Familial Aggregation of Psoriasis and Co-Aggregation of Autoimmune Diseases in Affected Families


Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population and Data Source
2.2. Genealogy Reconstruction
2.3. Case Definition of Psoriasis and Ascertainment of Other Autoimmune Diseases
2.4. Covariates
2.5. Statistical Analysis
3. Results
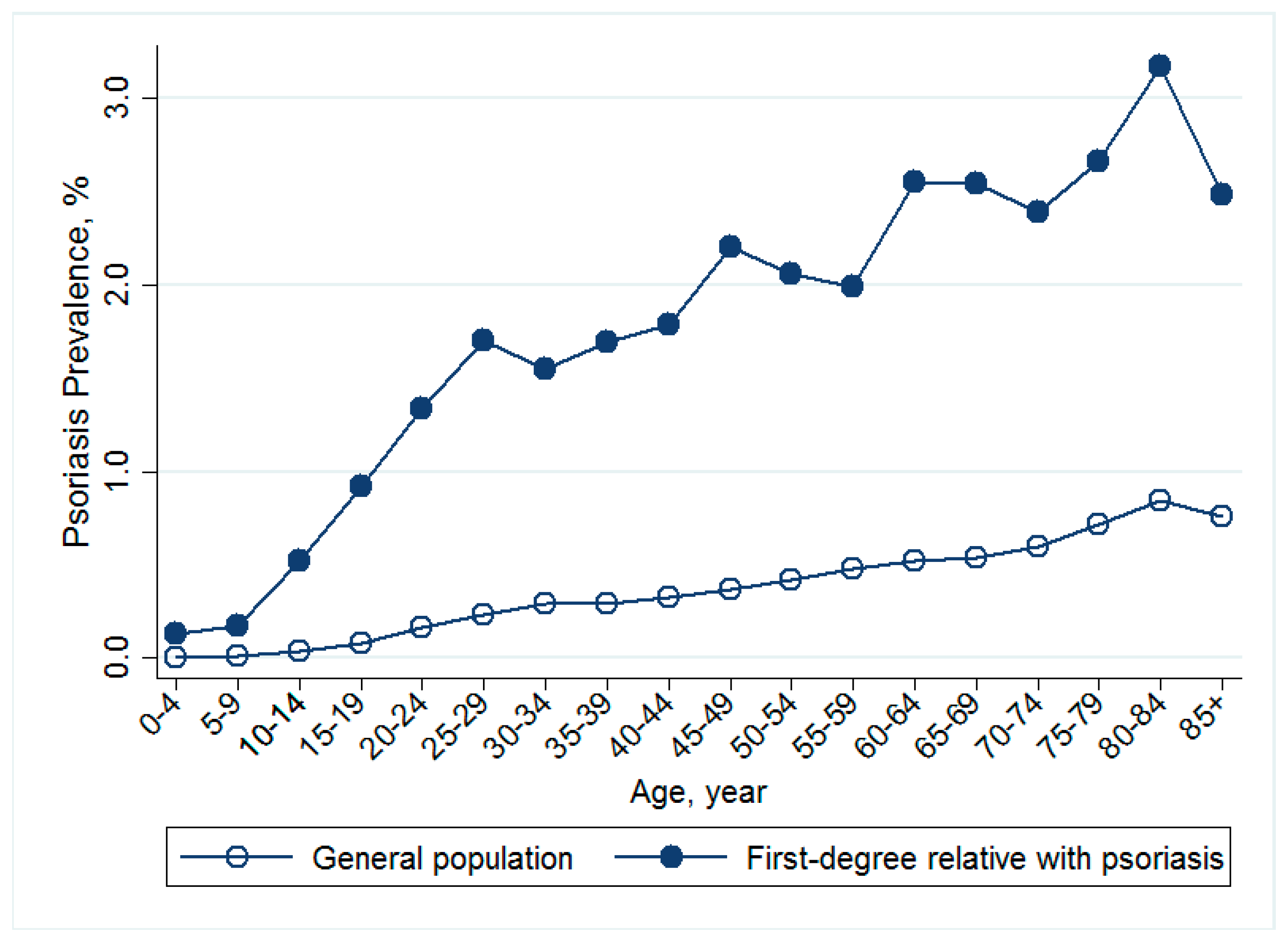
3.1. Prevalence of Psoriasis in Individuals with Affected First-Degree and Second-Degree Family Members versus the General Population
3.2. Relative Risks for Psoriasis in Individuals with Affected First-Degree and Second-Degree Relatives
3.3. Familial Transmission and Heritability of Psoriasis
3.4. Co-Aggregation of Other Autoimmune Diseases
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kupper, T.S.; Fuhlbrigge, R.C. Immune surveillance in the skin: Mechanisms and clinical consequences. Nat. Rev. Immunol. 2004, 4, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Di Meglio, P.; Perera, G.K.; Nestle, F.O. The multitasking organ: Recent insights into skin immune function. Immunity 2011, 35, 857–869. [Google Scholar] [CrossRef] [PubMed]
- Lowes, M.A.; Suarez-Farinas, M.; Krueger, J.G. Immunology of psoriasis. Annu. Rev. Immunol. 2014, 32, 227–255. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Kamijima, Y.; Sato, T.; Ooba, N.; Koide, D.; Iizuka, H.; Nakagawa, H. Epidemiology of psoriasis and palmoplantar pustulosis: A nationwide study using the japanese national claims database. BMJ Open 2015, 5, e006450. [Google Scholar] [CrossRef] [PubMed]
- Rachakonda, T.D.; Schupp, C.W.; Armstrong, A.W. Psoriasis prevalence among adults in the united states. J. Am. Acad. Dermatol. 2014, 70, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.T.; Chen, T.J.; Liu, P.C.; Chen, Y.C.; Chen, Y.J.; Huang, Y.L.; Jih, J.S.; Chen, C.C.; Lee, D.D.; Wang, W.J.; et al. Epidemiological study of psoriasis in the national health insurance database in taiwan. Acta Dermato-Venereol. 2009, 89, 262–266. [Google Scholar] [CrossRef]
- Farber, E.M.; Nall, M.L.; Watson, W. Natural history of psoriasis in 61 twin pairs. Arch. Dermatol. 1974, 109, 207–211. [Google Scholar] [CrossRef]
- Brandrup, F.; Hauge, M.; Henningsen, K.; Eriksen, B. Psoriasis in an unselected series of twins. Arch. Dermatol. 1978, 114, 874–878. [Google Scholar] [CrossRef]
- Brandrup, F.; Holm, N.; Grunnet, N.; Henningsen, K.; Hansen, H.E. Psoriasis in monozygotic twins: Variations in expression in individuals with identical genetic constitution. Acta Dermato-Venereol. 1982, 62, 229–236. [Google Scholar]
- Duffy, D.L.; Spelman, L.S.; Martin, N.G. Psoriasis in australian twins. J. Am. Acad. Dermatol. 1993, 29, 428–434. [Google Scholar] [CrossRef]
- Grjibovski, A.M.; Olsen, A.O.; Magnus, P.; Harris, J.R. Psoriasis in norwegian twins: Contribution of genetic and environmental effects. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Lonnberg, A.S.; Skov, L.; Skytthe, A.; Kyvik, K.O.; Pedersen, O.B.; Thomsen, S.F. Heritability of psoriasis in a large twin sample. Br. J. Dermatol. 2013, 169, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Elder, J.T.; Nair, R.P.; Guo, S.W.; Henseler, T.; Christophers, E.; Voorhees, J.J. The genetics of psoriasis. Arch. Dermatol. 1994, 130, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Di Lernia, V.; Ficarelli, E.; Lallas, A.; Ricci, C. Familial aggregation of moderate to severe plaque psoriasis. Clin. Exp. Dermatol. 2014, 39, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Henseler, T.; Christophers, E. Psoriasis of early and late onset: Characterization of two types of psoriasis vulgaris. J. Am. Acad. Dermatol. 1985, 13, 450–456. [Google Scholar] [CrossRef]
- Tsoi, L.C.; Spain, S.L.; Knight, J.; Ellinghaus, E.; Stuart, P.E.; Capon, F.; Ding, J.; Li, Y.; Tejasvi, T.; Gudjonsson, J.E.; et al. Identification of 15 new psoriasis susceptibility loci highlights the role of innate immunity. Nat. Genet. 2012, 44, 1341–1348. [Google Scholar] [CrossRef] [Green Version]
- Schön, M.P.; Boehncke, W.-H. Psoriasis. N. Engl. J. Med. 2005, 352, 1899–1912. [Google Scholar] [CrossRef]
- Naldi, L.; Peli, L.; Parazzini, F. Association of early-stage psoriasis with smoking and male alcohol consumption: Evidence from an italian case-control study. Arch. Dermatol. 1999, 135, 1479–1484. [Google Scholar] [CrossRef]
- Cotsapas, C.; Voight, B.F.; Rossin, E.; Lage, K.; Neale, B.M.; Wallace, C.; Abecasis, G.R.; Barrett, J.C.; Behrens, T.; Cho, J.; et al. Pervasive sharing of genetic effects in autoimmune disease. PLoS Genet. 2011, 7, e1002254. [Google Scholar] [CrossRef]
- Bureau of National Health Insurance. The National Health Insurance Statistics. 2010. Available online: http://www.Nhi.Gov.Tw/english/webdata/webdata.Aspx?Menu=11&menu_id=296&webdata_id=1942&wd_id=296 (accessed on 15 May 2012).
- Kuo, C.F.; Grainge, M.J.; See, L.C.; Yu, K.H.; Luo, S.F.; Valdes, A.M.; Zhang, W.; Doherty, M. Familial aggregation of gout and relative genetic and environmental contributions: A nationwide population study in taiwan. Ann. Rheum. Dis. 2015, 74, 369–374. [Google Scholar] [CrossRef]
- Kuo, C.F.; Grainge, M.J.; Valdes, A.M.; See, L.C.; Luo, S.F.; Yu, K.H.; Zhang, W.; Doherty, M. Familial risk of sjogren’s syndrome and co-aggregation of autoimmune diseases in affected families: A nationwide population study. Arthrit. Rheumatol. 2015, 67, 1904–1912. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.F.; Grainge, M.J.; Valdes, A.M.; See, L.C.; Luo, S.F.; Yu, K.H.; Zhang, W.; Doherty, M. Familial aggregation of systemic lupus erythematosus and coaggregation of autoimmune diseases in affected families. JAMA Intern Med. 2015, 175, 1518–1526. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Huang, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating development stratification of taiwan townships into sampling design of large scale health interview survey. J. Health Manag. 2006, 14, 1–22. [Google Scholar]
- Risch, N. Linkage strategies for genetically complex traits. I. Multilocus models. Am. J. Hum. Genet. 1990, 46, 222–228. [Google Scholar] [PubMed]
- Lee, J.; Chia, K.S. Estimation of prevalence rate ratios for cross sectional data: An example in occupational epidemiology. Br. J. Ind. Med. 1993, 50, 861–862. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.Y. Cox regression analysis of multivariate failure time data: The marginal approach. Stat. Med. 1994, 13, 2233–2247. [Google Scholar] [CrossRef]
- Falconer, D.S. The inheritance of liability to diseases with variable age of onset, with particular reference to diabetes mellitus. Ann. Hum. Genet. 1967, 31, 1–20. [Google Scholar] [CrossRef]
- Reich, T.; James, J.W.; Morris, C.A. The use of multiple thresholds in determining the mode of transmission of semi-continuous traits. Ann. Hum. Genet. 1972, 36, 163–184. [Google Scholar] [CrossRef]
- Reich, T.; Rice, J.; Cloninger, C.R.; Wette, R.; James, J. The use of multiple thresholds and segregation analysis in analyzing the phenotypic heterogeneity of multifactorial traits. Ann. Hum. Genet. 1979, 42, 371–390. [Google Scholar] [CrossRef]
- Yang, J.; Visscher, P.M.; Wray, N.R. Sporadic cases are the norm for complex disease. Eur. J. Hum. Genet. 2010, 18, 1039–1043. [Google Scholar] [CrossRef]
- Eder, L.; Chandran, V.; Gladman, D.D. What have we learned about genetic susceptibility in psoriasis and psoriatic arthritis? Curr. Opin. Rheumatol. 2015, 27, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.T.; Nijsten, T.; Elder, J.T. Recent highlights in psoriasis research. J. Investig. Dermatol. 2017, 137, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Manolio, T.A.; Collins, F.S.; Cox, N.J.; Goldstein, D.B.; Hindorff, L.A.; Hunter, D.J.; McCarthy, M.I.; Ramos, E.M.; Cardon, L.R.; Chakravarti, A.; et al. Finding the missing heritability of complex diseases. Nature 2009, 461, 747–753. [Google Scholar] [CrossRef] [Green Version]
- Zuk, O.; Hechter, E.; Sunyaev, S.R.; Lander, E.S. The mystery of missing heritability: Genetic interactions create phantom heritability. Proc. Natl. Acad. Sci. USA 2012, 109, 1193–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, N.; Frisch, M.; Rostgaard, K.; Wohlfahrt, J.; Hjalgrim, H.; Koch-Henriksen, N.; Melbye, M.; Westergaard, T. Autoimmune diseases in patients with multiple sclerosis and their first-degree relatives: A nationwide cohort study in denmark. Mult. Scler. J. 2008, 14, 823–829. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Women | Men | |||||
|---|---|---|---|---|---|---|
| Variable | With Affected FDR | General Population | p-Value | With Affected FDR | General Population | p-Value |
| No. | 69,146 | 11,651,851 | 71,500 | 11,322,921 | ||
| Age, mean (SD), y | 34.6 (18.7) | 38.1 (20.6) | <0.0001 | 34.7 (18.4) | 37.5 (20.8) | <0.0001 |
| Psoriasis, no. (%) | 971 (1.40) | 25,869 (0.22) | 1227 (1.72) | 43,959 (0.39) | ||
| Place of residence, no. (%) | ||||||
| Urban | 22,713 (32.85) | 3,612,878 (31.01) | <0.0001 | 21,774 (30.45) | 3,252,550 (28.73) | <0.0001 |
| Suburban | 20,195 (29.21) | 3,335,036 (28.62) | 20,962 (29.32) | 3,191,129 (28.18) | ||
| Rural | 26,238 (37.95) | 4,703,766 (40.37) | 28,763 (40.23) | 4,879,055 (43.09) | ||
| Income levels, no. (%) | ||||||
| Quintile 1 | 10,495 (15.18) | 1,915,419 (16.44) | <0.0001 | 11,644 (16.29) | 2,0616,15 (18.21) | <0.0001 |
| Quintile 2 | 11,059 (15.99) | 1,839,396 (15.79) | 9880 (13.82) | 1,492,191 (13.18) | ||
| Quintile 3 | 17,034 (24.63) | 3,252,344 (27.91) | 18,831 (26.34) | 3,218,505 (28.42) | ||
| Quintile 4 | 15,384 (22.25) | 2,297,299 (19.72) | 16,380 (22.91) | 2,326,478 (20.55) | ||
| Quintile 5 | 15,128 (21.88) | 2,3387,21 (20.07) | 14,733 (20.61) | 2,217,347 (19.58) | ||
| Occupation, no. (%) | ||||||
| Dependents of the insured individuals | 27,246 (39.4) | 4,529,265 (38.87) | <0.0001 | 24,591 (34.39) | 3,781,887 (33.4) | <0.0001 |
| Civil servants, teachers, military personnel, and veterans | 2707 (3.910) | 414,522 (3.56) | 3256 (4.55) | 604,575 (5.34) | ||
| Nonmanual workers and professionals | 21,502 (31.10) | 3,096,472 (26.57) | 24198 (33.84) | 3,382,170 (29.87) | ||
| Manual workers | 12,348 (17.86) | 2,699,172 (23.17) | 12,308 (17.21) | 2,347,070 (20.73) | ||
| Other | 5343 (7.73) | 912,420 (7.83) | 7147 (10.00) | 1,207,219 (10.66) | ||
| Type of Affected Relative | Gender of Affected Relative | Gender of Individual | No. of Cases | Relative Risks (95% Confidence Interval) 1 |
|---|---|---|---|---|
| Any | Male | Male | 765 | 4.81 (4.37–5.29) |
| Female | 555 | 5.86 (5.39–6.37) | ||
| All | 1320 | 5.20 (4.86–5.56) | ||
| Female | Male | 523 | 5.41 (4.95–5.90) | |
| Female | 459 | 8.55 (7.54–9.70) | ||
| All | 982 | 6.55 (6.06–7.07) | ||
| All | Male | 1227 | 4.84 (4.53–5.18) | |
| Female | 971 | 6.61 (6.14–7.12) | ||
| All | 2198 | 5.50 (5.19–5.82) | ||
| Parent | Male | Male | 295 | 4.19 (3.74–4.71) |
| Female | 183 | 4.59 (3.98–5.31) | ||
| All | 478 | 4.33 (3.95–4.75) | ||
| Female | Male | 235 | 5.76 (5.05–6.57) | |
| Female | 175 | 8.69 (7.49–10.09) | ||
| All | 410 | 6.75 (6.10–7.47) | ||
| All | Male | 510 | 4.62 (4.23–5.04) | |
| Female | 349 | 5.85 (5.27–6.49) | ||
| All | 859 | 5.05 (4.72–5.41) | ||
| Offspring | Male | Male | 268 | 4.35 (3.87–4.90) |
| Female | 237 | 6.26 (5.52–7.11) | ||
| All | 505 | 5.08 (4.65–5.55) | ||
| Female | Male | 161 | 4.19 (3.60–4.88) | |
| Female | 170 | 8.14 (7.01–9.45) | ||
| All | 331 | 5.61 (5.04–6.25) | ||
| All | Male | 418 | 4.21 (3.83–4.62) | |
| Female | 396 | 6.79 (6.15–7.49) | ||
| All | 814 | 5.16 (4.81–5.54) | ||
| Sibling | Male | Male | 203 | 7.43 (6.16–8.96) |
| Female | 146 | 8.35 (7.09–9.82) | ||
| All | 349 | 7.83 (6.88–8.91) | ||
| Female | Male | 139 | 7.74 (6.55–9.15) | |
| Female | 111 | 8.8 (6.82–11.36) | ||
| All | 250 | 8.19 (7.06–9.50) | ||
| All | Male | 336 | 7.45 (6.54–8.49) | |
| Female | 251 | 8.38 (7.26–9.68) | ||
| All | 587 | 7.85 (7.02–8.77) | ||
| Twin | Male | Male | 18 | 57.63 (33.87–98.08) |
| Female | 1 | 45.7 (7.00–298.5) | ||
| All | 19 | 52.3 (31.37–87.2) | ||
| Female | Male | N/A | N/A | |
| Female | 15 | 91.95 (48.49–174.38) | ||
| All | 15 | 85.83 (44.27–166.42) | ||
| All | Male | 18 | 51.77 (30.22–88.69) | |
| Female | 16 | 86.61 (46.94–159.83) | ||
| All | 34 | 63.19 (42.02–95.05) | ||
| Spouse | Female | Male | 252 | 3.80 (3.36–4.29) |
| Male | Female | 263 | 3.62 (3.21–4.08) | |
| All | All | 515 | 3.63 (3.24–4.07) |
| Type of Affected relative | Gender of Affected relative | Gender of Individual | No. of Cases | Relative Risks (95% Confidence Interval) 1 |
|---|---|---|---|---|
| Any | Male | Male | 42 | 1.80 (1.21–2.70) |
| Female | 42 | 2.40 (1.78–3.24) | ||
| All | 84 | 2.05 (1.58–2.66) | ||
| Female | Male | 48 | 2.94 (2.18–3.95) | |
| Female | 51 | 4.06 (2.80–5.90) | ||
| All | 99 | 3.42 (2.67–4.38) | ||
| All | Male | 86 | 2.19 (1.70–2.82) | |
| Female | 90 | 3.03 (2.36–3.89) | ||
| All | 176 | 2.54 (2.08–3.12) | ||
| Aunt/uncle | Male | Male | 10 | 1.97 (1.07–3.66) |
| Female | 7 | 1.79 (0.85–3.74) | ||
| All | 17 | 1.89 (1.18–3.03) | ||
| Female | Male | 1 | 0.62 (0.09–4.36) | |
| Female | 8 | 6.25 (2.91–13.43) | ||
| All | 9 | 3.10 (1.51–6.36) | ||
| All | Male | 11 | 1.65 (0.92–2.97) | |
| Female | 15 | 2.89 (1.69–4.94) | ||
| All | 26 | 2.19 (1.47–3.25) | ||
| Niece/nephew | Male | Male | 11 | 2.22 (1.23–3.99) |
| Female | 1 | 0.71 (0.10–5.05) | ||
| All | 12 | 1.91 (1.09–3.35) | ||
| Female | Male | 8 | 2.29 (1.15–4.56) | |
| Female | 8 | 7.96 (4.02–15.77) | ||
| All | 16 | 3.61 (2.16–6.05) | ||
| All | Male | 19 | 2.26 (1.45–3.54) | |
| Female | 9 | 3.79 (1.99–7.23) | ||
| All | 28 | 2.63 (1.80–3.85) | ||
| Grandparent | Male | Male | 12 | 1.45 (0.83–2.55) |
| Female | 14 | 2.07 (1.23–3.48) | ||
| All | 26 | 1.72 (1.16–2.56) | ||
| Female | Male | 28 | 3.76 (2.51–5.62) | |
| Female | 19 | 3.15 (2.01–4.93) | ||
| All | 47 | 3.48 (2.55–4.75) | ||
| All | Male | 37 | 2.37 (1.68–3.34) | |
| Female | 32 | 2.52 (1.79–3.56) | ||
| All | 69 | 2.43 (1.90–3.12) | ||
| Grandchildren | Male | Male | 9 | 1.77 (0.93–3.39) |
| Female | 20 | 3.64 (2.36–5.62) | ||
| All | 29 | 2.72 (1.85–4.00) | ||
| Female | Male | 11 | 2.89 (1.61–5.17) | |
| Female | 16 | 3.75 (2.31–6.10) | ||
| All | 27 | 3.31 (2.26–4.86) | ||
| All | Male | 19 | 2.16 (1.38–3.37) | |
| Female | 34 | 3.52 (2.52–4.92) | ||
| All | 53 | 2.85 (2.17–3.75) |
| Autoimmune Diseases | Gender of Individual | With Affected Relatives | General Population | Relative Risk (95% Confidence Interval) 1 | ||
|---|---|---|---|---|---|---|
| No. of Cases | Prevalence (%) | No. of Cases | Prevalence (%) | |||
| >With affected first-degree relatives with psoriasis | ||||||
| Rheumatoid arthritis | Male | 62 | 0.09 | 7739 | 0.07 | 1.50 (1.17–1.92) |
| Female | 175 | 0.25 | 29273 | 0.25 | 1.27 (1.10–1.47) | |
| All | 237 | 0.17 | 37,012 | 0.16 | 1.32 (1.16–1.50) | |
| Sjögren’s syndrome | Male | 8 | 0.01 | 1237 | 0.01 | 1.32 (0.66–2.62) |
| Female | 78 | 0.11 | 11,019 | 0.09 | 1.47 (1.18–1.84) | |
| All | 86 | 0.06 | 12,256 | 0.05 | 1.45 (1.17–1.79) | |
| Systemic lupus erythematosus | Male | 13 | 0.02 | 1963 | 0.02 | 1.06 (0.61–1.82) |
| Female | 124 | 0.18 | 16,646 | 0.14 | 1.27 (1.07–1.52) | |
| All | 137 | 0.10 | 18,609 | 0.08 | 1.25 (1.05–1.48) | |
| Systemic sclerosis | Male | 1 | 0.001 | 377 | 0.003 | 0.47 (0.07–3.29) |
| Female | 14 | 0.02 | 1451 | 0.01 | 1.45 (1.17–1.79) | |
| All | 15 | 0.01 | 1828 | 0.01 | 1.94 (1.15–3.27) | |
| Polymyositis/Dermatomyositis | Male | 6 | 0.01 | 529 | 0.004 | 1.86 (0.84–4.13) |
| Female | 3 | 0.004 | 1219 | 0.01 | 0.46 (0.15–1.43) | |
| All | 194 | 0.14 | 34,000 | 0.15 | 1.17(1.01–1.35) | |
| Inflammatory Bowel Disease | Male | 16 | 0.02 | 1651 | 0.01 | 1.55 (0.95–2.52) |
| Female | 4 | 0.01 | 993 | 0.01 | 0.76 (0.29–2.04) | |
| All | 20 | 0.01 | 2644 | 0.01 | 1.29 (0.83–1.99) | |
| Multiple Sclerosis | Male | 1 | 0.001 | 279 | 0.002 | 0.53 (0.07–3.73) |
| Female | 7 | 0.01 | 926 | 0.01 | 1.29 (0.62–2.71) | |
| All | 8 | 0.01 | 1205 | 0.01 | 1.09 (0.55–2.19) | |
| With affected second-degree relatives with psoriasis | ||||||
| Rheumatoid arthritis | Male | 6 | 0.02 | 7739 | 0.07 | 0.89 (0.40–1.97) |
| Female | 24 | 0.10 | 29273 | 0.25 | 1.13 (0.76–1.69) | |
| All | 30 | 0.06 | 37,012 | 0.16 | 1.07 (0.75–1.52) | |
| Sjögren’s syndrome | Male | 2 | 0.01 | 1237 | 0.01 | 2.38 (0.60–9.54) |
| Female | 9 | 0.04 | 11,019 | 0.09 | 1.23 (0.60–2.52) | |
| All | 11 | 0.02 | 12,256 | 0.05 | 1.30 (0.69–2.47) | |
| Systemic lupus erythematosus | Male | 4 | 0.02 | 1963 | 0.02 | 1.78 (0.67–4.76) |
| Female | 16 | 0.07 | 16,646 | 0.14 | 0.99 (0.61–1.62) | |
| All | 20 | 0.04 | 18,609 | 0.08 | 1.09 (0.70–1.68) | |
| Systemic sclerosis | Male | N/A | N/A | 377 | 0.003 | N/A 2 |
| Female | N/A | N/A | 1451 | 0.01 | N/A | |
| All | N/A | N/A | 1828 | 0.01 | N/A | |
| Polymyositis/Dermatomyositis | Male | 1 | 0.004 | 529 | 0.004 | 1.62 (0.23–11.57) |
| Female | 1 | 0.004 | 1219 | 0.01 | 0.87 (0.12–6.24) | |
| All | 32 | 0.07 | 34000 | 0.15 | 1.17(0.82–1.67) | |
| Inflammatory Bowel Disease | Male | 2 | 0.01 | 1651 | 0.01 | 1.25 (0.31–4.99) |
| Female | N/A | N/A | 993 | 0.01 | N/A | |
| All | 2 | 0.004 | 2644 | 0.01 | 0.81 (0.20–3.22) | |
| Multiple Sclerosis | Male | N/A | N/A | 279 | 0.002 | N/A |
| Female | 1 | 0.004 | 926 | 0.01 | 1.18 (0.17–8.36) | |
| All | 1 | 0.002 | 1205 | 0.01 | 0.84 (0.12–5.96) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-H.; Kuo, C.-F.; Huang, L.-H.; Hsieh, M.-Y. Familial Aggregation of Psoriasis and Co-Aggregation of Autoimmune Diseases in Affected Families. J. Clin. Med. 2019, 8, 115. https://doi.org/10.3390/jcm8010115
Huang Y-H, Kuo C-F, Huang L-H, Hsieh M-Y. Familial Aggregation of Psoriasis and Co-Aggregation of Autoimmune Diseases in Affected Families. Journal of Clinical Medicine. 2019; 8(1):115. https://doi.org/10.3390/jcm8010115
Chicago/Turabian StyleHuang, Yu-Huei, Chang-Fu Kuo, Lu-Hsiang Huang, and Mei-Yun Hsieh. 2019. "Familial Aggregation of Psoriasis and Co-Aggregation of Autoimmune Diseases in Affected Families" Journal of Clinical Medicine 8, no. 1: 115. https://doi.org/10.3390/jcm8010115