
Transplant and Recipient Factors in Prediction of Kidney Transplant Outcomes: A UK-Wide Paired Analysis

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Missing Data
3.2. DBD and DCD Cohorts
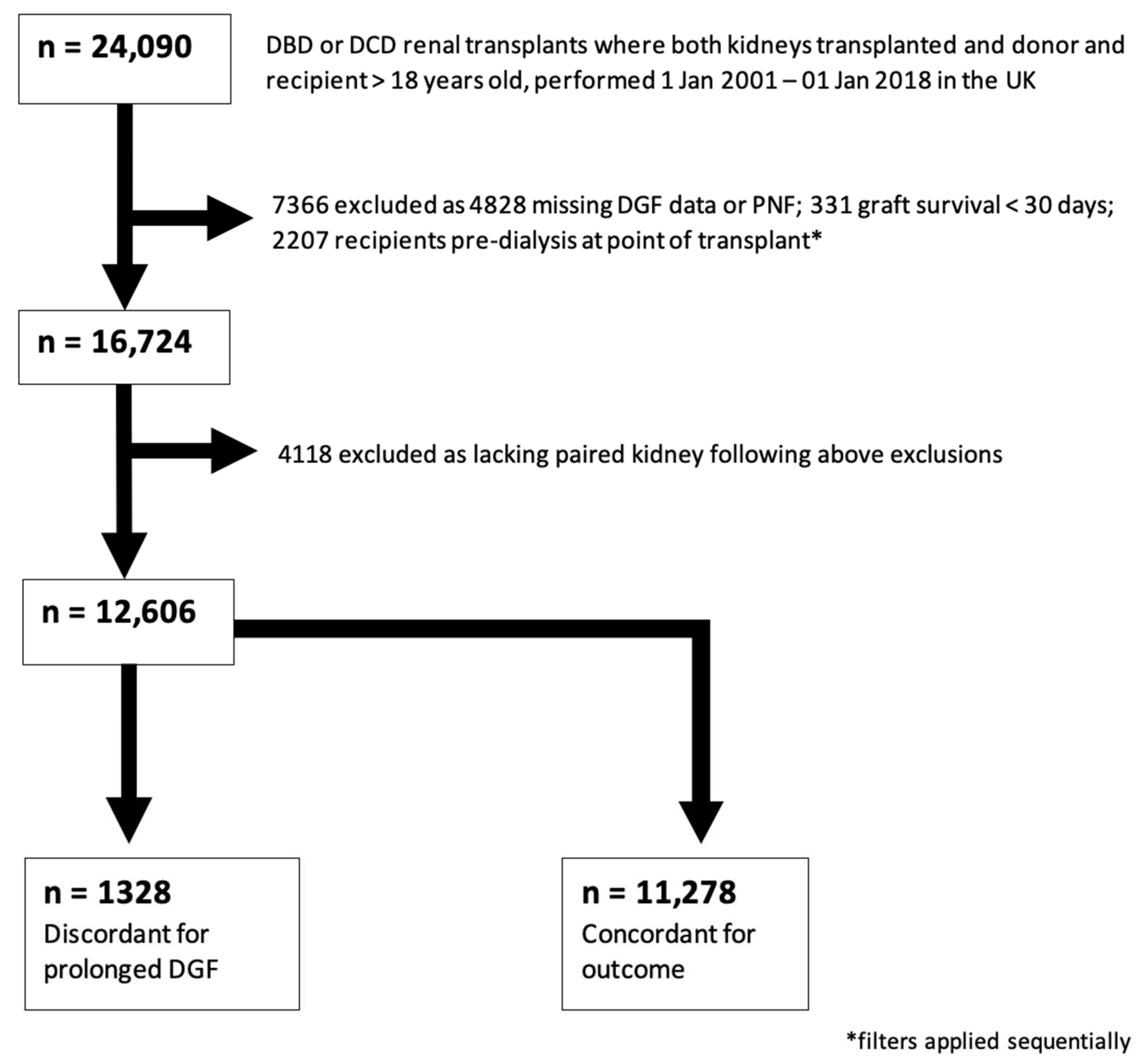
3.3. Prolonged DGF Discordant Pairs
3.3.1. Cohort
3.3.2. Univariate Analysis
3.3.3. Multivariate Analysis
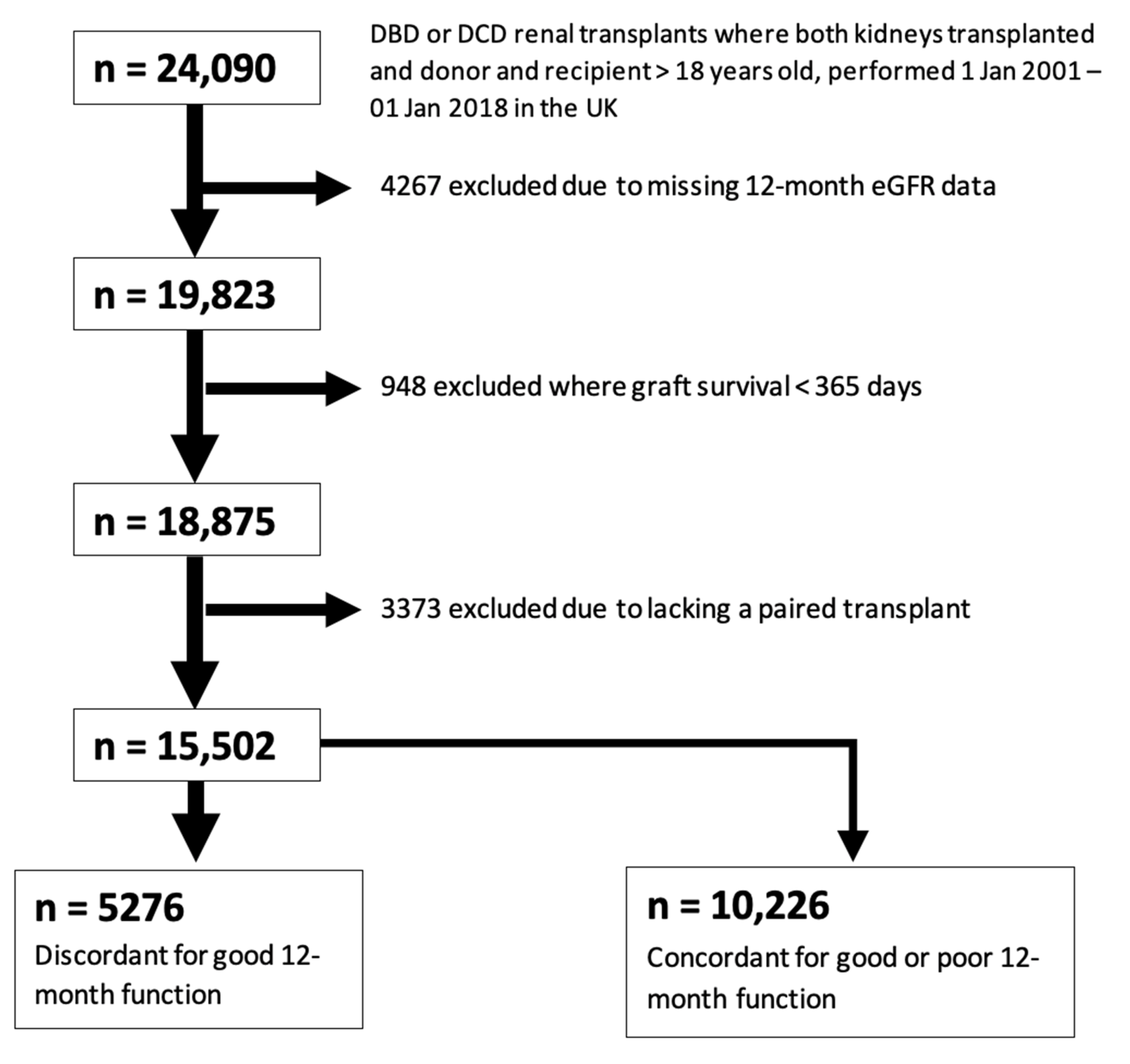
3.4. Graft Function at 12 Months
3.4.1. Cohort
3.4.2. Univariate Analysis
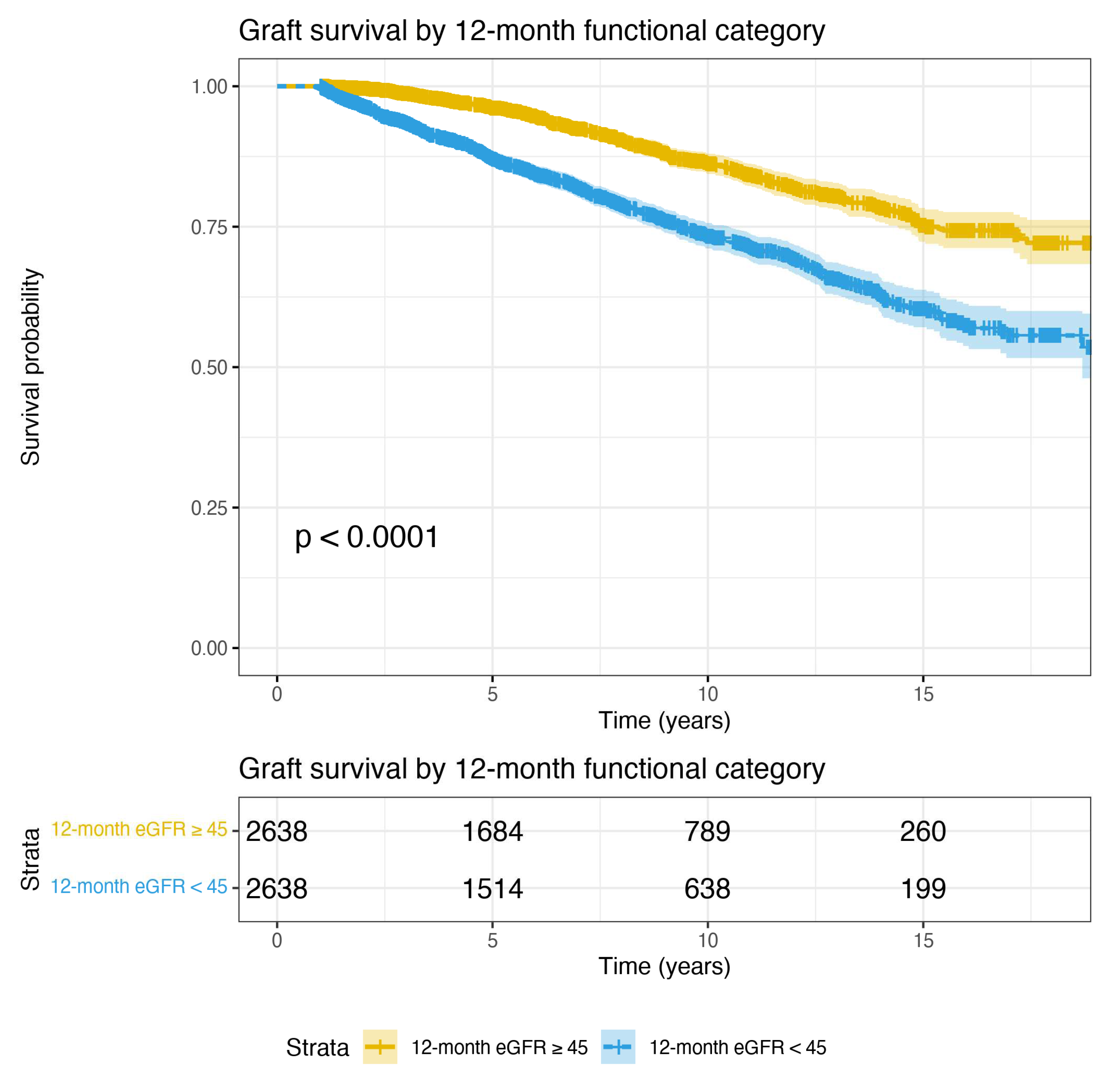
3.4.3. Multivariate and Graft Survival Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| CKD | Chronic Kidney Disease |
| DBD | Donation after Brainstem Death |
| DCD | Donation after Circulatory Death |
| DGF | Delayed Graft Function |
| eGFR | Estimated Glomerular Filtration Rate |
| HD | Haemodialysis |
| HLA | Human Leucocyte Antigen |
| HR | Hazard Ratio |
| IRI | Ischemia Reperfusion Injury |
| KDIGO | Kidney Disease Improving Global Outcomes |
| MICE | Multiple Imputation by Chained Equations |
| OPTN | Organ Procurement and Transplantation Network |
| PD | Peritoneal Dialysis |
| PNF | Primary Non-Function |
| UK | United Kingdom |
| USRDS | United States Renal Data System |
References
- Quiroga, I.; McShane, P.; Koo, D.D.H.; Gray, D.; Friend, P.J.; Fuggle, S.; Darby, C. Major effects of delayed graft function and cold ischaemia time on renal allograft survival. Nephrol. Dial. Transplant. 2006, 21, 1689–1696. [Google Scholar] [CrossRef]
- Avigan, Z.M.; Singh, N.; Kliegel, J.A.; Weiss, M.; Moeckel, G.W.; Cantley, L.G. Tubular cell dropout in preimplantation deceased donor biopsies as a predictor of delayed graft function. Transplant. Direct 2021, 7, e716. [Google Scholar] [CrossRef]
- Cherukuri, A.; Mehta, R.; Sood, P.; Hariharan, S. Early allograft inflammation and scarring associate with graft dysfunction and poor outcomes in renal transplant recipients with delayed graft function: A prospective single center cohort study. Transpl. Int. 2018, 31, 1369–1379. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.J.; Bradbury, L.L.; Martin, K.; Neuberger, J. Organ donation and transplantation in the UK-The last decade: A report from the UK national transplant registry. Transplantation 2014, 97, S1–S27. [Google Scholar] [CrossRef]
- Rao, P.S.; Schaubel, D.E.; Guidinger, M.K.; Andreoni, K.A.; Wolfe, R.A.; Merion, R.M.; Port, F.K.; Sung, R.S. A comprehensive risk quantification score for deceased donor kidneys: The kidney donor risk index. Transplantation 2009, 88, 231–236. [Google Scholar] [CrossRef]
- Senanayake, S.; Kularatna, S.; Healy, H.; Graves, N.; Baboolal, K.; Sypek, M.P.; Barnett, A. Development and validation of a risk index to predict kidney graft survival: The kidney transplant risk index. BMC Med. Res. Methodol. 2021, 21, 127. [Google Scholar] [CrossRef]
- Sureshkumar, K.K.; Chopra, B.; Josephson, M.A.; Shah, P.B.; McGill, R.L. Recipient Obesity and Kidney Transplant Outcomes: A Mate-Kidney Analysis. Am. J. Kidney Dis. 2021, 78, 501–510. [Google Scholar] [CrossRef]
- Bresnahan, B.A.; Johnson, C.P.; McIntosh, M.J.; Stablein, D.; Hariharana, S. A comparison between recipients receiving matched kidney and those receiving mismatched kidney from the same cadaver donor. Am. J. Transplant. 2002, 2, 366–372. [Google Scholar] [CrossRef]
- Lim, W.H.; McDonald, S.P.; Russ, G.R.; Chapman, J.R.; Ma, M.K.M.; Pleass, H.; Jaques, B.; Wong, G. Association between delayed graft function & graft loss in donation after cardiac death kidney transplants—A paired kidney registry analysis. Transplantation 2017, 101, 1139–1143. [Google Scholar]
- Louvar, D.W.; Li, N.; Snyder, J.; Peng, Y.; Kasiske, B.L.; Israni, A.K. “Nature versus nurture” study of deceased-donor pairs in kidney transplantation. J. Am. Soc. Nephrol. 2009, 20, 1351–1358. [Google Scholar] [CrossRef] [Green Version]
- Kerr, K.F.; Morenz, E.R.; Thiessen-Philbrook, H.; Coca, S.G.; Wilson, F.P.; Reese, P.P.; Parikh, C.R. Quantifying Donor Effects on Transplant Outcomes Using Kidney Pairs from Deceased Donors. Clin. J. Am. Soc. Nephrol. 2019, 14, 1781–1787. [Google Scholar] [CrossRef] [PubMed]
- Cosio, F.G.; Qiu, W.; Henry, M.L.; Falkenhain, M.E.; Elkhammas, E.A.; Davies, E.A.; Bumgardner, G.L.; Ferguson, R.M. Factors related to the donor organ are major determinants of renal allograft function and survival. Transplantation 1996, 62, 1571–1576. [Google Scholar] [CrossRef] [PubMed]
- Traynor, C.; O’Kelly, P.; Denton, M.; Magee, C.; Conlon, P.J. Concordance of outcomes of pairs of kidneys transplanted into different recipients. Transpl. Int. 2012, 25, 918–924. [Google Scholar] [CrossRef]
- Nagaraja, P.; Roberts, G.W.; Stephens, M.; Horvath, S.; Fialova, J.; Chavez, R.; Asderakis, A.; Kaposztas, Z. Influence of delayed graft function and acute rejection on outcomes after kidney transplantation from donors after cardiac death. Transplantation 2012, 94, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.P.; Farney, A.C.; Rogers, J.; Zuckerman, J.; Reeves-Daniel, A.; Hartmann, E.; Iskandar, S.; Adams, P.; Stratta, R.J. Kidney transplantation from donation after cardiac death donors: Lack of impact of delayed graft function on post-transplant outcomes. Clin. Transplant. 2011, 25, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Siedlecki, A.; Irish, W.; Brennan, D.C. Delayed graft function in the kidney transplant. Am. J. Transplant. 2011, 11, 2279–2296. [Google Scholar] [CrossRef] [Green Version]
- Phillips, B.L.; Ibrahim, M.; Greenhall, G.H.B.; Mumford, L.; Dorling, A.; Callaghan, C.J. Effect of delayed graft function on longer-term outcomes after kidney transplantation from donation after circulatory death donors in the United Kingdom: A national cohort study. Am. J. Transplant. 2021, 21, 3346–3355. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Robinson, C. Kidney Transplantation: Deceased Donor Organ Allocation. Policy POL186/10. 9 June 2019. Available online: https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/16915/kidney-allocation-policy-pol186.pdf (accessed on 11 April 2022).
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Alam, A.; Soo, A.P.; George, A.J.T.; Ma, D. Ischemia-Reperfusion Injury Reduces Long Term Renal Graft Survival: Mechanism and Beyond. EBioMedicine 2018, 28, 31–42. [Google Scholar] [CrossRef] [Green Version]
- Vonbrunn, E.; Ries, T.; Söllner, S.; Müller-Deile, J.; Büttner-Herold, M.; Amann, K.; Daniel, C. Multiplex gene analysis reveals T-cell and antibody-mediated rejection-specific upregulation of complement in renal transplants. Sci. Rep. 2021, 11, 15464. [Google Scholar] [CrossRef] [PubMed]
- Franzin, R.; Stasi, A.; Fiorentino, M.; Stallone, G.; Cantaluppi, V.; Gesualdo, L.; Castellano, G. Inflammaging and Complement System: A Link Between Acute Kidney Injury and Chronic Graft Damage. Front. Immunol. 2020, 11, 734. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Curwood, V.; White, S.A.; Furness, P.N.; Nicholson, M.L. Sub-clinical acute rejection detected using protocol biopsies in patients with delayed graft function. Transpl. Int. 2000, 13, S52–S55. [Google Scholar] [CrossRef]
- Pontrelli, P.; Cariello, M.; Rascio, F.; Gigante, M.; Verrienti, R.; Tataranni, T.; Castellano, G.; Divella, C.; Ranieri, E.; Stallone, G.; et al. Thrombin may modulate dendritic cell activation in kidney transplant recipients with delayed graft function. Nephrol. Dial. Transplant. 2015, 30, 1480–1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauzurica, R.; Pastor, M.C.; Bayés, B.; Hernández, J.M.; Bonet, J.; Doladé, M.; Navarro, M.; Romero, R. Pretransplant inflammation: A risk factor for delayed graft function? J. Nephrol. 2008, 21, 221–228. [Google Scholar] [PubMed]
- Tang, M.; Li, T.; Liu, H. A comparison of transplant outcomes in peritoneal and hemodialysis patients: A meta-analysis. Blood Purif. 2016, 42, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Van Biesen, W.; Vanholder, R.; Van Loo, A.; Van Der Vennet, M.; Lameire, N. Peritoneal dialysis favorably influences early graft function after renal transplantation compared to hemodialysis. Transplantation 2000, 69, 508–514. [Google Scholar] [CrossRef]
- Kulkarni, S.; Wei, G.; Jiang, W.; Lopez, L.A.; Parikh, C.R.; Hall, I.E. Outcomes From Right Versus Left Deceased-Donor Kidney Transplants: A US National Cohort Study. Am. J. Kidney Dis. 2020, 75, 725–735. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | DGF < 14 Days or Primary Function | Prolonged DGF | p-Value for the Difference |
|---|---|---|---|
| N | 664 | 664 | - |
| Donor age, years, mean (sd) | 52.5 (13.8) | 52.5 (13.8) | - |
| Donor sex, male, n (%) | 414 (62.3) | 414 (62.3) | - |
| Donor BMI, mean (sd) | 27.2 (5.0) | 27.2 (5.0) | - |
| Donor type, DCD, n (%) | 321 (48.3) | 321 (48.3) | - |
| Donor creatinine at retrieval | 93.1 (69.7) | 93.1 (69.7) | - |
| Donor side, right, n (%) | 334 (50.3) | 330 (49.7) | 0.87 |
| HLA mismatch group, n (%) | 0.001 | ||
| Group 1 | 57 (8.6) | 39 (5.9) | |
| Group 2 | 249 (37.5) | 198 (29.8) | |
| Group 3 | 297 (44.7) | 361 (54.4) | |
| Group 4 | 61 (9.2) | 66 (9.9) | |
| Cold ischaemic time, hours, mean (sd) | 15.8 (5.3) | 17.2 (5.9) | <0.001 |
| Recipient age, years, mean (sd) | 52.1 (13.1) | 52.2 (13.0) | 0.90 |
| Recipient sex, male, n (%) | 420 (63.3) | 434 (65.4) | 0.46 |
| Recipient BMI, mean (sd) | 26.6 (4.7) | 27.4 (4.9) | 0.01 |
| Recipient dialysis modality PD at transplant, n (%) | 205 (30.9) | 123 (18.5) | <0.001 |
| Recipient diabetes, n (%) | 52 (7.8) | 79 (11.9) | 0.02 |
| Recipient wait-time, years, mean (sd) | 2.7 (2.3) | 3.3 (2.8) | <0.001 |
| Retransplant, YES, n (%) | 73 (11.0) | 128 (19.3) | <0.001 |
| Highly sensitised recipient, n (%) | 45 (6.8) | 66 (10) | 0.045 |
| HLA incompatible transplant, n (%) | 3 (0.5) | 18 (2.7) | 0.002 |
| Tacrolimus at transplant, n (%) | 546 (82.4) | 523 (78.9) | 0.13 |
| Prednisolone at transplant, n (%) | 558 (84.0) | 551 (83.1) | 0.70 |
| Parameter | OR (95% CI) | Significance (p-Value) |
|---|---|---|
| Mismatch group 1 (reference) | - | - |
| Mismatch group 2 | 2.59 (1.16–5.78) | 0.02 |
| Mismatch group 3 | 3.3 (1.45–7.52) | <0.01 |
| Mismatch group 4 | 2.92 (1.11–7.69) | 0.01 |
| Cold Ischaemia Time (hours) | 1.06 (1.04–1.09) | <0.01 |
| Waitlist time (years) | 1.12 (1.04–1.21) | <0.01 |
| Recipient age (years) | 1.01 (0.99–1.02) | 0.26 |
| Recipient sex (male) | 1.18 (0.91–1.54) | 0.21 |
| Recipient BMI (units) | 1.02 (1.00–1.05) | 0.06 |
| Recipient dialysis type (PD) | 0.53 (0.39–0.72) | <0.01 |
| Recipient diabetes | 1.68 (1.09–2.59) | 0.02 |
| Recipient previous renal transplant | 2.40 (1.53–3.78) | <0.01 |
| Recipient rejection within 14 days | 2.47 (1.65–3.69) | <0.01 |
| Recipient highly sensitised | 1.30 (0.70–2.42) | 0.40 |
| Donor organ side (right) | 1.08 (0.90–1.29) | 0.42 |
| HLA incompatible transplant | 3.26 (0.88–12.06) | 0.08 |
| Tacrolimus at transplant | 0.56 (0.36–0.88) | 0.01 |
| Prednisolone at transplant | 0.76 (0.49–1.19) | 0.23 |
| 12-Month eGFR > 45 mL/min/1.73 m2 | 12-Month eGFR < 45 mL/min/1.73 m2 | p-Value for the Difference | |
|---|---|---|---|
| n | 2595 | 2595 | - 1 |
| Donor age, years, mean (sd) | 51.68 (12.87) | 51.68 (12.87) | - 1 |
| Donor sex, male, n (%) | 1345 (51.8) | 1345 (51.8) | - 1 |
| Donor BMI, mean (sd) | 26.90 (5.27) | 26.90 (5.27) | - 1 |
| Donor type, DCD, n (%) | 815 (31.4) | 825 (31.3) | - 1 |
| Donor creatinine at retrieval | 85.06 (47.81) | 85.06 (47.81) | - 1 |
| HLA mismatch group, n (%) | 0.968 2 | ||
| Group 1 | 339 (13.1) | 339 (13.1) | |
| Group 2 | 973 (37.5) | 959 (37.0) | |
| Group 3 | 1098 (42.3) | 1115 (43.0) | |
| Group 4 | 185 (7.1) | 182 (7.0) | |
| Cold ischaemic time, hours, mean (sd) | 16.28 (5.82) | 16.55 (5.76) | 0.099 3 |
| Recipient age, years, mean (sd) | 50.60 (13.19) | 50.90 (12.29) | 0.404 3 |
| Recipient sex, male, n (%) | 1725 (66.5) | 1492 (57.5) | <0.001 2 |
| Recipient BMI, mean (sd) | 25.98 (4.56) | 26.98 (4.88) | <0.001 3 |
| Recipient dialysis modality at transplant, n (%) | 0.538 2 | ||
| HD | 1653 (64.0) | 1617 (62.6) | |
| PD | 658 (25.5) | 677 (26.2) | |
| Predialysis | 273 (10.6) | 291 (11.3) | |
| Recipient diabetes, n (%) | 222 (8.6) | 203 (7.8) | 0.362 2 |
| Recipient wait-time, years, mean (sd) | 2.67 (2.31) | 2.74 (2.48) | 0.287 3 |
| Retransplant, YES, n (%) | 337 (13.0) | 393 (15.1) | 0.028 2 |
| Highly sensitised recipient, n (%) | 195 (7.6) | 239 (9.3) | 0.033 2 |
| Donor kidney side, right, n (%) | 1360 (52.4) | 1235 (47.6) | 0.001 2 |
| HLA incompatible transplant, n (%) | 15 (0.6) | 27 (1.0) | 0.088 2 |
| Prolonged DGF, n (%) | 85 (3.9) | 159 (7.2) | <0.001 2 |
| Tacrolimus at transplant, n (%) | 2045 (79.0) | 1932 (74.6) | <0.001 2 |
| Prednisolone at transplant, n (%) | 2229 (86.1) | 2168 (83.7) | 0.018 2 |
| Parameter | Odds Ratio (95% CI) | p-Value for the Difference |
|---|---|---|
| Prolonged DGF | 2.03 (1.49–2.78) | <0.01 |
| HLA mismatch group 1 (reference) | - | - |
| Group 2 | 1.05 (0.80–1.39) | 0.71 |
| Group 3 | 1.04 (0.78–1.39) | 0.80 |
| Group 4 | 1.01 (0.69–1.49) | 0.95 |
| Cold ischaemia time (hours) | 1.01 (1.00–1.02) | 0.11 |
| Waitlist time (years) | 1.00 (0.97–1.04) | 0.77 |
| Recipient age (years) | 1 (1.00–1.01) | 0.28 |
| Recipient sex (male) | 0.66 (0.58–0.74) | <0.01 |
| Recipient BMI (units) | 1.02 (1.00–1.05) | 0.03 |
| Recipient dialysis type, HD (reference) | - | - |
| PD | 1.05 (0.91–1.20) | 0.52 |
| Predialysis | 1.19 (0.97–1.44) | 0.09 |
| Recipient diabetes | 0.88 (0.71–1.09) | 0.25 |
| Recipient—retransplant | 1.29 (1.07–1.56) | 0.01 |
| Recipient—highly sensitised | 1.12 (0.86–1.46) | 0.40 |
| Donor kidney right (reference left) | 0.91 (0.84–0.99) | 0.03 |
| HLA incompatible transplant | 1.42 (0.74–2.73) | 0.29 |
| Rejection episode within 14 days | 1.66 (1.31–2.11) | <0.01 |
| Tacrolimus use at transplant | 0.6 (0.5–0.73) | <0.01 |
| Prednisolone use at transplant | 0.72 (0.59–0.88) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dumbill, R.; Jaques, R.; Robb, M.; Johnson, R.; Ploeg, R.J.; Kaisar, M.E.; Sharples, E.J. Transplant and Recipient Factors in Prediction of Kidney Transplant Outcomes: A UK-Wide Paired Analysis. J. Clin. Med. 2022, 11, 2222. https://doi.org/10.3390/jcm11082222
Dumbill R, Jaques R, Robb M, Johnson R, Ploeg RJ, Kaisar ME, Sharples EJ. Transplant and Recipient Factors in Prediction of Kidney Transplant Outcomes: A UK-Wide Paired Analysis. Journal of Clinical Medicine. 2022; 11(8):2222. https://doi.org/10.3390/jcm11082222
Chicago/Turabian StyleDumbill, Richard, Roderick Jaques, Matthew Robb, Rachel Johnson, Rutger J. Ploeg, Maria E. Kaisar, and Edward J. Sharples. 2022. "Transplant and Recipient Factors in Prediction of Kidney Transplant Outcomes: A UK-Wide Paired Analysis" Journal of Clinical Medicine 11, no. 8: 2222. https://doi.org/10.3390/jcm11082222