

Identification of Low- versus High-Risk Acute Coronary Syndrome for a Selective ECG Monitoring Strategy
 and
and
Abstract
:1. Introduction
2. Materials and Methods
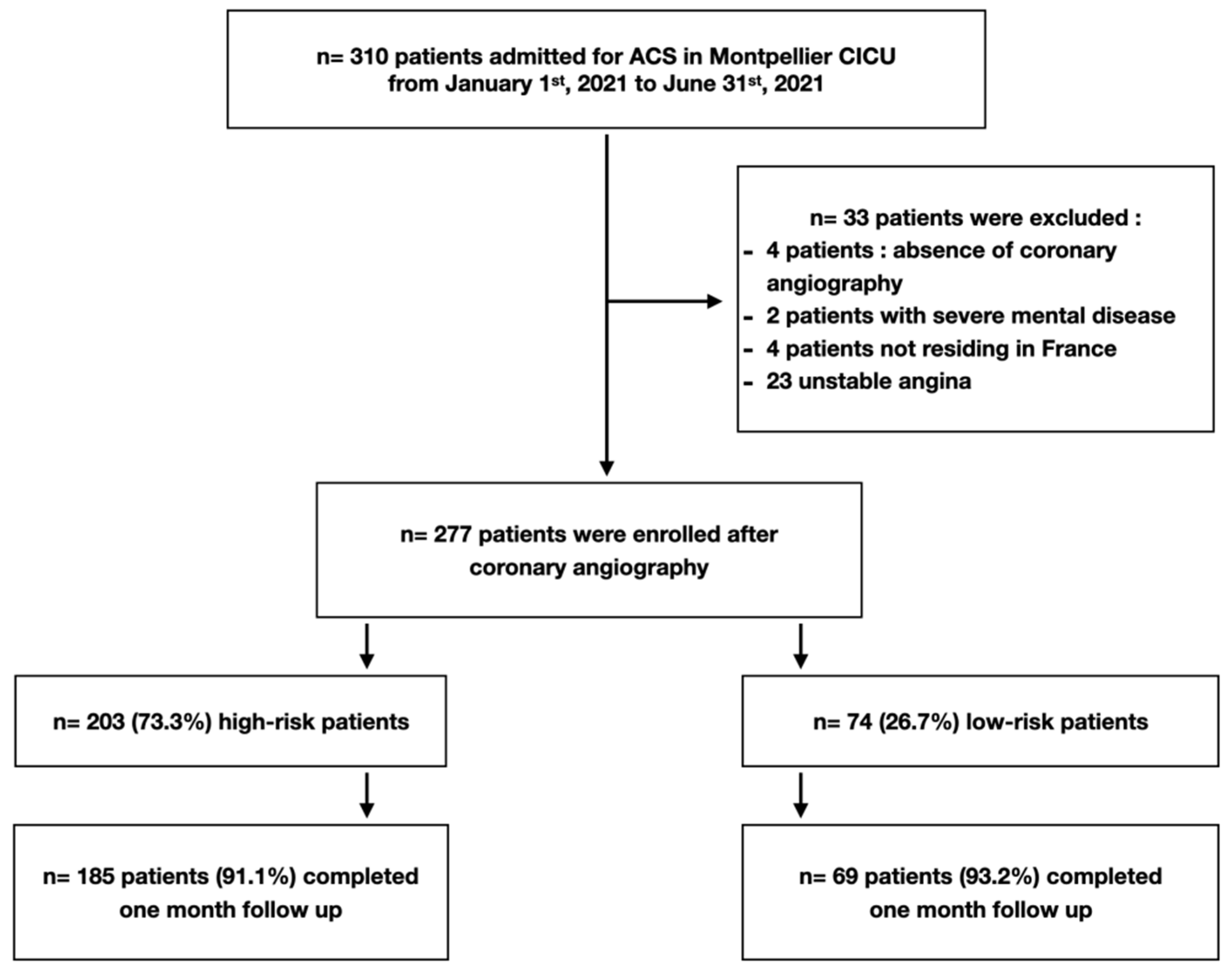
2.1. Study Design and Patients
2.2. High vs. Low-Risk Patients
2.3. Coronary Angiography Evaluation
2.4. Study Endpoints
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. End Points
4. Discussion
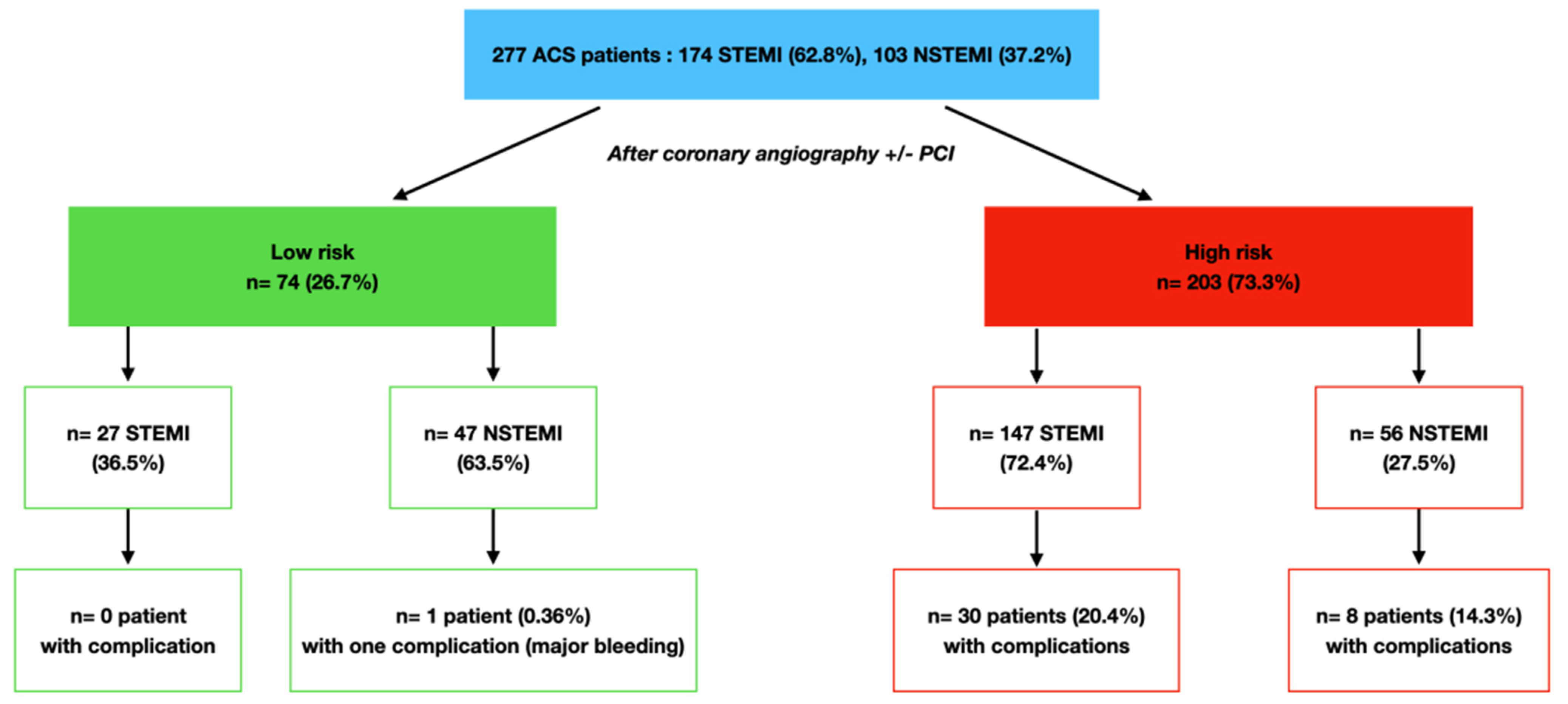
- Approximately 1/4 of all ACS and 1/2 of NSTEMI patients may be considered at low risk of in-hospital major outcomes based on simple and routinely assessed clinical and angiographic criteria;
- Following early invasive strategy and PCI for the vast majority of patients, a low rate of complications with no life-threatening event, rhythmic or conduction disorders was observed in the low-risk group (NPV 98.6% for all ACS and NPV 100% in the STEMI group).
4.1. Low vs. High-Risk ACS Patients
4.2. Early Invasive Strategy for Patient Stratification
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Puymirat, E.; Simon, T.; Cayla, G.; Cottin, Y.; Elbaz, M.; Coste, P.; Lemesle, G.; Motreff, P.; Popovic, B.; Khalife, K.; et al. Acute myocardial infarction: Changes in patient characteristics, management, and 6-month outcomes over a period of 20 years in the FAST-MI program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation 2017, 136, 19081919. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Bebb, O.J.; Dondo, T.B.; Yan, A.T.; Goodman, S.G.; Bueno, H.; Chew, D.P.; Brieger, D.; Batin, P.D.; Farkouh, M.E.; et al. Guideline-indicated treatments and diagnostics, GRACE risk score, and survival for non-ST elevation myocardial infarction. Eur. Heart J. 2018, 39, 37983806. [Google Scholar] [CrossRef] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [PubMed]
- Chen, R.; Strait, K.M.; Dharmarajan, K.; Li, S.X.; Ranasinghe, I.; Martin, J.; Fazel, R.; Masoudi, F.A.; Cooke, C.R.; Nallamothu, B.K.; et al. Hospital variation in admission to intensive care units for patients with acute myocardial infarction. Am. Heart J. 2015, 170, 1161–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Diepen, S.; Lin, M.; Bakal, J.A.; McAlister, F.A.; Kaul, P.; Katz, J.N.; Fordyce, C.B.; Southern, D.A.; Graham, M.M.; Wilton, S.B.; et al. Do stable non-ST-segment elevation acute coronary syndromes require admission to coronary care units? Am. Heart J. 2016, 175, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Insam, C.; Paccaud, F.; Marques-Vidal, P. The region makes the difference: Disparities in management of acute myocardial infarction within Switzerland. Eur. J. Prev. Cardiol. 2014, 21, 541–548. [Google Scholar] [CrossRef]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.I.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar]
- Antman, E.M.; Cohen, M.; Bernink, P.J.; McCabe, C.H.; Horacek, T.; Papuchis, G.; Mautner, B.; Corbalan, R.; Radley, D.; Braunwald, E. The TIMI risk score for unstable angina/non–ST elevation MI: A method for prognostication and therapeutic decision making. JAMA 2000, 284, 835. [Google Scholar] [CrossRef] [Green Version]
- Boersma, E.; Pieper, K.S.; Steyerberg, E.W.; Wilcox, R.G.; Chang, W.C.; Lee, K.L.; Akkerhuis, K.M.; Harrington, R.A.; Deckers, J.W.; Armstrong, P.W.; et al. Predictors of outcome in patients with acute coronary syndromes without persistent ST-segment elevation. Results from an international trial of 9461 patients. Circulation 2000, 101, 2557–2567. [Google Scholar] [CrossRef] [Green Version]
- Chin, C.T.; Chen, A.Y.; Wang, T.Y.; Alexander, K.P.; Mathews, R.; Rumsfeld, J.S.; Cannon, C.P.; Fonarow, G.C.; Peterson, E.D.; Roe, M.T. Risk adjustment for in-hospital mortality of contemporary patients with acute myocardial infarction: The acute coronary treatment and intervention outcomes network (ACTION) Registry–get with the guidelines (GWTG) acute myocardial infarction mortality model and risk score. Am. Heart J. 2011, 161, 113–122. [Google Scholar]
- Granger, C.B.; Goldberg, R.J.; Dabbous, O.; Pieper, K.S.; Eagle, K.A.; Cannon, C.P.; Van De Werf, F.; Avezum, A.; Goodman, S.G.; Flather, M.D.; et al. Predictors of Hospital Mortality in the Global Registry of Acute Coronary Events. Arch. Intern. Med. 2003, 163, 2345–2353. [Google Scholar] [CrossRef] [Green Version]
- Eagle, K.A.; Lim, M.J.; Dabbous, O.H.; Pieper, K.S.; Goldberg, R.J.; Van de Werf, F.; Goodman, S.G.; Granger, C.B.; Steg, P.G.; Gore, J.M.; et al. A validated prediction model for all forms of acute coronary syndrome: Estimating the risk of 6-Month postdischarge death in an international registry. JAMA 2004, 291, 2727–2733. [Google Scholar] [CrossRef] [Green Version]
- Fanaroff, A.C.; Chen, A.Y.; Thomas, L.E.; Pieper, K.S.; Garratt, K.N.; Peterson, E.D.; Newby, L.K.; De Lemos, J.A.; Kosiborod, M.N.; Amsterdam, E.A.; et al. Risk Score to Predict Need for Intensive Care in Initially Hemodynamically Stable Adults With Non-ST-Segment–Elevation Myocardial Infarction. J. Am. Heart Assoc. 2018, 7, e008894. [Google Scholar] [CrossRef] [Green Version]
- Guimarães, P.O.; Sampaio, M.C.; Malafaia, F.L.; Lopes, R.D.; Fanaroff, A.C.; de Barros ESilva, P.G.M.; Dos Santos, T.M.; Okada, M.Y.; Mouallem, A.R.E.; Diniz, M.D.S.; et al. Clinical outcomes and need for intensive care after non-ST-segment-elevation myocardial infarction. Eur. J. Intern. Med. 2020, 76, 58–63. [Google Scholar] [CrossRef]
- Vasquez-Rodriguez, J.F.; Idrovo-Turbay, C.; Perez-Fernandez, O.M.; Cruz-Tapias, P.; Isaza, N.; Navarro, A.; Medina-Mur, R.; Ramirez-Lovera, V.; Giraldo, L.E.; Ariza, N.; et al. Risk of complications after a non-ST segment elevation acute myocardial infarction in a Latin-American cohort: An application of the ACTION ICU score. Heart Lung 2023, 57, 124–129. [Google Scholar] [CrossRef]
- Ran, P.; Yang, J.Q.; Li, J.; Li, G.; Wang, Y.; Qiu, J.; Zong, Q.I.; Weil, X.B.; Huang, J.L.; Siu, C.W.; et al. A risk score to predict in-hospital mortality in patients with acute coronary syndrome at early medical contact: Results from the Improving Care for Cardiovascular Disease in China-Acute Coronary Syndrome (CCC-ACS) Project. Ann. Transl. Med. 2021, 9, 167. [Google Scholar] [CrossRef]
- Lansky, A.J.; Goto, K.; Cristea, E.; Fahy, M.; Parise, H.; Feit, F.; Ohman, E.M.; White, H.D.; Alexander, K.P.; Bertrand, M.E.; et al. Clinical and angiographic predictors of short- and long-term ischemic events in acute coronary syndromes: Results from the Acute Catheterization and Urgent Intervention Triage strategY (ACUITY) trial. Circ. Cardiovasc. Interv. 2010, 3, 308–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, G.W.; Bertrand, M.; Colombo, A.; Dangas, G.; Farkouh, M.E.; Feit, F.; Lansky, A.J.; Lincoff, A.M.; Mehran, R.; Moses, J.W.; et al. Acute Catheterization and Urgent Intervention Triage strategY (ACUITY) trial: Study design and rationale. Am. Heart J. 2004, 148, 764–775. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Ware, J.H.; Bertrand, M.E.; Lincoff, A.M.; Moses, J.W.; Ohman, E.M.; White, H.D.; Feit, F.; Colombo, A.; McLaurin, B.T.; et al. Antithrombotic Strategies in Patients with Acute Coronary Syndromes Undergoing Early Invasive Management: One-Year Results From the ACUITY Trial. JAMA 2007, 298, 2497–2506. [Google Scholar] [CrossRef]
- Navarese, E.P.; Gurbel, P.A.; Andreotti, F.; Tantry, U.; Jeong, Y.H.; Kozinski, M.; Engstrøm, T.; Di Pasquale, G.; Kochman, W.; Ardissino, D.; et al. Optimal timing of coronary invasive strategy in non-ST-segment elevation acute coronary syndromes: A systematic review and meta-analysis. Ann. Intern. Med. 2013, 158, 261–270. [Google Scholar] [CrossRef]
- Jobs, A.; Mehta, S.R.; Montalescot, G.; Vicaut, E.; Van’t Hof, A.W.J.; Badings, E.A.; Neumann, F.J.; Kastrati, A.; Sciahbasi, A.; Reuter, P.G.; et al. Optimal timing of an invasive strategy in patients with non-ST-elevation acute coronary syndrome a meta-analysis of randomised trials. Lancet 2017, 390, 737–746. [Google Scholar] [CrossRef]
- Fefer, P.; Beigel, R.; Atar, S.; Aronson, D.; Pollak, A.; Zahger, D.; Asher, E.; Iakobishvili, Z.; Shlomo, N.; Alcalai, R.; et al. Outcomes of Patients Presenting with Clinical Indices of Spontaneous Reperfusion in ST-Elevation Acute Coronary Syndrome Undergoing Deferred Angiography. J. Am. Heart Assoc. 2017, 6, e004552. [Google Scholar] [CrossRef]
- Bohula, E.A.; Van Diepen, S.; Katz, J.; Morrow, D. Can triage to cardiac intensive care units for acute coronary syndromes be refined: Data from the Critical Care Cardiology Trials Network (CCCTN) registry. J. Am. Coll. Cardiol. 2019, 73, 27. [Google Scholar] [CrossRef]
- Fanaroff, A.C.; Peterson, E.D.; Chen, A.Y.; Thomas, L.; Doll, J.A.; Fordyce, C.B.; Newby, L.K.; Amsterdam, E.A.; Kosiborod, M.N.; De Lemos, J.A.; et al. Intensive Care Unit Utilization and Mortality Among Medicare Patients Hospitalized with Non–ST-Segment Elevation Myocardial Infarction. JAMA Cardiol. 2017, 2, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Bray, M.; Hollings, S.; Roebuck, C.; Gale, C.P.; Mamas, M.A.; et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Vecchio, S.; Fileti, L.; Reggi, A.; Moschini, C.; Lorenzetti, S.; Rubboli, A. Impatto della pandemia COVID-19 sui ricoveri per sindrome coronarica acuta: Revisione della letteratura ed esperienza monocentrica. G. Ital. Di Cardiol. 2020, 21, 502–508. [Google Scholar]



{kind=link}
{kind=link}
| Low-Risk Group | High-Risk Group | |
|---|---|---|
| NSTEMI and STEMI patients | ||
| Age > 80 years | - | + |
| Unstable hemodynamics @ | - | + |
| Severe comorbidities ▲ | - | + |
| Left ventricular ejection fraction < 40% | - | + |
| Rhythmic state requiring specific therapeutic intervention & | - | + |
| Failure of reperfusion or unsatisfactory result of PCI ⌀ | - | + |
| Severe residual coronary lesions requiring further revascularization ⌀ | - | + |
| High bleeding risk * | - | + |
| STEMI patients | ||
| Early and successfully reperfused STEMI # | + | - |
| Total Population n = 277 | Low-Risk Group n = 74 | High-Risk Group n = 203 | p-Value | |
|---|---|---|---|---|
| Age (years), median | 66 (56–75) | 63 (54–70) | 67 (57–78) | <0.01 |
| Male sex, n (%) | 208 (75.1) | 61 (82.4) | 147 (72.4) | 0.09 |
| Body mass index (kg/m2), median | 26 (24–29) | 26 (24–29) | 26 (23–29) | 0.27 |
| Hypertension, n (%) | 122 (44.0) | 27 (36.5) | 95 (46.8) | 0.13 |
| Active smoker, n (%) | 115 (41.5) | 35 (47.3) | 80 (39.4) | 0.24 |
| Prior MI, n (%) | 45 (16.3) | 6 (8.1) | 39 (19.2) | 0.03 |
| Severe pulmonary disease, n (%) | 12 (4.3) | 2 (2.7) | 10 (5) | 0.52 |
| Severe chronic renal disease ▲, n (%) | 6 (2.2) | 0 (0) | 6 (2.9) | 0.49 |
| Severe chronic lung disease, n (%) | 0 (0) | 0 (0) | 0 (0) | 1 |
| Oral anticoagulants, n (%) | 16 (5.8) | 0 (0) | 16 (7.9) | 0.01 |
| Type of AMI | ||||
| STEMI, n (%) | 174 (62.8) | 27 (15.5) | 147 (84.5) | <0.01 |
| NSTEMI, n (%) | 103 (37.1) | 47(45.6) | 56 (54.4) | <0.01 |
| LVEF, median | 50 (45–60) | 60 (50–60) | 50 (40–55) | <0.01 |
| Antiplatelet therapy | ||||
| Clopidogrel, n (%) | 22 (7.94) | 4 (5.4) | 18 (8.9) | 0.3 |
| Ticagrelor, n (%) | 255 (92.1) | 70 (94.6) | 185 (91.1) | 0.3 |
| Coronary angiogram | ||||
| Single vessel disease, n (%) | 95 (34.3) | 36 (48.7) | 59 (29.1) | <0.01 |
| Multivessel disease, n (%) | 182 (65.7) | 38 (51.4) | 144 (70.9) | <0.01 |
| LM disease | 10 (3.6) | 0 (0.0) | 10 (4.9) | 0.05 |
| LAD disease | 143 (51.6) | 40 (54.1) | 103 (50.7) | 0.6 |
| Circumflex disease | 57 (20.6) | 17 (22.9) | 40 (19.7) | 0.6 |
| RCA disease | 99 (35.7) | 21 (28.4) | 78 (38.4) | 0.1 |
| Stent thrombosis, n (%) | 4 (1.4) | 0 (0.0) | 4 (2.0) | 0.2 |
| Revascularization strategy | ||||
| PCI, n (%) | 260 (93.9) | 73 (98.7) | 187 (92.1) | 0.05 |
| Bypass surgery, n (%) | 15 (5.4) | 0 (0.0) | 15 (7.4) | 0.02 |
| Medical therapy only | 2 (0.7) | 1 (1.3) | 1 (0.5) | 0.5 |
| Total Population n = 277 | Low-Risk Group n = 74 | High-Risk Group n = 203 | p-Value | |
|---|---|---|---|---|
| Total in-hospital complications, n (%) * | 38 (14.1) | 1 (1.3) | 37 (18.2) | <0.01 |
| Unstable hemodynamic state, n (%) | 17 (6.1) | 0 (0.0) | 17 (8.4) | <0.01 |
| Pericardial effusion requiring treatment, n (%) | 7 (2.5) | 0 (0.0) | 7 (3.5) | 0.11 |
| Sustained or poorly tolerated ventricular arrhythmia, n (%) | 13 (4.7) | 0 (0.0) | 13 (6.4) | 0.03 |
| Severe conduction disorders, n (%) | 11 (4.0) | 0 (0.0) | 11 (5.2) | 0.04 |
| Chest pain recurrence requiring coronary angiography, n (%) | 7 (2.5) | 0 (0.0) | 7 (3.5) | 0.1 |
| Death from any cause, n (%) | 6 (2.2) | 0 (0.0) | 6 (3.0) | 0.4 |
| Heart failure, n (%) | 7 (2.5) | 0 (0.0) | 7 (3.5) | 0.1 |
| Major bleeding, n (%) | 3 (1.1) | 1 (1.3) | 2 (1.0) | 1 |
| Stroke, n (%) | 1 (0.4) | 0 (0.0) | 1 (0.5) | 1 |
| Secondary transfer to CICU, n (%) | 3 (1.1) | 0 (0.0) | 3 (1.5) | 0.6 |
| Number of Events | ||||||||
|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | Total | |
| Low-risk, n (%) | 73 (98.6) | 1 (1.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 74 (26.8) |
| High-risk, n (%) | 165 (81.3) | 19 (9.4) | 10 (4.9) | 5 (2.5) | 2 (1.0) | 1 (0.5) | 1 (0.5) | 203 (73.2) |
| Total, n (%) | 238 (85.9) | 20 (7.2) | 10 (3.6) | 5 (1.8) | 2 (0.7) | 1 (0.4) | 1 (0.4) | 277 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akodad, M.; Meunier, P.-A.; Padovani, C.; Cayla, G.; Zitouni, W.; Macia, J.-C.; Robert, P.; Steinecker, M.; Roubille, F.; Leclercq, F. Identification of Low- versus High-Risk Acute Coronary Syndrome for a Selective ECG Monitoring Strategy. J. Clin. Med. 2023, 12, 4604. https://doi.org/10.3390/jcm12144604
Akodad M, Meunier P-A, Padovani C, Cayla G, Zitouni W, Macia J-C, Robert P, Steinecker M, Roubille F, Leclercq F. Identification of Low- versus High-Risk Acute Coronary Syndrome for a Selective ECG Monitoring Strategy. Journal of Clinical Medicine. 2023; 12(14):4604. https://doi.org/10.3390/jcm12144604
Chicago/Turabian StyleAkodad, Mariama, Pierre-Alain Meunier, Caroline Padovani, Guillaume Cayla, Wassim Zitouni, Jean-Christophe Macia, Pierre Robert, Matthieu Steinecker, François Roubille, and Florence Leclercq. 2023. "Identification of Low- versus High-Risk Acute Coronary Syndrome for a Selective ECG Monitoring Strategy" Journal of Clinical Medicine 12, no. 14: 4604. https://doi.org/10.3390/jcm12144604