
Strategies to Overcome HLA Sensitization and Improve Access to Retransplantation after Kidney Graft Loss
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. The Benefits of Retransplantation
4. The HLA Barrier and Sensitization
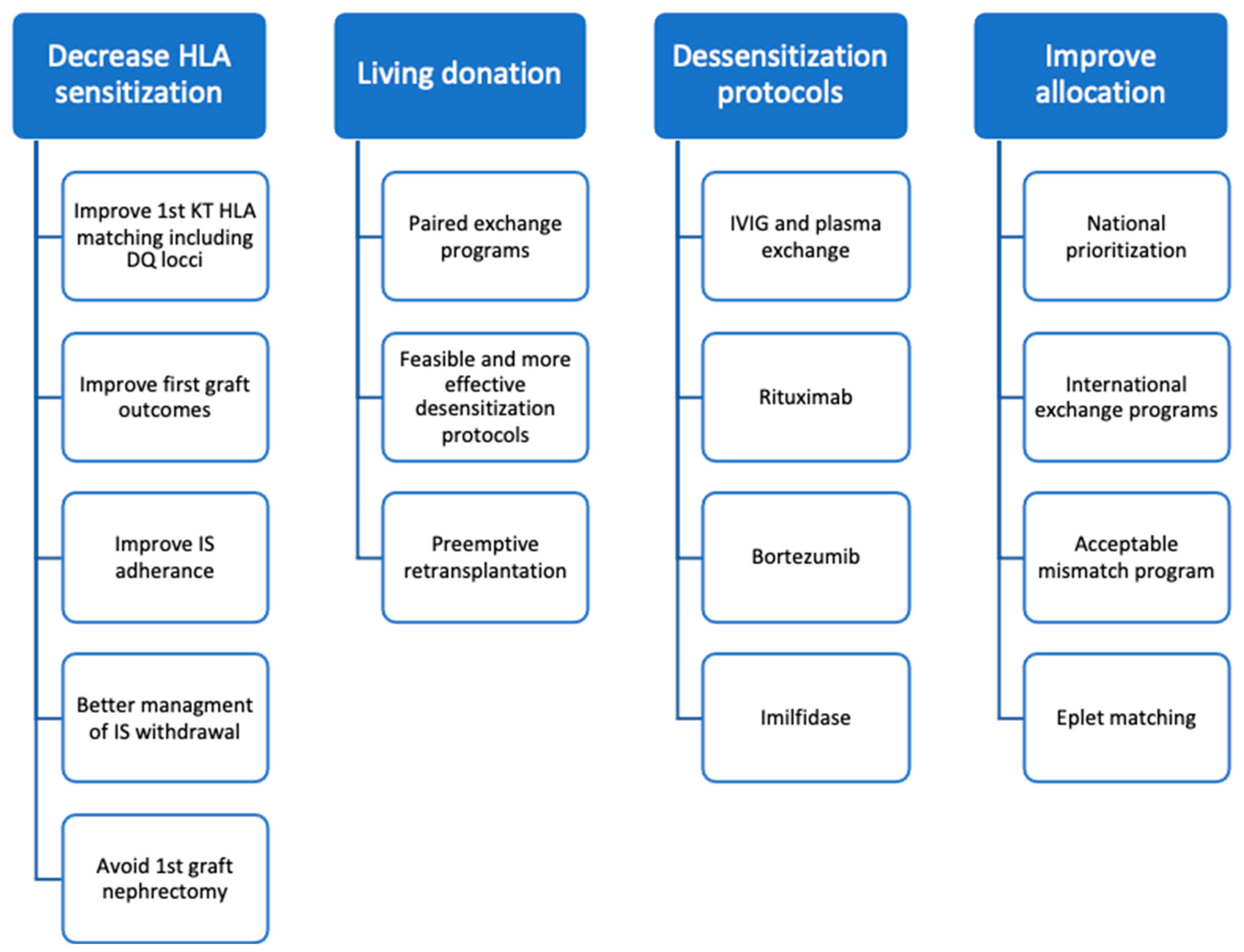
5. Strategies to Increase Retransplantation Access (Figure 1)
5.1. Improve HLA Matching in First Kidney Graft

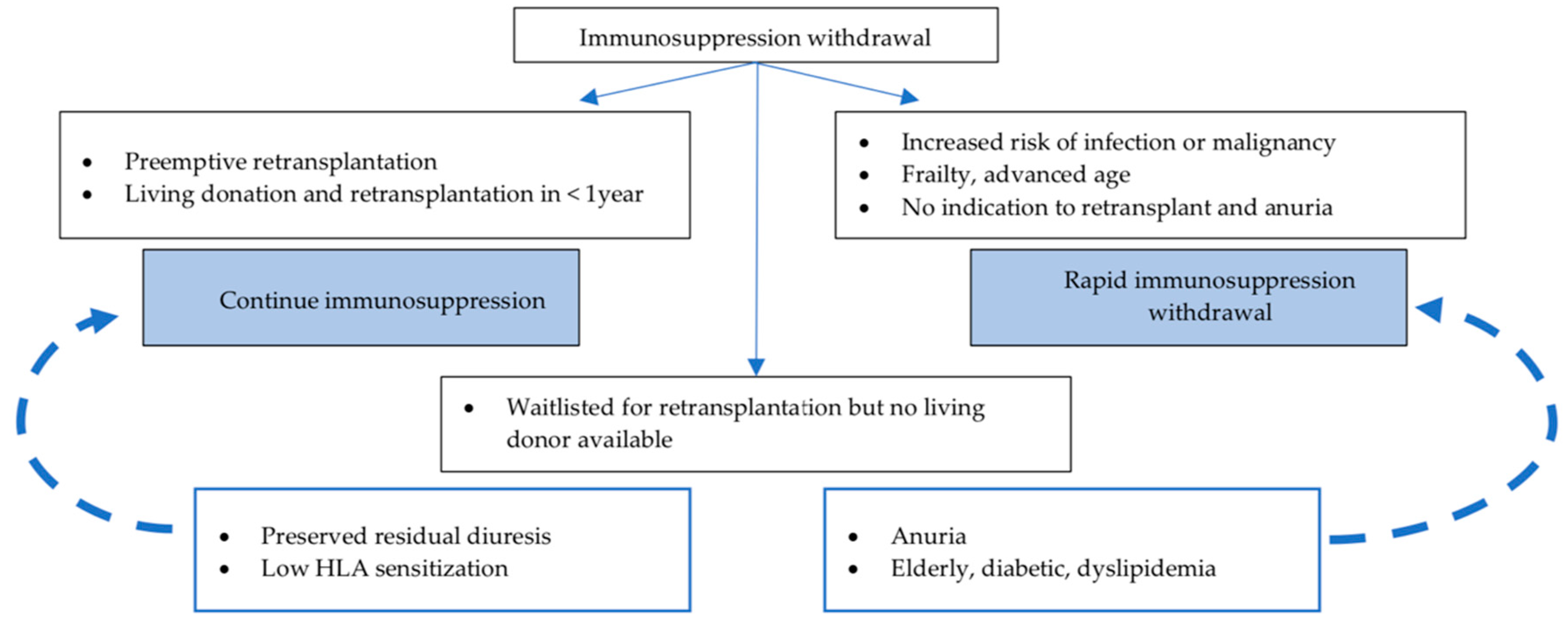
5.2. Immunosuppression Withdrawal and Graft Nephrectomy after Graft Loss
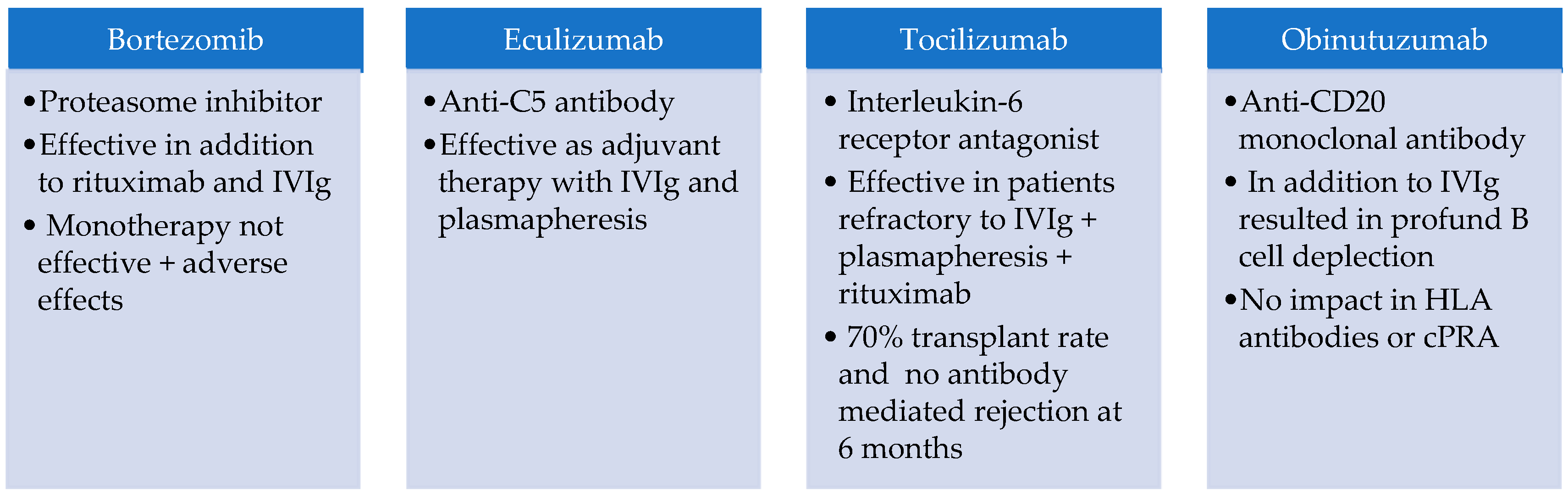
5.3. Desensitization Protocols
5.4. Living Donation, Kidney Paired-Donation and Preemptive Retransplantation
5.5. Allocation Programs for the Highly Sensitized Patients
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| BAFF | B cell activating factor |
| CKD | chronic kidney disease |
| CNI | calcineurin inhibitor |
| cPRA | calculated panel reactive antibody |
| DSA | donor specific antibody |
| GIS | graft intolerance syndrome |
| IS | immunosuppression |
| IVIg | intravenous immunoglobulin (IVIg) |
| KAS | Kidney Allocation System |
| KT | kidney transplant |
| MFI | mean fluorescence intensity |
| PRA | panel reactive antibody |
References
- Heaphy, E.L.G.; Poggio, E.D.; Flechner, S.M.; Goldfarb, D.A.; Askar, M.; Fatica, R.; Srinivas, T.R.; Schold, J.D. Risk Factors for Retransplant Kidney Recipients: Relisting and Outcomes from Patients’ Primary Transplant. Am. J. Transplant. 2014, 14, 1356–1367. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Smith, J.M.; Hart, A.; Miller, J.; Skeans, M.A.; Larkin, L.; Robinson, A.; Gauntt, K.; Israni, A.K.; Hirose, R.; et al. OPTN/SRTR 2020 Annual Data Report: Kidney. Am. J. Transplant. 2022, 22 (Suppl. 2), 21–136. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.; Kadatz, M.; Gill, J.; Gill, J.S. Access to kidney transplantation after a failed first kidney transplant and associations with patient and allograft survival: An analysis of national data to inform allocation policy. Clin. J. Am. Soc. Nephrol. 2019, 14, 1228–1237. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.S.; Schaubel, D.E.; Wei, G.; Fenton, S.S.A. Evaluating the survival benefit of kidney retransplantation. Transplantation 2006, 82, 669–674. [Google Scholar] [CrossRef]
- Kosmoliaptsis, V.; Gjorgjimajkoska, O.; Sharples, L.D.; Chaudhry, A.N.; Chatzizacharias, N.; Peacock, S.; Torpey, N.; Bolton, E.M.; Taylor, C.J.; Bradley, J.A. Impact of donor mismatches at individual HLA-A, -B, -C, -DR, and -DQ loci on the development of HLA-specific antibodies in patients listed for repeat renal transplantation. Kidney Int. 2014, 86, 1039–1048. [Google Scholar] [CrossRef]
- Tafulo, S.; Malheiro, J.; Dias, L.; Almeida, M.; Martins, L.S.; Pedroso, S.; Osório, E.; Lobato, L.; Castro-Henriques, A. Eplet-based virtual PRA increases transplant probability in highly-sensitized patients. Transpl. Immunol. 2021, 65, 101362. [Google Scholar] [CrossRef]
- Manook, M.; Koeser, L.; Ahmed, Z.; Robb, M.; Johnson, R.; Shaw, O.; Kessaris, N.; Dorling, A.; Mamode, N. Post-listing survival for highly sensitised patients on the UK kidney transplant waiting list: A matched cohort analysis. Lancet 2017, 389, 727–734. [Google Scholar] [CrossRef]
- Meier-Kriesche, H.U.; Scornik, J.C.; Susskind, B.; Rehman, S.; Schold, J.D. A lifetime versus a graft life approach redefines the importance of HLA matching in kidney transplant patients. Transplantation 2009, 88, 23–29. [Google Scholar] [CrossRef]
- Gebel, H.M.; Bray, R.A. HLA antibody detection with solid phase assays: Great expectations or expectations too great? Am. J. Transplant. 2014, 14, 1964–1975. [Google Scholar] [CrossRef]
- Wiebe, C.; Kosmoliaptsis, V.; Pochinco, D.; Taylor, C.J.; Nickerson, P. A Comparison of HLA Molecular Mismatch Methods to Determine HLA Immunogenicity. Transplantation 2018, 102, 1338–1343. [Google Scholar] [CrossRef] [Green Version]
- Lucisano, G.; Brookes, P.; Santos-Nunez, E.; Firmin, N.; Gunby, N.; Hassan, S.; Gueret-Wardle, A.; Herbert, P.; Papalois, V.; Willicombe, M.; et al. Allosensitization after transplant failure: The role of graft nephrectomy and immunosuppression—A retrospective study. Transpl. Int. 2019, 32, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.Y.; Manook, M.; Olaso, D.; Ezekian, B.; Park, J.; Freischlag, K.; Jackson, A.; Knechtle, S.; Kwun, J. Emerging New Approaches in Desensitization: Targeted Therapies for HLA Sensitization. Front. Immunol. 2021, 12, 2219. [Google Scholar] [CrossRef] [PubMed]
- Mumford, L.; Fuggle, S.V.; Martorell, J.; Slavcev, A.; Iniotaki, A.; Haasnoot, G.W.; Heidt, S.; Claas, F.H.J. A Europe wide acceptable mismatch program will enable transplantation of long waiting highly sensitised patients with a compatible donor. Transpl. Immunol. 2021, 64, 101354. [Google Scholar] [CrossRef] [PubMed]
- Heidt, S.; Haasnoot, G.W.; Witvliet, M.D.; H van der Linden-van Oevelen, M.J.; Kamburova, E.G.; Wisse, B.W.; Joosten, I.; Allebes, W.A.; van der Meer, A.; Hilbrands, L.B.; et al. Allocation to highly sensitized patients based on acceptable mismatches results in low rejection rates comparable to nonsensitized patients. Am. J. Transplant. 2019, 19, 2926–2933. [Google Scholar] [CrossRef] [PubMed]
- Alhamad, T.; Lubetzky, M.; Lentine, K.L.; Edusei, E.; Parsons, R.; Pavlakis, M.; Woodside, K.J.; Adey, D.; Blosser, C.D.; Concepcion, B.P.; et al. Kidney recipients with allograft failure, transition of kidney care (KRAFT): A survey of contemporary practices of transplant providers. Am. J. Transplant. 2021, 21, 3034–3042. [Google Scholar] [CrossRef]
- Mamode, N.; Bestard, O.; Claas, F.; Furian, L.; Griffin, S.; Legendre, C.; Pengel, L.; Naesens, M. European Guideline for the Management of Kidney Transplant Patients with HLA Antibodies: By the European Society for Organ Transplantation Working Group. Transpl. Int. 2022, 35, 10511. [Google Scholar] [CrossRef]
- Brar, A.; Markell, M.; Stefanov, D.G.; Timpo, E.; Jindal, R.M.; Nee, R.; Sumrani, N.; John, D.; Tedla, F.; Salifu, M.O. Mortality after Renal Allograft Failure and Return to Dialysis. Am. J. Nephrol. 2017, 45, 180–186. [Google Scholar] [CrossRef]
- Gill, J.S.; Abichandani, R.; Kausz, A.T.; Pereira, B.J.G. Mortality after kidney transplant failure: The impact of non-immunologic factors. Kidney Int. 2002, 62, 1875–1883. [Google Scholar] [CrossRef]
- Rao, P.S.; Schaubel, D.E.; Jia, X.; Li, S.; Port, F.K.; Saran, R. Survival on dialysis post-kidney transplant failure: Results from the Scientific Registry of Transplant Recipients. Am. J. Kidney Dis. 2007, 49, 294–300. [Google Scholar] [CrossRef]
- Perl, J.; Zhang, J.; Gillespie, B.; Wikström, B.; Fort, J.; Hasegawa, T.; Fuller, D.S.; Pisoni, R.L.; Robinson, B.M.; Tentori, F. Reduced survival and quality of life following return to dialysis after transplant failure: The Dialysis Outcomes and Practice Patterns Study. Nephrol. Dial. Transplant. 2012, 27, 4464–4472. [Google Scholar] [CrossRef] [Green Version]
- López-Gómez, J.M.; Pérez-Flores, I.; Jofré, R.; Carretero, D.; Rodríguez-Benitez, P.; Villaverde, M.; Pérez-García, R.; Nassar, G.M.; Niembro, E.; Ayus, J.C. Presence of a failed kidney transplant in patients who are on hemodialysis is associated with chronic inflammatory state and erythropoietin resistance. J. Am. Soc. Nephrol. 2004, 15, 2494–2501. [Google Scholar] [CrossRef] [PubMed]
- Ojo, A.O.; Wolfe, R.A.; Agoda, L.Y.; Held, P.J.; Port, F.K.; Leavey, S.F.; Callard, S.E.; Dickinson, D.M.; Schmouder, R.L.; Leichtman, A.B. Prognosis after primary renal transplant failure and the beneficial effects of repeat transplantation: Multivariate analyses from the United States Renal Data System. Transplantation 1998, 66, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- McCaughan, J.A.; Patterson, C.C.; Maxwell, A.P.; Courtney, A.E. Factors influencing survival after kidney transplant failure. Transplant. Res. 2014, 3, 18. [Google Scholar] [CrossRef] [PubMed]
- Leeaphorn, N.; Thongprayoon, C.; Chewcharat, A.; Hansrivijit, P.; Jadlowiec, C.C.; Cummings, L.S.; Katari, S.; Mao, S.A.; Mao, M.A.; Cheungpasitporn, W. Outcomes of kidney retransplantation in recipients with prior posttransplant lymphoproliferative disorders: An analysis of the 2000-2019 UNOS/OPTN database. Am. J. Transplant. 2021, 21, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Leeaphorn, N.; Thongprayoon, C.; Chon, W.J.; Cummings, L.S.; Mao, M.A.; Cheungpasitporn, W. Outcomes of kidney retransplantation after graft loss as a result of BK virus nephropathy in the era of newer immunosuppressant agents. Am. J. Transplant. 2020, 20, 1334–1340. [Google Scholar] [CrossRef] [PubMed]
- Dabare, D.; Kassimatis, T.; Hodson, J.; Khurram, M.A.; Papadakis, G.; Rompianesi, G.; Shaw, O.; Karydis, N.; Callaghan, C.; Olsburgh, J.; et al. Outcomes in Third and Fourth Kidney Transplants Based on the Type of Donor. Transplantation 2019, 103, 1494–1503. [Google Scholar] [CrossRef]
- Sandal, S.; Ahn, J.B.; Cantarovich, M.; Chu, N.M.; Segev, D.L.; McAdams-Demarco, M.A. Evolving Trends in Risk Profiles and Outcomes in Older Adults Undergoing Kidney Retransplantation. Transplantation 2022, 106, 1051–1060. [Google Scholar] [CrossRef]
- Pardinhas, C.; Leal, R.; Figueiredo, C.; Rodrigues, L.; Guedes, M.; Santos, L.; Romãozinho, C.; Sá, H.; Alves, R.; Figueiredo, A. Kidney Retransplant: Not Too Old for a Second Chance. Transplant. Proc. 2022, 54, 1242–1246. [Google Scholar] [CrossRef]
- Girerd, S.; Duarte, K.; Couchoud, C.; Laurain, E.; Courivaud, C.; Bauwens, M.; Kessler, M.; Frimat, L.; Girerd, N. Association between kidney retransplantation and survival according to age in the French national cohort of dialysis patients. Am. J. Transplant. 2022, 22, 2028–2040. [Google Scholar] [CrossRef]
- Khalil, A.K.; Slaven, J.E.; Mujtaba, M.A.; Yaqub, M.S.; Mishler, D.P.; Taber, T.E.; Sharfuddin, A.A.; Khalil, A. Re-transplants compared to primary kidney transplants recipients: A mate kidney paired analysis of the OPTN/UNOS database. Clin. Transplant. 2016, 30, 566–578. [Google Scholar] [CrossRef]
- Management of the Failing Kidney Transplant British Transplantation Society Guidelines; British Transplantation Society: Sheffield, UK, 2014.
- Kainz, A.; Kammer, M.; Reindl-Schwaighofer, R.; Strohmaier, S.; Petr, V.; Viklicky, O.; Abramowicz, D.; Naik, M.; Mayer, G.; Oberbauer, R. Waiting Time for Second Kidney Transplantation and Mortality. Clin. J. Am. Soc. Nephrol. 2022, 17, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Chua, S.; Chadban, S.J.; Clayton, P.; Pilmore, H.; Hughes, P.D.; Ferrari, P.; Lim, W.H. Waiting Time Between Failure of First Graft and Second Kidney Transplant and Graft and Patient Survival. Transplantation 2016, 100, 1767–1775. [Google Scholar] [CrossRef] [PubMed]
- Redfield, R.R.; Scalea, J.R.; Zens, T.J.; Mandelbrot, D.A.; Leverson, G.; Kaufman, D.B.; Djamali, A. The mode of sensitization and its influence on allograft outcomes in highly sensitized kidney transplant recipients. Nephrol. Dial. Transplant. 2016, 31, 1746–1753. [Google Scholar] [CrossRef] [PubMed]
- Campos, A.; Malheiro, J.; Tafulo, S.; Santos, S.; Dias, L.; Martins, L.S.; Almeida, M.; Pedroso, S.; Henriques, A.C.; Cabrita, A. Increase of allosensitization after a kidney graft failure: Predictors and effect on retransplantation outcomes. Nefrologia 2017, 37, 397–405. [Google Scholar] [CrossRef]
- Sullivan, H.C.; Gebel, H.M.; Bray, R.A. Understanding solid-phase HLA antibody assays and the value of MFI. Hum. Immunol. 2017, 78, 471. [Google Scholar] [CrossRef]
- Malheiro, J.; Tafulo, S. Clinical implications of anti-HLA antibodies testing in kidney transplantation. Port. J. Nephrol. Hypertens. 2018, 32, 5–14. [Google Scholar]
- Salvadori, M.; Bertoni, E. Renal transplant allocation criteria, desensitization strategies and immunosuppressive therapy in retransplant renal patients. J. Nephrol. 2012, 25, 890–899. [Google Scholar] [CrossRef]
- Gombos, P.; Opelz, G.; Scherer, S.; Morath, C.; Zeier, M.; Schemmer, P.; Süsal, C. Influence of test technique on sensitization status of patients on the kidney transplant waiting list. Am. J. Transplant. 2013, 13, 2075–2082. [Google Scholar] [CrossRef]
- Snanoudj, R.; Kamar, N.; Cassuto, E.; Caillard, S.; Metzger, M.; Merville, P.; Thierry, A.; Jollet, I.; Grimbert, P.; Anglicheau, D.; et al. Epitope load identi fi es kidney transplant recipients at risk of allosensitization following minimization of immunosuppression. Kidney Int. 2019, 95, 1471–1485. [Google Scholar] [CrossRef]
- Duquesnoy, R.J. HLAMatchmaker: A molecularly based algorithm for histocompatibility determination. I. Description of the algorithm. Hum. Immunol. 2002, 63, 339–352. [Google Scholar] [CrossRef]
- Claas, F.H.J.; Witvliet, M.D.; Duquesnoy, R.J.; Persijn, G.G.; Doxiadis, I.I.N. The acceptable mismatch program as a fast tool for highly sensitized patients awaiting a cadaveric kidney transplantation: Short waiting time and excellent graft outcome. Transplantation 2004, 78, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Bestard, O.; Couzi, L.; Crespo, M.; Kessaris, N.; Thaunat, O. Stratifying the humoral risk of candidates to a solid organ transplantation: A proposal of the ENGAGE working group Transplant International. Transpl. Int. 2021, 34, 1005–1018. [Google Scholar] [CrossRef] [PubMed]
- Mills, D.M.; Cambier, J.C. B lymphocyte activation during cognate interactions with CD4+ T lymphocytes: Molecular dynamics and immunologic consequences. Semin. Immunol. 2003, 15, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Heidt, S.; Eikmans, M.; Roelen, D.L.; van Kooten, C.; Claas, F.H.J. Immunogenetics and immunology of transplantation in Leiden. Transpl. Immunol. 2014, 31, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Wehmeier, C.; Karahan, G.E.; Krop, J.; De Vaal, Y.; Langerak-Langerak, J.; Binet, I.; Schaub, S.; Roelen, D.L.; Claas, F.H.J.; Heidt, S. Donor-specific B Cell Memory in Alloimmunized Kidney Transplant Recipients: First Clinical Application of a Novel Method. Transplantation 2020, 104, 1026–1032. [Google Scholar] [CrossRef]
- Singh, P.; Filippone, E.J.; Colombe, B.W.; Shah, A.P.; Zhan, T.; Harach, M.; Gorn, C.; Frank, A.M. Sensitization trends after renal allograft failure: The role of DQ eplet mismatches in becoming highly sensitized. Clin. Transplant. 2016, 30, 71–80. [Google Scholar] [CrossRef]
- Tambur, A.R.; Kosmoliaptsis, V.; Claas, F.H.J.; Mannon, R.B.; Nickerson, P.; Naesens, M. Significance of HLA-DQ in kidney transplantation: Time to reevaluate human leukocyte antigen-matching priorities to improve transplant outcomes? An expert review and recommendations. Kidney Int. 2021, 100, 1012–1022. [Google Scholar] [CrossRef]
- Lee, H.; Min, J.W.; Kim, J.I.; Moon, I.S.; Park, K.H.; Yang, C.W.; Chung, B.H.; Oh, E.J. Clinical Significance of HLA-DQ Antibodies in the Development of Chronic Antibody-Mediated Rejection and Allograft Failure in Kidney Transplant Recipients. Medicine 2016, 95, e3094. [Google Scholar] [CrossRef]
- Jameson, S.C.; Masopust, D. Diversity in T cell memory: An embarrassment of riches. Immunity 2009, 31, 859–871. [Google Scholar] [CrossRef]
- Tinckam, K.J.; Rose, C.; Hariharan, S.; Gill, J. Re-Examining Risk of Repeated HLA Mismatch in Kidney Transplantation. J. Am. Soc. Nephrol. 2016, 27, 2833–2841. [Google Scholar] [CrossRef]
- Regrafts—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/1306711/ (accessed on 24 June 2022).
- Doxiadis, I.I.N.; De Lange, P.; D’Amaro, J.; De Meester, J.; Schreuder, G.M.T.; Claas, F.H.J. Repeated HLA mismatches in cadaveric renal transplantation: Is it safe to transplant? Transplant. Proc. 1997, 29, 1408–1409. [Google Scholar] [CrossRef]
- Mjörnstedt, L.; Nyberg, G.; Olausson, M.; Karlberg, I.; Konar, J.; Sandberg, L. Renal retransplantation in patients with HLA-antibodies. Transpl. Int. 1992, 5 (Suppl. 1), 32–34. [Google Scholar] [CrossRef]
- Does Re-Exposure to Mismatched HLA Antigens Decrease Renal Re-Transplant Allograft Survival?—PubMed [Internet]. Available online: https://pubmed.ncbi.nlm.nih.gov/8664509/ (accessed on 24 June 2022).
- Coupel, S.; Giral-Classe, M.; Karam, G.; Morcet, J.F.; Dantal, J.; Cantarovich, D.; Blancho, G.; Bignon, J.D.; Daguin, P.; Soulillou, J.P.; et al. Ten-year survival of second kidney transplants: Impact of immunologic factors and renal function at 12 months. Kidney Int. 2003, 64, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Augustine, J.J.; Woodside, K.J.; Padiyar, A.; Sanchez, E.Q.; Hricik, D.E.; Schulak, J.A. Independent of Nephrectomy, Weaning Immunosuppression Leads to Late Sensitization After Kidney Transplant Failure. Transplant. J. 2012, 94, 738–743. [Google Scholar] [CrossRef]
- Martin, K.; Cantwell, L.; Barraclough, K.A.; Lian, M.; Masterson, R.; Hughes, P.D.; Chow, K.V. Prolonged immunosuppression does not improve risk of sensitization or likelihood of retransplantation after kidney transplant graft failure. Transpl. Int. 2021, 34, 2353–2362. [Google Scholar] [CrossRef]
- Knoll, G.; Campbell, P.; Chassé, M.; Fergusson, D.; Ramsay, T.; Karnabi, P.; Perl, J.; House, A.A.; Kim, J.; Johnston, O.; et al. Immunosuppressant Medication Use in Patients with Kidney Allograft Failure: A Prospective Multicenter Canadian Cohort Study. J. Am. Soc. Nephrol. 2022, 33, 1182–1192. [Google Scholar] [CrossRef]
- Smak Gregoor, P.J.H.; Zietse, R.; Van Saase, J.L.C.M.; De Op Hoek, C.T.; Ijzermans, J.N.M.; Lavrijssen, A.T.J.; De Jong, G.; Kramer, P.; Weimar, W. Immunosuppression should be stopped in patients with renal allograft failure. Clin. Transplant. 2001, 15, 397–401. [Google Scholar] [CrossRef]
- Ryu, H.; Kim, Y.C.; Moon, J.J.; Song, E.Y.; Min, S.; Ha, J.; Joo, K.W.; Kim, Y.S.; Ahn, C.; Lee, H. Weaning Immunosuppressant in Patients with Failing Kidney Grafts and The Outcomes: A Single-Center Retrospective Cohort Study. Sci. Rep. 2020, 10, 6425–6429. [Google Scholar] [CrossRef]
- Lubetzky, M.; Tantisattamo, E.; Molnar, M.Z.; Lentine, K.L.; Basu, A.; Parsons, R.F.; Woodside, K.J.; Pavlakis, M.; Blosser, C.D.; Singh, N.; et al. The failing kidney allograft: A review and recommendations for the care and management of a complex group of patients. Am. J. Transplant. 2021, 21, 2937–2949. [Google Scholar] [CrossRef]
- Nimmo, A.M.S.A.; McIntyre, S.; Turner, D.M.; Henderson, L.K.; Battle, R.K. The impact of withdrawal of maintenance immunosuppression and graft nephrectomy on HLA sensitization and calculated chance of future transplant. Transplant. Direct 2018, 4, e409. [Google Scholar] [CrossRef]
- Ghyselen, L.; Naesens, M. Indications, risks and impact of failed allograft nephrectomy. Transplant. Rev. 2019, 33, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Del Bello, A.; Congy-Jolivet, N.; Sallusto, F.; Guilbeau-Frugier, C.; Cardeau-Desangles, I.; Fort, M.; Esposito, L.; Guitard, J.; Cointault, O.; Lavayssière, L.; et al. Donor-specific antibodies after ceasing immunosuppressive therapy, with or without an allograft nephrectomy. Clin. J. Am. Soc. Nephrol. 2012, 7, 1310–1319. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.C.; Quartel, A.W.; Czer, L.S.C.; Admon, D.; Chen, G.; Fishbein, M.C.; Schwieger, J.; Steiner, R.W.; Davis, C.; Tyan, D.B. Posttransplant therapy using high-dose human immunoglobulin (intravenous gammaglobulin) to control acute humoral rejection in renal and cardiac allograft recipients and potential mechanism of action. Transplantation 1998, 66, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.C.; Vo, A.; Bunnapradist, S.; Toyoda, M.; Peng, A.; Puliyanda, D.; Kamil, E.; Tyan, D. Intravenous immune globulin treatment inhibits crossmatch positivity and allows for successful transplantation of incompatible organs in living-donor and cadaver recipients. Transplantation 2003, 76, 631–636. [Google Scholar] [CrossRef]
- Vo, A.A.; Lukovsky, M.; Toyoda, M.; Wang, J.; Reinsmoen, N.L.; Lai, C.-H.; Peng, A.; Villicana, R.; Jordan, S.C. Rituximab and intravenous immune globulin for desensitization during renal transplantation. N. Engl. J. Med. 2008, 359, 242–251. [Google Scholar] [CrossRef]
- Montgomery, R.A.; Lonze, B.E.; King, K.E.; Kraus, E.S.; Kucirka, L.M.; Locke, J.E.; Warren, D.S.; Simpkins, C.E.; Dagher, N.N.; Singer, A.L.; et al. Desensitization in HLA-Incompatible Kidney Recipients and Survival. N. Engl. J. Med. 2011, 365, 318–326. [Google Scholar] [CrossRef]
- Stegall, M.D.; Gloor, J.; Winters, J.L.; Moore, S.B.; DeGoey, S. A comparison of plasmapheresis versus high-dose IVIG desensitization in renal allograft recipients with high levels of donor specific alloantibody. Am. J. Transplant. 2006, 6, 346–351. [Google Scholar] [CrossRef]
- Vo, A.A.; Peng, A.; Toyoda, M.; Kahwaji, J.; Cao, K.; Lai, C.H.; Reinsmoen, N.L.; Villicana, R.; Jordan, S.C. Use of intravenous immune globulin and rituximab for desensitization of highly HLA-sensitized patients awaiting kidney transplantation. Transplantation 2010, 89, 1095–1102. [Google Scholar] [CrossRef]
- Vo, A.A.; Choi, J.; Cisneros, K.; Reinsmoen, N.; Haas, M.; Ge, S.; Toyoda, M.; Kahwaji, J.; Peng, A.; Villicana, R.; et al. Benefits of rituximab combined with intravenous immunoglobulin for desensitization in kidney transplant recipients. Transplantation 2014, 98, 312–319. [Google Scholar] [CrossRef]
- Loupy, A.; Suberbielle-Boissel, C.; Zuber, J.; Anglicheau, D.; Timsit, M.O.; Martinez, F.; Thervet, E.; Bruneval, P.; Charron, D.; Hill, G.S.; et al. Combined posttransplant prophylactic IVIg/anti-CD 20/plasmapheresis in kidney recipients with preformed donor-specific antibodies: A pilot study. Transplantation 2010, 89, 1403–1410. [Google Scholar] [CrossRef]
- Shaffer, D.; Feurer, I.D.; Crowe, D.; Schaefer, H. Early and Sustained Reduction in Donor-Specific Antibodies in Desensitized Living Donor Kidney Transplant Recipients: A 3-Year Prospective Study. Transplant. Direct 2016, 2, E62. [Google Scholar] [CrossRef] [PubMed]
- Kozlowski, T.; Andreoni, K.A. Limitations of rituximab/IVIg desensitization protocol in kidney transplantation; is this better than a tincture of time? Ann. Transplant. 2011, 16, 19–25. [Google Scholar] [CrossRef]
- Vo, A.A.; Petrozzino, J.; Yeung, K.; Sinha, A.; Kahwaji, J.; Peng, A.; Villicana, R.; MacKowiak, J.; Jordan, S.C. Efficacy, outcomes, and cost-effectiveness of desensitization using IVIG and rituximab. Transplantation 2013, 95, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.C.; Jambaldorj, E.; Kwon, H.Y.; Kim, M.G.; Im, H.J.; Jeon, H.J.; In, J.W.; Han, M.; Koo, T.Y.; Chung, J.; et al. Desensitization Using Bortezomib and High-dose Immunoglobulin Increases Rate of Deceased Donor Kidney Transplantation. Medicine 2016, 95, e2635. [Google Scholar] [CrossRef]
- Everly, M.J.; Terasaki, P.I.; Trivedi, H.L. Durability of antibody removal following proteasome inhibitor-based therapy. Transplantation 2012, 93, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, M.A.M.; Gandhi, M.J.; Schinstock, C.A.; Moore, N.A.; Smith, B.H.; Braaten, N.Y.; Stegall, M.D. 32 doses of bortezomib for desensitization is not well-tolerated and is associated with only modest reductions in anti-HLA antibody. Transplantation 2017, 101, 1222. [Google Scholar] [CrossRef]
- Stegall, M.D.; Diwan, T.; Raghavaiah, S.; Cornell, L.D.; Burns, J.; Dean, P.G.; Cosio, F.G.; Gandhi, M.J.; Kremers, W.; Gloor, J.M. Terminal complement inhibition decreases antibody-mediated rejection in sensitized renal transplant recipients. Am. J. Transplant. 2011, 11, 2405–2413. [Google Scholar] [CrossRef]
- Fogal, B.; Yi, T.; Wang, C.; Rao, D.A.; Lebastchi, A.; Kulkarni, S.; Tellides, G.; Pober, J.S. Neutralizing IL-6 reduces human arterial allograft rejection by allowing emergence of CD161(+) CD4(+) T regulatory cells. J. Immunol. 2011, 187, 6268. [Google Scholar] [CrossRef]
- Redfield, R.R.; Jordan, S.C.; Busque, S.; Vincenti, F.; Woodle, E.S.; Desai, N.; Reed, E.F.; Tremblay, S.; Zachary, A.A.; Vo, A.A.; et al. Safety, pharmacokinetics, and pharmacodynamic activity of obinutuzumab, a type 2 anti-CD20 monoclonal antibody for the desensitization of candidates for renal transplant. Am. J. Transplant. 2019, 19, 3035. [Google Scholar] [CrossRef]
- Jordan, S.C.; Lorant, T.; Choi, J.; Kjellman, C.; Winstedt, L.; Bengtsson, M.; Zhang, X.; Eich, T.; Toyoda, M.; Eriksson, B.-M.; et al. IgG Endopeptidase in Highly Sensitized Patients Undergoing Transplantation. N. Engl. J. Med. 2017, 377, 442–453. [Google Scholar] [CrossRef]
- Jordan, S.C.; Legendre, C.; Desai, N.M.; Lorant, T.; Bengtsson, M.; Lonze, B.E.; Vo, A.A.; Runström, A.; Laxmyr, L.; Sjöholm, K.; et al. Imlifidase Desensitization in Crossmatch-positive, Highly Sensitized Kidney Transplant Recipients: Results of an International Phase 2 Trial (Highdes). Transplantation 2021, 105, 1808–1817. [Google Scholar] [CrossRef] [PubMed]
- Lonze, B.E. A review of imlifidase in solid organ transplantation. Expert Opin. Biol. Ther. 2021, 21, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Orandi, B.J.; Luo, X.; Massie, A.B.; Garonzik-Wang, J.M.; Lonze, B.E.; Ahmed, R.; Van Arendonk, K.J.; Stegall, M.D.; Jordan, S.C.; Oberholzer, J.; et al. Survival Benefit with Kidney Transplants from HLA-Incompatible Live Donors. N. Engl. J. Med. 2016, 374, 940–950. [Google Scholar] [CrossRef] [PubMed]
- Saran, R.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.C.; Bragg-Gresham, J.; Balkrishnan, R.; Bhave, N.; Dietrich, X.; Ding, Z.; Eggers, P.W.; et al. US Renal Data System 2018 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2019, 73, A7–A8. [Google Scholar] [CrossRef] [PubMed]
- De Groot, I.B.; Veen, J.I.E.; van der Boog, P.J.M.; van Dijk, S.; Stiggelbout, A.M.; Marang-van de Mheen, P.J.; Baranski, A.G.; Van der Boog, P.J.M.; Dam, R.E.; Dekker, F.W.; et al. Difference in quality of life, fatigue and societal participation between living and deceased donor kidney transplant recipients. Clin. Transplant. 2013, 27, E415–E423. [Google Scholar] [CrossRef]
- Bellini, M.I.; Courtney, A.E.; McCaughan, J.A. Living Donor Kidney Transplantation Improves Graft and Recipient Survival in Patients with Multiple Kidney Transplants. J. Clin. Med. 2020, 9, 2118. [Google Scholar] [CrossRef]
- Husain, S.A.; King, K.L.; Sanichar, N.; Crew, R.J.; Schold, J.D.; Mohan, S. Association Between Donor-Recipient Biological Relationship and Allograft Outcomes After Living Donor Kidney Transplant. JAMA Netw. Open 2021, 4, e215718. [Google Scholar] [CrossRef]
- Saat, T.C.; van den Akker, E.K.; IJzermans, J.N.M.; Dor, F.J.M.F.; de Bruin, R.W.F. Improving the outcome of kidney transplantation by ameliorating renal ischemia reperfusion injury: Lost in translation? J. Transl. Med. 2016, 14, 20. [Google Scholar] [CrossRef]
- Marfo, K.; Lu, A.; Ling, M.; Akalin, E. Desensitization protocols and their outcome. Clin. J. Am. Soc. Nephrol. 2011, 6, 922–936. [Google Scholar] [CrossRef]
- Kher, V.; Jha, P.K. Paired kidney exchange transplantation—Pushing the boundaries. Transpl. Int. 2020, 33, 975–984. [Google Scholar] [CrossRef]
- Ferrari, P.; Weimar, W.; Johnson, R.J.; Lim, W.H.; Tinckam, K.J. Kidney paired donation: Principles, protocols and programs. Nephrol. Dial. Transplant. 2015, 30, 1276–1285. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, R.A.; Lonze, B.E.; Jackson, A.M. Using donor exchange paradigms with desensitization to enhance transplant rates among highly sensitized patients. Curr. Opin. Organ Transplant. 2011, 16, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Flechner, S.M.; Thomas, A.G.; Ronin, M.; Veale, J.L.; Leeser, D.B.; Kapur, S.; Peipert, J.D.; Segev, D.L.; Henderson, M.L.; Shaffer, A.A.; et al. The first 9 years of kidney paired donation through the National Kidney Registry: Characteristics of donors and recipients compared with National Live Donor Transplant Registries. Am. J. Transplant. 2018, 18, 2730–2738. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Snyder, J.J.; Matas, A.J.; Ellison, M.D.; Gill, J.S.; Kausz, A.T. Preemptive kidney transplantation: The advantage and the advantaged. J. Am. Soc. Nephrol. 2002, 13, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.S.; Tonelli, M.; Johnson, N.; Pereira, B.J.G. Why do preemptive kidney transplant recipients have an allograft survival advantage? Transplantation 2004, 78, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Florit, E.A.; Bennis, S.; Rodriguez, E.; Revuelta, I.; De Sousa, E.; Esforzado, N.; Cofán, F.; Ricart, M.J.; Torregrosa, J.V.; Campistol, J.M.; et al. Pre-Emptive Retransplantation in Patients with Chronic Kidney Graft Failure. Transplant. Proc. 2015, 47, 2351–2353. [Google Scholar] [CrossRef]
- Gill, J.S.; Johnston, O.; Rose, C.L.; Gill, J.S. Risks and benefits of preemptive second kidney transplantation. Transplantation 2013, 95, 705–710. [Google Scholar]
- Vinson, A.J.; Kiberd, B.A.; West, K.; Mannon, R.B.; Foster, B.J.; Tennankore, K.K. Disparities in Access to Preemptive Repeat Kidney Transplant: Still Missing the Mark? Kidney360 2021, 3, 144–152. [Google Scholar] [CrossRef]
- Girerd, S.; Girerd, N.; Duarte, K.; Giral, M.; Legendre, C.; Mourad, G.; erie Garrigue, V.; Morelon, E.; Buron, F.; Kamar, N.; et al. Preemptive second kidney transplantation is associated with better graft survival compared with non-preemptive second transplantation: A multicenter French 2000-2014 cohort study Transplant International. Transpl. Int. 2018, 31, 408–423. [Google Scholar] [CrossRef]
- Huang, H.; Li, X.; Zhu, J.; Ye, S.; Zhang, H.; Wang, W.; Wu, X.; Peng, J.; Xu, B.; Lin, Y.; et al. Entecavir vs lamivudine for prevention of hepatitis B virus reactivation among patients with untreated diffuse large B-cell lymphoma receiving R-CHOP chemotherapy: A randomized clinical trial. JAMA-J. Am. Med. Assoc. 2014, 312, 2521–2530. [Google Scholar] [CrossRef]
- Heidt, S.; Haasnoot, G.W.; Claas, F.H.J. How the definition of acceptable antigens and epitope analysis can facilitate transplantation of highly sensitized patients with excellent long-term graft survival. Curr. Opin. Organ Transplant. 2018, 23, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Heidt, S.; Haasnoot, G.W.; van der Linden-van Oevelen, M.J.H.; Claas, F.H.J. Highly Sensitized Patients Are Well Served by Receiving a Compatible Organ Offer Based on Acceptable Mismatches. Front. Immunol. 2021, 12, 687254. [Google Scholar] [CrossRef] [PubMed]
- Kidney Offering Scheme—ODT Clinical—NHS Blood and Transplant [Internet]. Available online: https://www.odt.nhs.uk/odt-structures-and-standards/odt-hub-programme/kidney-offering-scheme/ (accessed on 11 July 2022).
- Watson, C.J.E.; Johnson, R.J.; Mumford, L. Overview of the Evolution of the UK Kidney Allocation Schemes. Curr. Transplant. Rep. 2020, 7, 140–144. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Highly Sensitized Definition | Strategies to Increase Transplantation in the Highly Sensitized | Consequences | |
|---|---|---|---|
| KAS (2014) | cPRA ≥ 98% |
|
|
| Eurotransplant Acceptable mismatch program (1989) | cPRA ≥ 85% (Include only HLA antibodies explained by sensitizing events) |
|
|
| Scandiatransplant Acceptable mismatch program (2020) | cPRA ≥ 80% |
|
|
| UK allocation program (2019) | cRF > 85% |
|
|
| Spain PATHI (2015) | cPRA ≥ 98% |
|
|
| France Authorized Antigen Program | cPRA ≥ 85% or cPRA > 70% at transplant |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leal, R.; Pardinhas, C.; Martinho, A.; Sá, H.O.; Figueiredo, A.; Alves, R. Strategies to Overcome HLA Sensitization and Improve Access to Retransplantation after Kidney Graft Loss. J. Clin. Med. 2022, 11, 5753. https://doi.org/10.3390/jcm11195753
Leal R, Pardinhas C, Martinho A, Sá HO, Figueiredo A, Alves R. Strategies to Overcome HLA Sensitization and Improve Access to Retransplantation after Kidney Graft Loss. Journal of Clinical Medicine. 2022; 11(19):5753. https://doi.org/10.3390/jcm11195753
Chicago/Turabian StyleLeal, Rita, Clara Pardinhas, António Martinho, Helena Oliveira Sá, Arnaldo Figueiredo, and Rui Alves. 2022. "Strategies to Overcome HLA Sensitization and Improve Access to Retransplantation after Kidney Graft Loss" Journal of Clinical Medicine 11, no. 19: 5753. https://doi.org/10.3390/jcm11195753