
The Impact of Cold Ischaemia Time on Outcomes of Living Donor Kidney Transplantation: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Outcome Parameters
2.3. Literature Screening
2.4. Data Extraction and Critical Appraisal
2.5. Statistical Analysis
3. Results
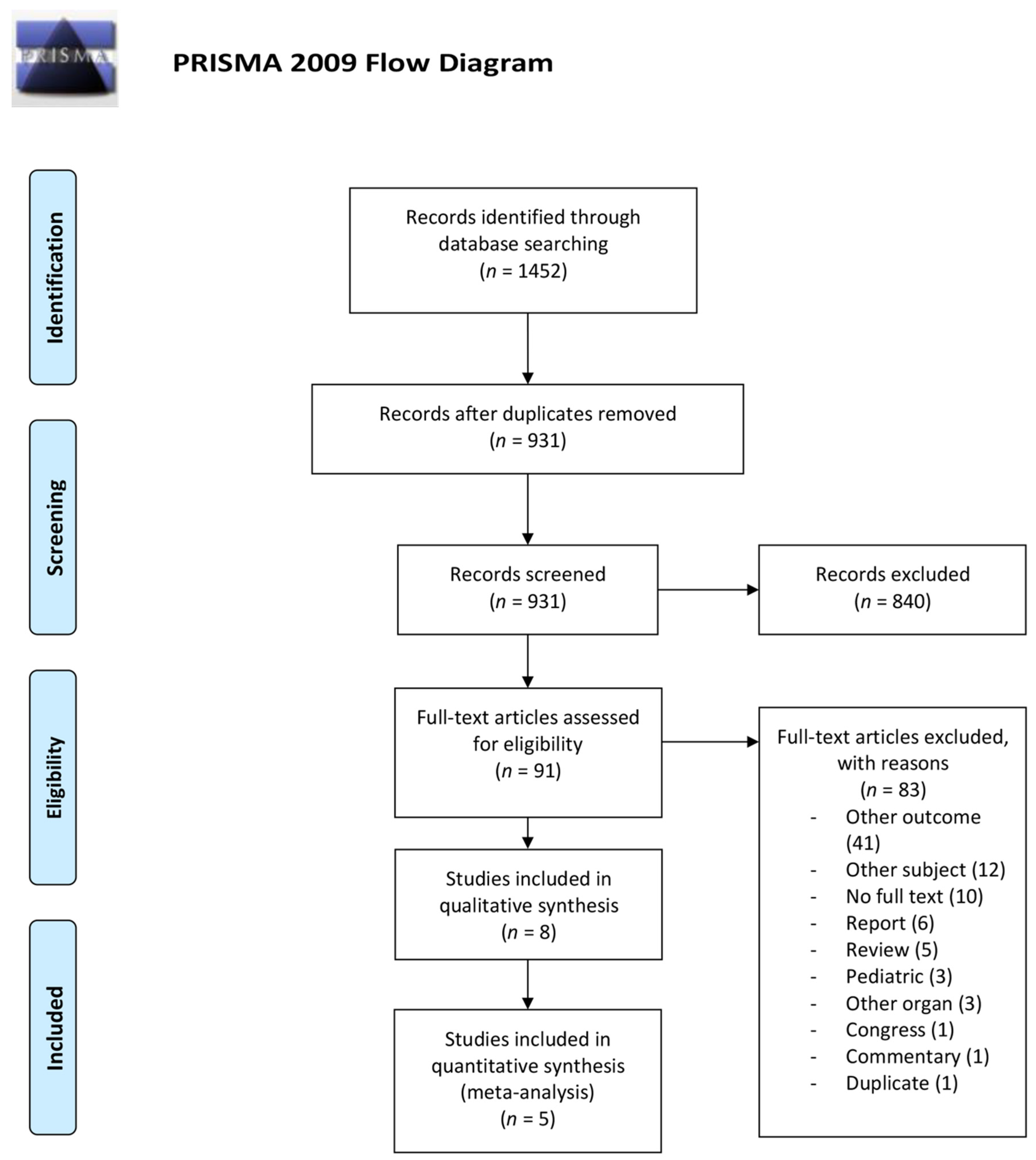
3.1. Literature Search Results
3.2. Outcomes
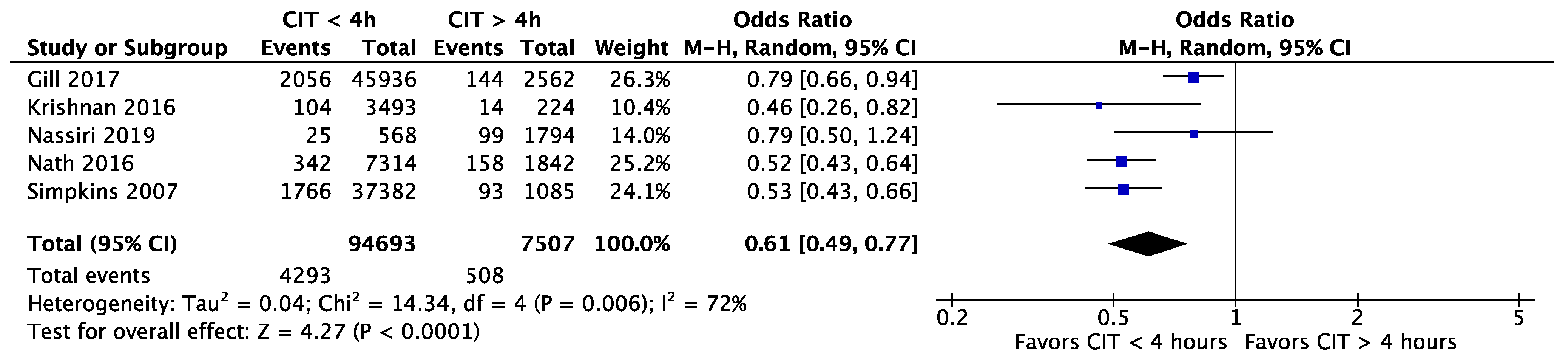
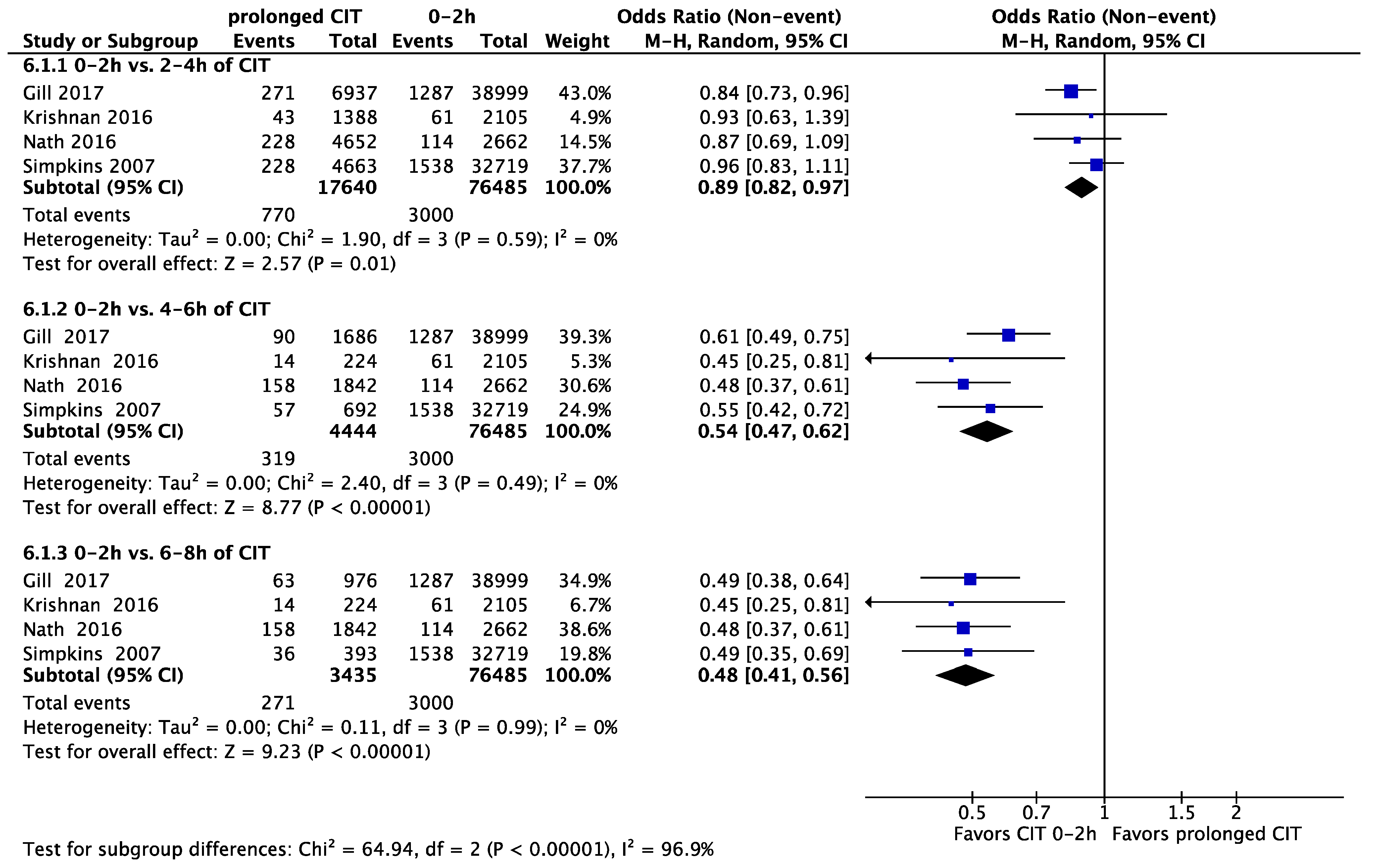
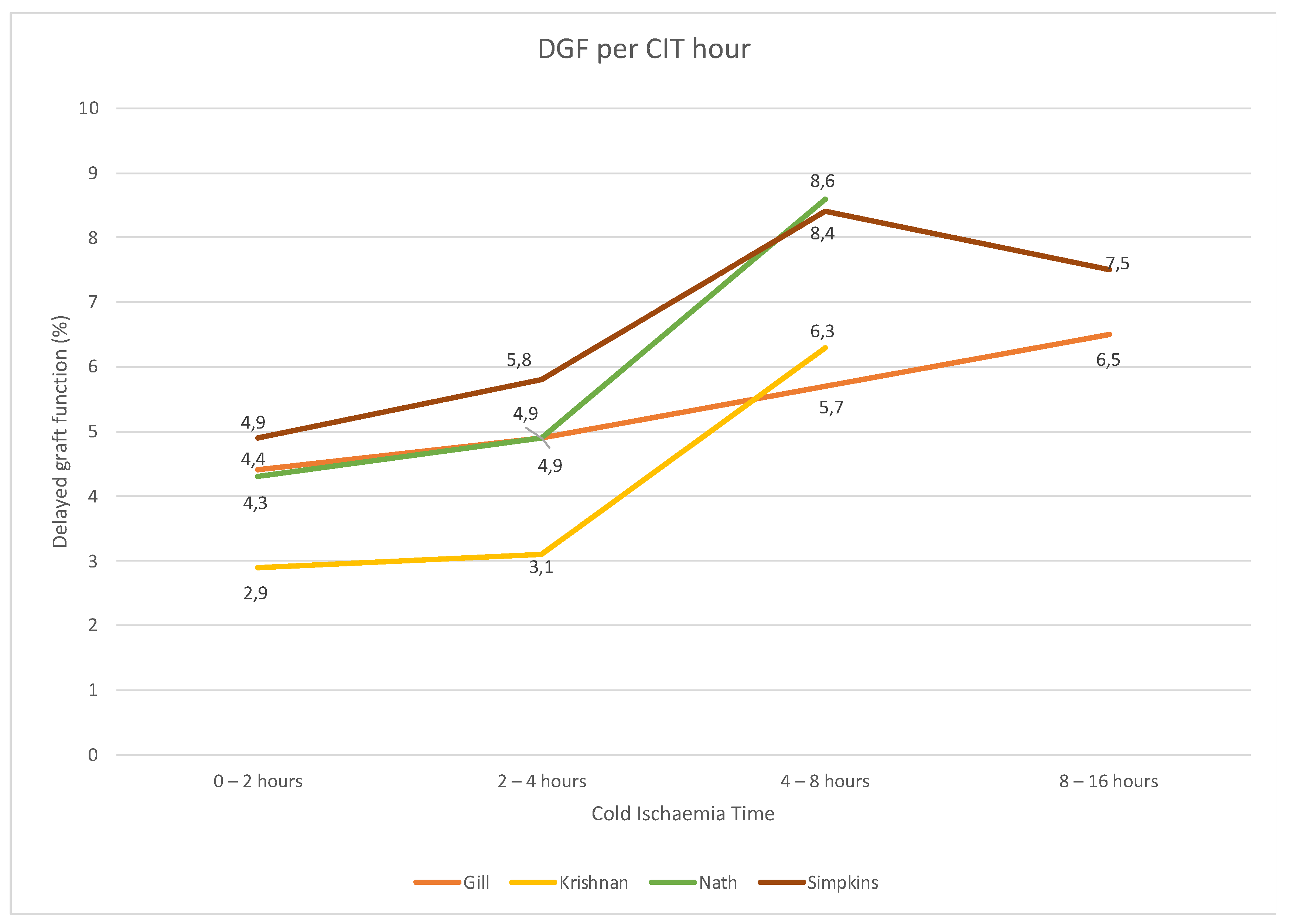
Delayed Graft Function
3.3. Graft Survival
3.3.1. One Year
3.3.2. Five Years
3.4. Five-Year Graft Survival Hazard Ratio
3.5. Ten-Year Graft Survival
3.6. Patient Survival
3.7. Acute Rejection
3.8. Kidney Function
3.9. Impact of CIT in Kidney Exchange Programmes (KEP)
3.10. Quality and Risk of Bias Assessment
3.11. Publication Bias
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A
- Embase.com (accessed on 12 July 2021) (603)
- Medline (Ovid) (339)
- Web of Science (318)
- Cochrane CENTRAL (47)
- Google Scholar 100 Top-Ranked
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Certainty Assessment | Patients (n) | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | a CIT <4 h | >4 h | Relative (95% CI) | Absolute (95% CI) | |
| 5 | observational studies | not serious | serious a | not serious | not serious | none | 4293/94,693 (4.5%) | 508/7507 (6.8%) | OR 0.61 (0.49 to 0.77) | 25 fewer per 1000 (from 33 fewer to 15 fewer) | ⨁⨁⨁◯ Moderate |
| Certainty Assessment | Patients (n) | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | a CIT <4 h | >4 h | Relative (95% CI) | Absolute (95% CI) | |
| 2 | observational studies | not serious | serious a | not serious | serious b | all plausible residual confounding would reduce the effect | 1664/44,696 (3.7%) | 132/2927 (4.5%) | OR 0.72 (0.60 to 0.87) | 12 fewer per 1000 (from 18 fewer to 6 fewer) | ⨁⨁⨁◯ Moderate |
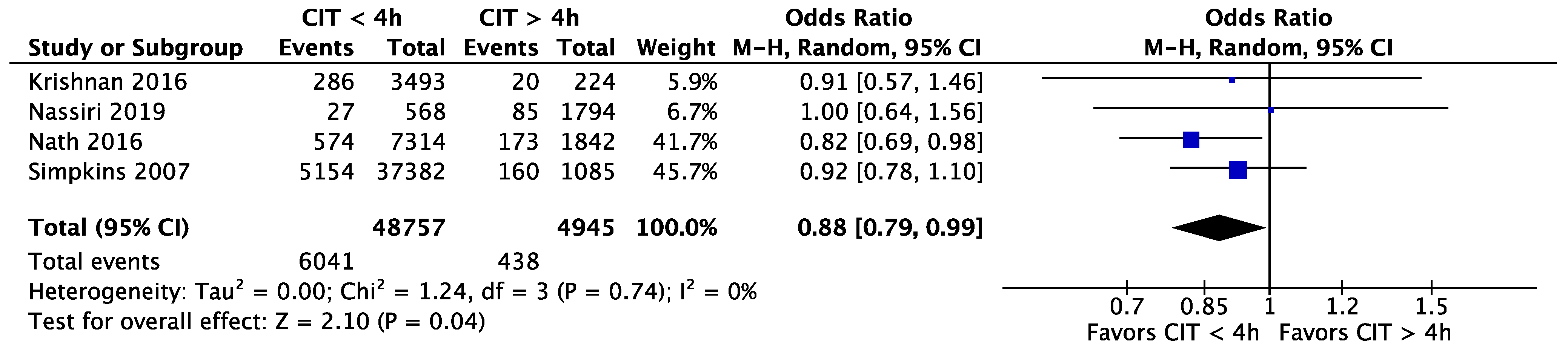
| 4 | observational studies | not serious | not serious | not serious | not serious | none | 6041/48,757 (12.4%) | 438/4945 (8.9%) | OR 0.88 (0.79 to 0.99) | 10 fewer per 1000 (from 17 fewer to 1 fewer) | ⨁⨁⨁⨁ High |
| Certainty Assessment | Patients (n) | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | a CIT <4 h | >4 h | Relative (95% CI) | Absolute (95% CI) | |
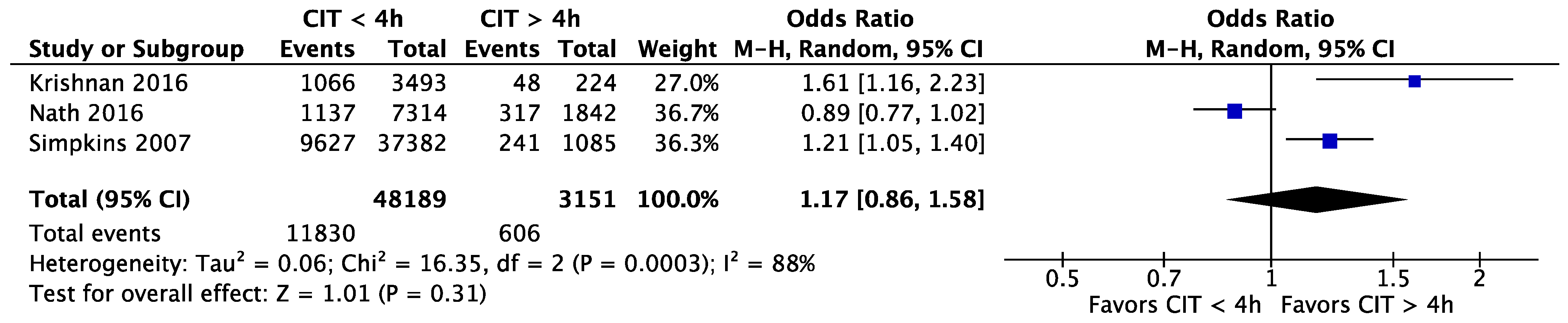
| 3 | observational studies | not serious | serious a | not serious | serious b | none | 11,830/48,189 (24.5%) | 606/3151 (19.2%) | OR 1.17 (0.86 to 1.58) | 26 more per 1000 (from 22 fewer to 81 more) | ⨁⨁◯◯ Low |
| Certainty Assessment | Patients (n) | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | a CIT <4 h | >4 h | Relative (95% CI) | Absolute (95% CI) | |
| 2 | observational studies | not serious | serious a | not serious | serious b | all plausible residual confounding would reduce the demonstrated effect | 319/10,753 (3.0%) | 43/2066 (2.1%) | OR 0.74 (0.51 to 1.07) | 5 fewer per 1000 (from 10 fewer to 1 more) | ⨁⨁⨁◯ Moderate |
| 2 | observational studies | not serious | very serious c | not serious | serious b | all plausible residual confounding would reduce the demonstrated effect | 424/10,807 (3.9%) | 105/2066 (5.1%) | OR 0.54 (0.20 to 1.45) | 23 fewer per 1000 (from 40 fewer to 21 more) | ⨁⨁◯◯ Low |
| Certainty Assessment | Patients (n) | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | 0–2 h of CIT | Prolonged CIT | Relative (95% CI) | Absolute (95% CI) | |
| 4 | observational studies | not serious | not serious | not serious | not serious | none | 770/17,640 (4.4%) | 2–4 h: 3000/76,485 (3.9%) | OR 0.89 (0.82 to 0.97) | 4 fewer per 1000 (from 7 fewer to 1 fewer) | ⨁⨁⨁⨁ High |
| 4 | observational studies | not serious | not serious | not serious | not serious | none | 319/4444 (7.2%) | 4–6 h: 3000/76,485 (3.9%) | OR 0.54 (0.47 to 0.62) | 18 fewer per 1000 (from 20 fewer to 15 fewer) | ⨁⨁⨁⨁ High |
| 4 | observational studies | not serious | not serious | not serious | not serious | strong association | 271/3435 (7.9%) | 6–8 h: 3000/76,485 (3.9%) | OR 0.48 (0.41 to 0.56) | 20 fewer per 1000 (from 23 fewer to 17 fewer) | ⨁⨁⨁⨁ High |
| Certainty Assessment | Patients (n) | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | 0–2 h of CIT | Prolonged CIT | Relative (95% CI) | Absolute (95% CI) | |
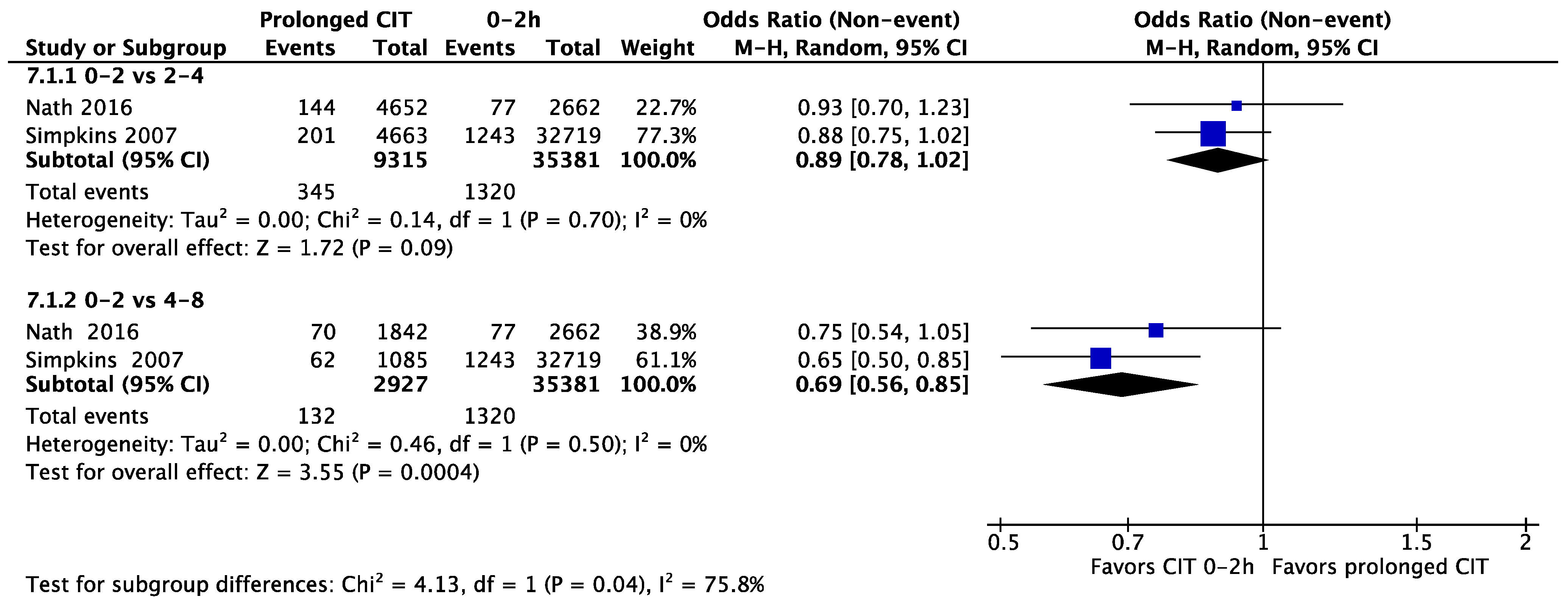
| 2 | observational studies | not serious | not serious | not serious | serious a | none | 345/9315 (3.7%) | 1320/35,381 (3.7%) | OR 0.89 (0.78 to 1.02) | 4 fewer per 1000 (from 8 fewer to 1 more) | ⨁⨁⨁◯ Moderate |
| 2 | observational studies | not serious | not serious | not serious | serious a | none | 132/2927 (4.5%) | 1320/35,381 (3.7%) | OR 0.69 (0.56 to 0.85) | 11 fewer per 1000 (from 16 fewer to 5 fewer) | ⨁⨁⨁◯ Moderate |
| Certainty Assessment | Patients (n) | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | 0–2 h of CIT | Prolonged CIT | Relative (95% CI) | Absolute (95% CI) | |
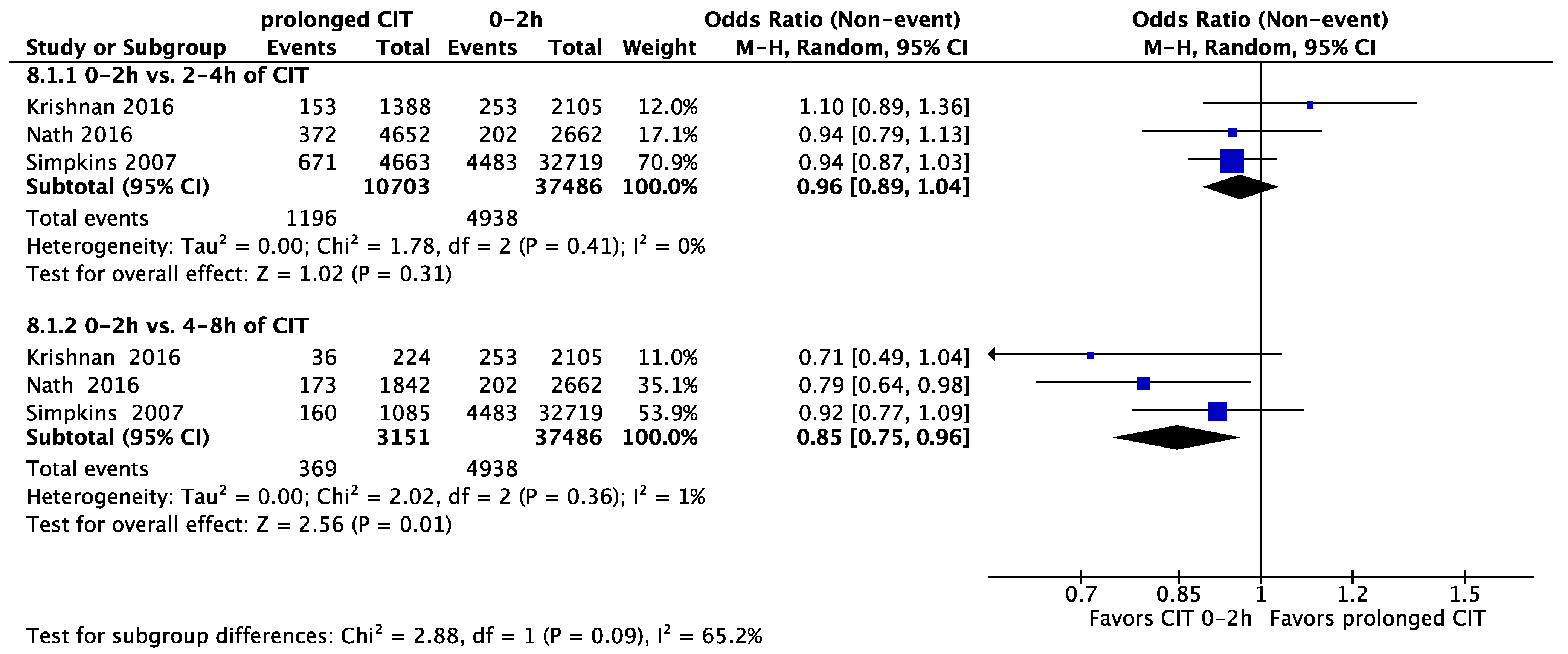
| 3 | observational studies | not serious | not serious | not serious | serious a | none | 1196/10,703 (11.2%) | 2–4 h: 4938/37,486 (13.2%) | OR 0.96 (0.89 to 1.04) | 5 fewer per 1000 (from 13 fewer to 5 more) | ⨁⨁⨁◯ Moderate |
| 3 | observational studies | not serious | not serious | not serious | serious b | none | 369/3151 (11.7%) | 4–8 h: 4938/37,486 (13.2%) | OR 0.85 (0.75 to 0.96) | 18 fewer per 1000 (from 30 fewer to 5 fewer) | ⨁⨁⨁◯ Moderate |
| Certainty Assessment | Patients (n) | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | CIT of <4 h | >4 h | Relative (95% CI) | Absolute (95% CI) | |
| 2 | observational studies | not serious | serious a | not serious | serious b | all plausible residual confounding would reduce the demonstrated effect | 429/1309 (32.8%) | 12,503/40,821 (30.6%) | OR 0.84 (0.64 to 1.09) | 36 fewer per 1000 (from 86 fewer to 19 more) | ⨁⨁⨁◯ Moderate |
References
- Clemens, K.K.; Thiessen-Philbrook, H.; Parikh, C.R.; Yang, R.C.; Karley, M.L.; Boudville, N.; Ramesh Prasad, G.V.; Garg, A.X.; Donor Nephrectomy Outcomes Research (DONOR) Network. Psychosocial Health of Living Kidney Donors: A Systematic Review. Am. J. Transplant. 2006, 6, 2965–2977. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Snyder, J.; Matas, A.; Collins, A. The impact of transplantation on survival with kidney failure. Clin. Transpl. 2000, 135–143. [Google Scholar] [PubMed]
- Lafranca, J.A.; Hesselink, D.A.; Dor, F.J.M.F. Oxford Textbook of Urological Surgery; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Clarkson, A.; Forsythe, J.L.; Gardiner, D. Transplant Activity in the UK, 2020–2021; National Health Service Blood and Transplant: Bristol, UK, 2021. [Google Scholar]
- Lumsdaine, J.A.; Wray, A.; Power, M.J.; Jamieson, N.V.; Akyol, M.; Andrew Bradley, J.; Forsythe, J.L.R.; Wigmore, S.J. Higher quality of life in living donor kidney transplantation: Prospective cohort study. Transpl. Int. 2005, 18, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Knoll, G.; Bello, A.; Browne, S.; Jadhav, D.; Klarenbach, S.; Gill, J. Systematic Review: Kidney Transplantation Compared With Dialysis in Clinically Relevant Outcomes. Am. J. Transplant. 2011, 11, 2093–2109. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, S.; Johnson, C.P.; Bresnahan, B.A.; Taranto, S.E.; McIntosh, M.J.; Stablein, D. Improved Graft Survival after Renal Transplantation in the United States, 1988 to 1996. N. Engl. J. Med. 2000, 342, 605–612. [Google Scholar] [CrossRef] [PubMed]
- van Dellen, D.; Burnapp, L.; Citterio, F.; Mamode, N.; Moorlock, G.; van Assche, K.; Zuidema, W.C.; Lennerling, A.; Dor, F.J. Pre-emptive live donor kidney transplantation-moving barriers to opportunities: An ethical, legal and psychological aspects of organ transplantation view. World J. Transpl. 2021, 11, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.; Pleass, H.; Clayton, P.A.; Woodroffe, C.; Ferrari, P. Outcomes of kidney paired donation transplants in relation to shipping and cold ischaemia time. Transpl. Int. 2016, 29, 425–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhargava, A.; Arora, S.; Marcus, R.J.; Sureshkumar, K.K. Outcomes of Paired-Exchange Live-Donor Kidney Transplantation: A Single-Center Experience. Transplant. Proc. 2014, 46, 3420–3422. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.; Rose, C.; Joffres, Y.; Kadatz, M.; Gill, J. Cold ischemia time up to 16 h has little impact on living donor kidney transplant outcomes in the era of kidney paired donation. Kidney Int. 2017, 92, 490–496. [Google Scholar] [CrossRef]
- Debout, A.; Foucher, Y.; Trébern-Launay, K.; Legendre, C.; Kreis, H.; Mourad, G.; Garrigue, V.; Morelon, E.; Buron, F.; Rostaing, L.; et al. Each additional hour of cold ischemia time significantly increases the risk of graft failure and mortality following renal transplantation. Kidney Int. 2015, 87, 343–349. [Google Scholar] [CrossRef] [Green Version]
- Lauronen, J.; Peräsaari, J.P.; Saarinen, T.; Jaatinen, T.; Lempinen, M.; Helanterä, I. Shorter Cold Ischemia Time in Deceased Donor Kidney Transplantation Reduces the Incidence of Delayed Graft Function Especially among Highly Sensitized Patients and Kidneys From Older Donors. Transplant. Proc. 2020, 52, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Doshi, M.D.; Garg, N.; Reese, P.P.; Parikh, C.R. Recipient risk factors associated with delayed graft function: A paired kidney analysis. Transplantation 2011, 91, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Kayler, L.K.; Srinivas, T.R.; Schold, J.D. Influence of CIT-induced DGF on kidney transplant outcomes. Am. J. Transpl. 2011, 11, 2657–2664. [Google Scholar] [CrossRef]
- Kayler, L.K.; Magliocca, J.; Zendejas, I.; Srinivas, T.R.; Schold, J.D. Impact of cold ischemia time on graft survival among ECD transplant recipients: A paired kidney analysis. Am. J. Transpl. 2011, 11, 2647–2656. [Google Scholar] [CrossRef] [PubMed]
- Summers, D.M.; Johnson, R.J.; Allen, J.; Fuggle, S.V.; Collett, D.; Watson, C.J.; Bradley, J.A. Analysis of factors that affect outcome after transplantation of kidneys donated after cardiac death in the UK: A cohort study. Lancet 2010, 376, 1303–1311. [Google Scholar] [CrossRef]
- Peters-Sengers, H.; Houtzager, J.H.E.; Idu, M.M.; Heemskerk, M.B.A.; van Heurn, E.L.W.; Homan van der Heide, J.J.; Kers, J.; Berger, S.P.; van Gulik, T.M.; Bemelman, F.J. Impact of Cold Ischemia Time on Outcomes of Deceased Donor Kidney Transplantation: An Analysis of a National Registry. Transpl. Direct 2019, 5, e448. [Google Scholar] [CrossRef]
- van der Vliet, J.A.; Warlé, M.C. The need to reduce cold ischemia time in kidney transplantation. Curr. Opin. Organ Transpl. 2013, 18, 174–178. [Google Scholar] [CrossRef] [PubMed]
- Kranenburg, L.W.; Visak, T.; Weimar, W.; Zuidema, W.; de Klerk, M.; Hilhorst, M.; Passchier, J.; IJzermans, J.N.M.; Busschbach, J.J. Starting a crossover kidney transplantation program in the Netherlands: Ethical and psychological considerations. Transplantation 2004, 78, 194–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Klerk, M.; Ijzermans, J.N.; Kranenburg, L.W.; Hilhorst, M.T.; van Busschbach, J.J.; Weimar, W. Cross-over transplantation; a new national program for living kidney donations. Ned. Tijdschr. Geneeskd. 2004, 148, 420–423. [Google Scholar]
- Andrews, P.; Burnapp, L. Guidelines for Living Donor Kidney Transplantation; British Transplantation Society: London, UK, 2018. [Google Scholar]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.1. 2020. Available online: www.training.cochrane.org/handbook (accessed on 7 October 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. 2013. Available online: Guidelinedevelopment.org/handbook (accessed on 21 May 2021).
- Moher, D.; Cook, D.J.; Eastwood, S.; Olkin, I.; Rennie, D.; Stroup, D.F. Improving the quality of reports of meta-analyses of randomised controlled trials: The QUOROM statement. Quality of Reporting of Meta-analyses. Lancet 1999, 354, 1896–1900. [Google Scholar] [CrossRef]
- Review Manager Web (RevMan Web). 1.22.0. 2020. Available online: Revman.cochrane.org (accessed on 15 November 2021).
- Nassiri, N.; Kwan, L.; Bolagani, A.; Thomas, A.G.; Sinacore, J.; Ronin, M.; Cooper, M.; Segev, D.L.; Cecka, J.M.; Veale, J.L. The “oldest and coldest” shipped living donor kidneys transplanted through kidney paired donation. Am. J. Transpl. 2020, 20, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.R.; Wong, G.; Chapman, J.R.; Coates, P.T.; Russ, G.R.; Pleass, H.; Russell, C.; He, B.; Lim, W.H. Prolonged Ischemic Time, Delayed Graft Function, and Graft and Patient Outcomes in Live Donor Kidney Transplant Recipients. Am. J. Transpl. 2016, 16, 2714–2723. [Google Scholar] [CrossRef] [Green Version]
- Nath, J.; Hodson, J.; Canbilen, S.W.; Al Shakarchi, J.; Inston, N.G.; Sharif, A.; Ready, A.R. Effect of cold ischaemia time on outcome after living donor renal transplantation. Br. J. Surg. 2016, 103, 1230–1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redfield, R.R.; Scalea, J.R.; Zens, T.J.; Muth, B. Predictors and outcomes of delayed graft function after living-donor kidney transplantation. Transpl. Int. 2016, 29, 81–87. [Google Scholar] [CrossRef]
- Roodnat, J.I.; Van Riemsdijk, I.C.; Mulder, P.G.H.; Doxiadis, I.; Claas, F.H.J.; Ijzermans, J.N.M.; Van Gelder, T.; Weimar, W. The superior results of living-donor renal transplantation are not completely caused by selection or short cold ischemia time: A single-center, multivariate analysis. Transplantation 2003, 75, 2014–2018. [Google Scholar] [CrossRef] [PubMed]
- Segev, D.L.; Veale, J.L.; Berger, J.C.; Hiller, J.M.; Hanto, R.L.; Leeser, D.B.; Geffner, S.R.; Shenoy, S.; Bry, W.I.; Katznelson, S.; et al. Transporting live donor kidneys for kidney paired donation: Initial national results. Am. J. Transpl. 2011, 11, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Simpkins, C.E.; Montgomery, R.A.; Hawxby, A.M.; Locke, J.E.; Gentry, S.E.; Warren, D.S.; Segev, D.L. Cold ischemia time and allograft outcomes in live donor renal transplantation: Is live donor organ transport feasible? Am. J. Transpl. 2007, 7, 99–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kute, V.B.; Patel, H.V.; Shah, P.R.; Modi, P.R.; Shah, V.R.; Rizvi, S.J.; Pal, B.C.; Modi, M.P.; Shah, P.S.; Varyani, U.T.; et al. Past, present and future of kidney paired donation transplantation in India. World J. Transplant. 2017, 7, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Böhmig, G.A.; Fronek, J.; Slavcev, A.; Fischer, G.F.; Berlakovich, G.; Viklicky, O. Czech-Austrian kidney paired donation: First European cross-border living donor kidney exchange. Transpl. Int. 2017, 30, 638–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Laar, S.C.; Robb, M.; Hogg, R.; Burnapp, L.; Papalois, V.E.; Dor, F. The Impact of Cold Ischaemia Time on Outcomes of Living Donor Kidney Transplantation in the UK Living Kidney Sharing Scheme. Ann. Surg. 2021, 274, 859–865. [Google Scholar] [CrossRef]
- Ahmadi, A.R.; Lafranca, J.A.; Claessens, L.A.; Imamdi, R.M.S.; Ijzermans, J.N.M.; Betjes, M.G.H.; Dor, F.J.M.F. Shifting paradigms in eligibility criteria for live kidney donation: A systematic review. Kidney Int. 2015, 87, 31–45. [Google Scholar] [CrossRef]
- Rutten, F.F.; Ploeg, R.J.; McDonnell, J.; Cohen, B. The cost-effectiveness of preservation with UW and EC solution for use in cadaveric kidney transplantation in the case of single kidney donors. Transplantation 1993, 56, 854–858. [Google Scholar] [CrossRef] [PubMed]
- Wight, J.; Chilcott, J.; Holmes, M.; Brewer, N. The clinical and cost-effectiveness of pulsatile machine perfusion versus cold storage of kidneys for transplantation retrieved from heart-beating and non-heart-beating donors. Health Technol. Assess 2003, 7, 1–94. [Google Scholar] [CrossRef] [Green Version]
- Moers, C.; Smits, J.M.; Maathuis, M.-H.J.; Treckmann, J.; van Gelder, F.; Napieralski, B.P.; van Kasterop-Kutz, M.; van der Heide, J.J.H.; Squifflet, J.-P.; van Heurn, E.; et al. Machine Perfusion or Cold Storage in Deceased-Donor Kidney Transplantation. N. Engl. J. Med. 2009, 360, 7–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, P.; Ding, Z.; He, Y.; Zhang, J.; Wang, X.; Yang, Z. Hypothermic Machine Perfusion Versus Static Cold Storage in Deceased Donor Kidney Transplantation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Artif. Organs 2019, 43, 478–489. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.A.J.; Ginther, N.; Luo, Y.; Beck, G.; Ginther, R.; Ewen, M.; Matsche-Neufeld, R.; Shoker, A.; Sawicki, G. Early experience with hypothermic machine perfusion of living donor kidneys—A retrospective study. Transpl. Int. 2017, 30, 706–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groen, H.; Moers, C.; Smits, J.M.; Treckmann, J.; Monbaliu, D.; Rahmel, A.; Paul, A.; Pirenne, J.; Ploeg, R.J.; Buskens, E. Cost-Effectiveness of Hypothermic Machine Preservation versus Static Cold Storage in Renal Transplantation. Am. J. Transplant. 2012, 12, 1824–1830. [Google Scholar] [CrossRef] [Green Version]
- Slagter, J.S.; Outmani, L.; Tran, K.T.C.K.; Ijzermans, J.N.M.; Minnee, R.C. Robot-assisted kidney transplantation as a minimally invasive approach for kidney transplant recipients: A systematic review and meta-analyses. Int. J. Surg. 2022, 99, 106264. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Snyder, J.J.; Matas, A.J.; Ellison, M.D.; Gill, J.S.; Kausz, A.T. Preemptive kidney transplantation: The advantage and the advantaged. J. Am. Soc. Nephrol. 2002, 13, 1358–1364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milton, C.A.; Russ, G.R.; McDonald, S.P. Pre-emptive renal transplantation from living donors in Australia: Effect on allograft and patient survival. Nephrology 2008, 13, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Meier-Kriesche, H.U.; Kaplan, B. Waiting time on dialysis as the strongest modifiable risk factor for renal transplant outcomes: A paired donor kidney analysis. Transplantation 2002, 74, 1377–1381. [Google Scholar] [CrossRef] [PubMed]
- Granholm, A.; Alhazzani, W.; Møller, M.H. Use of the GRADE approach in systematic reviews and guidelines. Br. J. Anaesth. 2019, 123, 554–559. [Google Scholar] [CrossRef] [PubMed]














| Year of Publication | Country | Study Design (Trial) | Intervention (n) | Control (n) | Total Patients | Follow-Up | Study Outcomes | ROBINS-I Tool (Risk of Bias) | |
|---|---|---|---|---|---|---|---|---|---|
| Gill | 2017 | United States | retrospective | 4–16 h (2562) | 0–4 h (45,936) | 48,498 | m 4.53 year | DGF, GS | moderate |
| Krishnan | 2016 | Australia and New Zealand | retrospective | >4–8 h (224) | 1–4 h (3493) | 3717 | m 6.6 year | DGF, AR, eGFR, GS, Mor, GF | moderate |
| Nassiri | 2020 | United States | retrospective | >16 h (141) | <16 h (2222) | 2363 | up to 7 years | DGF, DCGF | moderate |
| Nath | 2016 | United Kingdom | retrospective | >4–8 h (1842) | 0–4 h (7314) | 9156 | - | GS (1, 3, 5 y), DGF, sCreat, PS, AR | moderate |
| Redfield | 2016 | United States | retrospective | DGF (2282) | no-DGF (61,760) | 64,042 | median 6noDGF, 4DGF days | DGF | moderate |
| Roodnat | 2003 | The Netherlands | prospective | ≥12 h | <12 h | 243 | ≥1 year | PS, GS, Mor | moderate |
| Segev | 2011 | United States | prospective | ≥8 h (24) | <8 h (23) | 56 | - | UO | moderate |
| Simpkins | 2007 | United States | retrospective | 4–8 h (1077) | 0–4 h (37,390) | 38,467 | ≥1 year | PS, GF, sCreat1y, DGF1w, AR1y, GS10y | moderate |
| Studies | 0–4 h of CIT | 4–8 h of CIT | p Value | |||
|---|---|---|---|---|---|---|
| n | n | |||||
| Recipient age (mean (SD)) | 4 [11,30,31,35] | 62,126 | 45.40 (2.82) | 4737 | 45.27 (4.12) | 0.92 |
| Recipient sex (male) (%) | 4 [11,30,31,35] | 62,126 | 49.80 | 4737 | 53.99 | 0.92 |
| Pre-emptive KTx (%) | 3 [11,30,31] | 56,744 | 12.28 | 3652 | 26.09 | 0.51 |
| Donor age (mean (SD)) | 3 [11,30,31] | 56,744 | 42.57 (4.22) | 3652 | 41.90 (3.15) | 0.94 |
| Donor sex (male) (%) | 3 [11,30,31] | 56,744 | 39.87 | 3652 | 41.90 | 0.99 |
| HLA-mismatch (1–3) (%) | 2 [11,31] | 53,251 | 46.31 | 3428 | 58.13 | 0.99 |
| HLA-mismatch (4–6) (%) | 2 [11,31] | 53,251 | 41.81 | 3428 | 39.33 | 0.82 |
| Diabetes ESRD (%) | 4 [11,30,31,35] | 62,126 | 18.30 | 4737 | 15.15 | 1.00 |
| Peak PRA = 0 (%) | 2 [11,31] | 53,251 | 59.05 | 3428 | 47.03 | 0.06 |
| Peak PRA > 80 (%) | 2 [11,31] | 53,251 | 5.93 | 3428 | 16.70 | 0.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van de Laar, S.C.; Lafranca, J.A.; Minnee, R.C.; Papalois, V.; Dor, F.J.M.F. The Impact of Cold Ischaemia Time on Outcomes of Living Donor Kidney Transplantation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 1620. https://doi.org/10.3390/jcm11061620
van de Laar SC, Lafranca JA, Minnee RC, Papalois V, Dor FJMF. The Impact of Cold Ischaemia Time on Outcomes of Living Donor Kidney Transplantation: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(6):1620. https://doi.org/10.3390/jcm11061620
Chicago/Turabian Stylevan de Laar, Stijn C., Jeffrey A. Lafranca, Robert C. Minnee, Vassilios Papalois, and Frank J. M. F. Dor. 2022. "The Impact of Cold Ischaemia Time on Outcomes of Living Donor Kidney Transplantation: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 6: 1620. https://doi.org/10.3390/jcm11061620