Molecular Profile of Advanced Non-Small Cell Lung Cancers in Octogenarians: The Door to Precision Medicine in Elderly Patients

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Next-Generation Sequencing Analysis
2.3. Fluorescence in Situ Hybridization Analysis
2.4. PD-L1 Immunohistochemical Analysis
3. Results
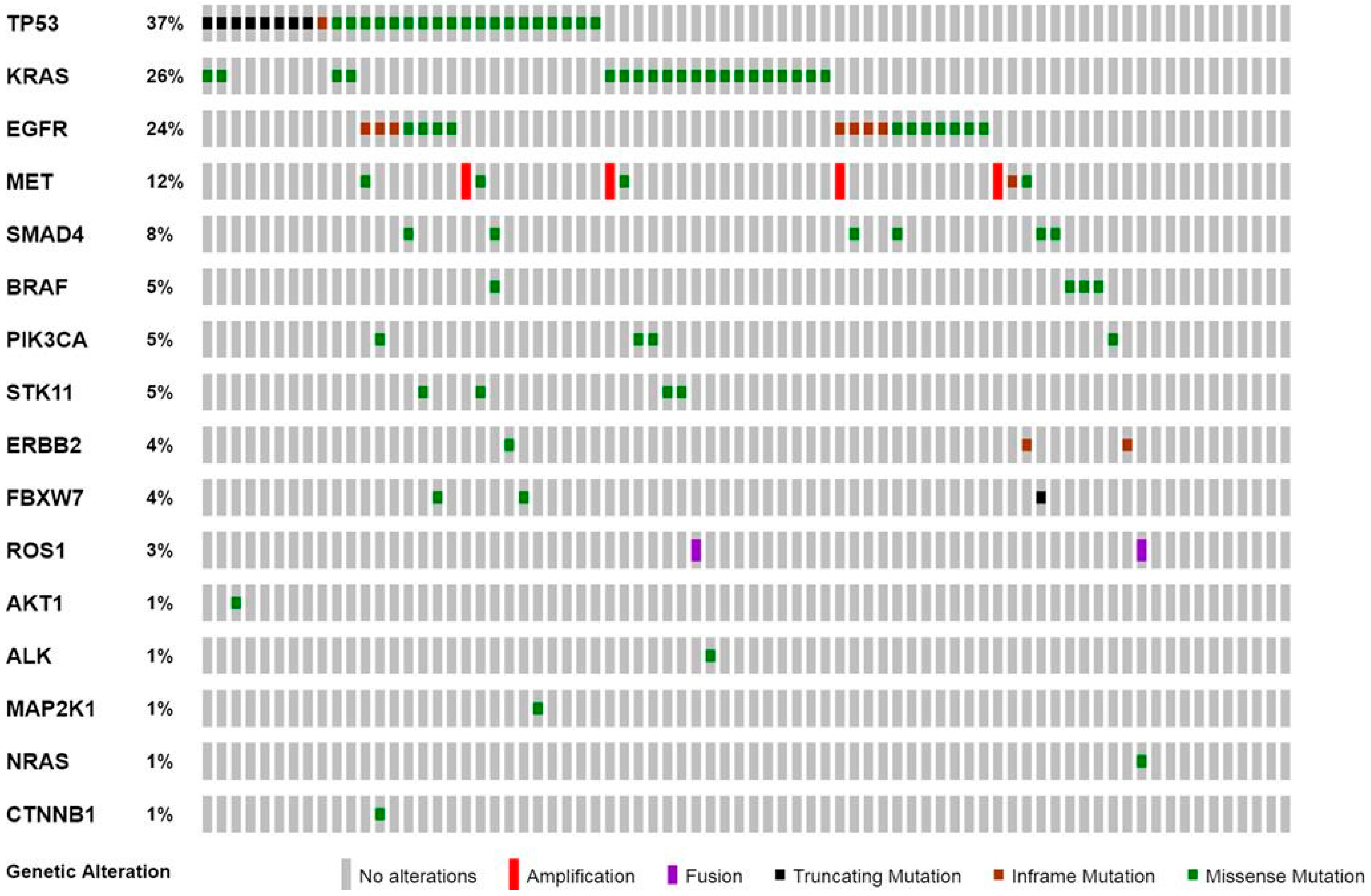
3.1. Molecular Profile of Advanced Non-Small Cell Lung Cancer in Octogenarian Patients
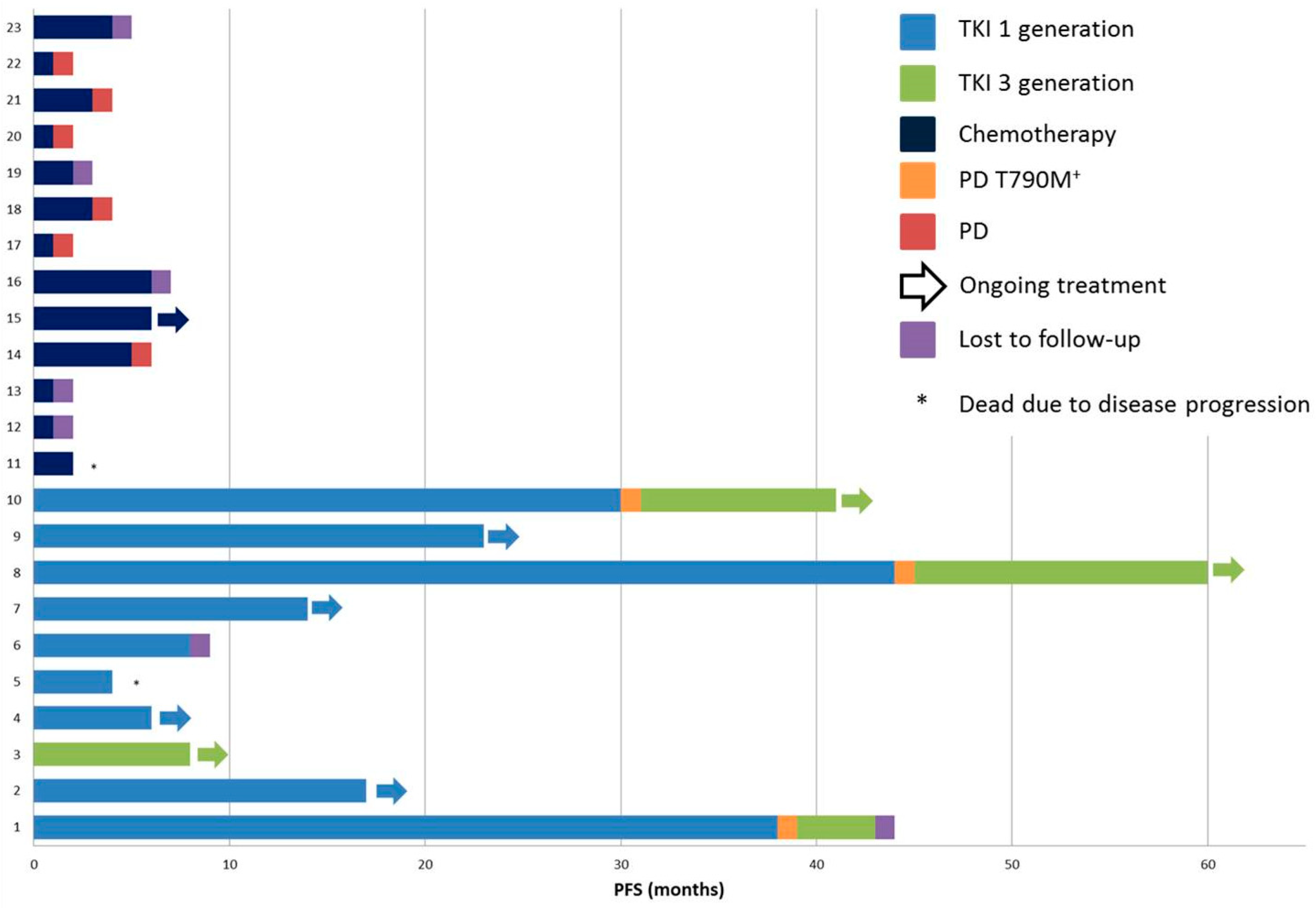
3.2. Treatment Regimens and Clinical Outcome of Octogenarian Patients with Advanced Non-Small Cell Lung Cancers
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. Cancer J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Bethesda. SEER Cancer Stat Facts: Lung and Bronchus Cancer. National Cancer Institute. Available online: https://seer.cancer.gov/statfacts/html/lungb.html (accessed on 21 November 2018).
- Gonzalez-Aragoneses, F.; Moreno-Mata, N.; Simon-Adiego, C.; Penalver-Pascual, R.; Gonzalez-Casaurran, G.; Perea, L.A. Lung cancer surgery in the elderly. Crit. Rev. Oncol. Hematol. 2009, 71, 266–271. [Google Scholar] [CrossRef]
- Vestergaard, H.H.; Christensen, M.R.; Lassen, U.N. A systematic review of targeted agents for non-small cell lung cancer. Acta Oncol. 2018, 57, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Ryser, C.O.; Diebold, J.; Gautschi, O. Treatment of anaplastic lymphoma kinase-positive non-small cell lung cancer: Update and perspectives. Curr. Opin. Oncol. 2019, 31, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wong, M.L.; Hamilton, N.; Davoren, J.B.; Jahan, T.M.; Walter, L.C. Impact of age and comorbidity on non-small-cell lung cancer treatment in older veterans. J. Clin. Oncol. 2012, 30, 1447–1455. [Google Scholar] [CrossRef] [PubMed]
- Schulkes, K.J.; Nguyen, C.; van den Bos, F.; van Elden, L.J.; Hamaker, M.E. Selection of Patients in Ongoing Clinical Trials on Lung Cancer. Lung 2016, 194, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Kalemkerian, G.P.; Narula, N.; Kennedy, E.B. Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors: American Society of Clinical Oncology Endorsement Summary of the College of American Pathologists/International Association for the Study of Lung Cancer/Association for Molecular Pathology Clinical Practice Guideline Update. J. Oncol. Pract. 2018, 14, 323–327. [Google Scholar] [CrossRef]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. J. Thorac. Oncol. 2018, 13, 323–358. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Fumagalli, C.; Vacirca, D.; Rappa, A.; Passaro, A.; Guarize, J.; Rafaniello Raviele, P.; de Marinis, F.; Spaggiari, L.; Casadio, C.; Viale, G.; et al. The long tail of molecular alterations in non-small cell lung cancer: A single-institution experience of next-generation sequencing in clinical molecular diagnostics. J. Clin. Pathol. 2018, 71, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef]
- Sukhai, M.A.; Craddock, K.J.; Thomas, M.; Hansen, A.R.; Zhang, T.; Siu, L.; Bedard, P.; Stockley, T.L.; Kamel-Reid, S. A classification system for clinical relevance of somatic variants identified in molecular profiling of cancer. Genet. Med. 2016, 18, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, A.; Barberis, M.; Franco, R.; De Luca, G.; Pace, M.V.; Staibano, S.; Volante, M.; Buttitta, F.; Guerini-Rocco, E.; Righi, L.; et al. Multicenter Comparison of 22C3 PharmDx (Agilent) and SP263 (Ventana) Assays to Test PD-L1 Expression for NSCLC Patients to Be Treated with Immune Checkpoint Inhibitors. J. Thorac. Oncol. 2017, 12, 1654–1663. [Google Scholar] [CrossRef] [PubMed]
- Kwak, E.L.; Bang, Y.J.; Camidge, D.R.; Shaw, A.T.; Solomon, B.; Maki, R.G.; Ou, S.H.; Dezube, B.J.; Janne, P.A.; Costa, D.B.; et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 1693–1703. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K.; Takeuchi, K.; Togashi, Y.; Hatano, S.; Ninomiya, H.; Motoi, N.; Mun, M.Y.; Sakao, Y.; Okumura, S.; Nakagawa, K.; et al. EML4-ALK lung cancers are characterized by rare other mutations, a TTF-1 cell lineage, an acinar histology, and young onset. Mod. Pathol. 2009, 22, 508–515. [Google Scholar] [CrossRef]
- Bergethon, K.; Shaw, A.T.; Ou, S.H.; Katayama, R.; Lovly, C.M.; McDonald, N.T.; Massion, P.P.; Siwak-Tapp, C.; Gonzalez, A.; Fang, R.; et al. ROS1 rearrangements define a unique molecular class of lung cancers. J. Clin. Oncol. 2012, 30, 863–870. [Google Scholar] [CrossRef]
- Davies, K.D.; Le, A.T.; Theodoro, M.F.; Skokan, M.C.; Aisner, D.L.; Berge, E.M.; Terracciano, L.M.; Cappuzzo, F.; Incarbone, M.; Roncalli, M.; et al. Identifying and targeting ROS1 gene fusions in non-small cell lung cancer. Clin. Cancer Res. 2012, 18, 4570–4579. [Google Scholar] [CrossRef]
- Lin, J.J.; Ritterhouse, L.L.; Ali, S.M.; Bailey, M.; Schrock, A.B.; Gainor, J.F.; Ferris, L.A.; Mino-Kenudson, M.; Miller, V.A.; Iafrate, A.J.; et al. ROS1 Fusions Rarely Overlap with Other Oncogenic Drivers in Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 872–877. [Google Scholar] [CrossRef]
- Zhu, Y.C.; Lin, X.P.; Li, X.F.; Wu, L.X.; Chen, H.F.; Wang, W.X.; Xu, C.W.; Shen, J.F.; Wei, J.G.; Du, K.Q. Concurrent ROS1 gene rearrangement and KRAS mutation in lung adenocarcinoma: A case report and literature review. Thorac. Cancer 2018, 9, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Li, B.T.; Shen, R.; Buonocore, D.; Olah, Z.T.; Ni, A.; Ginsberg, M.S.; Ulaner, G.A.; Offin, M.; Feldman, D.; Hembrough, T.; et al. Ado-Trastuzumab Emtansine for Patients With HER2-Mutant Lung Cancers: Results From a Phase II Basket Trial. J. Clin. Oncol. 2018, 36, 2532–2537. [Google Scholar] [CrossRef] [PubMed]
- Baik, C.S.; Myall, N.J.; Wakelee, H.A. Targeting BRAF-Mutant Non-Small Cell Lung Cancer: From Molecular Profiling to Rationally Designed Therapy. Oncologist 2017, 22, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.B. TP53 mutations are predictive and prognostic when co-occurring with ALK rearrangements in lung cancer. Ann. Oncol. 2018, 29, 2028–2030. [Google Scholar] [CrossRef] [PubMed]
- VanderLaan, P.A.; Rangachari, D.; Mockus, S.M.; Spotlow, V.; Reddi, H.V.; Malcolm, J.; Huberman, M.S.; Joseph, L.J.; Kobayashi, S.S.; Costa, D.B. Mutations in TP53, PIK3CA, PTEN and other genes in EGFR mutated lung cancers: Correlation with clinical outcomes. Lung Cancer 2017, 106, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Byers, L.A.; Diao, L.; Papadimitrakopoulou, V.A.; Tong, P.; Izzo, J.; Behrens, C.; Kadara, H.; Parra, E.R.; Canales, J.R.; et al. Co-occurring genomic alterations define major subsets of KRAS-mutant lung adenocarcinoma with distinct biology, immune profiles, and therapeutic vulnerabilities. Cancer Discov. 2015, 5, 860–877. [Google Scholar] [CrossRef] [PubMed]
- Haspinger, E.R.; Agustoni, F.; Torri, V.; Gelsomino, F.; Platania, M.; Zilembo, N.; Gallucci, R.; Garassino, M.C.; Cinquini, M. Is there evidence for different effects among EGFR-TKIs? Systematic review and meta-analysis of EGFR tyrosine kinase inhibitors (TKIs) versus chemotherapy as first-line treatment for patients harboring EGFR mutations. Crit. Rev. Oncol. Hematol. 2015, 94, 213–227. [Google Scholar] [CrossRef] [PubMed]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Sequist, L.V.; Yang, J.C.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.M.; Boyer, M.; et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef]
- Soria, J.C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Janne, P.A.; Yang, J.C.; Kim, D.W.; Planchard, D.; Ohe, Y.; Ramalingam, S.S.; Ahn, M.J.; Kim, S.W.; Su, W.C.; Horn, L.; et al. AZD9291 in EGFR inhibitor-resistant non-small-cell lung cancer. N. Engl. J. Med. 2015, 372, 1689–1699. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.-L.; Ahn, M.-J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.; et al. Osimertinib or Platinum-Pemetrexed in EGFR T790M-Positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, L. Lung cancer: AURA3 magic reveals new standard. Nat. Rev. Clin. Oncol. 2017, 14, 69. [Google Scholar] [CrossRef]
- Furuta, H.; Uemura, T.; Yoshida, T.; Kobara, M.; Yamaguchi, T.; Watanabe, N.; Shimizu, J.; Horio, Y.; Kuroda, H.; Sakao, Y.; et al. Efficacy and Safety Data of Osimertinib in Elderly Patients with NSCLC Who Harbor the EGFR T790M Mutation After Failure of Initial EGFR-TKI. Treat. Anticancer Res. 2018, 38, 5231–5237. [Google Scholar] [CrossRef] [PubMed]
- Brueckl, W.M.; Achenbach, H.J.; Ficker, J.H.; Schuette, W. Erlotinib treatment after platinum-based therapy in elderly patients with non-small-cell lung cancer in routine clinical practice—Results from the ElderTac study. BMC Cancer 2018, 18, 333. [Google Scholar] [CrossRef] [PubMed]
- Corre, R.; Gervais, R.; Guisier, F.; Tassy, L.; Vinas, F.; Lamy, R.; Fraboulet, G.; Greillier, L.; Doubre, H.; Descourt, R.; et al. Octogenarians with EGFR-mutated non-small cell lung cancer treated by tyrosine-kinase inhibitor: A multicentric real-world study assessing tolerance and efficacy (OCTOMUT study). Oncotarget 2018, 9, 8253–8262. [Google Scholar] [CrossRef]
- Casaluce, F.; Sgambato, A.; Maione, P.; Spagnuolo, A.; Gridelli, C. Lung cancer, elderly and immune checkpoint inhibitors. J. Thorac. Dis. 2018, 10, S1474–S1481. [Google Scholar] [CrossRef]
- Gomes, F.; Woolley, S.; Califano, R.; Summers, Y.; Baker, K.; Burns, K.; Yorke, J.; Blackhall, F. MA 10.07 Elderly Lung Cancer Patients on Immunotherapy: Preliminary Results from the ELDERS Study. J. Thorac. Oncol. 2017, 12, S1841–S1842. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age | Median (Range) |
|---|---|
| ≥80 years old | 82 (80–92) |
| Gender | n (%) |
| Male | 58 (76.3%) |
| Female | 18 (23.7%) |
| Histology | n (%) |
| Adenocarcinoma | 66 (86.8%) |
| Adenosquamous carcinoma | 2 (2.6%) |
| Non-squamous NSCLC | 8 (10.6%) |
| Smoking Habit | n (%) |
| Smokers | 6 (7.9%) |
| Recent ex-smokers | 14 (18.4%) |
| Long-term ex-smokers | 16 (21.1%) |
| Never-smokers | 18 (23.7%) |
| NA | 22 (28.9%) |
| Performance Status (PS) | n (%) |
| PS = 0 | 1 (1.3%) |
| PS = 1 | 20 (26.3%) |
| PS = 2 | 11 (14.5%) |
| PS > 2 | 5 (6.6%) |
| NA | 39 (51.3) |
| Treatment Regimens | n (%) |
| Chemotherapy | 13 (17%) |
| Tyrosine kinase inhibitor | 10 (13.2%) |
| Radiotherapy and/or best supportive care | 10 (13.2%) |
| NA | 43 (56.6%) |
| Gene (No. of cases tested = 76) | n (No. of cases) |
| EGFR mutation | 18 |
| ALK rearrangement | 0 |
| ROS1 rearrangement | 2 |
| KRAS mutation | 20 |
| MET mutation/amplification | 9 |
| BRAF mutation | 4 |
| ERBB2 mutation | 3 |
| Alterations in other genes | 22 |
| All genes wild-type | 10 |
| PD-L1 IHC (N. of cases tested = 22) | n |
| TPS < 1% | 5 |
| TPS = 1%–49% | 7 |
| TPS > 50% | 10 |
| Patient # | Mutational Status | PD-L1 TPS | Performance Status | Treatment |
|---|---|---|---|---|
| 1 | EGFR p.Glu746_Ala750del EGFR p.Thr790Met | >50% | PS 0 | TKIs—Gefitinib and Osimertinib |
| 2 | EGFR p.Glu746_Ala750del MET amplified | >50% | PS 1 | TKI—Gefitinib |
| 3 | EGFR p.Leu858Arg EGFR p.Thr790Met TP53 p.Asn131Tyr | 1%–49% | PS 1 | TKI—Osimertinib |
| 4 | EGFR p.Leu858Arg TP53 p.Pro80Ser | NA | PS 1 | TKI—Gefitinib |
| 5 | EGFR p.Leu858Arg | NA | PS 2 | TKI—Gefitinib |
| 6 | EGFR p.Glu746_Ala750del | 1%–49% | PS 1 | TKI—Gefitinib |
| 7 | EGFR p.Leu858Arg | NA | PS 1 | TKI—Gefitinib |
| 8 | EGFR p.Glu746_Thr752delinsAla EGFR p.Thr790Met TP53 p.Cys176Tyr SMAD4 p.Phe354Leu | NA | PS 1 | TKIs—Erlotinib and Osimertinib |
| 9 | EGFR p.Leu858Arg TP53 p.Val157Phe STK11 p.Phe354Leu | NA | PS 1 | TKI—Gefitinib |
| 10 | EGFR p.Glu746_Ala750del EGFR p.Thr790Met | NA | PS 1 | TKIs—Erlotinib and Osimertinib |
| 11 | WT | NA | PS 1 | Chemotherapy—Vinorelbine |
| 12 | WT | <1% | PS 2 | Chemotherapy—Combination regimens * |
| 13 | WT | <1% | PS 1 | Chemotherapy—Vinorelbine |
| 14 | KRAS p.Gly12Val | <1% | PS 2 | Chemotherapy—Vinorelbine |
| 15 | TP53 p.Asn131Tyr | NA | PS 1 | Chemotherapy—Vinorelbine |
| 16 | SMAD4 p.Gln256Leu | NA | PS 1 | Chemotherapy—Combination regimens * |
| 17 | PIK3CA p.Glu545Lys | NA | PS 1 | Chemotherapy—Vinorelbine |
| 18 | KRAS p.Gly12Cys PIK3CA p.Glu545Lys | NA | PS 2 | Chemotherapy—Vinorelbine |
| 19 | KRAS p.Gly12Cys TP53 Glu349Ter | <1% | PS 2 | Chemotherapy—Vinorelbine |
| 20 | KRAS p.Gly12Asp TP53 p.Val216Met | 1%–49% | PS 1 | Chemotherapy—Vinorelbine |
| 21 | KRAS p.Gly12Val STK11 p.Asp194Tyr | NA | PS 2 | Chemotherapy—Vinorelbine |
| 22 | KRAS p.Gly13Cys STK11 p.Arg331Trp | >50% | PS 2 | Chemotherapy—Vinorelbine |
| 23 | TP53 p.Gys275Phe ERBB2 p.Ile767Met | NA | PS 1 | Chemotherapy—Combination regimens * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fumagalli, C.; Catania, C.; Ranghiero, A.; Bosi, C.; Viale, G.; de Marinis, F.; Barberis, M.; Guerini-Rocco, E. Molecular Profile of Advanced Non-Small Cell Lung Cancers in Octogenarians: The Door to Precision Medicine in Elderly Patients. J. Clin. Med. 2019, 8, 112. https://doi.org/10.3390/jcm8010112
Fumagalli C, Catania C, Ranghiero A, Bosi C, Viale G, de Marinis F, Barberis M, Guerini-Rocco E. Molecular Profile of Advanced Non-Small Cell Lung Cancers in Octogenarians: The Door to Precision Medicine in Elderly Patients. Journal of Clinical Medicine. 2019; 8(1):112. https://doi.org/10.3390/jcm8010112
Chicago/Turabian StyleFumagalli, Caterina, Chiara Catania, Alberto Ranghiero, Carlo Bosi, Giuseppe Viale, Filippo de Marinis, Massimo Barberis, and Elena Guerini-Rocco. 2019. "Molecular Profile of Advanced Non-Small Cell Lung Cancers in Octogenarians: The Door to Precision Medicine in Elderly Patients" Journal of Clinical Medicine 8, no. 1: 112. https://doi.org/10.3390/jcm8010112