Turabian StyleKim, Do Kyung, Joo Yong Lee, Kwang Joon Kim, Namki Hong, Jong Won Kim, Yoon Soo Hah, Kyo Chul Koo, Jae Heon Kim, and Kang Su Cho. 2019. "Effect of Androgen-Deprivation Therapy on Bone Mineral Density in Patients with Prostate Cancer: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 1: 113. https://doi.org/10.3390/jcm8010113