
Determination of Relative Weightings for Sacroiliac Joint Pathologies in the OMERACT Juvenile Arthritis Magnetic Resonance Imaging Sacroiliac Joint Score
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
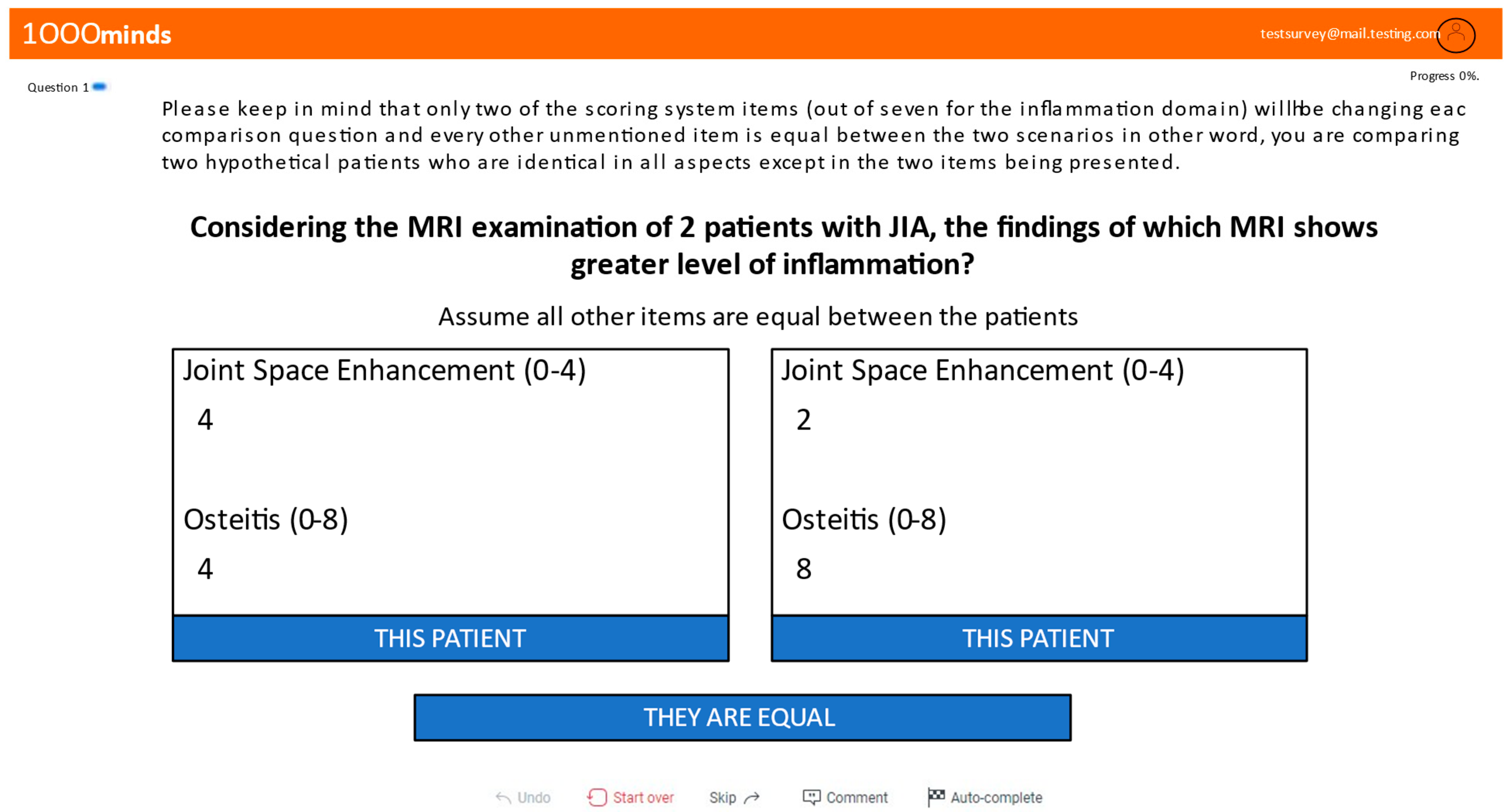
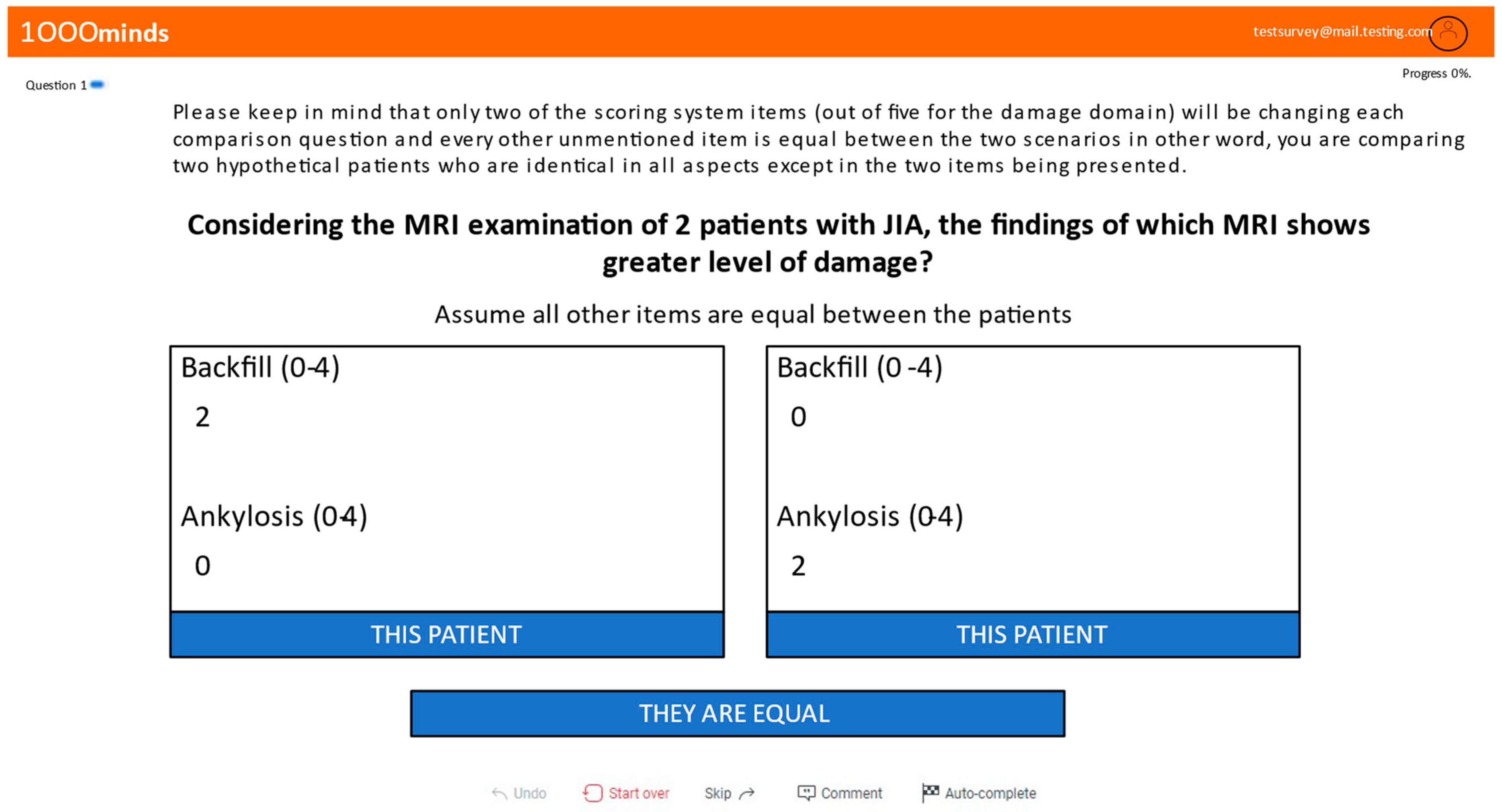
2.1. Conjoint Analysis Survey
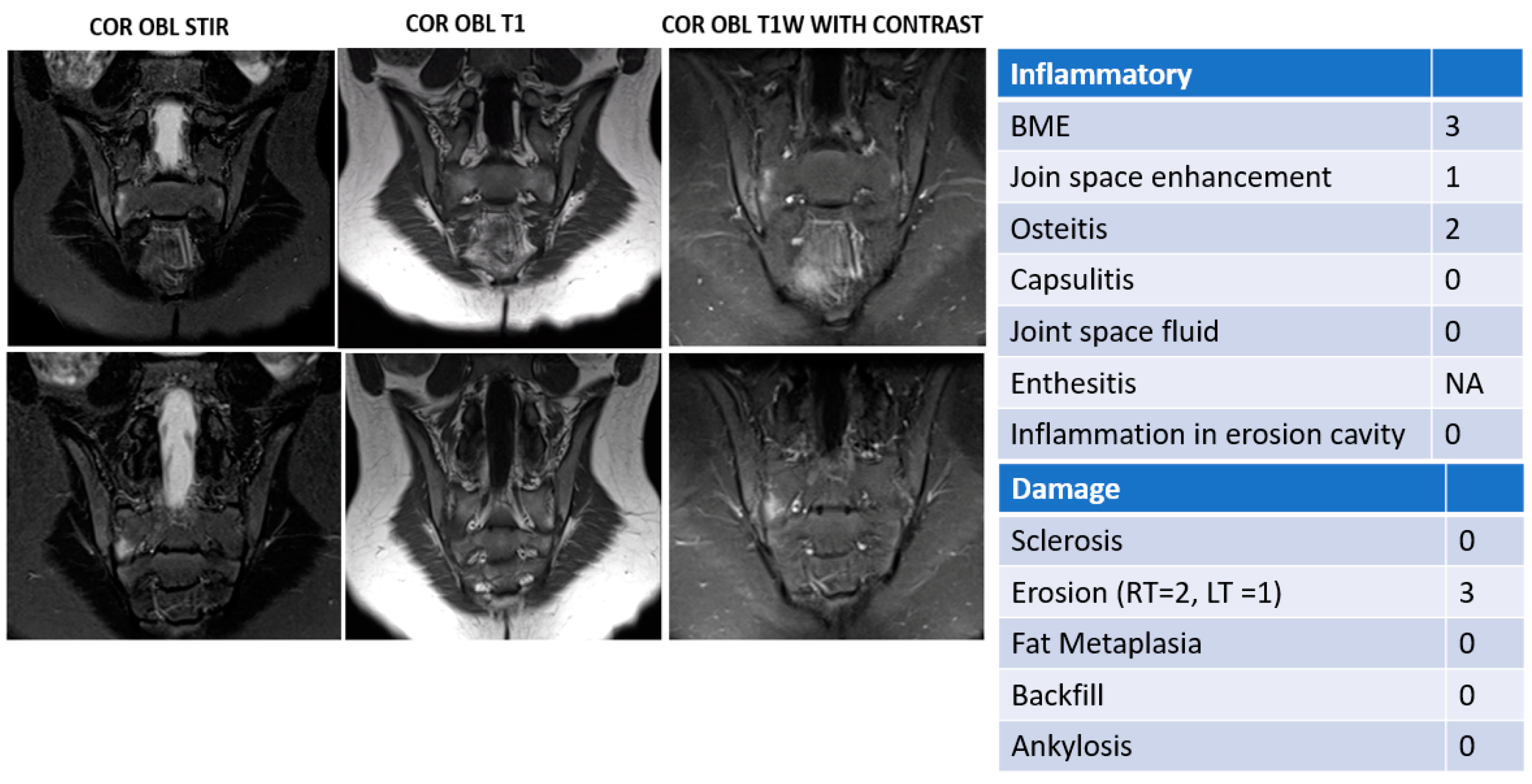
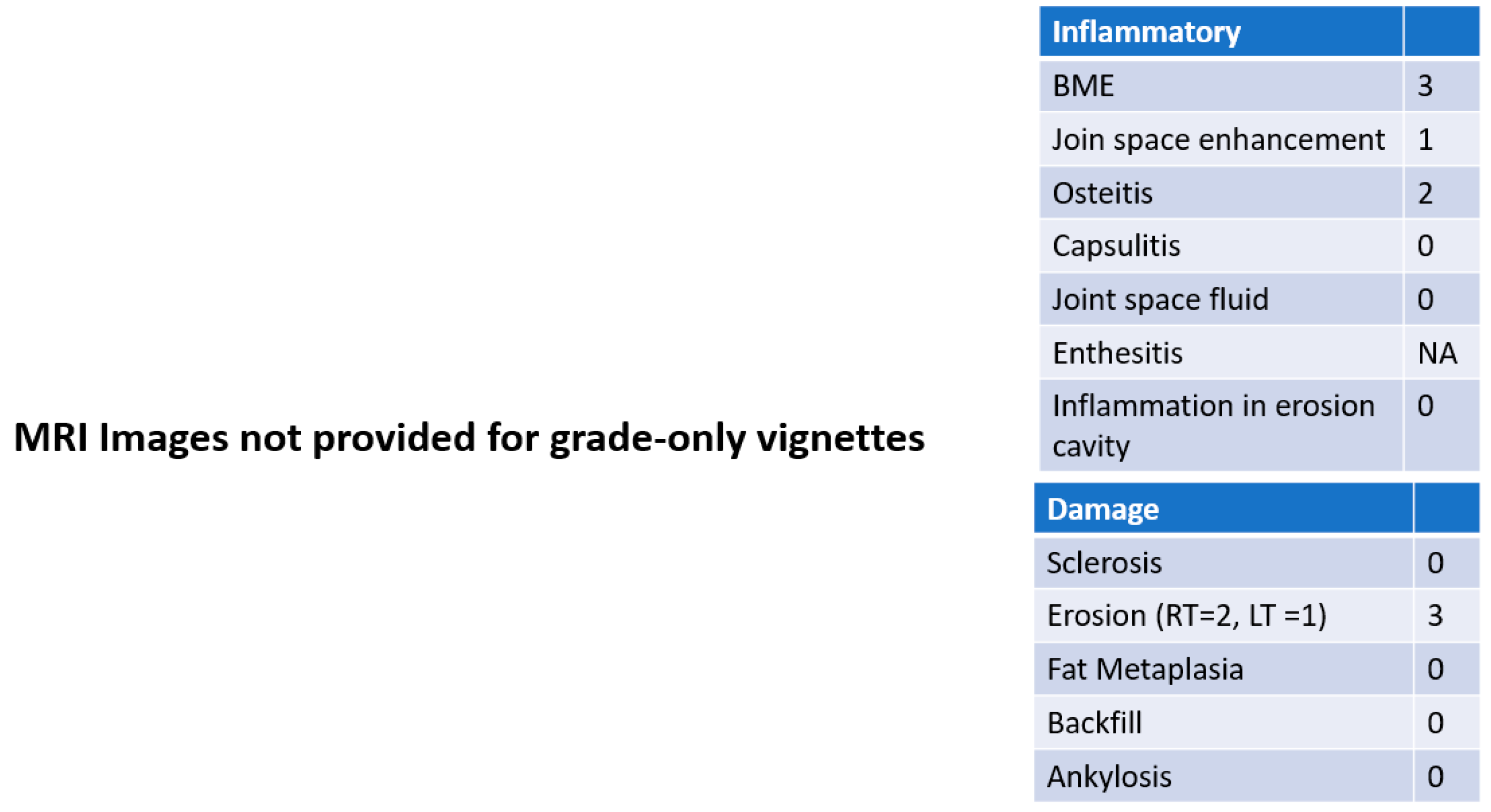
2.2. JAMRIS-SIJ Vignette Ranking Exercise
2.3. Statistical Analysis
3. Result
3.1. Summary of Survey Items
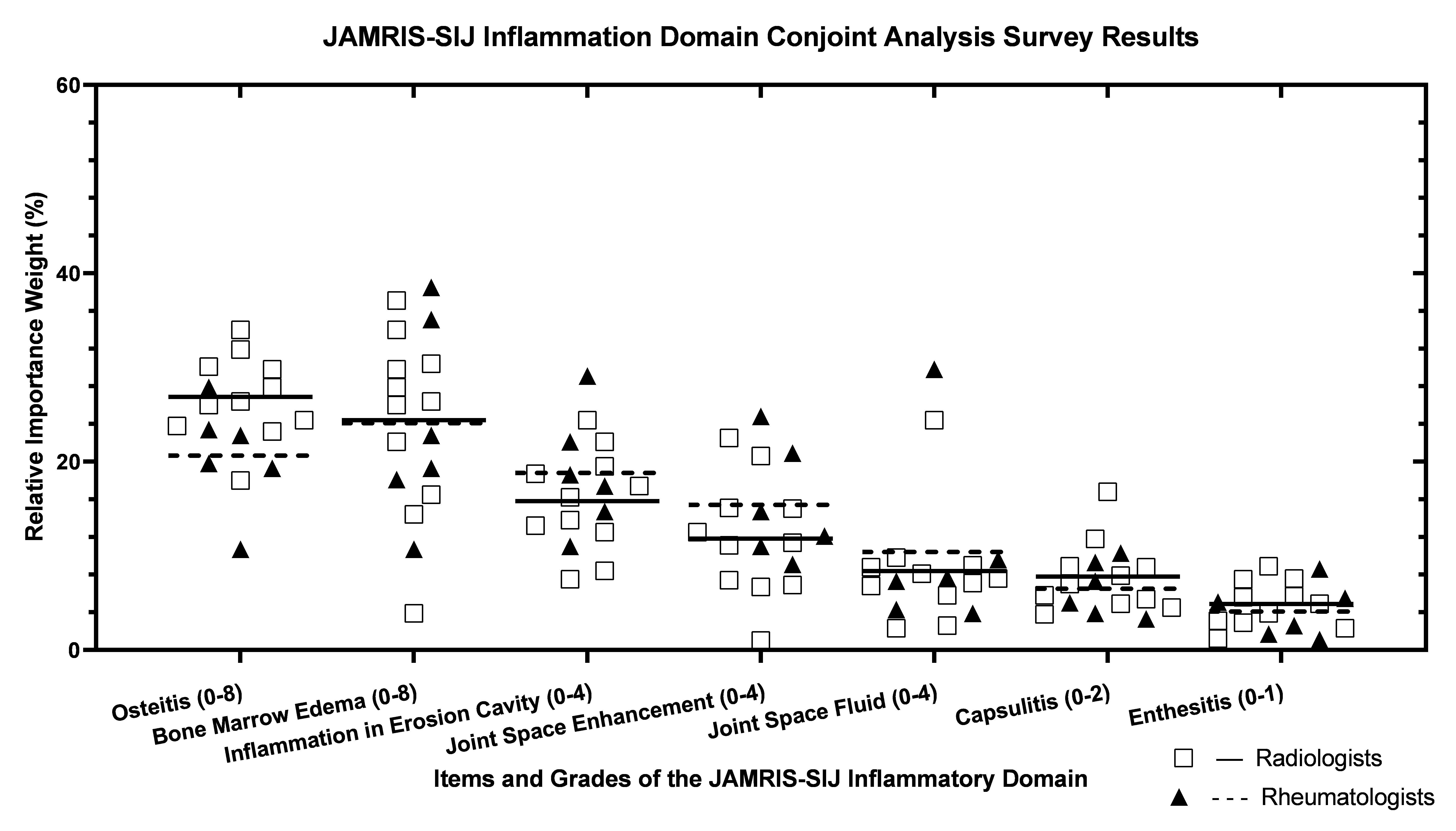
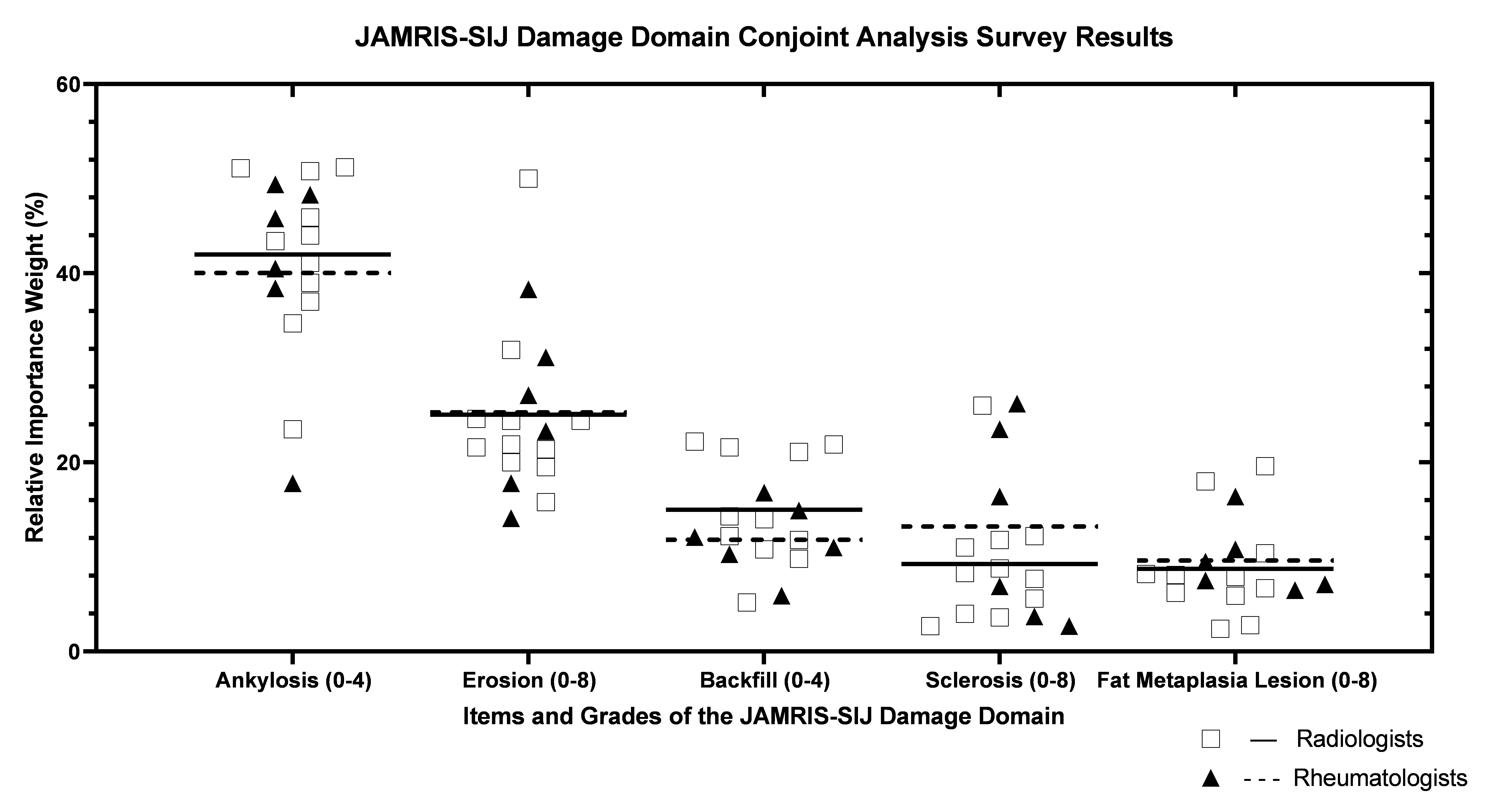
3.2. Conjoint Analysis Survey-Derived Relative JAMRIS-SIJ Weights
3.3. Concordance of Conjoint Analysis Survey-Derived JAMRIS-SIJ Weights among Experts
3.4. Homogeneity of Vignette Rankings (by Conjoint Analysis Survey (CAS) Score and by Explicit Expert Rank)
3.5. Correlation of JAMRIS-SIJ Vignette Ranking by MRI +/− Grade versus CAS Generated JAMRIS-SIJ Weights
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


Appendix B


References
- Martini, A.; Ravelli, A.; Avcin, T.; Beresford, M.W.; Burgos-Vargas, R.; Cuttica, R.; Ilowite, N.T.; Khubchandani, R.; Laxer, R.M.; Lovell, D.J.; et al. Toward New Classification Criteria for Juvenile Idiopathic Arthritis: First Steps, Pediatric Rheumatology International Trials Organization International Consensus. J. Rheumatol. 2019, 46, 190–197. [Google Scholar] [CrossRef] [Green Version]
- Bernatsky, S.; Duffy, C.; Malleson, P.; Feldman, D.E.; St Pierre, Y.; Clarke, A.E. Economic impact of juvenile idiopathic arthritis. Arthritis Rheum. 2007, 57, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Manners, P.J.; Bower, C. Worldwide prevalence of juvenile arthritis why does it vary so much? J. Rheumatol. 2002, 29, 1520–1530. [Google Scholar]
- Telli, H.; Telli, S.; Topal, M. The Validity and Reliability of Provocation Tests in the Diagnosis of Sacroiliac Joint Dysfunction. Pain Physician 2018, 21, E367–E376. [Google Scholar] [CrossRef]
- Vleeming, A.; Schuenke, M.D.; Masi, A.T.; Carreiro, J.E.; Danneels, L.; Willard, F.H. The sacroiliac joint: An overview of its anatomy, function and potential clinical implications. J. Anat. 2012, 221, 537–567. [Google Scholar] [CrossRef]
- Herregods, N.; Dehoorne, J.; Joos, R.; Jaremko, J.L.; Baraliakos, X.; Leus, A.; Van den Bosch, F.; Verstraete, K.; Jans, L. Diagnostic value of MRI features of sacroiliitis in juvenile spondyloarthritis. Clin. Radiol. 2015, 70, 1428–1438. [Google Scholar] [CrossRef]
- Jaremko, J.L.; Liu, L.; Winn, N.J.; Ellsworth, J.E.; Lambert, R.G. Diagnostic utility of magnetic resonance imaging and radiography in juvenile spondyloarthritis: Evaluation of the sacroiliac joints in controls and affected subjects. J. Rheumatol. 2014, 41, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Sieper, J.; Rudwaleit, M.; Baraliakos, X.; Brandt, J.; Braun, J.; Burgos-Vargas, R.; Dougados, M.; Hermann, K.G.; Landewe, R.; Maksymowych, W.; et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: A guide to assess spondyloarthritis. Ann. Rheum. Dis. 2009, 68 (Suppl. S2), ii1–ii44. [Google Scholar] [CrossRef]
- Otobo, T.M.; Conaghan, P.G.; Maksymowych, W.P.; van der Heijde, D.; Weiss, P.; Sudol-Szopinska, I.; Herregods, N.; Jaremko, J.L.; Meyers, A.B.; Rumsey, D.; et al. Preliminary Definitions for Sacroiliac Joint Pathologies in the OMERACT Juvenile Idiopathic Arthritis Magnetic Resonance Imaging Score (OMERACT JAMRIS-SIJ). J. Rheumatol. 2019, 46, 1192–1197. [Google Scholar] [CrossRef]
- Kirshner, B.; Guyatt, G. A methodological framework for assessing health indices. J. Chronic Dis. 1985, 38, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.; Farrar, S. Using conjoint analysis to elicit preferences for health care. BMJ 2000, 320, 1530–1533. [Google Scholar] [CrossRef] [Green Version]
- McMillan, J. Priority Setting and the Public. J. Med. Ethics 2002, 28, 59. [Google Scholar] [CrossRef] [Green Version]
- Hansen, P.; Ombler, F. A new method for scoring additive multi-attribute value models using pairwise rankings of alternatives. J. Multi-Criteria Decis. Anal. 2008, 15, 87–107. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Otobo, T.M.; Herregods, N.; Jaremko, J.L.; Lambert, R.G.; Sudoł-Szopińska, I.; Meyers, A.B.; Kirkhus, E.; Weiss, P.; Tse, S.M.; Appenzeller, S.; et al. Pos1323 Sacroiliac Joint Mri Abnormalities in Juvenile Spondyloarthritis: An Update of Definitions AND Scoring of the Omeract Juvenile Idiopathic Arthritis Mri Score. Ann. Rheum. Dis. 2021, 80, 943–944. [Google Scholar] [CrossRef]
- Tolend, M.; Junhasavasdikul, T.; Cron, R.Q.; Inarejos Clemente, E.J.; von Kalle, T.; Kellenberger, C.J.; Koos, B.; Miller, E.; van Rossum, M.A.; Saurenmann, R.K.; et al. Discrete Choice Experiment on a Magnetic Resonance Imaging Scoring System for Temporomandibular Joints in Juvenile Idiopathic Arthritis. Arthritis Care Res. 2022, 74, 308–316. [Google Scholar] [CrossRef]
- Cellucci, T.; Guzman, J.; Petty, R.E.; Batthish, M.; Benseler, S.M.; Ellsworth, J.E.; Houghton, K.M.; Le, B.C.; Huber, A.M.; Luca, N.; et al. Management of Juvenile Idiopathic Arthritis 2015: A Position Statement from the Pediatric Committee of the Canadian Rheumatology Association. J. Rheumatol. 2016, 43, 1773–1776. [Google Scholar] [CrossRef] [PubMed]
- Collidge, T.A.; Thomson, P.C.; Mark, P.B.; Traynor, J.P.; Jardine, A.G.; Morris, S.T.; Simpson, K.; Roditi, G.H. Gadolinium-enhanced MR imaging and nephrogenic systemic fibrosis: Retrospective study of a renal replacement therapy cohort. Radiology 2007, 245, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Ranga, A.; Agarwal, Y.; Garg, K.J. Gadolinium based contrast agents in current practice: Risks of accumulation and toxicity in patients with normal renal function. Indian J. Radiol. Imaging 2017, 27, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Herregods, N.; Jans, L.B.O.; Chen, M.; Paschke, J.; De Buyser, S.L.; Renson, T.; Dehoorne, J.; Joos, R.; Lambert, R.G.W.; Jaremko, J.L. Normal subchondral high T2 signal on MRI mimicking sacroiliitis in children: Frequency, age distribution, and relationship to skeletal maturity. Eur. Radiol. 2020, 31, 3498–3507. [Google Scholar] [CrossRef]
- Colebatch-Bourn, A.N.; Edwards, C.J.; Collado, P.; D’Agostino, M.A.; Hemke, R.; Jousse-Joulin, S.; Maas, M.; Martini, A.; Naredo, E.; Ostergaard, M.; et al. EULAR-PReS points to consider for the use of imaging in the diagnosis and management of juvenile idiopathic arthritis in clinical practice. Ann. Rheum. Dis. 2015, 74, 1946–1957. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inflammation Domain | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Grades | |||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ICC (2,1) | ICC (2,k) | |
| Osteitis | 0 | 3.9 | 7.7 | 11.2 | 14.4 | 17.2 | 19.8 | 23.3 | 24.7 | 0.66 | 0.97 |
| BME | 0 | 3.2 | 6.4 | 9.5 | 12.6 | 15.6 | 18.5 | 21.4 | 24.3 | 0.59 | 0.96 |
| IEC | 0 | 5.3 | 10 | 13.7 | 16.9 | -- | -- | -- | -- | 0.52 | 0.95 |
| JSE | 0 | 4.5 | 8.2 | 10.9 | 13.1 | -- | -- | -- | -- | 0.34 | 0.90 |
| JSF | 0 | 2.8 | 5.1 | 7.1 | 9.1 | -- | -- | -- | -- | 0.17 | 0.78 |
| Capsulitis | 0 | 3.9 | 7.3 | -- | -- | -- | -- | -- | -- | 0.41 | 0.92 |
| Enthesitis | 0 | 4.6 | -- | -- | -- | -- | -- | -- | -- | 0.76 | 0.98 |
| All Items | -- | -- | -- | -- | -- | -- | -- | -- | -- | 0.60 | 0.96 |
| Damage Domain | |||||||||||
| Grades | |||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ICC (2,1) | ICC (2,k) | |
| Ankylosis | 0 | 10 | 20.2 | 30.7 | 41.3 | 0.79 | 0.98 | ||||
| Erosion | 0 | 3.7 | 7.2 | 10.6 | 13.9 | 16.9 | 19.8 | 22.5 | 25.1 | 0.60 | 0.96 |
| Backfill | 0 | 3.9 | 7.5 | 10.8 | 13.9 | 0.59 | 0.96 | ||||
| Sclerosis | 0 | 1.8 | 3.6 | 55.2 | 6.6 | 7.8 | 8.9 | 9.8 | 10.7 | 0.23 | 0.83 |
| FML | 0 | 1.6 | 3.1 | 4.5 | 5.7 | 6.6 | 7.5 | 8.3 | 9.1 | 0.33 | 0.90 |
| All Items | 0.73 | 0.98 | |||||||||
| Spearman Correlation Coefficient of CAS-Weighted JAMRIS-SIJ vs. Graded ± Image Vignette Ranking | |||||
|---|---|---|---|---|---|
| Vignette Type | Expert Cohort | Inflammation Domain | Damage Domain | ||
| Median | IQR | Median | IQR | ||
| Grade only | All experts (n = 17) | 0.84 | 0.80–0.94 | 0.93 | 0.90–0.96 |
| Rheumatologists (n = 6) | 0.89 | 0.82–0.97 | 0.92 | 0.88–0.95 | |
| Radiologists (n = 11) | 0.82 | 0.73–0.93 | 0.94 | 0.91–0.97 | |
| Grade + Image | Radiologists (n = 10) Rheumatologist (n = 2) | 0.74 | 0.55–0.85 | 0.93 | 0.81–0.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otobo, T.M.; Tolend, M.; Meyers, A.B.; Sudol-Szopinska, I.; Joshi, S.; Stimec, J.; Herregods, N.; Jaremko, J.L.; Tse, S.M.L.; Haroon, N.; et al. Determination of Relative Weightings for Sacroiliac Joint Pathologies in the OMERACT Juvenile Arthritis Magnetic Resonance Imaging Sacroiliac Joint Score. J. Clin. Med. 2023, 12, 2729. https://doi.org/10.3390/jcm12072729
Otobo TM, Tolend M, Meyers AB, Sudol-Szopinska I, Joshi S, Stimec J, Herregods N, Jaremko JL, Tse SML, Haroon N, et al. Determination of Relative Weightings for Sacroiliac Joint Pathologies in the OMERACT Juvenile Arthritis Magnetic Resonance Imaging Sacroiliac Joint Score. Journal of Clinical Medicine. 2023; 12(7):2729. https://doi.org/10.3390/jcm12072729
Chicago/Turabian StyleOtobo, Tarimobo M., Mirkamal Tolend, Arthur B. Meyers, Iwona Sudol-Szopinska, Sayali Joshi, Jennifer Stimec, Nele Herregods, Jacob L. Jaremko, Shirley M. L. Tse, Nigil Haroon, and et al. 2023. "Determination of Relative Weightings for Sacroiliac Joint Pathologies in the OMERACT Juvenile Arthritis Magnetic Resonance Imaging Sacroiliac Joint Score" Journal of Clinical Medicine 12, no. 7: 2729. https://doi.org/10.3390/jcm12072729