
High-Throughput Sequencing of Complementarity Determining Region 3 in the Heavy Chain of B-Cell Receptor in Renal Transplant Recipients: A Preliminary Report

 , , and
, , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Selection, Therapeutic Protocol, and Biochemical/Immunological Biomarker Detections
2.2. NGS for CDR3 of BCR IGH
2.2.1. Blood-Collection Scheme
2.2.2. RNA Extraction
2.2.3. iR Library Preparation Process
2.2.4. MiSeq Sequencing
2.3. Data Analysis
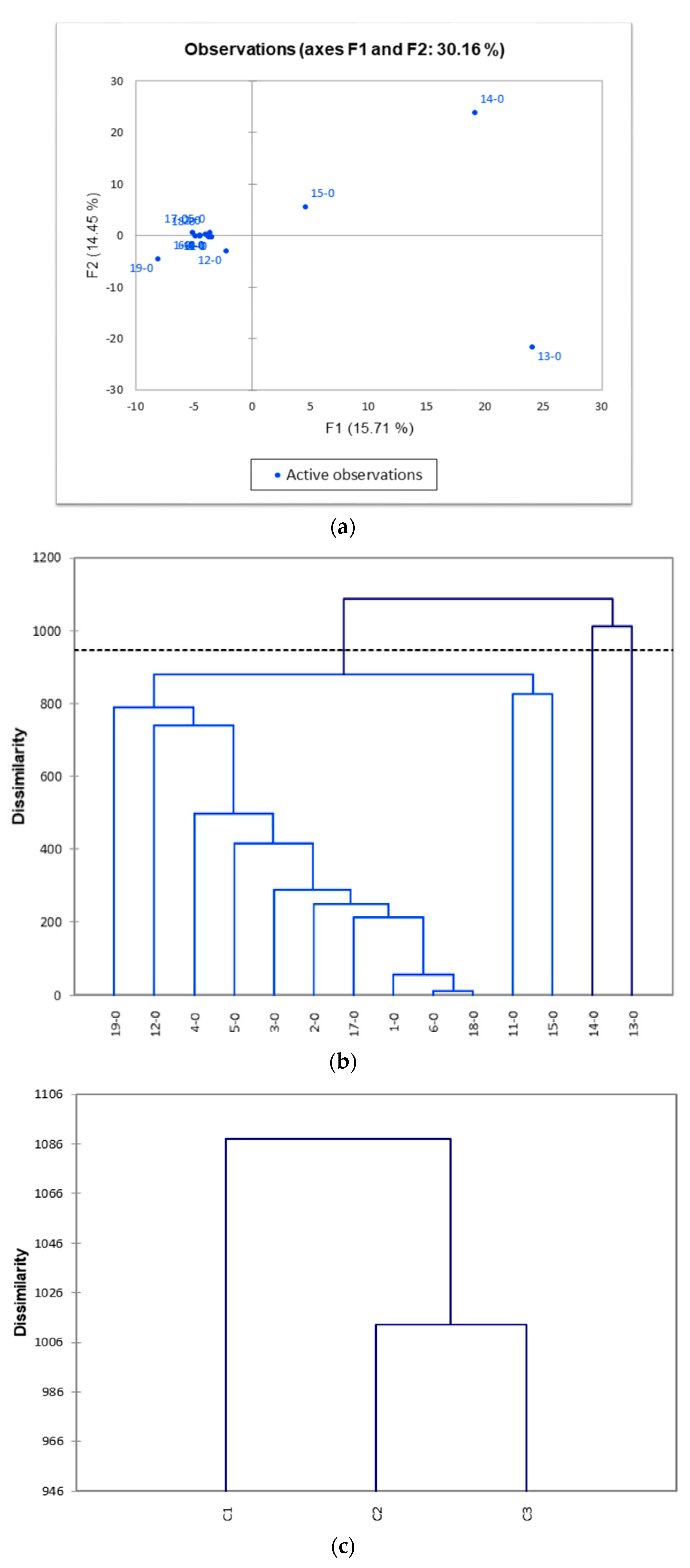
2.4. Principal Component Analysis (PCA) and Agglomerative Hierarchical Clustering (AHC) for Pre-Transplant Baseline IGH iR
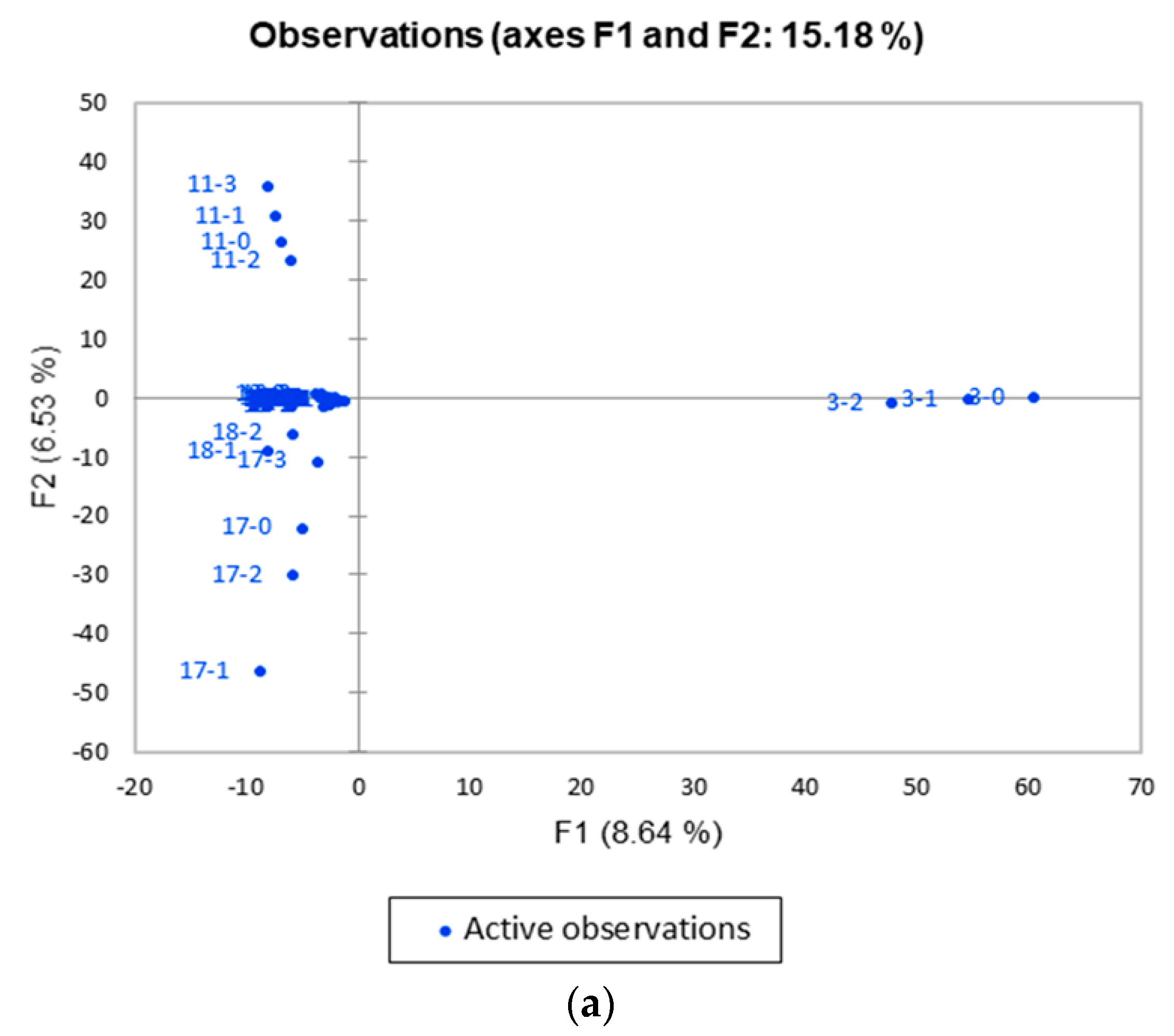
2.5. PCA and AHC for Post-Transplant IGH iR
2.6. Statistical Analysis
3. Results
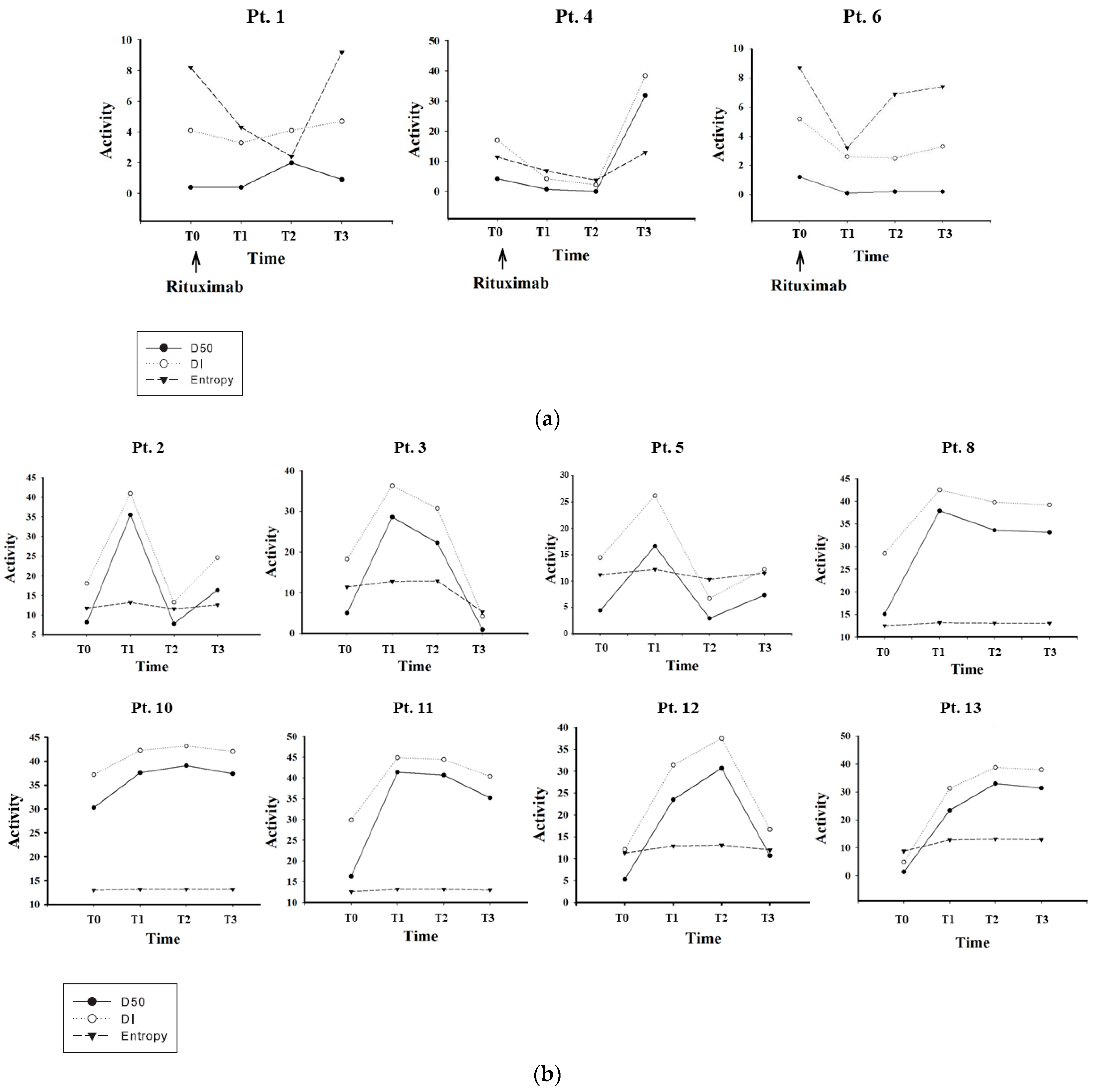
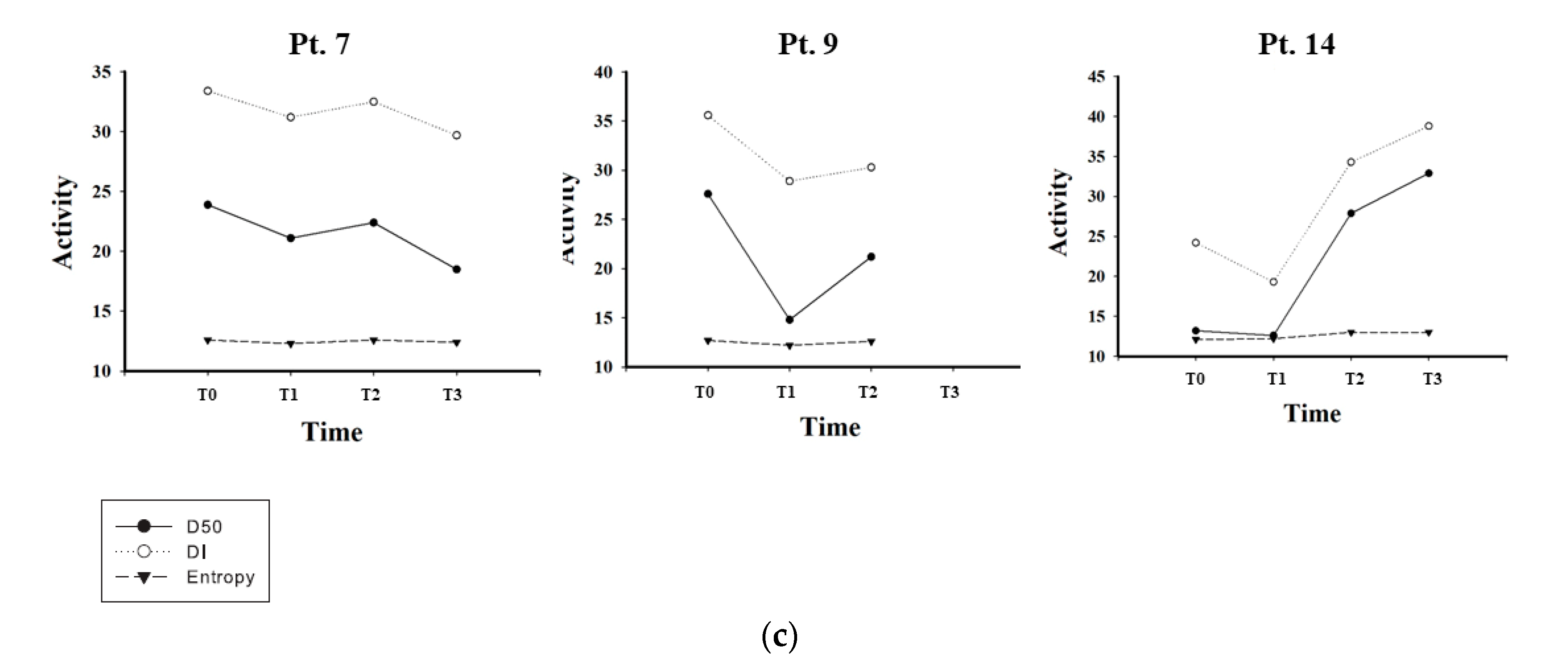
3.1. CDR3 Sequence, D50 and DI Analyses Show Distinct Profiles of Changes in iR
3.2. Distinct Clusters as Shown by PCA and AHC in Pre-Transplant Baseline IGH iR
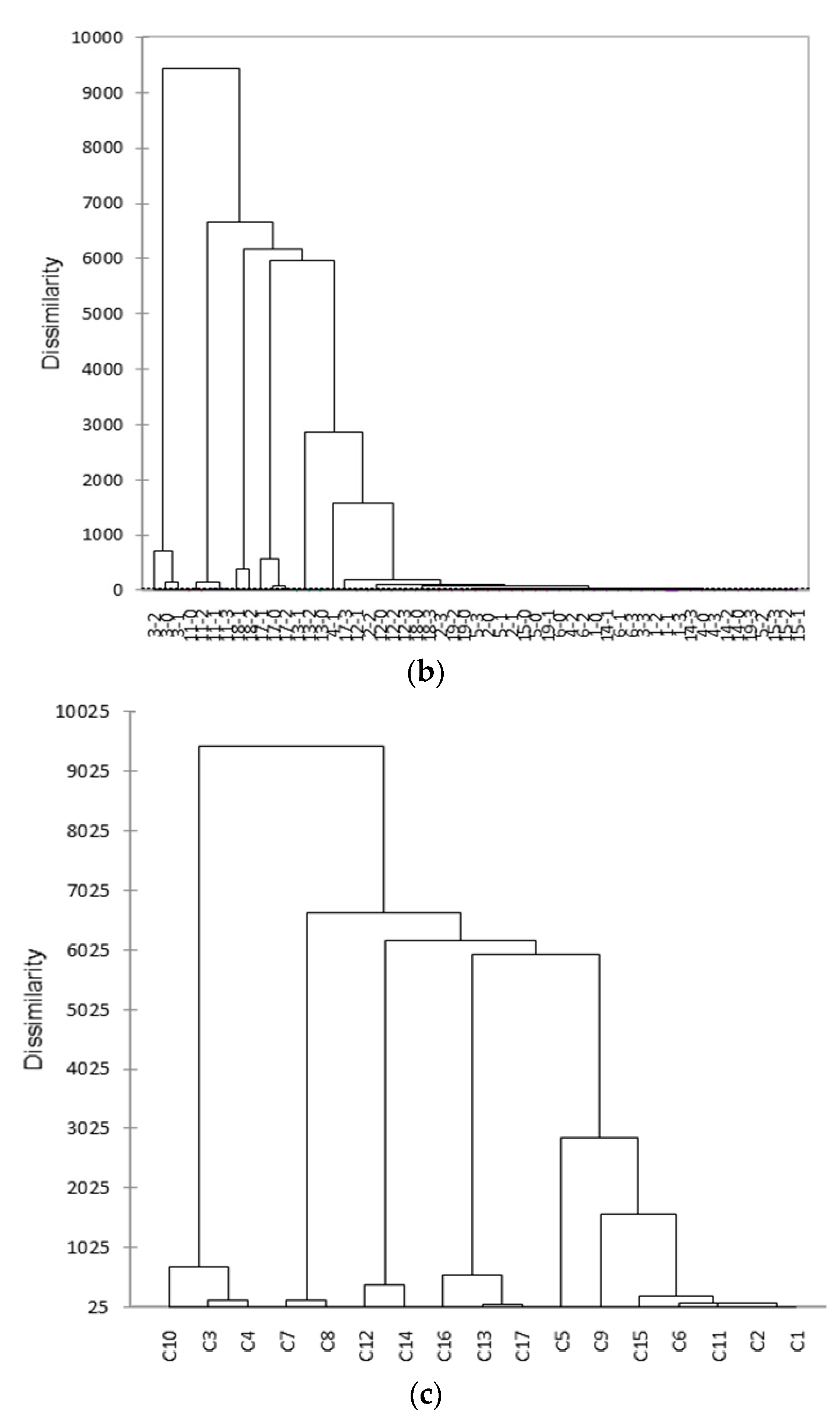
3.3. Distinct Clusters as Shown by PCA and AHC in Post-Transplant IGH iR
4. Discussion
4.1. D50 Profile Trajectory as a Good Companion Indicator for Predicting Graft Dysfunction/Failure and/or Rejection Episodes
4.2. Clusters of Changes in Immune Diversity as a Good Indicator for Searching Renal Failure Etiologies and Specific Gene Finders during Adverse Events in the Course of Renal Transplantation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clayton, P.A.; McDonald, S.P.; Russ, G.R.; Chadban, S.J. Long-term outcomes after acute rejection in kidney transplant recipients: An ANZDATA analysis. J. Am. Soc. Nephrol. 2019, 30, 1697–1707. [Google Scholar] [CrossRef] [PubMed]
- Hart, A.; Lentine, K.L.; Smith, J.M.; Miller, J.M.; Skeans, M.A.; Prentice, M.; Robinson, A.; Foutz, J.; Booker, S.E.; Israni, A.K.; et al. Organ Procurement and Transplantation Network (OPTN) and Scientific Registry of Transplant Recipients (SRTR): OPTN/SRTR 2019 Annual Data Report. Kidney 2021, 21, 21–137. [Google Scholar]
- Australia and New Zealand Dialysis and Transplant Registry. 43rd Annual Report 2020 (Data to 2019), Chapter 7. In Transplantation; Australia and New Zealand Dialysis and Transplant Registry: Adelaide, Australia, 2020. [Google Scholar]
- Valujskikh, A.; Baldwin, W.M.; Fairchild, R.L. Recent progress and new perspectives in studying T cell responses to allografts. Am. J. Transpl. 2010, 10, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Zarkhin, V.; Chalasani, G.; Sarwal, M.M. The yin and yang of B cells in graft rejection and tolerance. Transpl. Rev. 2010, 24, 67–78. [Google Scholar] [CrossRef]
- Tonegawa, S. Somatic generation of antibody diversity. Nature 1983, 302, 575–581. [Google Scholar] [CrossRef]
- Robins, H. Immunosequencing: Applications of immune repertoire deep sequencing. Curr. Opin. Immunol. 2013, 25, 646–652. [Google Scholar] [CrossRef]
- Arstila, T.P.; Casrouge, A.; Baron, V.; Even, J.; Kanellopoulos, J.; Kourilsky, P. A direct estimate of the human alphabeta T cell receptor diversity. Science 1999, 286, 958–961. [Google Scholar] [CrossRef]
- Price, D.A.; West, S.M.; Betts, M.R.; Ruff, L.E.; Brenchley, J.M.; Ambrozak, D.R.; Edghill-Smith, Y.; Kuroda, M.J.; Bogdan, D.; Kunstman, K.; et al. T cell receptor recognition motifs govern immune escape patterns in acute SIV infection. Immunity 2004, 21, 793–803. [Google Scholar] [CrossRef] [Green Version]
- Robinson, W.H. Sequencing the functional antibody repertoire- diagnostic and therapeutic discovery. Nat. Rev. Rheumatol. 2015, 11, 171–182. [Google Scholar] [CrossRef] [Green Version]
- Six, A.; Mariotti-Ferrandiz, M.E.; Chaara, W.; Magadan, S.; Pham, H.P.; Lefranc, M.P.; Mora, T.; Thomas-Vaslin, V.; Walczak, A.M.; Boudinot, P. The past, present, and future of immune repertoire biology- the rise of next-generation repertoire analysis. Front. Immunol. 2013, 4, 413. [Google Scholar] [CrossRef] [Green Version]
- Gorski, J.; Yassai, M.; Zhu, X.; Kissela, B.; Keever, C.; Flomenberg, N. Circulating T cell repertoire complexity in normal individuals and bone marrow recipients analyzed by CDR3 size spectratyping. Correlation with immune status. J. Immunol. 1994, 152, 5109–5119. [Google Scholar] [PubMed]
- Granato, A.; Chen, Y.; Wesemann, D.R. Primary immunoglobulin repertoire development: Time and space matter. Curr. Opin. Immunol. 2015, 33, 126–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, M.; Yew, P.-Y.; Hasegawa, K.; Ikeda, Y.; Fujiwara, K.; Fleming, G.F.; Nakamura, Y.; Park, J.H. Characterization of T cell repertoire of blood, tumor, and ascites in ovarian cancer patients using next generation sequencing. Oncoimmunology 2015, 4, e1030561. [Google Scholar] [CrossRef] [Green Version]
- Cao, X.; Wa, Q.; Wang, Q.; Li, L.; Liu, X.; An, L.; Cai, R.; Du, M.; Qiu, Y.; Han, J.; et al. High throughput sequencing reveals the diversity of TRB-CDR3 repertoire in patients with psoriasis vulgaris. Int. Immunopharmacol. 2016, 40, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Sanders, C.M.; Yang, Q.; Schroeder, H.W.; Wang, E.; Babrzadeh, F.; Gharizadeh, B.; Myers, R.M.; Hudson, J.R.; Davis, R.W.; et al. High throughput sequencing reveals a complex pattern of dynamic interrelationships among human T cell subsets. Proc. Natl. Acad. Sci. USA 2010, 107, 1518–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, L.; Wang, L.; Chen, H.; Zhang, J.; Yan, Q.; Ou, M.; Lin, H.; Hou, X.; Chen, S.; Dai, Y.; et al. T cell repertoire following kidney transplantation revealed by high-throughput sequencing. Transpl. Immunol. 2016, 39, 34–45. [Google Scholar] [CrossRef]
- Pineda, S.; Sigdel, T.K.; Liberto, J.M.; Vincenti, F.; Sirota, M.; Sarwal, M.M. Characterizing pre-transplant and post-transplant kidney rejection risk by B cell immune repertoire sequencing. Nat. Commun. 2019, 10, 1906. [Google Scholar] [CrossRef] [Green Version]
- Lai, L.; Zhou, X.; Chen, H.; Luo, Y.; Sui, W.; Zhang, J.; Tang, D.; Yan, Q.; Dai, Y. Composition and diversity analysis of the B-cell receptor immunoglobulin heavy chain complementarity-determining region 3 repertoire in patients with acute rejection after kidney transplantation using high-throughput sequencing. Exp. Ther. Med. 2019, 17, 2206–2220. [Google Scholar] [CrossRef] [Green Version]
- Abbas, A.K.; Lichtman, A.H. Cellular and Molecular Immunology, 5th ed.; Saunders: Philadelphia, PA, USA, 2003; ISBN 0-7216-0008-5. [Google Scholar]
- Paul, W.E. Fundamental Immunology, 6th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; ISBN 978-0-7817-6519-0. [Google Scholar]
- Shang, W.; Dong, L.; Feng, G.; Wang, Y.; Pang, X.; Li, J.; Liu, L.; Zhang, W. Panel-reactive antibody levels and renal transplantation rates in sensitized patients after desensitization and human leucocyte antigen amino acid residue matching. J. Int. Med. Res. 2013, 41, 1333–1341. [Google Scholar] [CrossRef]
- Tambur, A.R.; Leventhal, J.; Kaufman, D.B.; Friedewald, J.; Miller, J.; Abecassis, M.M. Tailoring antibody testing and how to use it in the calculated panel reactive antibody era: The Northwestern University experience. Transplantation 2008, 86, 1052–1059. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.; Stastny, P.; Süsal, C.; Döhler, B.; Opelz, G. Antibodies against MICA antigens and kidney-transplant rejection. N. Engl. J. Med. 2007, 357, 1293–1300. [Google Scholar] [PubMed] [Green Version]
- Poli, A.; Michel, T.; Thérésine, M.; Andrès, E.; Hentges, F.; Zimmer, J. CD56bright natural killer (NK) cells: An important NK cell subset. Immunology 2009, 126, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Townamchai, N.; Safa, K.; Chandraker, A. Immunologic monitoring in kidney transplant recipients. Kidney Res. Clin. Pract. 2013, 32, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Hou, D.; Ying, T.; Wang, L.; Chen, C.; Lu, S.; Wang, Q.; Seeley, E.; Xu, J.; Xi, X.; Li, T.; et al. Immune repertoire diversity correlated with mortality in avian influenza A (H7N9) virus infected patients. Sci. Rep. 2016, 6, 33843. [Google Scholar] [PubMed] [Green Version]
- Shannon, C.E. A mathematical theory of communication. Bell Syst. Tech. J. 1948, 27, 379–423. [Google Scholar] [CrossRef] [Green Version]
- Entropy (Information Theory). Available online: https://en.wikipedia.org/wiki/Entropy_(information_theory)#:~:text=An%20equivalent%20definition%20of%20entropy,communication%20channel%2C%20and%20a%20receiver (accessed on 22 February 2022).
- Rokach, L.; Maimon, O. Clustering methods. In Data Mining and Knowledge Discovery Handbook; Springer: New York, NY, USA, 2005; pp. 321–352. [Google Scholar]
- Nielsen, F. Hierarchical clustering. In Introduction to HPC with MPI for Data Science; Springer: Berlin/Heidelberg, Germany, 2016; pp. 105–211. [Google Scholar]
- Sibson, R. SLINK: An optimally efficient algorithm for the single-link cluster method. Comp. J. 1973, 16, 30–34. [Google Scholar] [CrossRef]
- Alachkar, H.; Mutonga, M.; Kato, T.; Kalluri, S.; Kakuta, Y.; Uemura, M.; Imamura, R.; Nonomura, N.; Vujjini, V.; Alasfar, S.; et al. Quantitative characterization of T-cell repertoire and biomarkers in kidney transplant rejection. BMC Nephrol. 2016, 17, 181. [Google Scholar] [CrossRef] [Green Version]
- Aschauer, C.; Jelencsics, K.; Hu, K.; Heinze, A.; Vetter, J.; Fraunhofer, T.; Schaller, S.; Winkler, S.; Pimenov, L.; Gualdoni, G.A.; et al. Next generation sequencing based assessment of the alloreactive T cell receptor repertoire in kidney transplant patients during rejection: A prospective cohort study. BMC Nephrol. 2019, 20, 346. [Google Scholar] [CrossRef] [Green Version]
- Greiff, V.; Bhat, P.; Cook, S.C.; Menzel, U.; Kang, W.; Reddy, S.T. A bioinformatic framework for immune repertoire diversity profiling enables detection of immunological status. Genome Med. 2015, 7, 49. [Google Scholar] [CrossRef]
- Schwartz, R.S. Diversity of the immune repertoire and immunoregulation. N. Eng. J. Med. 2003, 348, 1017–1026. [Google Scholar] [CrossRef] [Green Version]
- Mendez, L.M.G.; Cascino, M.D.; Garg, J.; Katsumoto, T.R.; Brakeman, P.; Dall’Era, M.; Looney, R.J.; Rovin, B.; Dragone, L.; Brunetta, P. Peripheral blood B cell depletion after rituximab and complete response in lupus nephritis. Clin. J. Am. Soc. Nephrol. 2018, 13, 1502–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, A.; Mengel, M.; Gwinner, W.; Radermacher, J.; Hiss, M.; Kreipe, H.; Haller, H. Risk factors for chronic allograft nephropathy after renal transplantation: A protocol biopsy study. Kidney Int. 2005, 67, 341–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, A. Protocol transplant biopsies: Are they really needed? Clin. J. Am. Soc. Nephrol. 2006, 1, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Recipient Age/Sex | Donor Age/Sex | Recipient ABO/Rh | Donor ABO/Rh | Allograft Source | HLA Mismatch | Cause of ESRD | Perico Score * | PRA-I * | PRA-II * | Remark | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 64/F | 62/M | O/+ | A | L | 3 | ? | <3 | 56.3 | N | DS |
| 2 | 46/M | 51/M | AB/+ | AB | C | 2 | CIN | 6 | N | N | DCD |
| 3 | 65/F | 51M | AB/+ | AB | C | 2 | CGN | 6 | N | N | DCD |
| 4 | 63/F | 67/M | A/+ | O/+ | L | 5 | DMN | 3 | N | 17.8 | DS |
| 5 | 55/M | 24/M | B/+ | B/+ | L | 3 | ? | <3 | N | N | |
| 6 | 34/F | 60/M | B/+ | AB/+ | L | 3 | IgAN | 3 | N | N | DS |
| 7 | 40/M | 61/F | A/+ | A/+ | L | 2 | DMN | <3 | N | N | TCMR |
| 8 | 39/M | 61/F | O/+ | O/+ | L | 2 | Nscl | <3 | 8.7 | N | |
| 9 | 49/F | 69/F | O/+ | O/+ | L | 3 | ? | <3 | N | N | TCMR |
| 10 | 38/F | 43/F | A/+ | A/+ | L | 5 | DMN | <3 | N | N | |
| 11 | 59/F | 63/M | O/+ | O/+ | L | 3 | ? | <3 | N | N | |
| 12 | 63/M | 59/M | B/+ | O/+ | L | 6 | CIN | 3 | N | N | |
| 13 | 36/F | 70/M | O/+ | O/+ | L | 2 | LN | 3 | N | N | |
| 14 | 40/F | 52/M | A/+ | A/+ | C | 2 | Nscl | 3 | N | N | TCMR |
| Patient | DGF | Infection | TCMR | AMR | Desensitization * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T1 | T2 | T3 | T1 | T2 | T3 | |||
| #1 | BKV, 4.5 M | −21 D, −1 D | |||||||||
| UTI (Ec), 3 M | UTI, 12 M | ||||||||||
| #2 | + | ||||||||||
| #3 | + | ||||||||||
| #4 | UTI (Ec), 1 M | −21 D | |||||||||
| #5 | UTI (Ef), 1.5 M | ||||||||||
| #6 | BKV, 2 M | PVN, 4 M | −21 D, 0 D | ||||||||
| #7 | PA, 1 M | UTI (Pm, Ec), 9 M | |||||||||
| #8 | + | CVP (Se), 7 D | |||||||||
| #9 | |||||||||||
| #10 | BKV, 8 M–10 M | ||||||||||
| #11 | BKV, 12 M | ||||||||||
| #12 | UTI (Ec), 1 M | 1 M | |||||||||
| #13 | UTI (Kp), 9 D | UTI (Kp), 2 M | |||||||||
| #14 | + | AWA, 1 M | CMV, 2 M | PVN, 4.5 M | 20 D | 4 M | 9 M | MVI (?) 9 M | |||
| Sample | CDR3 Reads | Unique CDR3 Reads | D50 | DI | H |
|---|---|---|---|---|---|
| 1-T0 | 332,605 | 8707 | 0.4 | 4.1 | 8.2 |
| 1-T1 | 44,829 | 906 | 0.4 | 3.3 | 4.3 |
| 1-T2 | 2709 | 102 | 2 | 4.1 | 2.4 |
| 1-T3 | 342,511 | 12,875 | 0.9 | 4.7 | 9.2 |
| 2-T0 | 1,350,497 | 114,401 | 8.2 | 18.1 | 11.8 |
| 2-T1 | 1,085,401 | 100,641 | 35.5 | 41 | 13.2 |
| 2-T2 | 201,291 | 15,366 | 7.8 | 13.3 | 11.6 |
| 2-T3 | 660,271 | 43,697 | 16.4 | 24.6 | 12.6 |
| 3-T0 | 1,153,784 | 137,153 | 5 | 18.2 | 11.4 |
| 3-T1 | 1,179,141 | 122,205 | 28.9 | 36.3 | 12.8 |
| 3-T2 | 841,419 | 58,891 | 22.2 | 30.7 | 12.9 |
| 3-T3 | 25,797 | 787 | 0.9 | 4.2 | 5.3 |
| 4-T0 | 1,137,969 | 92,997 | 4.2 | 17 | 11.4 |
| 4-T1 | 94,964 | 3075 | 0.7 | 4.2 | 6.8 |
| 4-T2 | 448,670 | 3028 | 0 | 2.2 | 3.7 |
| 4-T3 | 1,005,018 | 114,697 | 31.9 | 38.4 | 12.9 |
| 5-T0 | 1,402,168 | 84,251 | 4.4 | 14.4 | 11.2 |
| 5-T1 | 627,283 | 42,274 | 16.6 | 26.2 | 12.2 |
| 5-T2 | 294,124 | 14,043 | 2.9 | 6.7 | 10.3 |
| 5-T3 | 734,429 | 32,048 | 7.3 | 12.2 | 11.5 |
| 6-T0 | 151,185 | 6366 | 1.2 | 5.2 | 8.7 |
| 6-T1 | 71,825 | 831 | 0.1 | 2.6 | 3.2 |
| 6-T2 | 948,704 | 9602 | 0.2 | 2.5 | 6.9 |
| 6-T3 | 950,614 | 17,209 | 0.2 | 3.3 | 7.4 |
| 7-T0 | 1,183,078 | 132,636 | 23.9 | 33.4 | 12.6 |
| 7-T1 | 1,287,151 | 105,115 | 21.1 | 31.2 | 12.3 |
| 7-T2 | 1,207,732 | 120,182 | 22.4 | 32.5 | 12.6 |
| 7-T3 | 652,595 | 68,099 | 18.5 | 29.7 | 12.4 |
| 8-T0 | 1,645,902 | 168,487 | 15.1 | 28.5 | 12.5 |
| 8-T1 | 1,140,959 | 189,932 | 37.9 | 42.5 | 13.2 |
| 8-T2 | 1,258,039 | 157,665 | 33.6 | 39.8 | 13.1 |
| 8-T3 | 845,907 | 89,271 | 33.1 | 39.2 | 13.1 |
| 9-T0 | 1,313,895 | 144,136 | 27.6 | 35.6 | 12.7 |
| 9-T1 | 1,112,684 | 171,721 | 14.8 | 28.9 | 12.2 |
| 9-T2 | 1,047,150 | 70,334 | 21.2 | 30.3 | 12.6 |
| 10-T0 | 1,061,414 | 118,472 | 30.3 | 37.2 | 13 |
| 10-T1 | 918,080 | 200,001 | 37.6 | 42.3 | 13.2 |
| 10-T2 | 1,372,288 | 199,626 | 39.1 | 43.2 | 13.2 |
| 10-T3 | 906,739 | 105,136 | 37.4 | 42.1 | 13.2 |
| 11-T0 | 1,163,277 | 129,036 | 16.3 | 29.9 | 12.6 |
| 11-T1 | 1,361,199 | 233,772 | 41.4 | 44.9 | 13.2 |
| 11-T2 | 1,124,920 | 182,482 | 40.7 | 44.5 | 13.2 |
| 11-T3 | 1,123,497 | 183,386 | 35.2 | 40.4 | 13 |
| 12-T0 | 866,775 | 43,874 | 5.3 | 12.1 | 11.3 |
| 12-T1 | 2,220,129 | 111,706 | 23.5 | 31.4 | 12.9 |
| 12-T2 | 2,449,184 | 143,081 | 30.7 | 37.5 | 13.1 |
| 12-T3 | 779,336 | 39,210 | 10.7 | 16.7 | 12 |
| 13-T0 | 193,485 | 7240 | 1.4 | 4.9 | 8.8 |
| 13-T1 | 883,178 | 64,490 | 23.4 | 31.3 | 12.8 |
| 13-T2 | 979,861 | 83,809 | 33 | 38.8 | 13.1 |
| 13-T3 | 1,448,968 | 130,378 | 31.4 | 38 | 12.9 |
| 14-T0 | 1,054,484 | 68,213 | 13.2 | 24.2 | 12.1 |
| 14-T1 | 926,726 | 54,854 | 12.6 | 19.3 | 12.2 |
| 14-T2 | 1,050,148 | 80,138 | 27.9 | 34.3 | 13 |
| 14-T3 | 1,215,236 | 98,127 | 32.9 | 38.8 | 13 |
| Average | 925,113 | 86,012 | 18.0 | 24.7 | 11.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, T.-H.; Liao, H.-T.; Li, T.-H.; Tsai, H.-C.; Lin, N.-C.; Chen, C.-Y.; Tsai, S.-F.; Huang, T.-H.; Tsai, C.-Y.; Yu, C.-L. High-Throughput Sequencing of Complementarity Determining Region 3 in the Heavy Chain of B-Cell Receptor in Renal Transplant Recipients: A Preliminary Report. J. Clin. Med. 2022, 11, 2980. https://doi.org/10.3390/jcm11112980
Wu T-H, Liao H-T, Li T-H, Tsai H-C, Lin N-C, Chen C-Y, Tsai S-F, Huang T-H, Tsai C-Y, Yu C-L. High-Throughput Sequencing of Complementarity Determining Region 3 in the Heavy Chain of B-Cell Receptor in Renal Transplant Recipients: A Preliminary Report. Journal of Clinical Medicine. 2022; 11(11):2980. https://doi.org/10.3390/jcm11112980
Chicago/Turabian StyleWu, Tsai-Hung, Hsien-Tzung Liao, Tzu-Hao Li, Hung-Cheng Tsai, Niang-Cheng Lin, Cheng-Yen Chen, Shih-Feng Tsai, Tzu-Hao Huang, Chang-Youh Tsai, and Chia-Li Yu. 2022. "High-Throughput Sequencing of Complementarity Determining Region 3 in the Heavy Chain of B-Cell Receptor in Renal Transplant Recipients: A Preliminary Report" Journal of Clinical Medicine 11, no. 11: 2980. https://doi.org/10.3390/jcm11112980