
Transesophageal Endoscopic Ultrasound Fine Needle Biopsy for the Diagnosis of Mediastinal Masses: A Retrospective Real-World Analysis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
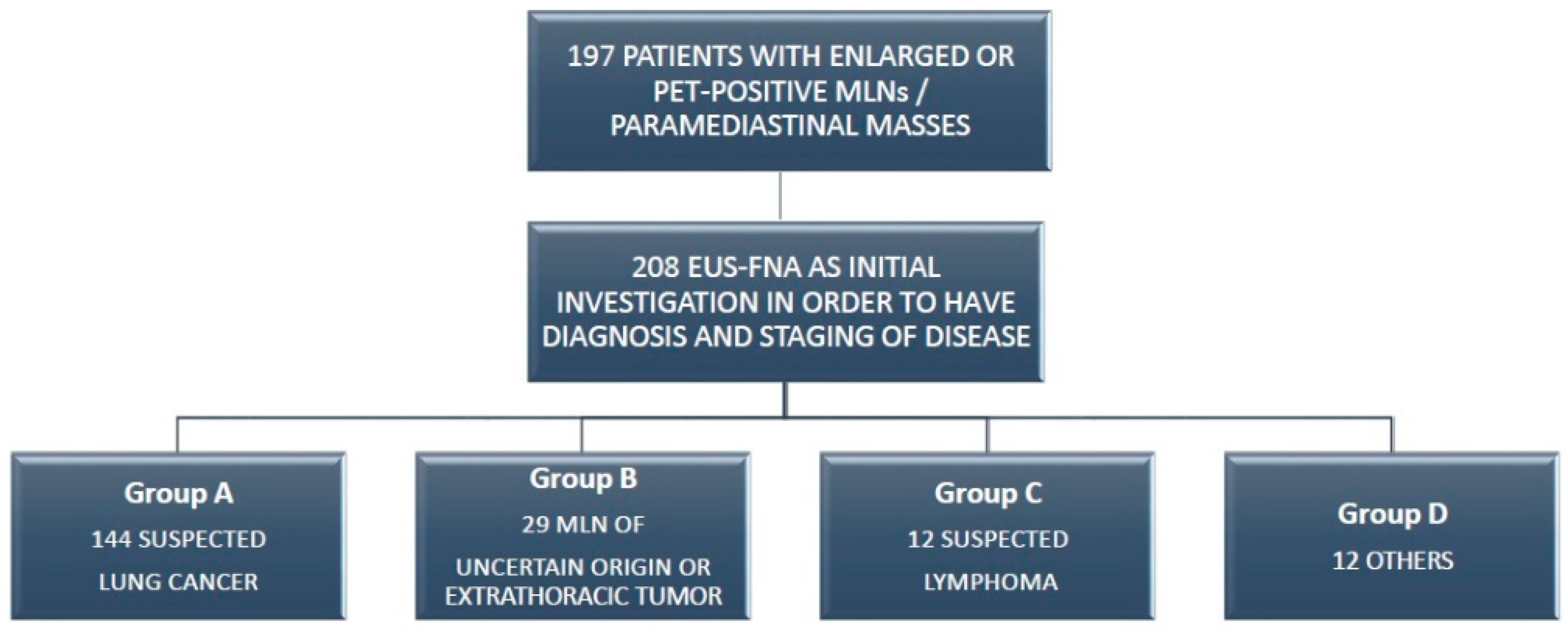
2.1. Study Design
2.2. Pre-Workup Evaluation
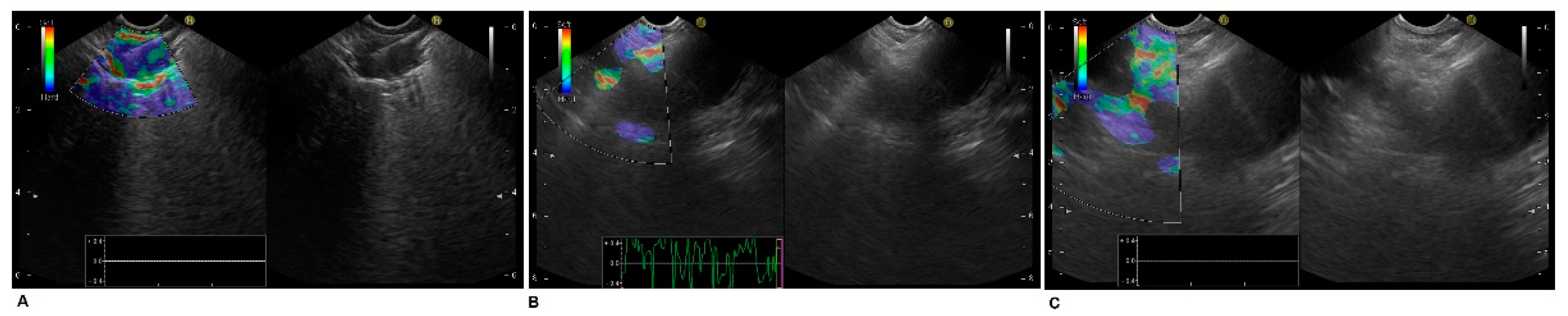
2.3. Endoscopic Ultrasound Technique
2.4. Cytology and Histology Preparation Method
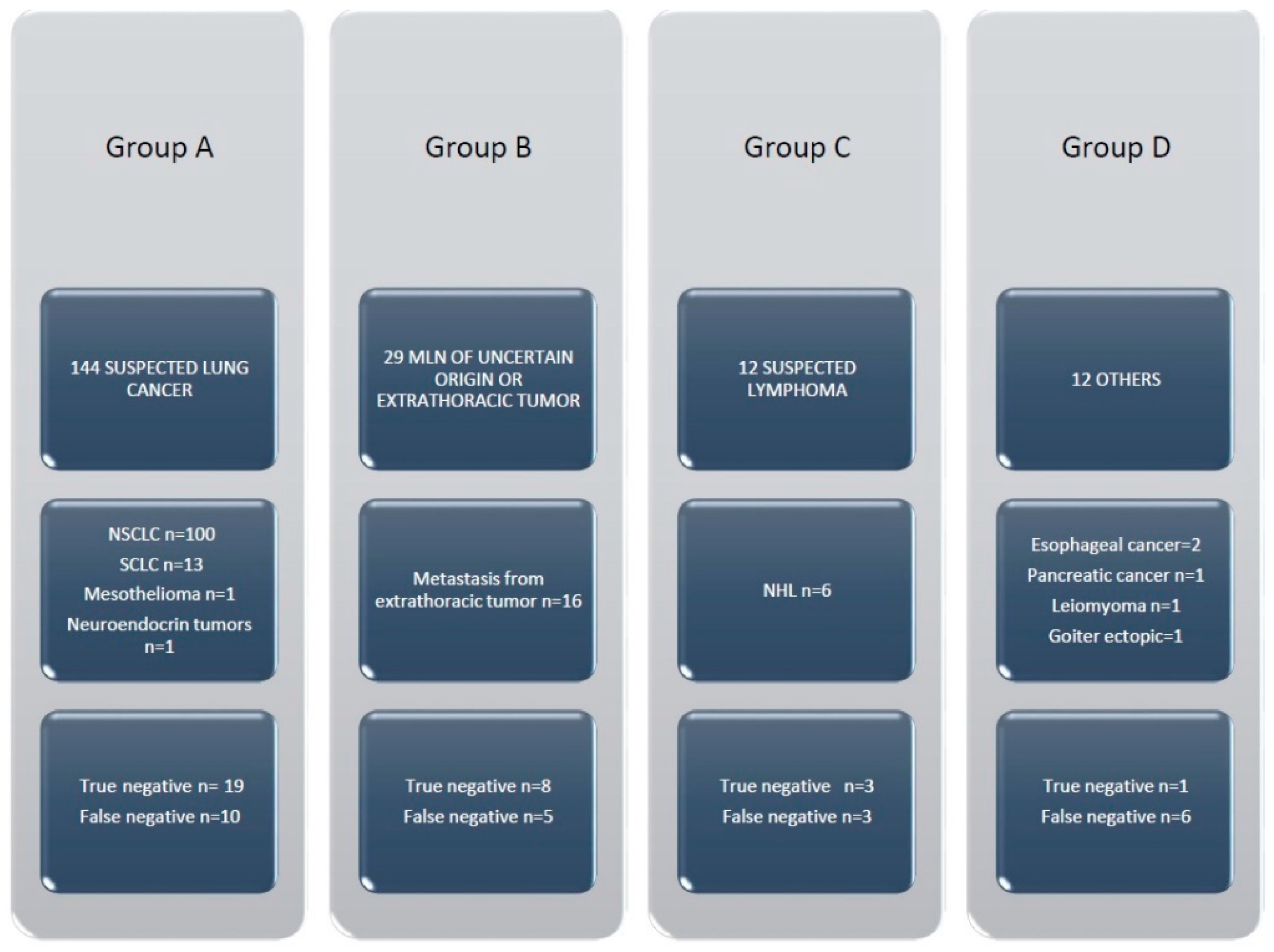
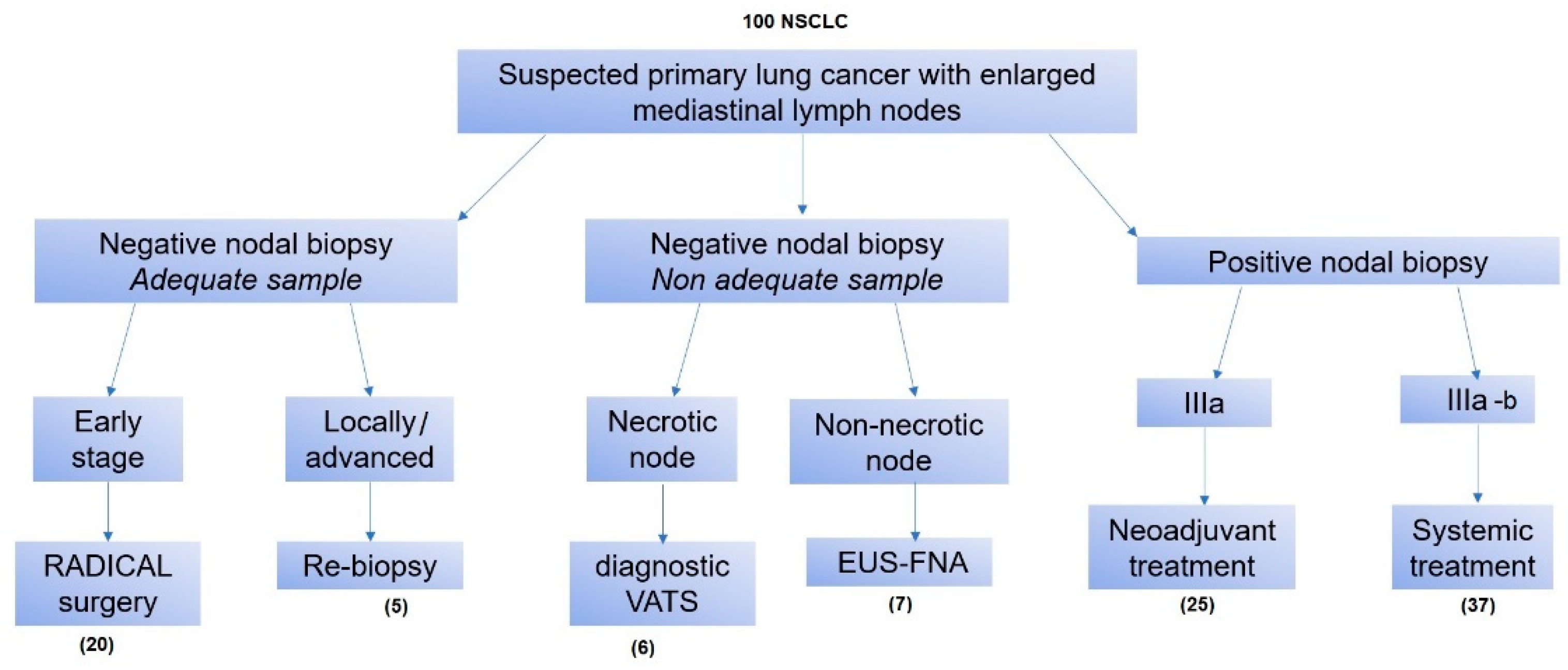
3. Results
Diagnostic Features
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dhooria, S.; Mehta, R.M.; Madan, K. A Multicenter Study on the Utility of EBUS-TBNA and EUS-B-FNA in the Diagnosis of Mediastinal Lymphoma. J. Bronchol. Interv. Pulmonol. 2019, 26, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Colella, S.; Scarlata, S.; Bonifazi, M.; Ravaglia, C.; Naur, T.M.H.; Pela, R.; Clementsen, P.F.; Gasparini, S.; Poletti, V. Biopsy needles for mediastinal lymph node sampling by endosonography: Current knowledge and future perspectives. J. Thorac. Dis. 2018, 10, 6960–6968. [Google Scholar] [CrossRef]
- Sakairi, Y.; Nakajima, T.; Yoshino, I. Role of endobronchial ultrasound-guided transbronchial needle aspiration in lung cancer management. Expert Rev. Respir. Med. 2019, 13, 863–870. [Google Scholar] [CrossRef]
- Youlden, D.R.; Cramb, S.M.; Baade, P.D. The International Epidemiology of Lung Cancer Geographical Distribution and Secular Trends. J. Thorac. Oncol. 2008, 3, 819–831. [Google Scholar] [CrossRef]
- Nanavaty, P.; Alvarez, M.S.; Alberts, W.M. Lung cancer screening: Advantages, controversies, and applications. Cancer Control 2014, 21, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Gridelli, C.; Rossi, A.; Carbone, D.P.; Guarize, J.; Karachaliou, N.; Mok, T.; Petrella, F.; Spaggiari, L.; Rosell, R. Non-small-cell lung cancer. Nat. Rev. Dis. Primers 2015, 1, 15009. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, M.M.; Silverstein, S.C.; Quinn, M.; Waterston, L.B.; Thomas, C.A.; Benneyan, J.C.; Han, P.K.J. Timeliness of access to lung cancer diagnosis and treatment: A scoping literature review. Lung Cancer 2017, 112, 156–164. [Google Scholar] [CrossRef]
- Lee, J.W.; Kim, E.Y.; Kim, D.J.; Lee, J.H.; Kang, W.J.; Lee, J.D.; Yun, M. The diagnostic ability of 18F-FDG PET/CT for mediastinal lymph node staging using 18F-FDG uptake and volumetric CT histogram analysis in non-small cell lung cancer. Eur. Radiol. 2016, 26, 4515–4523. [Google Scholar] [CrossRef]
- Schmidt-Hansen, M.; Baldwin, D.R.; Hasler, E.; Zamora, J.; Abraira, V.; Roqué I Figuls, M. PET-CT for assessing mediastinal lymph node involvement in patients with suspected resectable non-small cell lung cancer. Cochrane Database Syst. Rev. 2014, 11, CD009519. [Google Scholar] [CrossRef]
- Yin, Z.; Liang, Z.; Li, P.; Wang, Q. CT-guided core needle biopsy of mediastinal nodes through a transpulmonary approach: Retrospective analysis of the procedures conducted over six years. Eur. Radiol. 2017, 27, 3401–3407. [Google Scholar] [CrossRef]
- Groheux, D.; Quere, G.; Blanc, E.; Lemarignier, C.; Vercellino, L.; de Margerie-Mellon, C.; Merlet, P.; Querellou, S. FDG PET-CT for solitary pulmonary nodule and lung cancer: Literature review. Diagn Interv. Imaging 2016, 97, 1003–1017. [Google Scholar] [CrossRef] [PubMed]
- Vegar Zubović, S.; Kristić, S.; Hadžihasanović, B. Positron emission tomography/computed tomography (PET/CT) and CT for N staging of non-small cell lung cancer. Med Glas 2017, 14, 199–203. [Google Scholar]
- Gao, S.J.; Kim, A.W.; Puchalski, J.T.; Bramley, K.; Detterbeck, F.C.; Boffa, D.J.; Decker, R.H. Indications for invasive mediastinal staging in patients with early non-small cell lung cancer staged with PET-CT. Lung Cancer 2017, 109, 36–41. [Google Scholar] [CrossRef] [PubMed]
- De Leyn, P.; Dooms, C.; Kuzdzal, J.; Lardinois, D.; Passlick, B.; Rami-Porta, R.; Turna, A.; Van Schil, P.; Venuta, F.; Waller, D.; et al. Preoperative mediastinal lymph node staging for non-small cell lung cancer:2014 update of the 2007 ESTS guidelines. Transl. Lung Cancer Res. 2014, 3, 225–233. [Google Scholar] [PubMed]
- Rendina, E.A.; Venuta, F.; De Giacomo, T.; Ciccone, A.M.; Moretti, M.S.; Ibrahim, M.; Coloni, G.F. Biopsy of anterior mediastinal masses under local anesthesia. Ann. Thorac. Surg. 2002, 74, 1720–1722. [Google Scholar] [CrossRef]
- Witte, B.; Neumeister, W.; Huertgen, M. Does endoesophageal ultrasound-guided fine-needle aspiration replace mediastinoscopy in mediastinal staging of thoracic malignancies? Eur. J. Cardio-Thorac. Surg. 2008, 33, 1124–1128. [Google Scholar] [CrossRef]
- Trosini-Désert, V.; Jeny, F.; Maksud, P.; Giron, A.; Degos, V.; Similowski, T. Contribution of endobronchial ultrasound elastography to the characterization of mediastinal lymphadenopathy: A single-center, prospective, observational study. Respir. Med. Res. 2019, 76, 28–33. [Google Scholar] [CrossRef]
- Tournoy, K.G.; Praet, M.M.; Van Maele, G.; Van Meerbeeck, J.P. Esophageal endoscopic ultrasound with fine-needle aspiration with on-site pathologist:high accuracy for the diagnosis of mediastinal lymphadenopathy. Chest 2005, 128, 3004–3009. [Google Scholar] [CrossRef]
- Sanchez-Lorente, D.; Guzman, R.; Boada, M.; Guirao, A.; Carriel, N.; Molins, L. N2 disease in non-small-cell lung cancer: Straight to surgery? Future Oncol. 2018, 14, 13–16. [Google Scholar] [CrossRef]
- Boffa, D.; Fernandez, F.G.; Kim, S.; Kosinski, A.; Onaitis, M.W.; Cowper, P.; Jacobs, J.P.; Wright, C.D.; Putnam, J.B.; Furnary, A.P. Surgically Managed Clinical Stage IIIA-Clinical N2 Lung Cancer in The Society of Thoracic Surgeons Database. Ann. Thorac. Surg. 2017, 104, 395–403. [Google Scholar] [CrossRef]
- Annema, J.T.; Versteegh, M.I.; Veseliç, M.; Voigt, P.; Rabe, K.F. Endoscopic ultrasound-guided fine-needle aspiration in the diagnosis and staging of lung cancer and its impact on surgical staging. J. Clin. Oncol. 2005, 23, 8357–8361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toloza, E.M.; Harpole, L.; Detterbeck, F.; McCrory, D.C. Invasive staging of non-small cell lung cancer: A review of the current evidence. Chest 2003, 123 (Suppl. 1), 157–665. [Google Scholar] [CrossRef] [PubMed]
- Hujala, K.T.; Sipila, J.L.; Grenman, R. Mediastinoscopy: Its role and value today in the differential mediastinal pathology. Acta Oncol. 2001, 40, 79–82. [Google Scholar]
- Sehgal, I.S.; Dhooria, S.; Aggarwal, A.N.; Behera, D.; Agarwal, R. Endosonography Versus Mediastinoscopy in Mediastinal Staging of Lung Cancer: Systematic Review and Meta-Analysis. Ann. Thorac. Surg. 2016, 102, 1747–1755. [Google Scholar] [CrossRef] [PubMed]
- Sharples, L.D.; Jackson, C.; Wheaton, E.; Griffith, G.; Annema, J.T.; Dooms, C.; Tournoy, K.G.; Deschepper, E.; Hughes, V.; Magee, L.; et al. Clinical effectiveness and cost-effectiveness of endobronchial and endoscopic ultrasound relative to surgical staging in potentially resectable lung cancer: Results from the ASTER randomized controlled trial. Health technol Assess. Health Technol. Assess. 2012, 16, 18. [Google Scholar] [CrossRef] [PubMed]
- Gallina, F.T.; Assisi, D.; Forcella, D.; Pierconti, F.; Visca, P.; Melis, E.; Facciolo, F. Five years of thoracic endoscopy unit activity on lung cancer staging: How teamwork can improve the outcomes. Mediastinum 2021, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S.S.; Vilmann, P.; Krasnik, M.; Dirksen, A.; Clementsen, P.; Maltbaek, N.; Lassen, U.; Skov, B.G.; Jacobsen, G.K. Endoscopic ultrasound guided biopsy performed routinely in lung cancer staging spares futile thoracotomies: Preliminary results from a randomized clinical trial. Lung Cancer 2005, 49, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Kramer, H.; Koëter, G.H.; Sleijfer, D.T.; van Putten, J.W.; Groen, H.J. Endoscopic ultrasound-guided fine-needle aspiration in patients with mediastinal abnormalities and previous extrathoracic malignancy. Eur. J. Cancer 2004, 40, 559–562. [Google Scholar] [CrossRef]
- Woodard, G.A.; Jones, K.D.; Jablons, D.M. Lung Cancer Staging and Prognosis. Cancer Treat Res. 2016, 170, 47–75. [Google Scholar]
- Gamliel, Z. Mediastinal Staging in Non-Small Cell Lung Cancer. Surg. Oncol. Clin. N. Am. 2016, 25, 493–502. [Google Scholar] [CrossRef]
- Abdel-Rahman, O. Validation of the AJCC 8th lung cancer staging system among patients with small cell lung cancer. Clin. Transl. Oncol. 2018, 20, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.M.; Vangel, M.G.; Wagner, H.; Schiller, J.H.; Herskovic, A.; Komaki, R.; Marks, R.S.; Perry, M.C.; Livingston, R.B.; Johnson, D.H. Prolonged survival in patients with resected non-small cell lung cancer and single-level N2 disease. J. Thorac. Cardiovasc.Surg. 2004, 128, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Tsubota, N.; Yoshimura, M.; Miyamoto, Y.; Matsuoka, H. Prognosis of completely resected pN2 non-small cell lung carcinomas: What is the significant node that affecys survival? J. Thorac. Cardiovasc. Surg. 1999, 118, 270–275. [Google Scholar] [CrossRef] [Green Version]
- Larsen, S.S.; Vilmann, P.; Krasnik, M.; Dirksen, A.; Clementsen, P.; Skov, B.G.; Jacobsen, G.K. Endoscopic ultrasound guided biopsy versus mediastinoscopy for analysis of paratracheal and subcarinal lymph nodes in lung cancer staging. Lung Cancer 2005, 48, 85–92. [Google Scholar] [CrossRef]
- Talebian, M.; von Bartheld, M.B.; Braun, J.; Versteegh, M.I.; Dekkers, O.M.; Rabe, K.F.; Annema, J.T. EUS –FNA in the preoperative staging of non-small cell lung cancer. Lung Cancer 2010, 69, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Zielinski, M.; Szlubowski, A.; Kołodziej, M.; Orzechowski, S.; Laczynska, E.; Pankowski, J.; Jakubiak, M.; Obrochta, A. Comparison of endobronchial ultrasound and/or endoesophageal ultrasound with transcervical extended mediastinal lymphadenectomy for staging and restaging of Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2013, 8, 630–636. [Google Scholar] [CrossRef]
- Cerfolio, R.J.; Bryant, A.S.; Eloubeidi, M.A. Accessing the aortopulmonary window (#5) and the paraaortic (#6) lymph nodes in patients with Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2007, 84, 940–945. [Google Scholar]
- Cerfolio, R.J.; Bryant, A.S.; Eloubeidi, M.A.; Frederick, P.A.; Minnich, D.J.; Harbour, K.C.; Dransfield, M.T. The true false negative rates of esophageal and endobronchial ultrasound in the staging of mediastinal lymph nodes in patients with Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2010, 90, 427–434. [Google Scholar] [CrossRef]
- Rusch, V.W.; Asamura, H.; Watanabe, H.; Giroux, D.J.; Rami-Porta, R.; Goldstraw, P. The IASLC Lung Cancer Staging Project: A proposal for a new international lymph node map in the forthcoming seventh edition of the TNM classification for lung cancer. J. Thorac. Oncol. 2009, 4, 568–577. [Google Scholar] [CrossRef]
- Roth, K.; Eagan, T.; Hardie, J. Expert opinion of mediastinal lymph node positions from an intrabronchial view. BMC Pulm. Med. 2016, 16, 15. [Google Scholar] [CrossRef]
- Oliveira, R.L.; Liberman, M. Endosonographic Mediastinal Lymph Node Staging in Non-Small Cell Lung Cancer: How I Teach It. Ann. Thorac. Surg. 2017, 104, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.W.; Marom, E.M.; Detterbeck, F.C. Approaching the patient with an anterior mediastinal mass: A guide for clinicians. J. Thorac. Oncol. 2014, 9, S102–S109. [Google Scholar] [CrossRef] [PubMed]
- Tournoy, K.G.; Annema, J.T.; Krasnik, M.; Herth, F.J.; van Meerbeeck, J.P. Endoscopic and Endobronchial Ultrasonography According to the proposed lymph node map definition in the seventh edition of the tumor, node, metastasis classification for lung cancer. J. Thorac. Oncol. 2009, 4, 1576–1584. [Google Scholar] [CrossRef] [PubMed]
- Creemers, K.; van der Heiden, O.; Los, J.; van Esser, J.; Newhall, D.; Djamin, R.S.; Aerts, J.G. Endoscopic Ultrasound Fine Needle Aspiration in the Diagnosis of Lymphoma. J. Oncol. 2011, 2011, 785425. [Google Scholar] [CrossRef]
- Yim, A.P. Video-assisted thoracoscopic management of anterior mediastinal masses. Preliminary experience and results. Surg. Endosc. 1995, 9, 1184–1188. [Google Scholar] [CrossRef]
- Agid, R.; Sklair-Levy, M.; Bloom, A.I.; Lieberman, S.; Polliack, A.; Ben-Yehuda, D.; Sherman, Y.; Libson, E. CT-guided biopsy with cutting-edge needle for the diagnosis of malignant lymphoma: Experience of 267 biopsies. Clin. Radiol. 2003, 58, 143–147. [Google Scholar] [CrossRef]
- Gupta, D.; Dadhwal, D.S.; Agarwal, R.; Gupta, N.; Bal, A.; Aggarwal, A.N. Endobronchial Ultrasound.Guided Transbronchia Needle Aspiration vs Conventional Transbronchial Needle Aspiration in The Diagnosis of Sarcoidosis. Chest 2014, 146, 547–556. [Google Scholar] [CrossRef]
- Prasse, A. The Diagnosis, Differential Diagnosis, and Treatment of Sarcoidosis. Dtsch. Arztebl. Int. 2016, 113, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Soto-Gomez, N.; Peters, J.I.; Nambiar, A.M. Diagnosis and Management of Sarcoidosis. Am. Fam. Physician 2016, 93, 840–848. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Group A | Group B | Group C | Group D |
|---|---|---|---|---|
| Age | 65 (37–82) | 67 (29–80) | 49 (24–65) | 54 (27–79) |
| Gender (M/F) | 96/48 | 17/12 | 8/4 | 7/5 |
| ECOG score | 3 (2–4) | 3 (2–4) | 2 (1–4) | 3 (2–5) |
| Median diameter of puncture target | 23 (12–45) | 19 (13–40) | 25 (17–55) | 22 (11–39) |
| Needle size (22/19) | 112/35 | 20/9 | 4/8 | 8/4 |
| Number of punctures | 4 (3–6) | 3 (2–6) | 4 (3–6) | 4 (3–6) |
| Perioperative complications | 1 | 0 | 0 | 0 |
| Site of the Biopsy | Number of Patients | Sensitivity | Negative Predictive Value | Diagnostic Accuracy |
|---|---|---|---|---|
| Overall MLNs | 154 | 81.1% | 52.1% | 84.4% |
| Stations 7 + 8 + 9 | 123 | 82.1% | 55% | 87.5% |
| Station 4L | 14 | 70% | 57.1% | 78.5% |
| Station 5 | 16 | 80% | 25% | 81.2% |
| Station 3P | 1 | 100% | 0 | 81.2% |
| Lung Mass | 32 | 96.4% | 80% | 96.8% |
| Lung Mass and MLN | 9 | 100% | NA | 100% |
| Others | 2 | 100% | NA | 100% |
| Pathology Group | Stations 7, 8 and 9 (Sensitivity, NPV, Accuracy) | Station 4L (Sensitivity, NPV, Accuracy) | Station 5 (Sensitivity, NPV, Accuracy) |
|---|---|---|---|
| Group A | 90.5%; 66%; 92% | 75%; 33%; 77% | 87.5%; NC; 87.5% |
| Group B | 80%; 62.5%; 83.3% | 50%; 66%; 75% | 75%; 50%; 80% |
| Group C | 57.1%; 40%; 66% | NA; 100%; 100% | 100%; NA; 100% |
| Group D | 0%; 16.6%; 16.6% | NA; NA; NA | 0%; 0%; 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assisi, D.; Gallina, F.T.; Forcella, D.; Tajè, R.; Melis, E.; Visca, P.; Pierconti, F.; Venti, E.; Facciolo, F. Transesophageal Endoscopic Ultrasound Fine Needle Biopsy for the Diagnosis of Mediastinal Masses: A Retrospective Real-World Analysis. J. Clin. Med. 2022, 11, 5469. https://doi.org/10.3390/jcm11185469
Assisi D, Gallina FT, Forcella D, Tajè R, Melis E, Visca P, Pierconti F, Venti E, Facciolo F. Transesophageal Endoscopic Ultrasound Fine Needle Biopsy for the Diagnosis of Mediastinal Masses: A Retrospective Real-World Analysis. Journal of Clinical Medicine. 2022; 11(18):5469. https://doi.org/10.3390/jcm11185469
Chicago/Turabian StyleAssisi, Daniela, Filippo Tommaso Gallina, Daniele Forcella, Riccardo Tajè, Enrico Melis, Paolo Visca, Federico Pierconti, Emanuela Venti, and Francesco Facciolo. 2022. "Transesophageal Endoscopic Ultrasound Fine Needle Biopsy for the Diagnosis of Mediastinal Masses: A Retrospective Real-World Analysis" Journal of Clinical Medicine 11, no. 18: 5469. https://doi.org/10.3390/jcm11185469