

Face Transplant: Indications, Outcomes, and Ethical Issues—Where Do We Stand?

 ,
,  ,
,
Abstract
:1. Introduction
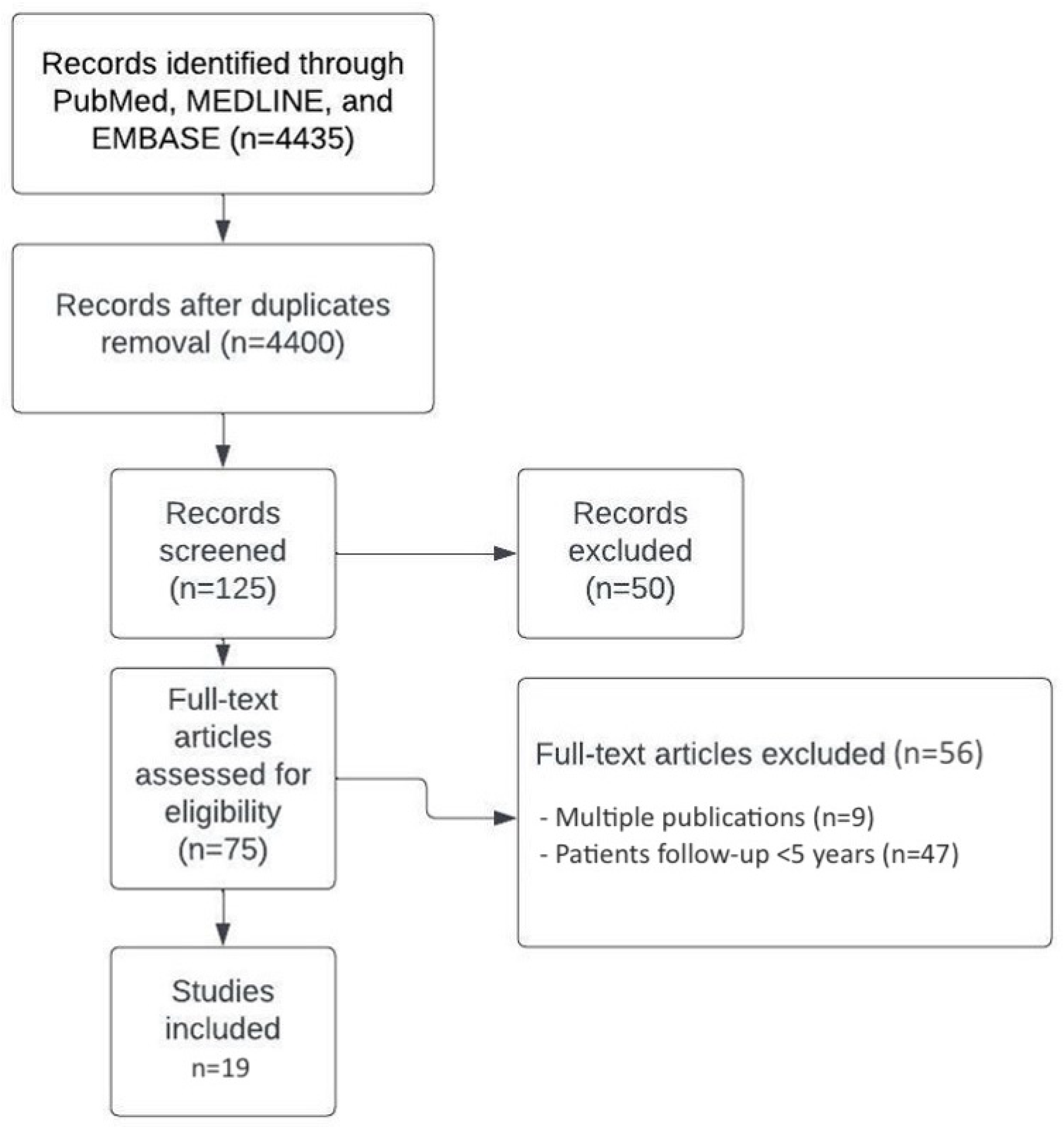
2. Materials and Methods
3. Results
3.1. FT: Surgical Indications
3.1.1. What Kind of Patient Can Really Benefit from Facial VCA?
3.1.2. What Kind of Pathologies Can Lead to Facial VCA?
3.1.3. The Cancer Sequelae Problem
3.2. Preoperative Considerations and Surgical Procedures
3.2.1. Donor Selection
3.2.2. Recipient Preparation
3.2.3. What Does the Procedure Consist of for the Donor?
3.2.4. Operation on the Recipient
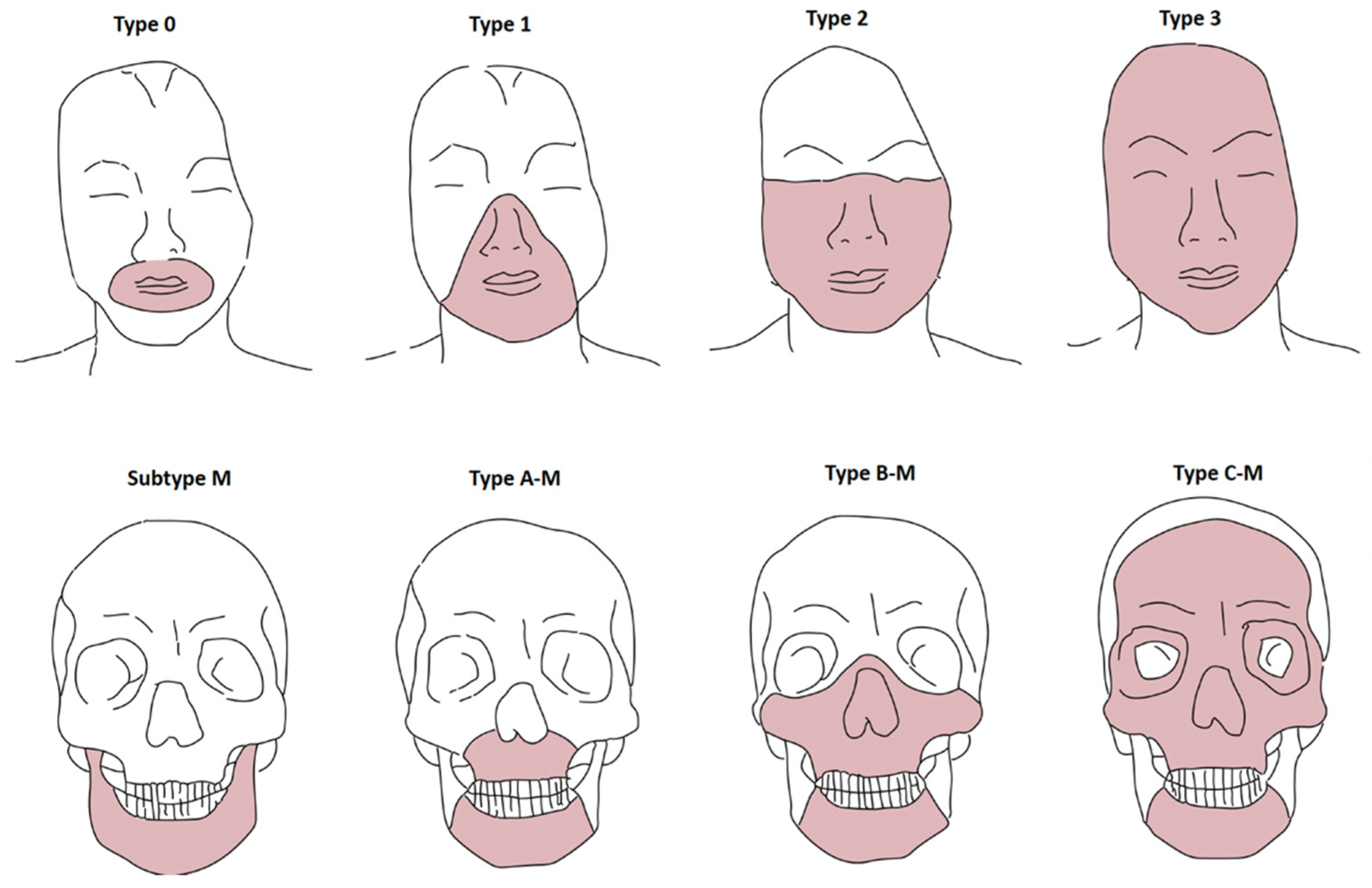
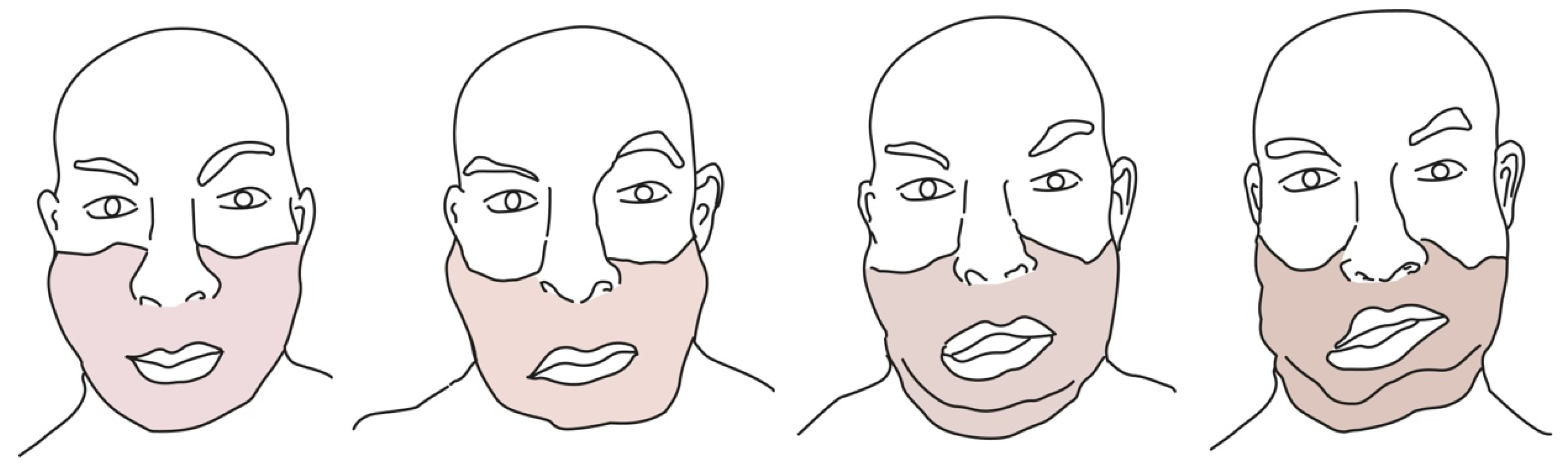
3.3. Facial Defect Classification System for FT
3.4. Immunosuppressive Treatment
3.5. The Importance of Rehabilitation
Functional Recovery
3.6. Immunological Rejection
- CR0: Absence of any clinical or histological evidence of CR.
- CR1: Histological evidence (capillary thrombosis and loss of microvasculature, hair follicle apoptosis, tertiary lymphoid organ-like follicles, skin atrophy and adnexal loss, fibrosis, and vasculopathy/intimal proliferation/hypertrophy) of CR without external evidence or functional decline of the VCA.
- CR2: Clinical and histological (skin atrophy and fibrosis with adnexal loss) evidence of CR in the absence of the functional decline of the VCA.
- CR3: Overt functional decline of the graft with external and histological evidence of CR (skin necrosis, purpuric skin lesions/bruising, adnexal loss, and pain).
3.7. Long-Term Outcomes and Deceased Patients
3.8. Ethical Issues
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Devauchelle, B.; Badet, L.; Lengelé, B.; Morelon, E.; Testelin, S.; Michallet, M.; D’Hauthuille, C.; Dubernard, J.-M. First human face allograft: Early report. Lancet 2006, 368, 203–209. [Google Scholar] [CrossRef]
- Kantar, R.S.; Alfonso, A.R.; Diep, G.K.; Berman, Z.P.; Rifkin, W.J.; Diaz-Siso, J.R.; Sosin, M.; Gelb, B.E.; Ceradini, D.J.; Rodriguez, E.D. Facial Transplantation: Principles and Evolving Concepts. Plast. Reconstr. Surg. 2021, 147, 1022e–1038e. [Google Scholar] [CrossRef] [PubMed]
- Diep, G.K.; Berman, Z.P.; Alfonso, A.R.; Ramly, E.P.; Boczar, D.; Trilles, J.; Colon, R.R.; Chaya, B.F.; Rodriguez, E.D. The 2020 Facial Transplantation Update: A 15-Year Compendium. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3586. [Google Scholar] [CrossRef] [PubMed]
- Kantar, R.S.; Alfonso, A.R.; Ramly, E.P.; Diaz-Siso, J.R.; Jacoby, A.; Sosin, M.; Ceradini, D.J.; Rodriguez, E.D. Incidence of Preventable Nonfatal Craniofacial Injuries and Implications for Facial Transplantation. J. Craniofac. Surg. 2019, 30, 2023–2025. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Chandraker, A.; Arscott, R.; Murphy, G.F.; Lian, C.; Bueno, E.M.; Marty, F.; Rennke, H.G.; Milford, E.; Tullius, S.G.; Pomahac, B. The Management of Antibody-Mediated Rejection in the First Presensitized Recipient of a Full-Face Allotransplant. Am. J. Transplant. 2014, 14, 1446–1452. [Google Scholar] [CrossRef]
- Bharadia, D.; Sinha, I.; Pomahac, B. Role of Facial Vascularized Composite Allotransplantation in Burn Patients. Clin. Plast. Surg. 2017, 44, 857–864. [Google Scholar] [CrossRef]
- Rifkin, W.; David, J.A.; Plana, N.M.; Kantar, R.S.; Diaz-Siso, J.R.; Gelb, B.; Ceradini, D.J.; Rodriguez, E.D. Achievements and Challenges in Facial Transplantation. Ann. Surg. 2018, 268, 260–270. [Google Scholar] [CrossRef]
- Sosin, M.; Rodriguez, E.D. The face transplantation update: 2016. Plast. Reconstr. Surg. 2016, 137, 1841–1850. [Google Scholar] [CrossRef]
- Lindford, A.J.; Mäkisalo, H.; Jalanko, H.; Lauronen, J.; Anttila, V.-J.; Juteau, S.; Ämmälä, A.-J.; Eskola, A.; Saarni, S.; Isoniemi, H.; et al. The Helsinki approach to face transplantation. J. Plast. Reconstr. Aesthetic Surg. 2018, 72, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Ramly, E.P.; Kantar, R.S.; Diaz-Siso, J.R.; Alfonso, A.R.; Rodriguez, E.D. Computerized approach to facial transplantation: Evolution and application in 3 consecutive face transplants. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2379. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Siso, J.R.; Plana, N.M.; Schleich, B.; Irving, H.; Gelb, B.E.; Rodriguez, E.D. Novel donor transfer algorithm for multi- organ and facial allograft procurement. Am. J. Transplant. 2017, 17, 2496–2497. [Google Scholar] [CrossRef] [PubMed]
- Rifkin, W.J.; Manjunath, A.; Kimberly, L.L.; Plana, N.M.; Kantar, R.S.; Bernstein, G.L.; Diaz-Siso, J.R.; Rodriguez, E.D. Long-distance care of face transplant recipients in the United States. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Lantieri, L.; Grimbert, P.; Ortonne, N.; Suberbielle, C.; Bories, D.; Gil-Vernet, S.; Lemogne, C.; Bellivier, F.; Lefaucheur, J.P.; Schaffer, N.; et al. Face transplant: Long-term follow-up and results of a prospective open study. Lancet 2016, 388, 1398–1407. [Google Scholar] [CrossRef]
- Ramly, E.P.; Kantar, R.S.; Diaz-Siso, J.R.; Alfonso, A.R.; Shetye, P.R.; Rodriguez, E.D. Outcomes after tooth-bearing maxilloman- dibular facial transplantation: Insights and lessons learned. J. Oral. Maxillofac. Surg. 2019, 77, 2085–2103. [Google Scholar] [CrossRef]
- Khalifian, S.; Brazio, P.S.; Mohan, R.; Shaffer, C.; Brandacher, G.; Barth, R.N.; Rodriguez, E.D. Facial transplantation: The first 9 years. Lancet 2014, 384, 2153–2163. [Google Scholar] [CrossRef]
- Lantieri, L.; Cholley, B.; Lemogne, C.; Guillemain, R.; Ortonne, N.; Grimbert, P.; Thervet, E.; Lellouch, A.G. First human facial retransplantation: 30-month follow-up. Lancet 2020, 396, 1758–1765. [Google Scholar] [CrossRef]
- Kauke, M.; Panayi, A.C.; Safi, A.F.; Haug, V.; Perry, B.; Kollar, B.; Nizzi, M.C.; Broyles, J.; Annino, D.J.; Marty, F.M. Full facial retransplantation in a female patient-Technical, immunologic, and clinical considerations. Am. J. Transplant. 2021, 21, 3472–3480. [Google Scholar] [CrossRef]
- Fischer, S.; Kueckelhaus, M.; Pauzenberger, R.; Bueno, E.M.; Pomahac, B. Functional outcomes of face transplantation. Am. J. Transpl. 2015, 15, 220–233. [Google Scholar] [CrossRef]
- Petruzzo, P.; Testelin, S.; Kanitakis, J.; Badet, L.; Lengelé, B.; Girbon, J.P.; Parmentier, H.; Malcus, C.; Morelon, E.; Devauchelle, B.; et al. First human face transplantation: 5 years out-comes. Transplantation 2012, 93, 236–240. [Google Scholar] [CrossRef]
- Cavadas, P.C.; Ibáñez, J.; Thione, A. Surgical Aspects of a Lower Face, Mandible, and Tongue Allotransplantation. J. Reconstr. Microsurg. 2011, 28, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Cia, T.; Sicilia-Castro, D.; Infante-Cossio, P.; Barrera-Pulido, F.; Gacto-Sanchez, P.; Lagares-Borrego, A.; Narros-Gimenez, R.; Garcia-Perla, A.; Hernandez-Guisado, J.-M.; González-Padilla, J.-D. Second Human Facial Allotransplantation to Restore a Severe Defect following Radical Resection of Bilateral Massive Plexiform Neurofibromas. Plast. Reconstr. Surg. 2011, 127, 995–996. [Google Scholar] [CrossRef] [PubMed]
- Lantieri, L.; Meningaud, J.P.; Grimbert, P.; Bellivier, F.; Lefaucheur, J.P.; Ortonne, N.; Benjoar, M.D.; Lang, P.; Wolkenstein, P. Repair of the lower and middle parts of the face by composite tissue allotransplantation in a patient with massive plexiform neurofibroma: A 1-year follow-up study. Lancet 2008, 372, 639–645. [Google Scholar] [CrossRef]
- Meningaud, J.P.; Pirnay, P. La Greffe de Visage; Breal: Paris, France, 2011; pp. 1–167. [Google Scholar]
- Brazio, P.S.; Barth, R.N.; Bojovic, B.; Dorafshar, A.H.; Garcia, J.P.; Brown, E.N.; Bartlett, S.T.; Rodriguez, E.D. Algorithm for Total Face and Multiorgan Procurement From a Brain-Dead Donor. Am. J. Transplant. 2013, 13, 2743–2749. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, N.; Allen, K.; Miller, B.; Nolan, T.; Sheerin, K. Perioperative nursing management of donor and recipient patients undergoing face transplantation. AORN J. 2017, 106, 8–19. [Google Scholar] [CrossRef]
- Sosin, M.; Ceradini, D.J.; Hazen, A.; Levine, J.P.; Staffenberg, D.A.; Saadeh, P.B.; Flores, R.L.; Brecht, L.E.; Bernstein, G.L.; Rodriguez, E.D. Total face, eyelids, ears, scalp, and skeletal subunit transplant cadaver simulation: The culmination of aesthetic, craniofacial, and microsurgery principles. Plast. Reconstr. Surg. 2016, 137, 1569–1581. [Google Scholar] [CrossRef]
- Brown, E.N.; Dorafshar, A.H.; Bojovic, B.; Christy, M.R.; Borsuk, D.E.; Kelley, T.N.; Shaffer, C.K.; Rodriguez, E.D. Total face, double jaw, and tongue transplant simulation: A cadaveric study using computer-assisted techniques. Plast. Reconstr. Surg. 2012, 130, 815–823. [Google Scholar] [CrossRef]
- Meningaud, J.P.; Benjoar, M.D.; Hivelin, M.; Hermeziu, O.; Toure, G.; Lantieri, L. Procurement of total human face graft for allotransplantation: A preclinical study and the first clinical case. Plast. Reconstr. Surg. 2010, 126, 1181–1190. [Google Scholar] [CrossRef]
- Dorafshar, A.H.; Bojovic, B.; Christy, M.R.; Borsuk, D.E.; Iliff, N.T.; Brown, E.N.; Shaffer, C.K.; Kelley, T.N.; Kukuruga, D.L.; Barth, R.N.; et al. Total face, double jaw, and tongue transplantation: An evolutionary concept. Plast. Reconstr. Surg. 2013, 131, 241–251. [Google Scholar] [CrossRef]
- Sosin, M.; Robinson, I.S.; Diep, G.K.; Alfonso, A.R.; Maliha, S.G.; Ceradini, D.J.; Levine, J.P.; Staffenberg, D.A.; Saadeh, P.B.; Rodriguez, E.D. Feasibility and perception of cross-sex face transplantation to expand the donor pool. Plast. Reconstr. Surg. Glob. Open 2020, 8, e3100. [Google Scholar] [CrossRef]
- Mohan, R.; Borsuk, D.E.; Dorafshar, A.H.; Wang, H.D.; Bojovic, B.; Christy, M.R.; Rodriguez, E.D. Aesthetic and functional facial transplantation: A classification system and treatment algorithm. Plast. Reconstr. Surg. 2014, 133, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Pomahac, B.; Pribaz, J.J.; Bueno, E.M.; Sisk, G.C.; Diaz-Siso, J.R.; Chandawarkar, A.; Westvik, T.S.; Malin, E.W.; Eriksson, E. Novel Surgical Technique for Full Face Transplantation. Plast. Reconstr. Surg. 2012, 130, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.Q.; Wang, Y.; Hu, X.B.; Li, Y.S.; Li, J.S. Composite tissue allograft transplantation of cepha-locervical skin flap and two ears. Plast. Reconstr. Surg. 2005, 115, 31e–35e. [Google Scholar] [CrossRef]
- Burra, P.; Rodriguez-Castro, K.I. Neoplastic disease after liver transplantation: Focus on de novo neoplasms. World J. Gastroenterol. 2015, 21, 8753–8768. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Siso, J.R.; Sosin, M.; Plana, N.M.; Eduardo, D.; Rodriguez, E.D. Face transplantation: Complications, implications, and an update for the oncologic surgeon. J. Surg. Oncol. 2016, 113, 971–975. [Google Scholar] [CrossRef] [PubMed]
- di Pompeo, F.S.; Longo, B.; Giovanoli, P.; Plock, J.A.; Campanale, A.; Laporta, R.; Sorotos, M.; Paolini, G.; Renzi, L.; Nuccitelli, G.; et al. Facial Transplantation: Nonimmune-Related Hyperacute Graft Failure-The Role of Perfusion Injury: A Case Report. Ann. Plast. Surg. 2021, 86, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Siemionow, M. New minimal immunosuppression strategies for composite tissue allograft transplantation: The cleveland clinic experience. J. Am. Acad. Orthop. Surg. 2011, 19 (Suppl. 1), S38–S39. [Google Scholar] [CrossRef] [PubMed]
- Hequet, O.; Bourgeot, J.-P.; Michallet, M.; Morelon, E.; Dubernard, J.-M.; Dubois, V.; Devauchelle, B. Allogeneic donor bone marrow cells recovery and infusion after allogeneic face transplantation from the same donor. Bone Marrow Transplant. 2008, 41, 1059–1061. [Google Scholar] [CrossRef]
- Cendales, L.C.; Kanitakis, J.; Schneeberger, S.; Burns, C.; Ruiz, P.; Landin, L.; Remmelink, M.; Hewitt, C.W.; Landgren, T.; Lyons, B.; et al. The Banff 2007 Working Classification of Skin-Containing Composite Tissue Allograft Pathology. Am. J. Transplant. 2008, 8, 1396–1400. [Google Scholar] [CrossRef]
- Duhamel, P.; Suberbielle, C.; Grimbert, P.; Leclerc, T.; Jacquelinet, C.; Audry, B.; Bargues, L.; Charron, D.; Bey, E.; Lantieri, L.; et al. Anti-HLA sensitization in extensively burned patients: Extent, associated factors, and reduction in potential access to vascularized composite allotransplantation. Transpl. Int. 2015, 28, 582–593. [Google Scholar] [CrossRef]
- Benghiac, A.G.; Garrett, J.R.; Carter, B.S. Ethical issues in pediatric face transplantation. Pediatr. Transplant. 2017, 21, e13032. [Google Scholar] [CrossRef] [PubMed]
- Morelon, E.; Petruzzo, P.; Kanitakis, J.; Dakpé, S.; Thaunat, O.; Dubois, V.; Choukroun, G.; Testelin, S.; Dubernard, J.M.; Badet, L.; et al. Face transplantation: Partial graft loss of the first case ten years later. Am. J. Transplant. 2017, 17, 1935–1940. [Google Scholar] [CrossRef] [PubMed]
- Hersant, B.; SidAhmed-Mezi, M.; Aboud, C.; Niddam, J.; Levy, S.; Mernier, T.; La Padula, S.; Meningaud, J.P. Synergistic Effects of Autologous Platelet-Rich Plasma and Hyaluronic Acid Injections on Facial Skin Rejuvenation. Aesthet. Surg. J. 2021, 41, NP854–NP865. [Google Scholar] [CrossRef] [PubMed]
- La Padula, S.; Hersant, B.; Pizza, C.; Chesné, C.; Jamin, A.; Ben Mosbah, I.; Errico, C.; D’Andrea, F.; Rega, U.; Persichetti, P.; et al. Striae Distensae: In Vitro Study and Assessment of Combined Treatment With Sodium Ascorbate and Platelet-Rich Plasma on Fibroblasts. Aesthetic. Plast. Surg. 2021, 45, 1282–1293. [Google Scholar] [CrossRef]
- La Padula, S.; Hersant, B.; Noel, W.; Niddam, J.; Hermeziu, O.; Bouhassira, J.; Bosc, R.; Meningaud, J.P. Use of the retrograde limb of the internal mammary vein to avoid venous congestion in DIEP flap breast reconstruction: Further evidences of a reliable and timesparing procedure. Microsurgery 2016, 36, 447–452. [Google Scholar] [CrossRef]
- La Padula, S.; Hersant, B.; Meningaud, J.P. Intraoperative use of indocyanine green angiography for selecting the more reliable perforator of the anterolateral thigh flap: A comparison study. Microsurgery 2018, 38, 738–744. [Google Scholar] [CrossRef]
- Ruiz, R.; Hersant, B.; La Padula, S.; Meningaud, J.P. Facelifts: Improving the long-term outcomes of lower face and neck rejuvenation surgery: The lower face and neck rejuvenation combined method. J. Craniomaxillofac. Surg. 2018, 46, 697–704. [Google Scholar] [CrossRef]
- La Padula, S.; Hersant, B.; Chatel, H.; Aguilar, P.; Bosc, R.; Roccaro, G.; Ruiz, R.; Meningaud, J.P. One-step facial feminization surgery: The importance of a custom-made preoperative planning and patient satisfaction assessment. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 1694–1699. [Google Scholar] [CrossRef]
- Uygun, B.E.; Soto-Gutierrez, A.; Yagi, H.; Izamis, M.L.; Guzzardi, M.A.; Shulman, C.; Milwid, J.; Kobayashi, N.; Tilles, A.; Berthiaume, F.; et al. Organ reengineering through development of a transplantable recellularized liver graft using decellularized liver matrix. Nat. Med. 2010, 16, 814–820. [Google Scholar] [CrossRef]
- Jank, B.J.; Xiong, L.; Moser, P.T.; Guyette, J.P.; Ren, X.; Cetrulo, C.L.; Leonard, D.A.; Fernandez, L.; Fagan, S.P.; Ott, H.C. Engineered composite tissue as a bioartificial limb graft. Biomaterials 2015, 61, 246–256. [Google Scholar] [CrossRef] [Green Version]
- Orlando, G.; Soker, S.; Stratta, R.J.; Atala, A. Will regenerative medicine replace transplantation? Cold Spring Harb. Perspect. Med. 2013, 3, a015693. [Google Scholar] [CrossRef] [PubMed]
- Duisit, J.; Maistriaux, L.; Taddeo, A.; Orlando, G.; Joris, V.; Coche, E.; Behets, C.; Lerut, J.; Dessy, C.; Cossu, G.; et al. Bioengineering a Human Face Graft: The Matrix of Identity. Ann Surg. 2017, 266, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Kauke-Navarro, M.; Safi, A.-F.; Zhegibe, A.; Haug, V.; Kollar, B.; Nelms, L.; Palmer, W.J.; Tchiloemba, B.; Lian, C.G.; Murphy, G.F.; et al. Mucosa and Rejection in Facial Vascularized Composite Allotransplantation: A Systematic Review. Transplantation 2020, 104, 2616–2624. [Google Scholar] [CrossRef]
- Kaufman, C.L.; Kanitakis, J.; Weissenbacher, A.; Brandacher, G.; Mehra, M.R.; Amer, H.; Zelger, B.G.; Zelger, B.; Pomahac, B.; McDiarmid, S.; et al. Defining chronic rejection in vascularized composite allotransplantation—The American Society of Reconstructive Transplantation and International Society of Vascularized Composite Allotransplantation chronic rejection working group: 2018 American Society of Reconstructive Transplantation meeting report and white paper Research goals in defining chronic rejection in vascularized composite allotransplantation. SAGE Open Med. 2020, 8, 2050312120940421. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors | Title | Journal | Year of Publication |
|---|---|---|---|
| Kantar RS et al. [2] | Facial Transplantation: Principles and Evolving Concepts | Plast. Reconstr. Surg. | 2021 |
| Diep GK et al. [3] | The 2020 Facial Transplantation Update: A 15-Year Compendium | Plast. Reconstr. Surg. Glob. Open | 2021 |
| Kantar RS et al. [4] | Incidence of preventable nonfatal craniofacial injuries and implications for facial transplantation | J. Craniofac. Surg. | 2019 |
| Chandraker A et al. [6] | The management of antibody-mediated rejection in the first presensitized recipient of a full-face allotransplant | Am. J. Transplant. | 2014 |
| Bharadia D et al. [7] | Role of facial vascularized composite allotransplantation in burn patients | Clin. Plast. Surg. | 2017 |
| Rifkin WJ et al. [8] | Achievements and challenges in facial transplantation | Ann. Surg. | 2018 |
| Sosin M, Rodriguez ED. [9] | The face transplantation update: 2016 | Plast. Reconstr. Surg. | 2016 |
| Lindford AJ et al. [10] | The Helsinki approach to face transplantation | J. Plast. Reconstr. Aesthet. Surg. | 2019 |
| Ramly EP et al. [11] | Computerized approach to facial transplantation: Evolution and application in 3 consecutive face transplants | Plast. Reconstr. Surg. Glob. Open | 2019 |
| Diaz-Siso JR et al. [12] | Novel donor transfer algorithm for multi-organ and facial allograft procurement | Am. J. Transplant. | 2017 |
| Rifkin WJ [13] | Long-distance care of face transplant recipients in the United States | J. Plast. Reconstr. Aesthet. Surg. | 2018 |
| Lantieri L et al. [14] | Face transplant: Long-term follow-up and results of a prospective open study | Lancet | 2016 |
| Ramly EP et al. [15] | Outcomes after tooth-bearing maxilloman-dibular facial transplantation: Insights and lessons learned | J. Oral. Maxillofac. Surg. | 2019 |
| Khalifian S et al. [16] | Facial transplantation: The first 9 years | Lancet | 2014 |
| Lantieri L et al. [17] | First human facial retransplantation: 30-month follow-up | Lancet | 2020 |
| Kauke M et al. [18] | Full facial retransplantation in a female patient-Technical, immunologic, and clinical considerations | Am. J. Transplant. | 2021 |
| Fischer S et al. [19] | Functional outcomes of face transplantation | Am. J. Transpl. | 2015 |
| Petruzzo P et al. [20] | First human face transplantation: 5 years outcomes | Transplantation | 2012 |
| Morelon E et al. [43] | Face transplantation: partial graft loss of the first case ten years later | Am. J. Transplant. | 2017 |
| Patient | Team | Location and Date of FT | Patient (Age, Gender) | Indication | Allograft Type | Cause of Death, Time from Transplantation | AR | CR |
|---|---|---|---|---|---|---|---|---|
| 1 | Devauchelle, Dubernard | Amiens, France, 2005 | 38, woman | Animal attack | Partial | Malignancy, 8 years | Yes | Yes |
| 2 | Guo | Xi’an, China, 2006 | 30, woman | Animal attack | Partial | Non-compliance, 27 months | Yes | No |
| 3 | Siemionow | Cleveland, Ohio, 2008 | 45, woman | Ballistic trauma | Partial | Infection, 11 years and 7 months | Yes | No |
| 4 | Lantieri, Meningaud | Créteil, France, 2009 | 37, man | Third-degree burn | Partial + Hands | Sepsis (multidrug-resistant Pseudomonas), 2 months | No | No |
| 5 | Pomahac | Boston, Massachusetts, 2009 | 59, man | Electrical burn | Partial | Hepatocellular carcinoma, 10 years | Yes | Yes |
| 6 | Cavadas | Valencia, Spain, 2009 | 42, man | Osteoradionecrosis after malignancy | Partial | Malignancy (unknown) | Yes | No |
| 7 | Lantieri, Meningaud | Créteil, France, 2011 | 41, man | Ballistic Trauma | Partial | Suicide, 36 months | Yes | No |
| 8 | Ozkan | Ankara, Turkey, 2013 | 54, man | Ballistic Trauma | Full | Multiorgan deficiency resulting from progressive infectious (pulmonary and cerebellar aspergillosis) and metabolic complications, 11 months | Yes | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Padula, S.; Pensato, R.; Pizza, C.; Coiante, E.; Roccaro, G.; Longo, B.; D’Andrea, F.; Wirz, F.S.; Hersant, B.; Meningaud, J.P. Face Transplant: Indications, Outcomes, and Ethical Issues—Where Do We Stand? J. Clin. Med. 2022, 11, 5750. https://doi.org/10.3390/jcm11195750
La Padula S, Pensato R, Pizza C, Coiante E, Roccaro G, Longo B, D’Andrea F, Wirz FS, Hersant B, Meningaud JP. Face Transplant: Indications, Outcomes, and Ethical Issues—Where Do We Stand? Journal of Clinical Medicine. 2022; 11(19):5750. https://doi.org/10.3390/jcm11195750
Chicago/Turabian StyleLa Padula, Simone, Rosita Pensato, Chiara Pizza, Edoardo Coiante, Giovanni Roccaro, Benedetto Longo, Francesco D’Andrea, Francesco Saverio Wirz, Barbara Hersant, and Jean Paul Meningaud. 2022. "Face Transplant: Indications, Outcomes, and Ethical Issues—Where Do We Stand?" Journal of Clinical Medicine 11, no. 19: 5750. https://doi.org/10.3390/jcm11195750