
Comparison of 7-Year, Real-World Clinical Outcomes between Drug-Coated Balloon Angioplasty versus Drug-Eluting Stent Implantation in Patients with Drug-Eluting Stent In-Stent Restenosis
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Definition of Study Endpoints
2.3. Statistical Analysis
3. Results
3.1. Baseline LOCO-Oriented Clinical and Angiographic Characteristics
3.2. Procedural Characteristics
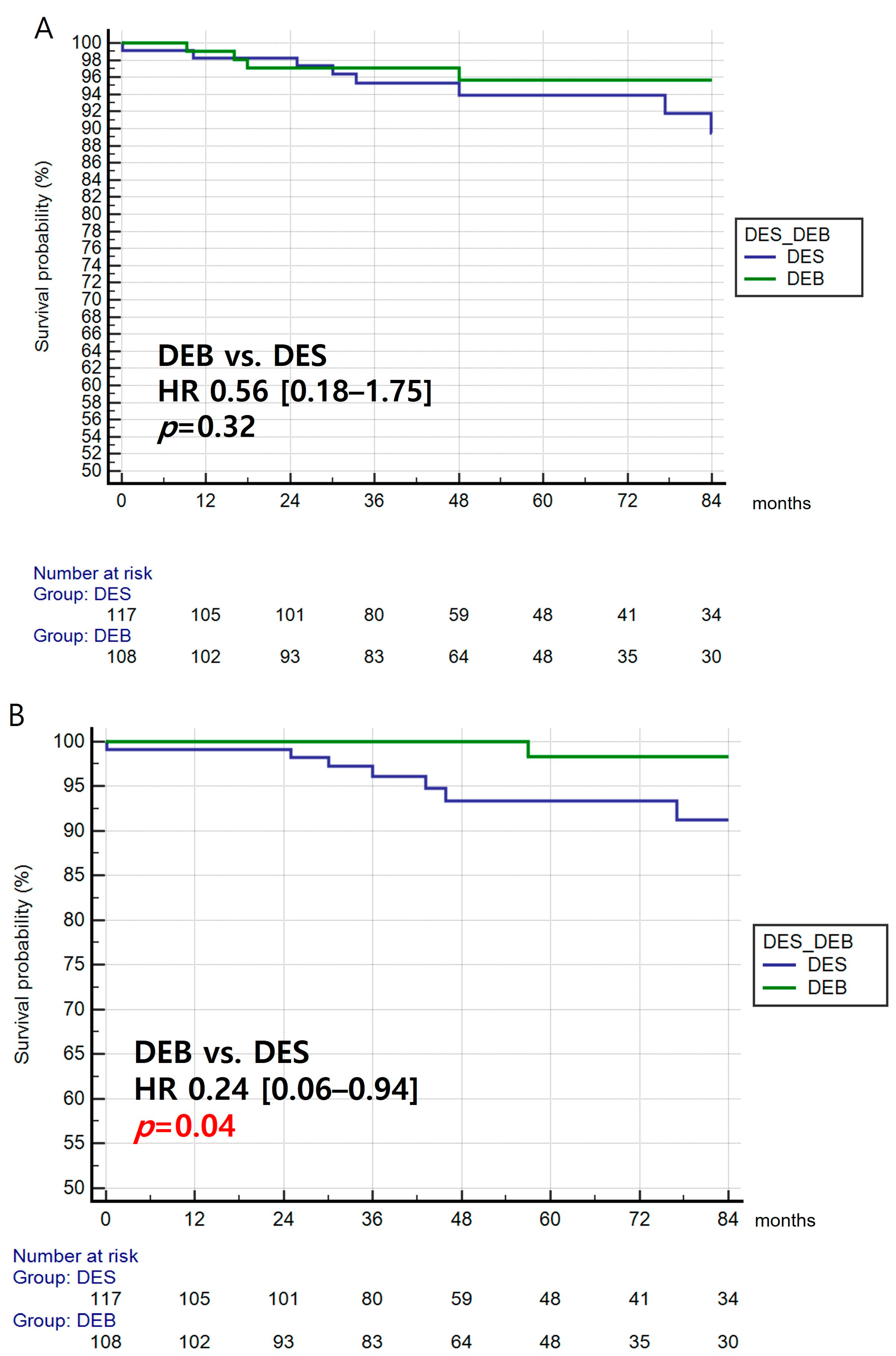
3.3. Primary Efficacy Endpoint, TLR
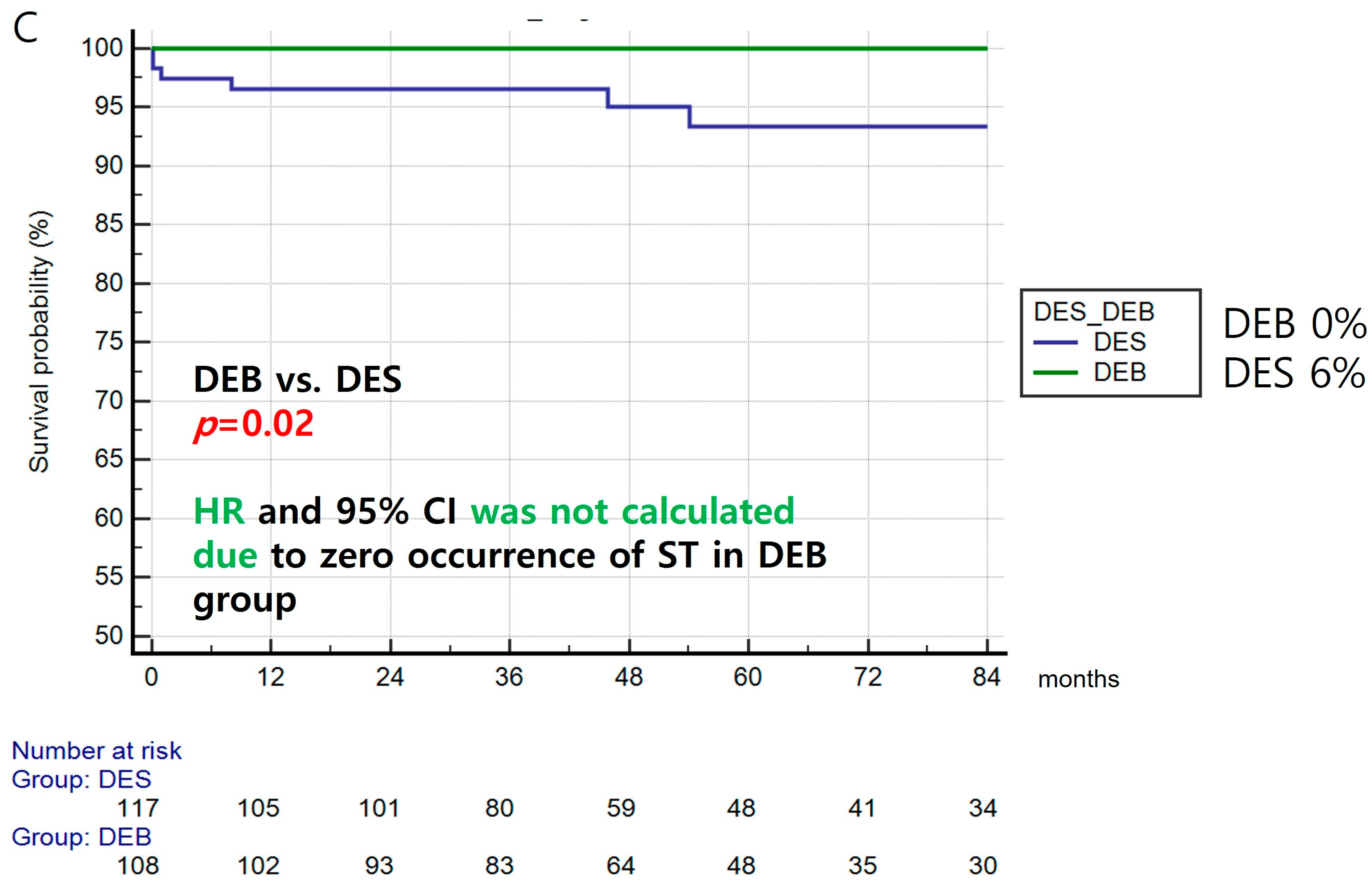
3.4. Primary Safety Endpoint
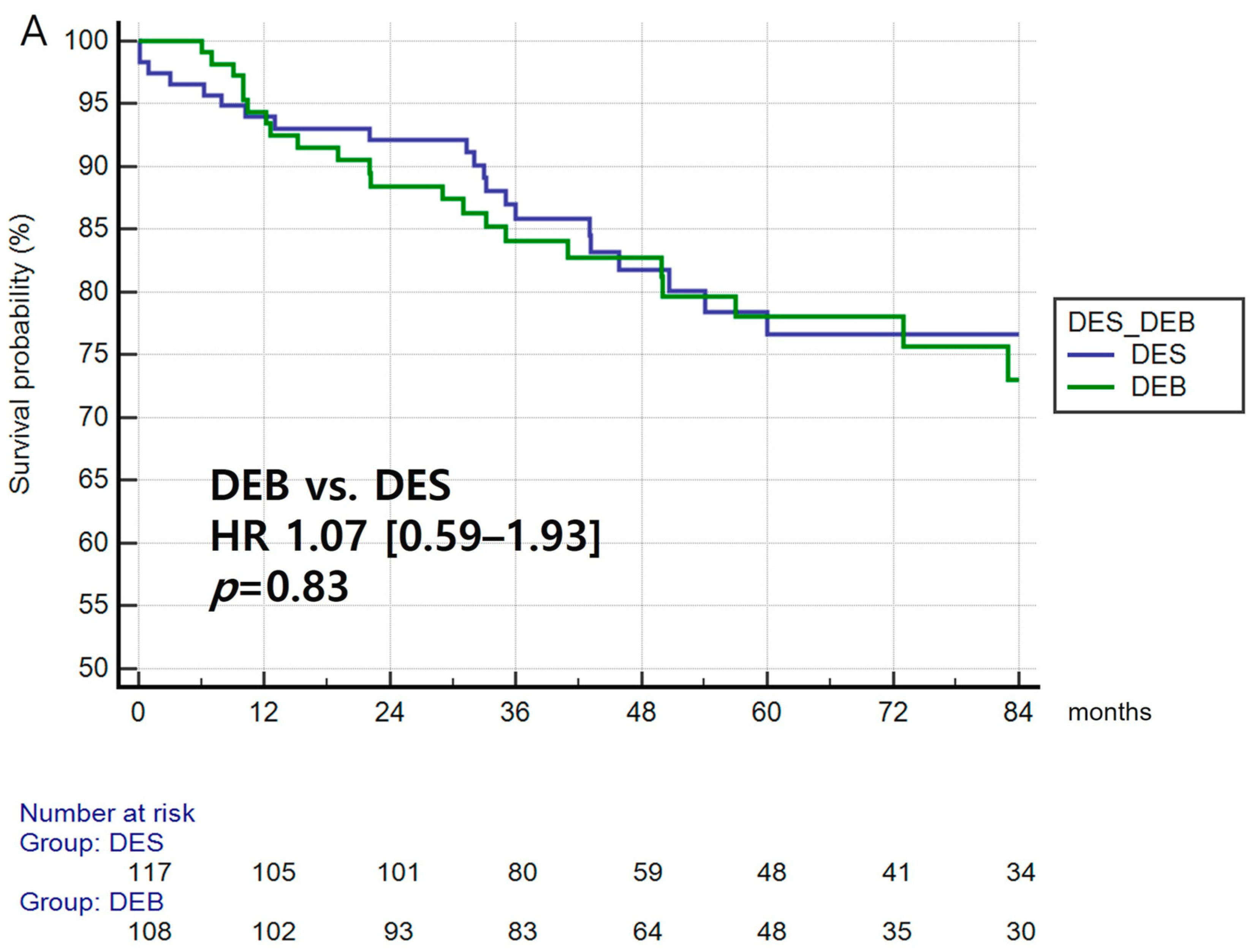
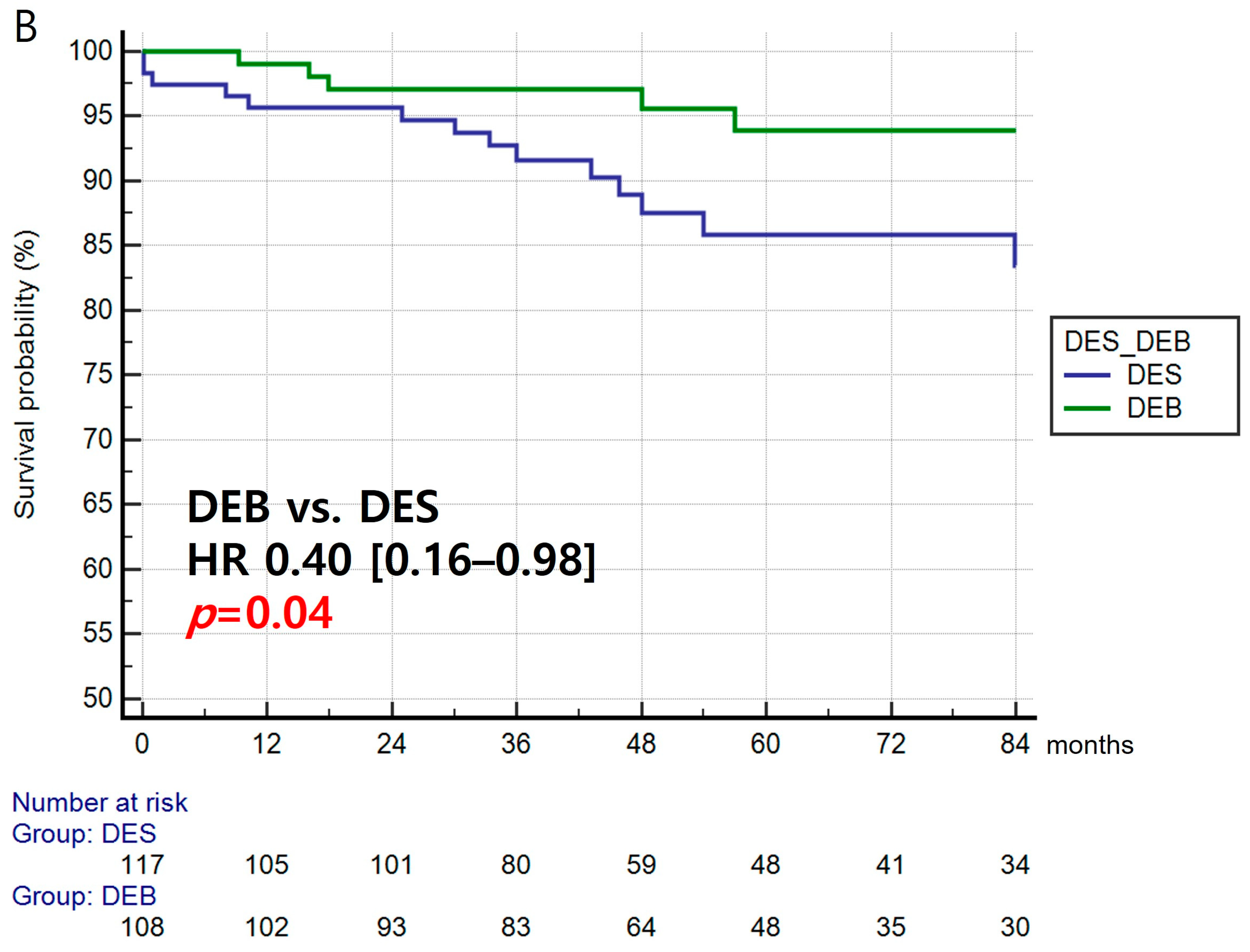
3.5. Secondary Endpoints
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CABG | Coronary Artery Bypass Grafting |
| DEB | drug-eluting balloon |
| DES | Drug-eluting stent |
| ISR | In-stent restenosis |
| TLR | Target lesion revascularization |
| LOCO | Lesion-oriented composite outcome |
| MI | Myocardial infarction |
| MACE | Major adverse cardiovascular event |
| PCI | Percutaneous coronary intervention |
References
- Dangas, G.D.; Claessen, B.E.; Caixeta, A.; Sanidas, E.A.; Mintz, G.S.; Mehran, R. In-stent restenosis in the drug-eluting stent era. J. Am. Coll. Cardiol. 2010, 56, 1897–1907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iqbal, J.; Serruys, P.W.; Silber, S.; Kelbaek, H.; Richardt, G.; Morel, M.A.; Negoita, M.; Buszman, P.E.; Windecker, S. Comparison of zotarolimus- and everolimus-eluting coronary stents: Final 5-year report of the RESOLUTE all-comers trial. Circ. Cardiovasc. Interv. 2015, 8, e002230. [Google Scholar] [CrossRef] [Green Version]
- Kufner, S.; Joner, M.; Thannheimer, A.; Hoppmann, P.; Ibrahim, T.; Mayer, K.; Cassese, S.; Laugwitz, K.L.; Schunkert, H.; Kastrati, A.; et al. Ten-Year Clinical Outcomes From a Trial of Three Limus-Eluting Stents with Different Polymer Coatings in Patients with Coronary Artery Disease. Circulation 2019, 139, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Pilgrim, T.; Piccolo, R.; Heg, D.; Roffi, M.; Tuller, D.; Muller, O.; Moarof, I.; Siontis, G.C.M.; Cook, S.; Weilenmann, D.; et al. Ultrathin-strut, biodegradable-polymer, sirolimus-eluting stents versus thin-strut, durable-polymer, everolimus-eluting stents for percutaneous coronary revascularisation: 5-year outcomes of the BIOSCIENCE randomised trial. Lancet 2018, 392, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Vlachojannis, G.J.; Smits, P.C.; Hofma, S.H.; Togni, M.; Vazquez, N.; Valdes, M.; Voudris, V.; Slagboom, T.; Goy, J.J.; den Heijer, P.; et al. Biodegradable Polymer Biolimus-Eluting Stents Versus Durable Polymer Everolimus-Eluting Stents in Patients With Coronary Artery Disease: Final 5-Year Report From the COMPARE II Trial (Abluminal Biodegradable Polymer Biolimus-Eluting Stent Versus Durable Polymer Everolimus-Eluting Stent). JACC Cardiovasc. Interv. 2017, 10, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Cortese, B.; Di Palma, G.; Guimaraes, M.G.; Piraino, D.; Orrego, P.S.; Buccheri, D.; Rivero, F.; Perotto, A.; Zambelli, G.; Alfonso, F. Drug-Coated Balloon Versus Drug-Eluting Stent for Small Coronary Vessel Disease: PICCOLETO II Randomized Clinical Trial. JACC Cardiovasc. Interv. 2020, 13, 2840–2849. [Google Scholar] [CrossRef] [PubMed]
- Franchin, L.; Piroli, F.; D’Ascenzo, F.; Nunez-Gil, I.; Wojakowski, W.; Imori, Y.; Trabattoni, D.; Huczek, Z.; Venuti, G.; Muscoli, S.; et al. Impact of stent thickness on clinical outcomes in small vessel and bifurcation lesions: A RAIN-CARDIOGROUP VII sub-study. J. Cardiovasc. Med. 2021, 22, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Saylik, F.; Cinar, T.; Selcuk, M.; Cicek, V.; Hayiroglu, M.I.; Orhan, A.L. Comparison of outcomes between single long stent and overlapping stents: A meta-analysis of the literature. Herz 2023, 1–8. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacoppo, D.; Alfonso, F.; Xu, B.; Claessen, B.; Adriaenssens, T.; Jensen, C.; Perez-Vizcayno, M.J.; Kang, D.Y.; Degenhardt, R.; Pleva, L.; et al. Paclitaxel-coated balloon angioplasty vs. drug-eluting stenting for the treatment of coronary in-stent restenosis: A comprehensive, collaborative, individual patient data meta-analysis of 10 randomized clinical trials (DAEDALUS study). Eur. Heart J. 2020, 41, 3715–3728. [Google Scholar] [CrossRef]
- Jang, A.Y.; Yu, J.; Oh, P.C.; Kim, M.; Suh, S.Y.; Lee, K.; Han, S.H.; Kang, W.C. Real-World Long-Term Clinical Outcomes of Ultrathin Strut Biodegradable Polymer Drug-Eluting Stents in Korean ST-Segment-Elevation Myocardial Infarction (STEMI) Patients with or without Acute Heart Failure Undergoing Primary Percutaneous Coronary Intervention. J. Clin. Med. 2021, 10, 5898. [Google Scholar] [CrossRef]
- Kufner, S.; Cassese, S.; Valeskini, M.; Neumann, F.J.; Schulz-Schupke, S.; Hoppmann, P.; Fusaro, M.; Schunkert, H.; Laugwitz, K.L.; Kastrati, A.; et al. Long-Term Efficacy and Safety of Paclitaxel-Eluting Balloon for the Treatment of Drug-Eluting Stent Restenosis: 3-Year Results of a Randomized Controlled Trial. JACC Cardiovasc. Interv. 2015, 8, 877–884. [Google Scholar] [CrossRef] [Green Version]
- Alfonso, F.; Perez-Vizcayno, M.J.; Cuesta, J.; Garcia Del Blanco, B.; Garcia-Touchard, A.; Lopez-Minguez, J.R.; Masotti, M.; Zueco, J.; Cequier, A.; Velazquez, M.; et al. 3-Year Clinical Follow-Up of the RIBS IV Clinical Trial: A Prospective Randomized Study of Drug-Eluting Balloons Versus Everolimus-Eluting Stents in Patients With In-Stent Restenosis in Coronary Arteries Previously Treated With Drug-Eluting Stents. JACC Cardiovasc. Interv. 2018, 11, 981–991. [Google Scholar] [CrossRef]
- Park, S.J.; Kang, S.J.; Virmani, R.; Nakano, M.; Ueda, Y. In-stent neoatherosclerosis: A final common pathway of late stent failure. J. Am. Coll. Cardiol. 2012, 59, 2051–2057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.M.; Park, J.; Kang, J.; Jeon, K.H.; Jung, J.H.; Lee, S.E.; Han, J.K.; Kim, H.L.; Yang, H.M.; Park, K.W.; et al. Comparison Among Drug-Eluting Balloon, Drug-Eluting Stent, and Plain Balloon Angioplasty for the Treatment of In-Stent Restenosis A Network Meta-Analysis of 11 Randomized, Controlled Trials. Jacc-Cardiovasc. Interv. 2015, 8, 382–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Condello, F.; Spaccarotella, C.; Sorrentino, S.; Indolfi, C.; Stefanini, G.G.; Polimeni, A. Stent Thrombosis and Restenosis with Contemporary Drug-Eluting Stents: Predictors and Current Evidence. J. Clin. Med. 2023, 12, 1238. [Google Scholar] [CrossRef] [PubMed]
- Tekkesin, A.I.; Kaya, A.; Cakilli, Y.; Turkkan, C.; Hayiroglu, M.I.; Borklu, E.B.; Kalenderoglu, K.; Gumusdag, A.; Yildirimturk, O.; Bozbeyoglu, E.; et al. The first six-month clinical outcomes and risk factors associated with high on-treatment platelet reactivity of clopidogrel in patients undergoing coronary interventions. Anatol. J. Cardiol. 2016, 16, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Giacoppo, D.; Alvarez-Covarrubias, H.A.; Koch, T.; Cassese, S.; Xhepa, E.; Kessler, T.; Wiebe, J.; Joner, M.; Hochholzer, W.; Laugwitz, K.L.; et al. Coronary artery restenosis treatment with plain balloon, drug-coated balloon, or drug-eluting stent: 10-year outcomes of the ISAR-DESIRE 3 trial. Eur. Heart J. 2023, 44, 1343–1357. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DEB (n = 108) | DES (n = 117) | p-Value | |
|---|---|---|---|
| Age, years | 63.0 ± 11.1 | 62.2 ± 12.0 | 0.63 |
| Male | 69 (63.9) | 79 (67.5) | 0.58 |
| HTN | 66 (61.1) | 67 (57.3) | 0.59 |
| Diabetes | 50 (46.3) | 48 (41.0) | 0.50 |
| Dyslipidaemia | 57 (52.8) | 65 (55.6) | 0.69 |
| Current smoking | 21 (19.4) | 16 (13.7) | 0.28 |
| ACS | 97 (89.8) | 92 (78.6) | 0.03 |
| EF | 58.6 ± 10.4 | 55.9 ± 12.5 | 0.08 |
| ISR location | 0.44 | ||
| LM | 2 (1.9) | 0 | |
| LAD | 55 (50.9) | 73 (62.4) | |
| LCX | 21 (19.4) | 13 (11.1) | |
| RCA | 30 (27.8) | 31 (26.5) | |
| Previous DES stent: | |||
| -Taxol-based stent | 19 (17.6) | 33 (28.2) | 0.08 |
| -Limus-based stent | 89 (82.4) | 84 (71.8) | |
| -1st generation DES | 55 (50.9) | 62 (53.0) | 0.70 |
| -2nd generation DES | 53 (49.1) | 55 (47.0) | |
| -Pre-stent diameter, mm | 3.0 ± 0.4 | 3.0 ± 0.4 | 0.63 |
| -Pre-stent length, mm | 24.3 ± 6.6 | 25.6 ± 7.6 | 0.17 |
| ISR pattern: | 0.02 | ||
| I (focal) | 73 (67.6) | 65 (55.6) | |
| II (diffuse intra-stent) | 12 (11.1) | 15 (12.8) | |
| III (proliferative) | 13 (12.0) | 11 (9.4) | |
| IV (occlusive) | 10 (9.3) | 26 (22.2) | |
| Total obstruction | 10 (9.3) | 26 (22.2) | 0.01 |
| Edge involvement | 56 (51.9) | 78 (66.7) | 0.02 |
| CTO | 8 (7.4) | 5 (4.3) | 0.32 |
| Variable | |
|---|---|
| Pre-dilation, % | 100% |
| DEB diameter, mm | 2.8 ± 0.3 |
| DEB length, mm | 22.0 ± 5.5 |
| Inflation time, s | 41.5 ± 20.5 |
| Inflation pressure, atm | 10.1 ± 3.3 |
| Variable | |
|---|---|
| DES diameter, mm | 3.0 ± 0.4 mm |
| DES length, mm | 24.5 ± 9.3 mm |
| Inflation time, s | 17.1 ± 20.2 s |
| Inflation pressure, atm | 13.2 ± 3.3 atm |
| 1st generation stents | 33 (28.2) |
| 2nd generation stents | 84 (71.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Jang, A.Y.; Lee, J.; Seo, J.; Shin, Y.H.; Oh, P.C.; Suh, S.Y.; Lee, K.; Kang, W.C.; Han, S.-H. Comparison of 7-Year, Real-World Clinical Outcomes between Drug-Coated Balloon Angioplasty versus Drug-Eluting Stent Implantation in Patients with Drug-Eluting Stent In-Stent Restenosis. J. Clin. Med. 2023, 12, 4246. https://doi.org/10.3390/jcm12134246
Kim M, Jang AY, Lee J, Seo J, Shin YH, Oh PC, Suh SY, Lee K, Kang WC, Han S-H. Comparison of 7-Year, Real-World Clinical Outcomes between Drug-Coated Balloon Angioplasty versus Drug-Eluting Stent Implantation in Patients with Drug-Eluting Stent In-Stent Restenosis. Journal of Clinical Medicine. 2023; 12(13):4246. https://doi.org/10.3390/jcm12134246
Chicago/Turabian StyleKim, Minsu, Albert Youngwoo Jang, Joonpyo Lee, Jeongduk Seo, Yong Hoon Shin, Pyung Chun Oh, Soon Yong Suh, Kyounghoon Lee, Woong Chol Kang, and Seung-Hwan Han. 2023. "Comparison of 7-Year, Real-World Clinical Outcomes between Drug-Coated Balloon Angioplasty versus Drug-Eluting Stent Implantation in Patients with Drug-Eluting Stent In-Stent Restenosis" Journal of Clinical Medicine 12, no. 13: 4246. https://doi.org/10.3390/jcm12134246