
Electrical Storm Has Worse Prognosis Compared to Sustained Ventricular Tachycardia after VT Ablation
 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Electrophysiological Study
2.3. Image Integration of Pre-Procedural Cardiac MRI or CTs
2.4. Post-Ablation Management
2.5. Prognostic Study Endpoints
2.6. Statistical Methods
3. Results
3.1. Baseline Characteristics
3.2. Catheter Ablation and Acute Procedural Outcomes
3.3. Predictors of Acute Ablation Success
3.4. Adverse Events during Ablation Procedure
3.5. Long-Term Success Rate and Cardiovascular Mortality
3.6. Propensity Score-Matched Cohort
4. Discussion
4.1. Electrical Storm and Mortality
4.2. Electrical Storm and VT Ablation
4.3. Value of Programmed Electrical Stimulation after VT Ablation in ES Patients
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pedersen, C.T.; Kay, G.N.; Kalman, J.; Borggrefe, M.; Della-Bella, P.; Dickfeld, T.; Dorian, P.; Huikuri, H.; Kim, Y.H.; Knight, B.; et al. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm 2014, 11, e166–e196. [Google Scholar] [CrossRef]
- Villacastin, J.; Almendral, J.; Arenal, A.; Albertos, J.; Ormaetxe, J.; Peinado, R.; Bueno, H.; Merino, J.L.; Pastor, A.; Medina, O.; et al. Incidence and clinical significance of multiple consecutive, appropriate, high-energy discharges in patients with implanted cardioverter-defibrillators. Circulation 1996, 93, 753–762. [Google Scholar] [CrossRef]
- Credner, S.C.; Klingenheben, T.; Mauss, O.; Sticherling, C.; Hohnloser, S.H. Electrical storm in patients with transvenous implantable cardioverter-defibrillators: Incidence, management and prognostic implications. J. Am. Coll. Cardiol. 1998, 32, 1909–1915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, A.; Kilicaslan, F.; Marrouche, N.F.; Minor, S.; Khan, M.; Wazni, O.; Burkhardt, J.D.; Belden, W.A.; Cummings, J.E.; Abdul-Karim, A.; et al. Prevalence, predictors, and mortality significance of the causative arrhythmia in patients with electrical storm. J. Cardiovasc. Electrophysiol. 2004, 15, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Israel, C.W.; Barold, S.S. Electrical storm in patients with an implanted defibrillator: A matter of definition. Ann. Noninvasive Electrocardiol. 2007, 12, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Israel, C.W.; Manegold, J.C. Electrical storm: Definition, prevalence, causes and prognostic implications. Herzschrittmachertherapie + Elektrophysiologie 2014, 25, 59–65. [Google Scholar] [CrossRef]
- Priori, S.G.; Blomstrom-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar] [CrossRef] [Green Version]
- Muser, D.; Liang, J.J.; Pathak, R.K.; Magnani, S.; Castro, S.A.; Hayashi, T.; Garcia, F.C.; Supple, G.E.; Riley, M.P.; Lin, D.; et al. Long-Term Outcomes of Catheter Ablation of Electrical Storm in Nonischemic Dilated Cardiomyopathy Compared With Ischemic Cardiomyopathy. JACC Clin. Electrophysiol. 2017, 3, 767–778. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Marchlinski, F.E.; Callans, D.J.; Gottlieb, C.D.; Zado, E. Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation 2000, 101, 1288–1296. [Google Scholar] [CrossRef] [Green Version]
- Jaïs, P.; Maury, P.; Khairy, P.; Sacher, F.; Nault, I.; Komatsu, Y.; Hocini, M.; Forclaz, A.; Jadidi, A.S.; Weerasooryia, R.; et al. Elimination of local abnormal ventricular activities: A new end point for substrate modification in patients with scar-related ventricular tachycardia. Circulation 2012, 125, 2184–2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sosa, E.; Scanavacca, M.; d’Avila, A.; Pilleggi, F. A new technique to perform epicardial mapping in the electrophysiology laboratory. J. Cardiovasc. Electrophysiol. 1996, 7, 531–536. [Google Scholar] [CrossRef]
- Bansch, D.; Bocker, D.; Brunn, J.; Weber, M.; Breithardt, G.; Block, M. Clusters of ventricular tachycardias signify impaired survival in patients with idiopathic dilated cardiomyopathy and implantable cardioverter defibrillators. J. Am. Coll. Cardiol. 2000, 36, 566–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behnes, M.; Müller, J.; Ellguth, D.; Schupp, T.; Taton, G.; Reiser, L.; Engelke, N.; Reichelt, T.; Bollow, A.; Kim, S.H.; et al. Electrical storm is associated with impaired prognosis compared to ventricular tachyarrhythmias. Int. J. Cardiol. 2019, 292, 119–125. [Google Scholar] [CrossRef]
- Vergara, P.; Tung, R.; Vaseghi, M.; Brombin, C.; Frankel, D.S.; Di Biase, L.; Nagashima, K.; Tedrow, U.; Tzou, W.S.; Sauer, W.H.; et al. Successful ventricular tachycardia ablation in patients with electrical storm reduces recurrences and improves survival. Heart Rhythm 2018, 15, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Guerra, F.; Shkoza, M.; Scappini, L.; Flori, M.; Capucci, A. Role of electrical storm as a mortality and morbidity risk factor and its clinical predictors: A meta-analysis. Europace 2014, 16, 347–353. [Google Scholar] [CrossRef]
- Pires, L.A.; Lehmann, M.H.; Steinman, R.T.; Baga, J.J.; Schuger, C.D. Sudden death in implantable cardioverter-defibrillator recipients: Clinical context, arrhythmic events and device responses. J. Am. Coll. Cardiol. 1999, 33, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, M.O.; Sherfesee, L.; DeGroot, P.J.; Wathen, M.S.; Wilkoff, B.L. Differences in effects of electrical therapy type for ventricular arrhythmias on mortality in implantable cardioverter-defibrillator patients. Heart Rhythm 2010, 7, 353–360. [Google Scholar] [CrossRef]
- Carbucicchio, C.; Santamaria, M.; Trevisi, N.; Maccabelli, G.; Giraldi, F.; Fassini, G.; Riva, S.; Moltrasio, M.; Cireddu, M.; Veglia, F.; et al. Catheter ablation for the treatment of electrical storm in patients with implantable cardioverter-defibrillators: Short- and long-term outcomes in a prospective single-center study. Circulation 2008, 117, 462–469. [Google Scholar] [CrossRef] [Green Version]
- Kozeluhova, M.; Peichl, P.; Cihak, R.; Wichterle, D.; Vancura, V.; Bytesnik, J.; Kautzner, J. Catheter ablation of electrical storm in patients with structural heart disease. Europace 2011, 13, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Dinov, B.; Fiedler, L.; Schönbauer, R.; Bollmann, A.; Rolf, S.; Piorkowski, C.; Hindricks, G.; Arya, A. Outcomes in catheter ablation of ventricular tachycardia in dilated nonischemic cardiomyopathy compared with ischemic cardiomyopathy: Results from the Prospective Heart Centre of Leipzig VT (HELP-VT) Study. Circulation 2014, 129, 728–736. [Google Scholar] [CrossRef]
- Kumar, S.; Fujii, A.; Kapur, S.; Romero, J.; Mehta, N.K.; Tanigawa, S.; Epstein, L.M.; Koplan, B.A.; Michaud, G.F.; John, R.M.; et al. Beyond the Storm: Comparison of Clinical Factors, Arrhythmogenic Substrate, and Catheter Ablation Outcomes in Structural Heart Disease Patients With versus Those Without a History of Ventricular Tachycardia Storm. J. Cardiovasc. Electrophysiol. 2017, 28, 56–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2018, 138, e272–e391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piers, S.R.; Leong, D.P.; van Huls van Taxis, C.F.; Tayyebi, M.; Trines, S.A.; Pijnappels, D.A.; Delgado, V.; Schalij, M.J.; Zeppenfeld, K. Outcome of ventricular tachycardia ablation in patients with nonischemic cardiomyopathy: The impact of noninducibility. Circ. Arrhythmia Electrophysiol. 2013, 6, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Dinov, B.; Arya, A.; Schratter, A.; Schirripa, V.; Fiedler, L.; Sommer, P.; Bollmann, A.; Rolf, S.; Piorkowski, C.; Hindricks, G. Catheter ablation of ventricular tachycardia and mortality in patients with nonischemic dilated cardiomyopathy: Can noninducibility after ablation be a predictor for reduced mortality? Circ. Arrhythmia Electrophysiol. 2015, 8, 598–605. [Google Scholar] [CrossRef] [Green Version]
- Muser, D.; Hayashi, T.; Castro, S.A.; Supple, G.E.; Schaller, R.D.; Santangeli, P.; Arkles, J.; Kumareswaran, R.; Nazarian, S.; Deo, R.; et al. Noninvasive Programmed Ventricular Stimulation-Guided Management Following Ventricular Tachycardia Ablation. JACC Clin. Electrophysiol. 2019, 5, 719–727. [Google Scholar] [CrossRef]
- Oloriz, T.; Baratto, F.; Trevisi, N.; Barbaro, M.; Bisceglia, C.; D’Angelo, G.; Yamase, M.; Paglino, G.; Radinovic, A.; Della Bella, P. Defining the Outcome of Ventricular Tachycardia Ablation: Timing and Value of Programmed Ventricular Stimulation. Circ. Arrhythmia Electrophysiol. 2018, 11, e005602. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Matching (n = 311) | After Matching (n = 184) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | ES (n = 108; 35%) | Non-ES (n = 203; 65%) | p Value | ES (n = 92; 50%) | Non-ES (n = 92; 50%) | p Value | ||||
| Age, median (range) | 65 ± 14 | 62 ± 15 | 0.165 | 65 ± 13 | 62 ± 14 | 0.279 | ||||
| Males, n (%) | 93 | (86) | 174 | (86) | 0.924 | 79 | (86) | 80 | (87) | 0.830 |
| Cardiovascular risk factors, n (%) | ||||||||||
| Arterial hypertension | 85 | (79) | 159 | (78) | 0.820 | 76 | (84) | 72 | (78) | 0.366 |
| Diabetes mellitus | 33 | (35) | 46 | (23) | 0.056 | 33 | (36) | 25 | (27) | 0.186 |
| Hyperlipidemia | 72 | (67) | 135 | (67) | 0.889 | 62 | (68) | 60 | (65) | 0.676 |
| Smoking | 32 | (30) | 72 | (36) | 0.324 | 28 | (31) | 34 | (37) | 0.377 |
| Cardiac family history | 16 | (15) | 38 | (19) | 0.865 | 14 | (15) | 13 | (14) | 0.811 |
| Comorbidities, n (%) | ||||||||||
| Atrial fibrillation | 47 | (44) | 77 | (38) | 0.338 | 37 | (40) | 36 | (39) | 0.880 |
| Stroke | 11 | (10) | 20 | (10) | 0.905 | 10 | (11) | 9 | (10) | 0.789 |
| Chronic kidney disease | 54 | (51) | 88 | (43) | 0.232 | 44 | (48) | 43 | (47) | 0.827 |
| Liver cirrhosis | 0 | (0) | 7 | (3) | 0.050 | 0 | (0) | 4 | (4) | 0.044 |
| COPD | 3 | (3) | 16 | (8) | 0.061 | 3 | (3) | 7 | (8) | 0.206 |
| Asthma | 0 | (0) | 3 | (2) | 0.279 | 0 | (0) | 1 | (1) | 0.319 |
| Structural heart disease, n (%) | ||||||||||
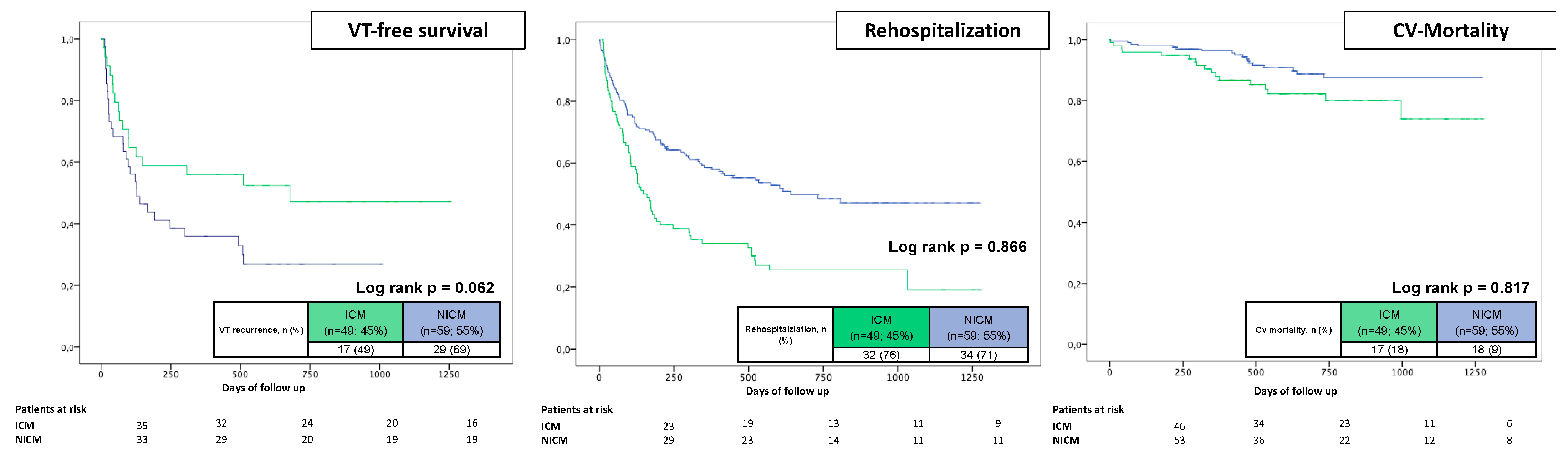
| Ischemic cardiomyopathy | 49 | (45) | 108 | (53) | 0.188 | 46 | (50) | 42 | (46) | 0.555 |
| Dilated cardiomyopathy | 33 | (31) | 35 | (17) | 0.007 | 24 | (26) | 23 | (25) | 0.866 |
| Myocarditis | 13 | (12) | 26 | (13) | 0.845 | 11 | (12) | 13 | (14) | 0.622 |
| Sarcoidosis | 6 | (6) | 9 | (4) | 0.660 | 5 | (5) | 8 | (9) | 0.388 |
| ARVC | 2 | (2) | 8 | (4) | 0.503 | 1 | (1) | 3 | (3) | 0.312 |
| HCM | 2 | (2) | 2 | (2) | 0.432 | 2 | (2) | 1 | (1) | 0.560 |
| HOCM | 2 | (2) | 2 | (2) | 0.432 | 1 | (1) | 0 | (0) | 1.000 |
| EMAH | 0 | (0) | 3 | (2) | 0.277 | - | - | - | - | - |
| Idiopathic | 2 | (2) | 12 | (6) | 0.082 | 1 | (1) | 3 | (3) | 0.312 |
| Cardiac biomarker | ||||||||||
| Potassium (mmol/L) | 4.33 ± 0.56 | 4.48 ± 0.51 | 0.019 | 4.30 ± 0.57 | 4.50 ± 0.49 | 0.014 | ||||
| Troponine (ng/mL) | 0.211 ± 0.546 | 0.190 ± 0.435 | 0.845 | 0.240 ± 0.593 | 0.080 ± 0.173 | 0.068 | ||||
| proBNP (pg/mL) | 2174 ± 1910 | 2048 ± 2150 | 0.707 | 2201 ± 1954 | 1947 ± 1727 | 0.518 | ||||
| Medication at admission, n (%) | ||||||||||
| Beta blocker | 94 | (89) | 181 | (90) | 0.803 | 78 | (87) | 82 | (89) | 0.610 |
| Amiodarone | 57 | (54) | 46 | (23) | 0.001 | 45 | (50) | 27 | (29) | 0.004 |
| Other AAD | 6 | (6) | 2 | (1) | 0.021 | 3 | (3) | 1 | (1) | 0.296 |
| LVEF, % | 33 ± 14 | 39 ± 15 | 0.001 | 34 ± 14 | 36 ± 14 | 0.440 | ||||
| Type of ICD, n (%) | ||||||||||
| ICD | 60 | (57) | 102 | (50) | 0.372 | 49 | (53) | 45 | (49) | 0.555 |
| CRT-D | 27 | (25) | 24 | (12) | 0.003 | 23 | (25) | 15 | (16) | 0.145 |
| s-ICD | 1 | (1) | 4 | (2) | 0.432 | 1 | (1) | 2 | (2) | 0.560 |
| ICD indication, n (%) | ||||||||||
| Primary prevention | 58 | (62) | 105 | (66) | 0.640 | 48 | (61) | 51 | (68) | 0.349 |
| Secondary prevention | 35 | (38) | 54 | (34) | 31 | (39) | 24 | (32) | ||
| Before Matching (n = 311) | After Matching (n = 184) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | ES (n = 108; 35%) | Non-ES (n = 203; 65%) | p Value | ES (n = 92; 50%) | Non-ES (n = 92; 50%) | p Value | ||||
| Preprocedural imaging, n (%) | 39 | (36) | 103 | (51) | 0.137 | 33 | (36) | 43 | (47) | 0.134 |
| MRI, n (%) | 18 | (17) | 34 | (17) | 0.985 | 16 | (17) | 30 | (33) | 0.017 |
| CT, n (%) | 21 | (19) | 69 | (34) | 0.007 | 17 | (19) | 13 | (14) | 0.425 |
| Epicardial ablation, n (%) | 29 | (27) | 26 | (13) | 0.001 | 19 | (21) | 21 | (23) | 0.721 |
| Noninducible with PES, n (%) | 17 | (16) | 56 | (28) | 0.019 | 16 | (17) | 19 | (21) | 0.573 |
| VTs inducible, n/patient | 1.9 ± 1.6 | 1.5 ± 1.5 | 0.033 | 1.8 ± 1.6 | 1.7 ± 1.6 | 0.927 | ||||
| Clinical VT CL, ms | 368 ± 86 | 350 ± 85 | 0.136 | 364 ± 84 | 357 ± 85 | 0.653 | ||||
| Procedural duration, min | 147 ± 44 | 138 ± 49 | 0.094 | 143 ± 40 | 150 ± 53 | 0.354 | ||||
| Fluoroscopy duration, min | 15.3 ± 10.0 | 12.3 ± 8.3 | 0.018 | 13.5 ± 7.6 | 13.4 ± 7.9 | 0.963 | ||||
| Ablation time, min | 31.0 ± 17.5 | 28.8 ± 43.1 | 0.531 | 29.9 ± 16.9 | 35.8 ± 60.9 | 0.387 | ||||
| Partial ablation success, n (%) | 102 | (94) | 194 | (95) | 0.663 | 86 | (94) | 85 | (92) | 0.774 |
| Hemodynamic not tolerated VT, n (%) | 37 | (35) | 43 | (21) | 0.010 | 28 | (30) | 25 | (27) | 0.625 |
| Catecholamine, n (%) | 17 | (16) | 10 | (5) | 0.001 | 14 | (15) | 7 | (8) | 0.105 |
| Intubation, n (%) | 8 | (8) | 2 | (1) | 0.004 | 7 | (8) | 2 | (2) | 0.087 |
| Full ablation success, n (%) | 79 | (76) | 177 | (91) | 0.001 | 77 | (84) | 75 | (82) | 0.697 |
| Beta blocker at discharge, n (%) | 100 | (95) | 191 | (95) | 0.798 | 84 | (94) | 85 | (93) | 0.785 |
| Amiodaron at discharge, n (%) | 43 | (41) | 38 | (19) | 0.001 | 32 | (36) | 26 | (29) | 0.289 |
| Characteristic | ES (n = 108; 35%) | Non-ES (n = 203; 65%) | p Value | ||
|---|---|---|---|---|---|
| Major complications, n (%) | 12 | (11) | 15 | (7) | 0.267 |
| Vascular access-related | 1 | (1) | 2 | (1) | 1.000 |
| Third-degree AV block | 4 | (2) | 5 | (5) | 0.504 |
| Pneumonia | 1 | (1) | 3 | (2) | 1.000 |
| Cardiogenic shock | 3 | (3) | 2 | (1) | 0.346 |
| Pneumothorax | 2 | (2) | 1 | (1) | 0.277 |
| Stroke | 1 | (1) | 1 | (1) | 1.000 |
| In-hospital mortality, n (%) | 2 | (1) | 1 | (1) | 0.277 |
| Before Matching (n = 311) | After Matching (n = 184) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | ES (n = 108; 35%) | Non-ES (n = 203; 65%) | p Value | ES (n = 92; 50%) | Non-ES (n = 92; 50%) | p Value | ||||
| Primary endpoint, n (%) | ||||||||||
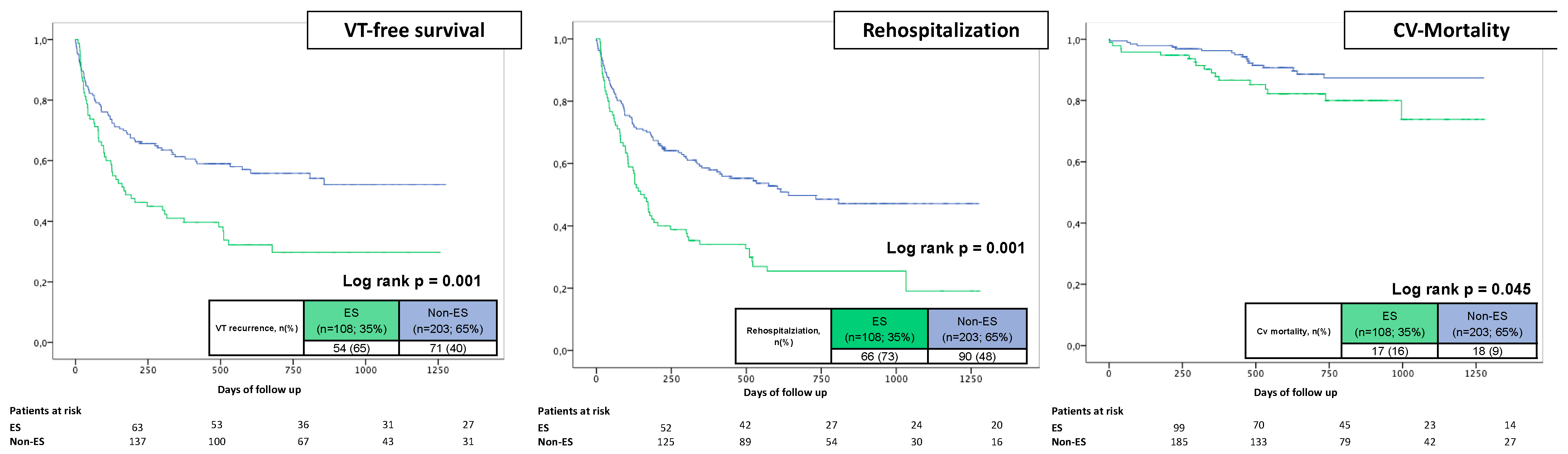
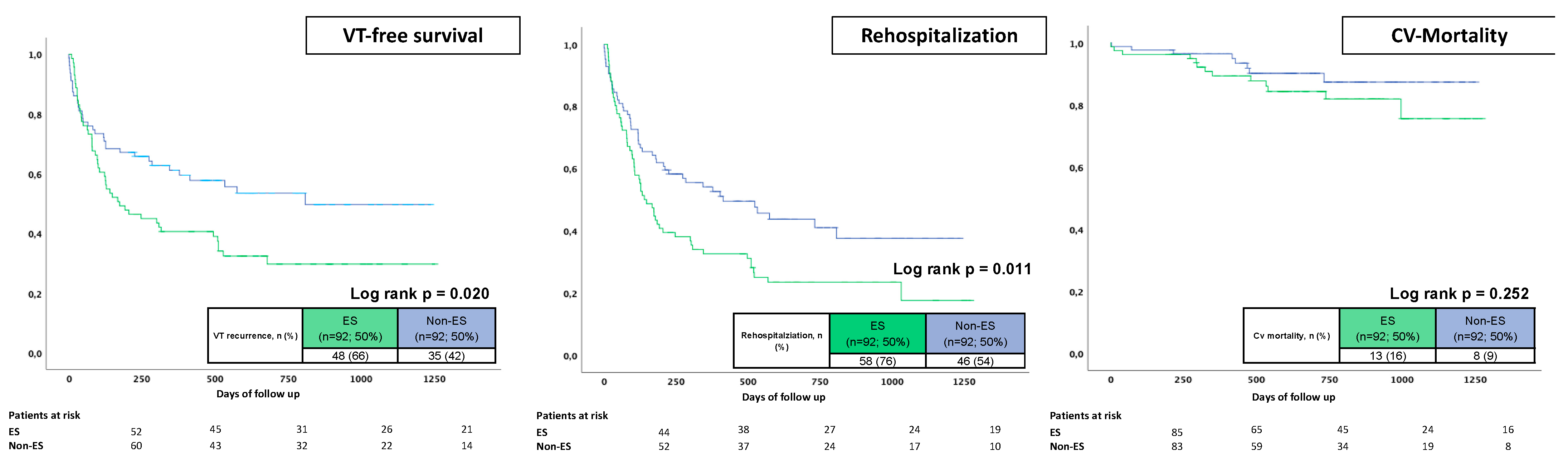
| VT recurrence | 54 | (65) | 71 | (40) | 0.001 | 48 | (66) | 35 | (42) | 0.003 |
| Secondary endpoints, n (%) | ||||||||||
| First rehospitalization, overall | 66 | (73) | 90 | (48) | 0.001 | 58 | (76) | 46 | (54) | 0.003 |
| VT | 49 | (54) | 62 | (32) | 0.001 | 44 | (54) | 32 | (38) | 0.037 |
| Acute heart failure | 12 | (13) | 23 | (12) | 0.954 | 10 | (13) | 11 | (12) | 0.885 |
| Acute myocardial infarction | 3 | (3) | 0 | (0) | 0.041 | 3 | (4) | 0 | (0) | 0.116 |
| Stroke | 0 | (0) | 3 | (2) | 0.554 | 0 | (0) | 2 | (2) | 0.497 |
| LVAD/HTX | 2 | (2) | 1 | (1) | 0.277 | 1 | (1) | 1 | (1) | 0.979 |
| Cardiovascular mortality | 17 | (18) | 18 | (9) | 0.040 | 13 | (16) | 8 | (9) | 0.178 |
| (A) | Univariable | Multivariable | ||||
| Variable | HR | 95% CI | p Value | HR | 95% CI | p Value |
| Age | 1.002 | 0.990–1.015 | 0.716 | - | - | - |
| Epicardial ablation | 1.343 | 0.866–2.083 | 0.188 | - | - | - |
| Any VT inducible | 1.912 | 1.235–2.961 | 0.004 | 1.590 | 1.016–2.488 | 0.042 |
| Clinical VT inducible | 1.266 | 0.590–2.719 | 0.545 | - | - | - |
| LVEF | 1.006 | 1.004–1.132 | 0.298 | - | - | - |
| DCM | 1.953 | 1.324–2.883 | 0.001 | 1.808 | 1.207–2.709 | 0.004 |
| Beta blocker at discharge | 0.938 | 0.437–2.011 | 0.869 | - | - | - |
| Amiodarone at discharge | 1.728 | 1.187–2.515 | 0.004 | - | - | - |
| Preprocedural imaging | 0.738 | 0.518–1.051 | 0.092 | - | - | - |
| ES | 1.841 | 1.289–2.628 | 0.001 | 1.621 | 1.112–2.362 | 0.012 |
| (B) | Univariable | Multivariable | ||||
| Variable | HR | 95% CI | p Value | HR | 95% CI | p Value |
| Age | 1.005 | 0.993–1.016 | 0.431 | - | - | - |
| Epicardial ablation | 1.402 | 0.941–2.090 | 0.097 | - | - | - |
| Any VT inducible | 1.487 | 0.984–2.246 | 0.059 | - | - | - |
| Clinical VT inducible | 1.338 | 0.724–2.473 | 0.353 | - | - | - |
| LVEF | 1.038 | 1.010–1.075 | 0.001 | 1.032 | 1.010–1.045 | 0.009 |
| DCM | 1.952 | 1.370–2.780 | 0.001 | - | - | - |
| Beta blocker at discharge | 1.108 | 0.554–2.257 | 0.778 | - | - | - |
| Amiodarone at discharge | 1.831 | 1.310–2.560 | 0.001 | - | - | - |
| Preprocedural imaging | 0.734 | 0.534–1.009 | 0.057 | 0.630 | 0.453–0.876 | 0.006 |
| ES | 1.948 | 1.415–2.682 | 0.001 | 1.582 | 1.127–2.219 | 0.008 |
| (C) | Univariable | Multivariable | ||||
| Variable | HR | 95% CI | p Value | HR | 95% CI | p Value |
| Age | 1.090 | 1.050–1.131 | 0.001 | 1.101 | 1.054–1.149 | 0.001 |
| Epicardial ablation | 0.793 | 0.307–2.043 | 0.630 | - | - | - |
| Any VT inducible | 1.636 | 0.710–3.771 | 0.248 | - | - | - |
| Clinical VT inducible | 2.208 | 0.773–6.308 | 0.139 | - | - | - |
| LVEF | 1.145 | 1.030–1.325 | 0.001 | 1.102 | 1.023–1.278 | 0.004 |
| DCM | 1.240 | 0.581–2.646 | 0.579 | - | - | - |
| Beta blocker at discharge | 1.738 | 0.237–12.752 | 0.587 | - | - | - |
| Amiodarone at discharge | 2.692 | 1.344–5.395 | 0.005 | - | - | - |
| Preprocedural imaging | 0.316 | 0.144–0.695 | 0.004 | 0.361 | 0.155–0.844 | 0.019 |
| ES | 1.948 | 1.004–3.780 | 0.049 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mueller, J.; Chakarov, I.; Halbfass, P.; Nentwich, K.; Ene, E.; Berkovitz, A.; Sonne, K.; Barth, S.; Waechter, C.; Schupp, T.; et al. Electrical Storm Has Worse Prognosis Compared to Sustained Ventricular Tachycardia after VT Ablation. J. Clin. Med. 2023, 12, 2730. https://doi.org/10.3390/jcm12072730
Mueller J, Chakarov I, Halbfass P, Nentwich K, Ene E, Berkovitz A, Sonne K, Barth S, Waechter C, Schupp T, et al. Electrical Storm Has Worse Prognosis Compared to Sustained Ventricular Tachycardia after VT Ablation. Journal of Clinical Medicine. 2023; 12(7):2730. https://doi.org/10.3390/jcm12072730
Chicago/Turabian StyleMueller, Julian, Ivaylo Chakarov, Philipp Halbfass, Karin Nentwich, Elena Ene, Artur Berkovitz, Kai Sonne, Sebastian Barth, Christian Waechter, Tobias Schupp, and et al. 2023. "Electrical Storm Has Worse Prognosis Compared to Sustained Ventricular Tachycardia after VT Ablation" Journal of Clinical Medicine 12, no. 7: 2730. https://doi.org/10.3390/jcm12072730