
Effects of Reminiscence Therapy on Cognition, Depression and Quality of Life in Elderly People with Alzheimer’s Disease: A Systematic Review of Randomized Controlled Trials
 and
and
Abstract
:1. Introduction
1.1. Alzheimer’s Disease (AD): Clinical Features and Assessment Tools
1.2. Pharmacological and Non-Pharmacological Interventions in AD
1.3. Reminiscence Therapy
1.4. Aim of the Study
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection Criteria
2.3. Outcome Measures
2.4. Quality of the Studies and Assessment of Risk of Bias Evaluation
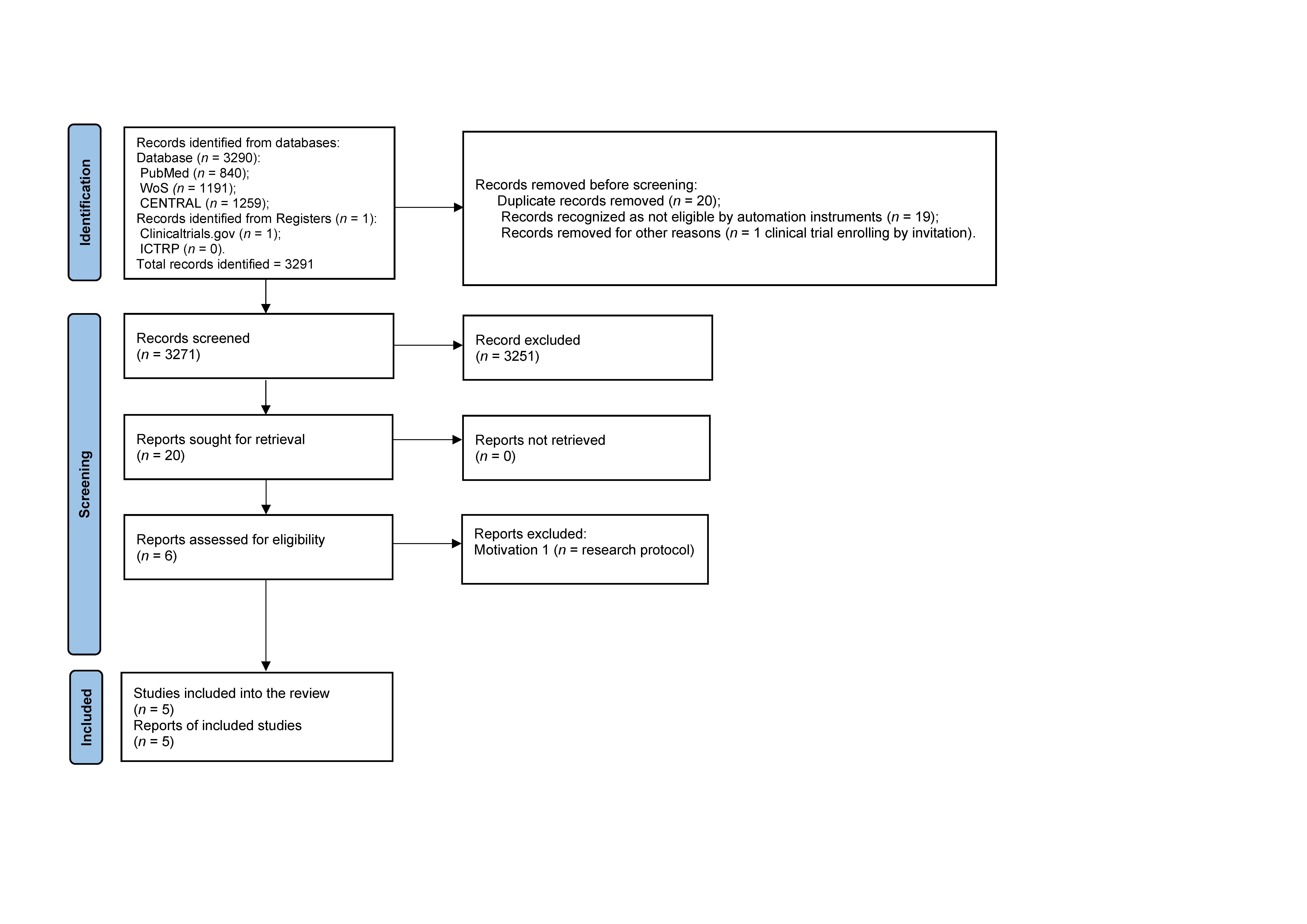
3. Results
Study Selection, Evaluation, and Report
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations; Department of Economic and Social Affairs; Population Division. World Population Ageing 2019: Highlights (ST/ESA/SER.A/430); United Nations: New York, NY, USA, 2019; pp. 5–10. [Google Scholar]
- Sink, K.M.; Covinsky, K.E.; Barnes, D.E.; Newcomer, R.J.; Yaffe, K. Caregiver characteristics are associated with neuropsychiatric symptoms of dementia. JAGS 2006, 54, 796–803. [Google Scholar] [CrossRef]
- Cammisuli, D.M.; Franzoni, F.; Scarfò, G.; Fusi, J.; Gesi, M.; Bonuccelli, U.; Daniele, S.; Castelnuovo, G. What Does the Brain Have to Keep Working at Its Best? Resilience Mechanisms Such as Antioxidants and Brain/Cognitive Reserve for Counteracting Alzheimer’s Disease Degeneration. Biology 2022, 11, 650. [Google Scholar] [CrossRef] [PubMed]
- Freitas, S.; Simões, M.R.; Alves, L.; Santana, I. Montreal cognitive assessment: Validation study for mild cognitive impairment and Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2013, 27, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-Mental State: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Fratiglioni, L.; Jorm, A.F.; Grut, M.; Viitanen, M.; Holmén, K.; Ahlbom, A.; Winblad, B. Predicting dementia from the Mini-Mental State Examination in an elderly population: The role of education. J. Clin. Epidemiol. 1993, 46, 281–287. [Google Scholar] [CrossRef]
- Brousseau, G.; Rourke, B.P.; Burke, B. Acetylcholinesterase inhibitors, neuropsychiatric symptoms, and Alzheimer’s disease subtypes: An alternate hypothesis to global cognitive enhancement. Exp. Clin. Psychophacol. 2007, 15, 546–554. [Google Scholar] [CrossRef]
- van Dalen-Kok, A.H.; Pieper, M.J.; de Waal, M.W.; Lukas, A.; Husebo, B.S.; Achterberg, W.P. Association between pain, neuropsychiatric symptoms, and physical function in dementia: A systematic review and meta-analysis. BMC Geriatr. 2005, 15, 1–18. [Google Scholar]
- Lyketsos, C.G.; Carrillo, M.C.; Ryan, J.M.; Khachaturian, A.S.; Trzepacz, P.; Amatniek, J. Neuropsychiatric symptoms in Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 532–539. [Google Scholar]
- Asmer, M.S.; Kirkham, J.; Newton, H.; Ismail, Z.; Elbayoumi, H.; Leung, R.H.; Seitz, D.P. Meta-analysis of the prevalence of major depressive disorder among older adults with dementia. J. Clin. Psychiatry 2018, 79, 17r11772. [Google Scholar] [CrossRef]
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The neuropsychiatric inventory: Comprehensive assessment of psychopathology in dementia. Neurology 2014, 44, 2308–2314. [Google Scholar] [CrossRef]
- Lai, C.K. The merits and problems of the Neuropsychiatric Inventory as an assessment tool in people with dementia and other neurological disorders. Clin. Interv. Aging 2014, 9, 1051–1061. [Google Scholar] [CrossRef] [PubMed]
- Kørner, A.; Lauritzen, L.; Abelskov, K.; Gulmann, N.; Marie Brodersen, A.; Wedervang-Jensen, T.; Marie Kjeldgaard, K. The geriatric depression scale and the cornell scale for depression in dementia. A validity study. Nord. J. Psychiatry 2006, 60, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Dodek, P.M.; You, J.J.; Sinuff, T.; Hiebert, T.; Tayler, C.; Jiang, X.; Simon, J.; Downar, J. Validation of quality indicators for the ACCEPT Study Team and the Canadian Researchers at the End of Life Network (CARENET). Validation of quality indicators for end-of-life communication: Results of a multicentre survey. Cmaj 2017, 189, E980–E989. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P. Quality of life in Alzheimer disease. Alzheimer Dis. Assoc. Disord. 1994, 8, 138–150. [Google Scholar] [CrossRef]
- Logsdon, R.G.; Gibbons, L.E.; McCurry, S.M.; Teri, L. Assessing quality of life in older adults with cognitive impairment. Psychosom. Med. 2002, 64, 510–519. [Google Scholar] [CrossRef]
- Burks, H.B.; des Bordes, J.K.; Chadha, R.; Holmes, H.M.; Rianon, N.J. Quality of Life assessment in older adults with dementia: A systematic review. Dement. Geriatr. Cogn. 2021, 50, 103–110. [Google Scholar] [CrossRef]
- Kane, R.A. Definition, measurement, and correlates of quality of life in nursing homes: Towards a reasonable practice, research and policy agenda. Gerontologist 2003, 43, 28–36. [Google Scholar] [CrossRef]
- Kane, R.A.; Kling, K.C.; Bershadsky, B.; Kane, R.L.; Giles, K.; Degenholtz, H.B.; Liu, J.; Cutler, L. Quality of life measures for nursing home residents. J. Gerontol. Med. Sci. 2003, 58, M240–M248. [Google Scholar] [CrossRef]
- Helmes, E.; Csapo, K.G.; Short, J.A. Standardization and validation of the multidimensional observation scale for elderly subjects (MOSES). J. Gerontol. 1987, 42, 395–405. [Google Scholar] [CrossRef]
- Pruchno, R.A.; Kleban, M.H.; Resh, N.L. Psychometric assessment of a multidimensional observation scale for the elderly subjects. J. Gerontol. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Douglas, I.J.; Smeeth, L. Exposure to antipsychotics and risk of stroke: Self-controlled case series study. BMJ 2008, 337, a1227. [Google Scholar] [CrossRef] [PubMed]
- Gerlach, L.B.; Kales, H.C. Pharmacological management of neuropsychiatric symptoms of Dementia. Curr. Treat. Options Psychiatry 2020, 7, 489–507. [Google Scholar] [CrossRef] [PubMed]
- Maust, D.T.; Strominger, J.; Bynum, J.P.; Langa, K.M.; Gerlach, L.B.; Zivin, K.; Marcus, S.C. Prevalence of psychotropic and opioid prescription fills among community-dwelling older adults with dementia in the US. JAMA 2020, 324, 706–708. [Google Scholar] [CrossRef] [PubMed]
- Markota, M.; Rummans, T.A.; Bostwick, J.M.; Lapid, M.I. Benzodiazepine use in older adults: Dangers, management, and alternative therapies. Mayo Clin. Proc. 2016, 91, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Kales, H.C.; Gitlin, L.N.; Lyketsos, C.G.; Detroit Expert Panel on the Assessment and Management of the Neuropsychiatric Symptoms of Dementia. Management of neuropsychiatric symptoms of dementia in clinical settings: Recommendations from a multidisciplinary expert panel. JAGS 2014, 62, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Tible, O.P.; Riese, F.; Savaskan, E.; von Gunten, A. Best practice in the management of behavioural and psychological symptoms of dementia. Ther. Adv. Neurol. Disord. 2017, 10, 297–309. [Google Scholar] [CrossRef]
- Cammisuli, D.M.; Danti, S.; Bosinelli, F.; Cipriani, G. Non-pharmacological interventions for people with Alzheimer’s Disease: A critical review of the scientific literature from the last ten years. Eur. Geriatr. Med. 2016, 7, 57–64. [Google Scholar] [CrossRef]
- Abraha, I.; Rimland, J.M.; Lozano-Montoya, I.; Dell’Aquila, G.; Vélez-Díaz-Pallarés, M.; Trotta, F.M.; Cruz-Jento, A.J.; Cherubini, A. Simulated presence therapy for dementia. Cochrane Database Syst. Rev. 2017, 4, CD011882. [Google Scholar] [CrossRef]
- Cammisuli, D.M.; Cipriani, G.; Castelnuovo, G. Technological Solutions for Diagnosis, Management and Treatment of Alzheimer’s Disease-Related Symptoms: A Structured Review of the Recent Scientific Literature. Int. J. Environ. Health Res. 2022, 19, 3122. [Google Scholar] [CrossRef]
- Butler, R.N. The life review: An interpretation of reminiscence in the aged. Psychiatry 1963, 26, 65–76. [Google Scholar] [CrossRef]
- Parker, R.G. Reminiscence as continuity: Comparison of young and older adults. J. Clin. Geropsychol. 1999, 5, 147–155. [Google Scholar] [CrossRef]
- McKeown, J.; Clarke, A.; Repper, J. Life story work in health and social care: Systematic literature review. J. Adv. Nurs. 2006, 55, 237–247. [Google Scholar] [CrossRef]
- Woods, B.; O’Philbin, L.; Farrell, E.M.; Spector, A.E.; Orrell, M. Reminiscence therapy for dementia. Cochrane Database Syst. Rev. 2018, 1, CD001120. [Google Scholar] [CrossRef] [PubMed]
- Thorgrimsen, L.; Schweitzer, P.; Orrell, M. Evaluating reminiscence for people with dementia: A pilot study. Arts Psychother. 2002, 29, 93–97. [Google Scholar] [CrossRef]
- Woods, R.; Orrell, M.; Bruce, E.; Edwards, R.T.; Hoare, Z.; Hounsome, B.; Keady, J.; Moniz-Cook, E.; Orgeta, V.; Rees, J.; et al. REMCARE: Pragmatic Multi-Centre Randomised Trial of Reminiscence Groups for People with Dementia and their Family Carers: Effectiveness and Economic Analysis. PLoS ONE 2016, 11, e0152843. [Google Scholar] [CrossRef]
- Imtiaz, D.; Khan, A.; Seelye, A. A mobile multimedia reminiscence therapy application to reduce behavioral and psychological symptoms in persons with Alzheimer’s. J. Healthc. Eng. 2018, 2018, 1536316. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Ferlisi, G.; Zullo, V.; Schirone, S.; Prisco, R.; Denitto, F. A computer-aided program for helping patients with moderate Alzheimer’s disease engage in verbal reminiscence. Res. Dev. Disabil. 2014, 35, 3026–3033. [Google Scholar] [CrossRef]
- Burnside, I.; Haight, B.K. Reminiscence and life review: Analyzing each concept. J. Adv. Nurs. 1992, 17, 855–862. [Google Scholar] [CrossRef]
- Park, K.; Lee, S.; Yang, J.; Song, T.; Hong, G.R.S. A systematic review and meta-analysis on the effect of reminiscence therapy for people with dementia. Int. Psychogeriatr. 2019, 31, 1581–1597. [Google Scholar] [CrossRef]
- Cotelli, M.; Manenti, R.; Zanetti, O. Reminiscence therapy in dementia: A review. Maturitas 2012, 72, 203–205. [Google Scholar] [CrossRef]
- O’Philbin, L.; Woods, B.; Farrell, E.M.; Spector, A.E.; Orrell, M. Reminiscence therapy for dementia: An abridged Cochrane systematic review of the evidence from randomized controlled trials. Expert Rev. Neurother. 2018, 18, 715–727. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, M.J.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, E.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group* under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Tadaka, E.; Kanagawa, K. Effects of reminiscence group in elderly people with Alzheimer disease and vascular dementia in a community setting. Geriatr. Gerontol. Int. 2007, 7, 167–173. [Google Scholar] [CrossRef]
- Azcurra, D.J.L.S. A reminiscence program intervention to improve the quality of life of long-term care residents with Alzheimer’s disease. A randomized controlled trial. Rev. Bras. Psiquiatr. 2012, 34, 422–433. [Google Scholar] [CrossRef]
- Van Bogaert, P.; Van Grinsven, R.; Tolson, D.; Wouters, K.; Engelborghs, S.; Van der Mussele, S. Effects of SolCos model-based individual reminiscence on older adults with mild to moderate dementia due to Alzheimer disease: A pilot study. JAMA 2013, 14, 528.e9–528.e13. [Google Scholar] [CrossRef]
- Duru Aşiret, G.; Kapucu, S. The effect of reminiscence therapy on cognition, depression, and activities of daily living for patients with Alzheimer disease. J. Geriatr. Neurol. 2016, 29, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Lök, N.; Bademli, K.; Selçuk-Tosun, A. The effect of reminiscence therapy on cognitive functions, depression, and quality of life in Alzheimer patients: Randomized controlled trial. Int. J. Geriatr. Psychiatry 2012, 34, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Irazoki, E.; Garcia-Casal, J.A.; Sanchez-Meca, J.; Franco-Martin, M. Efficacy of group reminiscence therapy for people with dementia. Systematic literature review and meta-analysis. Rev. Neurol. 2017, 65, 447–456. [Google Scholar] [PubMed]
- Douglas, S.; James, I.; Ballard, C. Non-pharmacological interventions in dementia. Adv. Psychiatr. Treat. 2004, 10, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Mitnitski, A.B.; MacKnight, C. Some mathematical models of frailty and their clinical implications. Rev. Clin. Gerontol. 2002, 12, 109–117. [Google Scholar] [CrossRef]
- Mitnitski, A.B.; Song, X.; Rockwood, K. The estimation of relative fitness and frailty in community-dwelling older adults using self-report data. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, M627–M632. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Forsteimer, S. Effects of reminiscence interventions on psychological outcomes: A meta-analysis. Aging Ment. Health 2012, 16, 541–558. [Google Scholar] [CrossRef] [PubMed]
- Macleod, F.; Storey, L.; Rusche, T.; McLaughlin, K. Towards an increased understanding of reminiscence therapy for people with dementia: A narrative analysis. Dementia 2021, 4, 1375–1407. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.M.; Sezgin, D. Effectiveness of reminiscence therapy in reducing agitation and depression and improving quality of life and cognition in long-term care residents with dementia: A systematic review and meta-analysis. Geriatric Nurs. 2021, 42, 1497–1506. [Google Scholar] [CrossRef]


{kind=link}
| Selected Studies | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Tadaka & Kanagawa, 2007 [47] | +/− | - | - | + | + |
| Azcurra, 2012 [48] | +/− | + | + | + | + |
| Van Bogaert et al., 2013 [49] | + | - | - | + | + |
| Duru Asiret and Kapaku, 2015 [50] | - | +/− | + | + | - |
| Lök et al., 2018 [51] | - | + | + | + | - |
| Selected Studies | Selection Bias | Study Design | Confounders | Blinding | Data Collection Methods | Withdrawals and Dropout | Average Score |
|---|---|---|---|---|---|---|---|
| Tadaka & Kanagawa, 2007 [47] | * | *** | *** | *** | *** | ** | *** |
| Azcurra, 2012 [48] | ** | *** | ** | *** | *** | *** | *** |
| Van Bogaert et al., 2013 [49] | * | *** | *** | * | *** | *** | ** |
| Duru Aşiret & Kapaku, 2015 [50] | * | ** | *** | * | ** | *** | ** |
| Lök et al., 2018 [51] | ** | *** | *** | * | *** | *** | *** |
| References | Characteristics of AD Participants | RT Sessions, Type Administration (Individual vs. Group) and Setting | RT Intervention | Outcomes Assessment | Follow-Up | Main Findings |
|---|---|---|---|---|---|---|
| Tadaka & Kanagawa, 2007 [47] | 24 participants assigned to the intervention group (n = 12; mean age, 82.5 ± 6.6) and to the control group (n = 12; mean age, 82.5 ± 6.6) | A group RT of 60–90 min per session, administered once a week for 8 weeks at a geriatric health facility | RT sessions started with the introduction of themes and prompts suitable to individual characteristics and life history, followed by a group discussion, and concluded by a reply of the participant to questions posed by the other ones. | MOSES MMSE | 6-month follow-up | A tendency towards significance in MOSES withdrawal; no improvement in MMSE |
| Azcurra, 2012 [48] | 135 participants assigned to the intervention group (n = 45; mean age, 85.3 ± 5.6), active control group receiving counselling and informal social contact (n = 45; mean age, 86.4 ± 4.9), and passive control group receiving unstructured social contact (n = 45, mean age, 85.8 ± 5.1) | An individual RT intervention delivered for 24 bi-weekly sessions lasting 1 hour each, over a period of 12 weeks at long-term nursing homes | The participants joined a group of peers and the coordinator offers memory triggers (i.e., photographs, recording, and newspaper clippings). Caregivers/relatives of the participants were sometimes included. A general discussion followed, fostering the emergence of shared concepts and reframing of patient’s initiative. | SRQoL | 6-month follow-up | Significant improvement in SRQoL |
| Van Bogaert et al., 2013 [49] | 82 participants assigned to the intervention group (n = 41; age in years mean/range = 83/65–98) and to the control group (n = 41; mean/range = 85/65–101). They were further divided into mild AD (MMSE > 18) and moderate AD (MMSE ≤ 18) | A structured individual RT intervention (i.e., “the SolCoS model”) consisting of two 45 minute sessions per week over a period of 4 weeks at three long-term facilities, two day care centres, and one psychiatric inpatients care facility | A standardized interview on participant awareness about family, home, community and life role. Memories are then evoked and recorded by audio, video, or written documents. Family, profession, holidays, and games are the topics explored. Facilitator’s role as changing agent in reminiscence process is also evaluated. | MMSE GDS CSDD | No follow-up | Improvements in MMSE for participants with moderate AD and in GDS for participants with mild and moderate AD |
| Duru Aşiret & Kapaku, 2015 [50] | 62 participants assigned to the intervention group (n = 31; mean age, 81.8 ± 4.8) and to the control group (n = 31; mean age, 82.2 ± 5.0) | A group RT administered once a week with 30–35 minutes per session for 12 weeks at four Ministry of Family and Social Policies elderly care and rehabilitation centres | RT sessions included introduction, childhood and family life, school days, starting work and work life, a day of fun outside the home, marriage, plants and animals, infants and children, food and cooking, holidays, travel and celebrations, followed by session evaluation and closure. | MMSE GDS | No follow-up | Improvements in MMSE and in GDS |
| Lök et al., 2018 [51] | 60 elderly participants (no mean age was specified) assigned to the intervention group (n = 30) and to the control group (n = 30) | A group RT once a week with 30–35 minutes per session for 12 weeks at a nursing home | RT sessions included discussions about childhood, festivals, memorable travel places, favourite food, important historical events, achievements and music. The participants were then encouraged to remember and share while group leader provides support to make them feeling stronger, valuable, and self-confident. | s-MMSE CSDD QOL-AD | No follow-up | Improvements in s-MMSE, CSDD and QOL-AD |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cammisuli, D.M.; Cipriani, G.; Giusti, E.M.; Castelnuovo, G. Effects of Reminiscence Therapy on Cognition, Depression and Quality of Life in Elderly People with Alzheimer’s Disease: A Systematic Review of Randomized Controlled Trials. J. Clin. Med. 2022, 11, 5752. https://doi.org/10.3390/jcm11195752
Cammisuli DM, Cipriani G, Giusti EM, Castelnuovo G. Effects of Reminiscence Therapy on Cognition, Depression and Quality of Life in Elderly People with Alzheimer’s Disease: A Systematic Review of Randomized Controlled Trials. Journal of Clinical Medicine. 2022; 11(19):5752. https://doi.org/10.3390/jcm11195752
Chicago/Turabian StyleCammisuli, Davide Maria, Gabriele Cipriani, Emanuele Maria Giusti, and Gianluca Castelnuovo. 2022. "Effects of Reminiscence Therapy on Cognition, Depression and Quality of Life in Elderly People with Alzheimer’s Disease: A Systematic Review of Randomized Controlled Trials" Journal of Clinical Medicine 11, no. 19: 5752. https://doi.org/10.3390/jcm11195752