
Endobronchial Ultrasound-Guided Transbronchial Forceps Biopsy: A Retrospective Bicentric Study Using the Olympus 1.5 mm Mini-Forceps

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
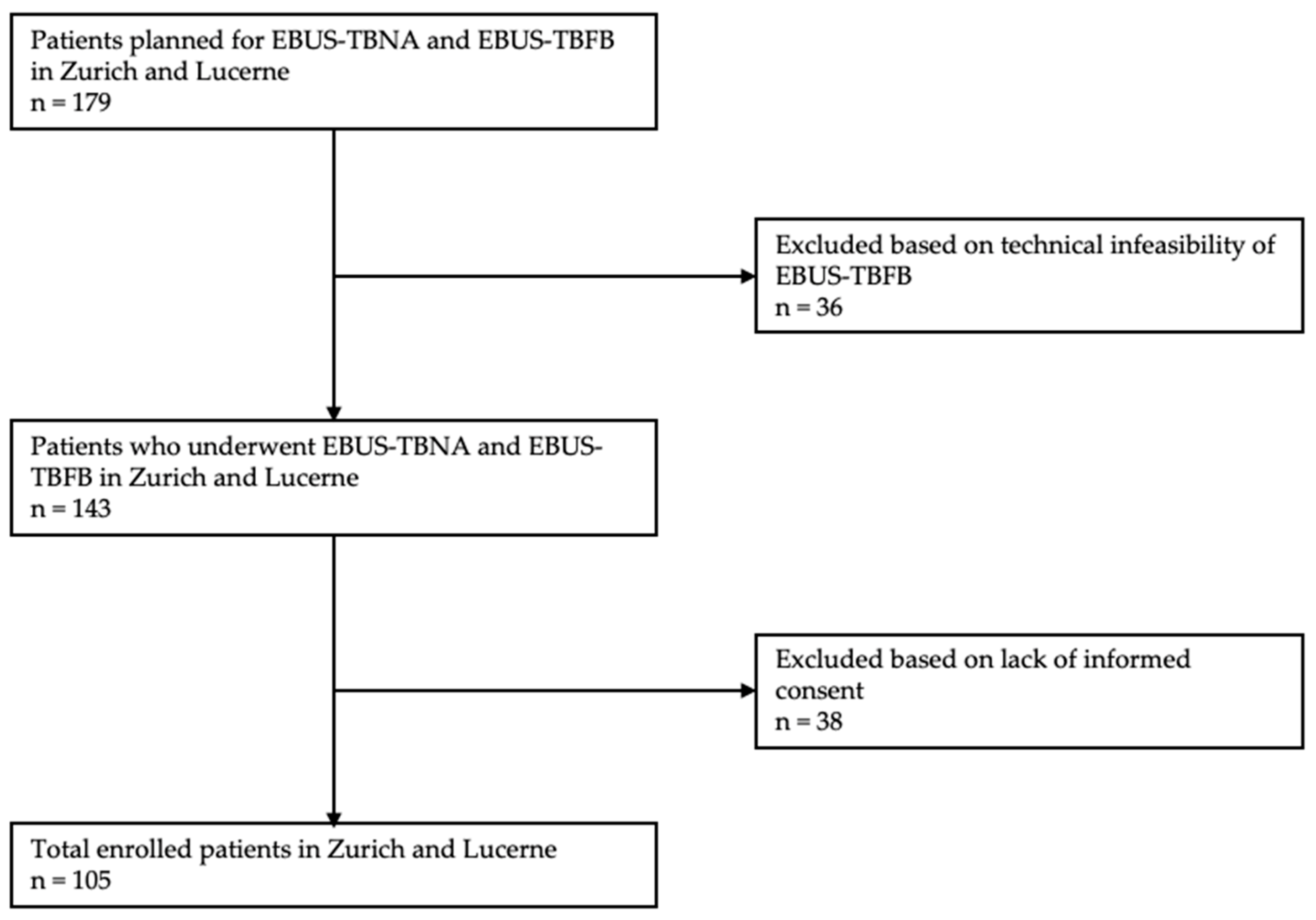
2.1. Patient Selection and Overall Study Design
2.2. Procedure and Sedation
2.3. Cytological and Histological Analyses
2.4. Safety
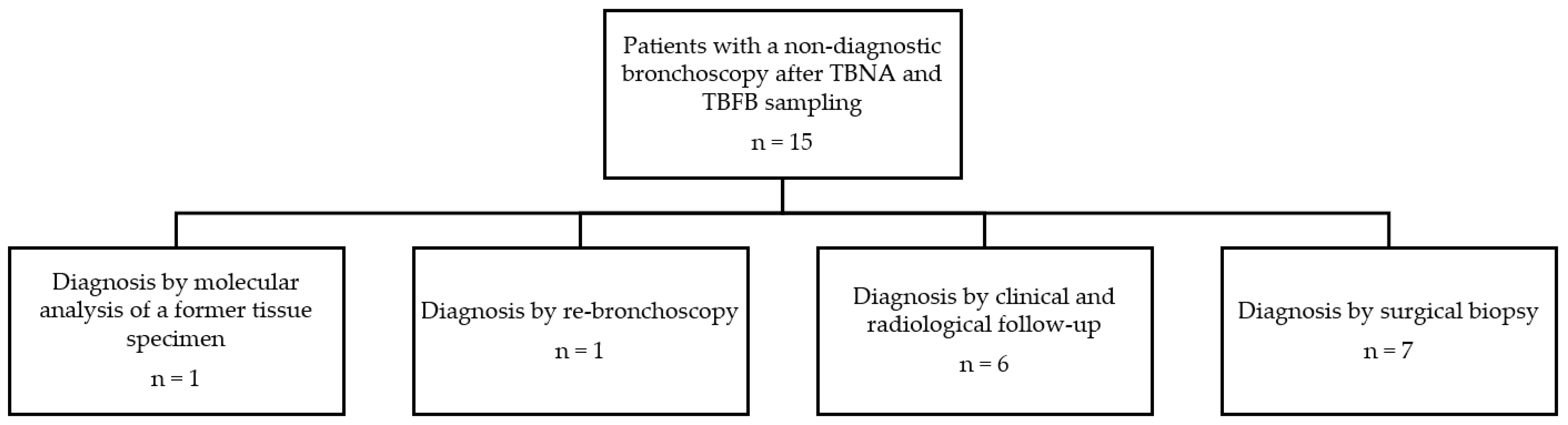
2.5. Reference Standard and Endpoints
2.6. Statistical Analysis
3. Results
3.1. Diagnostic Yield
3.2. Adverse Events
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Darwiche, K.; Freitag, L.; Nair, A.; Neumann, C.; Karpf-Wissel, R.; Welter, S.; Wohlschlaeger, J.; Theegarten, D. Evaluation of a novel endobronchial ultrasound-guided lymph node forceps in enlarged mediastinal lymph nodes. Respiration 2013, 86, 229–236. [Google Scholar] [CrossRef]
- Yasufuku, K.; Pierre, A.; Darling, G.; De Perrot, M.; Waddell, T.; Johnston, M.; Da Cunha Santos, G.; Geddie, W.; Boerner, S.; Le, L.W.; et al. A prospective controlled trial of endobronchial ultrasound-guided transbronchial needle aspiration compared with mediastinoscopy for mediastinal lymph node staging of lung cancer. J. Thorac. Cardiovasc. Surg. 2011, 142, 1393–1400.e1. [Google Scholar] [CrossRef] [PubMed]
- Rintoul, R.C.; Skwarski, K.M.; Murchison, J.T.; Wallace, W.A.; Walker, W.S.; Penman, I.D. Endobronchial and endoscopic ultrasound-guided real-time fine-needle aspiration for mediastinal staging. Eur. Respir. J. 2005, 25, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.; Shah, P.L.; Edmonds, L.; Lim, E. Test performance of endobronchial ultrasound and transbronchial needle aspiration biopsy for mediastinal staging in patients with lung cancer: Systematic review and meta-analysis. Thorax 2009, 64, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Gu, P.; Zhao, Y.Z.; Jiang, L.Y.; Zhang, W.; Xin, Y.; Han, B.H. Endobronchial ultrasound-guided transbronchial needle aspiration for staging of lung cancer: A systematic review and meta-analysis. Eur. J. Cancer 2009, 45, 1389–1396. [Google Scholar] [CrossRef]
- Chandra, S.; Nehra, M.; Agarwal, D.; Mohan, A. Diagnostic accuracy of endobronchial ultrasound-guided transbronchial needle biopsy in mediastinal lymphadenopathy: A systematic review and meta-analysis. Respir. Care 2012, 57, 384–391. [Google Scholar] [CrossRef]
- Alberts, W.M. Diagnosis and Management of Lung Cancer Executive Summary. Chest 2007, 132, 1S–19S. [Google Scholar] [CrossRef]
- De leyn, P.; Dooms, C.; Kuzdzal, J.; Lardinois, D.; Passlick, B.; Rami-Porta, R.; Turna, A.; Van Schil, P.; Venuta, F.; Waller, D.; et al. Revised ests guidelines for preoperative mediastinal lymph node staging for non-small-cell lung cancer. Eur. J. Cardio-Thorac. Surg. 2014, 45, 787–798. [Google Scholar] [CrossRef]
- Silvestri, G.A.; Gonzalez, A.V.; Jantz, M.A.; Margolis, M.L.; Gould, M.K.; Tanoue, L.T.; Harris, L.J.; Detterbeck, F.C. Methods for staging non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 2013, 143, e211S–e250S. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Srinivasan, A.; Aggarwal, A.N.; Gupta, D. Efficacy and safety of convex probe EBUS-TBNA in sarcoidosis: A systematic review and meta-analysis. Respir. Med. 2012, 106, 883–892. [Google Scholar] [CrossRef]
- Erer, O.F.; Erol, S.; Anar, C.; Aydoğdu, Z.; Aktoğu Özkan, S. Diagnostic yield of EBUS-TBNA for lymphoma and review of the literature. Endosc. Ultrasound 2017, 6, 317–322. [Google Scholar] [CrossRef]
- Cheng, G.; Mahajan, A.; Oh, S.; Benzaquen, S.; Chen, A. Endobronchial ultrasound-guided intranodal forceps biopsy (EBUS-IFB)—technical review. J. Thorac. Dis. 2019, 11, 4049–4058. [Google Scholar] [CrossRef]
- Labarca, G.; Sierra-Ruiz, M.; Kheir, F.; Folch, E.; Majid, A.; Mehta, H.J.; Jantz, M.A.; Fernandez-Bussy, S. Diagnostic accuracy of endobronchial ultrasound transbronchial needle aspiration in lymphoma a systematic review and meta-analysis. Ann. Am. Thorac. Soc. 2019, 16, 1432–1439. [Google Scholar] [CrossRef]
- Kennedy, M.P.; Jimenez, C.A.; Bruzzi, J.F.; Mhatre, A.D.; Lei, X.; Giles, F.J.; Fanning, T.; Morice, R.C.; Eapen, G.A. Endobronchial ultrasound-guided transbronchial needle aspiration in the diagnosis of lymphoma. Thorax 2008, 63, 360–365. [Google Scholar] [CrossRef]
- Moonim, M.T.; Breen, R.; Fields, P.A.; Santis, G. Diagnosis and subtyping of de novo and relapsed mediastinal lymphomas by endobronchial ultrasound needle aspiration. Am. J. Respir. Crit. Care Med. 2013, 188, 1216–1223. [Google Scholar] [CrossRef]
- Herth, F.J.F.; Morgan, R.K.; Eberhardt, R.; Ernst, A. Endobronchial Ultrasound-Guided Miniforceps Biopsy in the Biopsy of Subcarinal Masses in Patients with Low Likelihood of Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2008, 85, 1874–1878. [Google Scholar] [CrossRef]
- Ray, A.S.; Li, C.; Murphy, T.E.; Cai, G.; Araujo, K.L.B.; Bramley, K.; DeBiasi, E.M.; Pisani, M.A.; Cortopassi, I.O.; Puchalski, J.T. Improved Diagnostic Yield and Specimen Quality With Endobronchial Ultrasound-Guided Forceps Biopsies: A Retrospective Analysis. Ann. Thorac. Surg. 2020, 109, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Ghori, U.; Chaddha, U.; Murgu, S. Combined EBUS-IFB and EBUS-TBNA vs EBUS-TBNA alone for intrathoracic adenopathy: A Meta-analysis. Ann. Thorac. Surg. 2021, 114, 340–348. [Google Scholar] [CrossRef]
- Herth, F.J.F.; Schuler, H.; Gompelmann, D.; Kahn, N.; Gasparini, S.; Ernst, A.; Schuhmann, M.; Eberhardt, R. Endobronchial ultrasound-guided lymph node biopsy with transbronchial needle forceps: A pilot study. Eur. Respir. J. 2012, 39, 373–377. [Google Scholar] [CrossRef]
- Mehta, R.M.; Aurangabadbadwalla, R.; Singla, A.; Loknath, C.; Munavvar, M. Endobronchial ultrasound-guided mediastinal lymph node forceps biopsy in patients with negative rapid-on-site-evaluation: A new step in the diagnostic algorithm. Clin. Respir. J. 2020, 14, 314–319. [Google Scholar] [CrossRef]
- Lerner, A.D.; Feller-Kopman, D. Bronchoscopic techniques used in the diagnosis and staging of lung cancer. JNCCN J. Natl. Compr. Cancer Netw. 2017, 15, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Franke, K.J.; Bruckner, C.; Szyrach, M.; Ruhle, K.H.; Nilius, G.; Theegarten, D. The contribution of endobronchial ultrasound-guided forceps biopsy in the diagnostic workup of unexplained mediastinal and hilar lymphadenopathy. Lung 2012, 190, 227–232. [Google Scholar] [CrossRef]
- Chrissian, A.; Misselhorn, D.; Chen, A. Endobronchial-ultrasound guided miniforceps biopsy of mediastinal and hilar lesions. Ann. Thorac. Surg. 2011, 92, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Radchenko, C.C.; Cho, P.K.; Kang, L.; Saettele, T.M. Performance of endobronchial-ultrasound guided miniforceps biopsy of targeted mediastinal and hilar lesions. Respir. Med. 2019, 158, 92–96. [Google Scholar] [CrossRef]
- Plönes, T.; Mardanzai, K.; Gafencu, D.; Viehof, J.; Hager, T.; Theegarten, D.; Dührsen, U.; Darwiche, K.; Taube, C.; Aigner, C. Cytology Versus Histology in the Primary Diagnosis of Lymphoma Located in the Mediastinum. Ann. Thorac. Surg. 2019, 108, 244–248. [Google Scholar] [CrossRef]
- Zhang, J.; Guo, J.-R.; Huang, Z.-S.; Fu, W.-L.; Wu, X.-L.; Wu, N.; Kuebler, W.M.; Herth, F.J.F.; Fan, Y. Transbronchial mediastinal cryobiopsy in the diagnosis of mediastinal lesions: A randomised trial. Eur. Respir. J. 2021, 58, 2100055. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| EBUS-TBFB (Lymph Node n = 107 Tumor n = 11) | 19 G EBUS-TBNA (Lymph Nodes n = 130 Tumor n = 2) | 22 G EBUS-TBNA (Lymph Node n = 152 Tumor n = 9) | |||
|---|---|---|---|---|---|
| Lymph node station/Tumor | Lymph node station/Tumor | Lymph node station/Tumor | |||
| 4R | 7 | 4R | 30 | 4R | 30 |
| 11R | 24 | 11R | 22 | 11R | 26 |
| 4L | 4 | 4L | 10 | 4L | 21 |
| 11L | 21 | 11L | 23 | 11L | 30 |
| 7 | 48 | 7 | 42 | 7 | 41 |
| 10R | 1 | 2R | 2 | 10R | 1 |
| 12L | 2 | 12L | 1 | 10L | 2 |
| Tumor | 11 | Tumor | 2 | 12L | 1 |
| Tumor | 9 | ||||
| Size of Lymph node | Size of Lymph node | Size of Lymph node | |||
| ≥10–20 mm | 72 | ≥10–20 mm | 108 | ≥10–20 mm | 70 |
| ≥21–30 mm | 22 | ≥21–30 mm | 13 | ≥21–30 mm | 54 |
| ≥31 mm | 13 | ≥31 mm | 9 | ≥31 mm | 28 |
| Size of Tumor | Size of Tumor | Size of Tumor | |||
| ≥10–20 mm | 2 | ≥10–20 mm | 0 | ≥10–20 mm | 2 |
| ≥21–30 mm | 4 | ≥21–30 mm | 0 | ≥21–30 mm | 4 |
| ≥31 mm | 5 | ≥31 mm | 2 | ≥31 mm | 3 |
| Characteristics (n = 105) | |
|---|---|
| Mean Age at Intervention | 63.1 ± 13.6 |
| Gender | |
| Female | 37 (35.2) |
| Male | 68 (64.8) |
| Smoking | |
| Never smoker | 44 (41.9) |
| Active smoker | 31 (29.5) |
| Former smoker | 30 (28.6) |
| Concomitant diseases | |
| Cardiovascular disease | 59 (56.2) |
| Respiratory disease | 34 (32.4) |
| Renal disease | 11 (10.5) |
| Neurological disease | 19 (18.1) |
| Prior malignancy | 29 (27.6) |
| Diabetes | 13 (12.4) |
| Final Diagnosis | |||||
|---|---|---|---|---|---|
| Lung Cancer | Other Malignancies 1 | Lymphoma | Sarcoidosis | Other | |
| Total (n = 105) | 45 | 7 | 8 | 27 | 18 |
| Indication | |||||
| Lung cancer diagnosis 2 (n = 41) | 33/41 (80.5) | 3/41 (7.3) | 1/41 (2.4) | 1/41 (2.4) | 3/41 (7.3) |
| Staging (n = 15) | 11/15 (73.3) | 2/15 (13.3) | 1/15 (6.7) | 0 | 1/15 (6.7) |
| Sarcoidosis (n = 36) | 0 | 2/36 (5.6) | 1/36 (2.7) | 24/36 (66.7) | 9/36 (25) |
| Lymphoma (n = 9) | 1/9 (11.1) | 0 | 5/9 (55.6) | 2/9 (22.2) | 1/9 (11.1) |
| Infection 3 (n = 3) | 0 | 0 | 0 | 0 | 3/3 (100) |
| Other (n = 1) | 0 | 0 | 0 | 0 | 1/1 (100) |
| Total | TBNA | TBNA plus TBFB | p-Value | |
|---|---|---|---|---|
| Overall | 105 | 65/105 (61.9) | 90/105 (85.7) | <0.001 |
| Final diagnosis | ||||
| Lung cancer | 34 | 26/34 (76.5) | 33/34 (97.1) | 0.016 |
| Lung cancer staging | 11 | 7/11 (63.6) | 7/11 (63.6) | >0.05 |
| Other malignancies * | 7 | 3/7 (42.9) | 4/7 (57.1) | >0.05 |
| Lymphoma | 8 | 5/8 (62.5) | 6/8 (75) | >0.05 |
| Sarcoidosis | 27 | 12/27 (44.4) | 23/27 (85.2) | 0.001 |
| Other | 18 | 12/18 (66.7) | 17/18 (94.4) | >0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rüber, F.; Wiederkehr, G.; Steinack, C.; Höller, S.; Bode, P.K.; Kölbener, F.; Franzen, D.P. Endobronchial Ultrasound-Guided Transbronchial Forceps Biopsy: A Retrospective Bicentric Study Using the Olympus 1.5 mm Mini-Forceps. J. Clin. Med. 2022, 11, 4700. https://doi.org/10.3390/jcm11164700
Rüber F, Wiederkehr G, Steinack C, Höller S, Bode PK, Kölbener F, Franzen DP. Endobronchial Ultrasound-Guided Transbronchial Forceps Biopsy: A Retrospective Bicentric Study Using the Olympus 1.5 mm Mini-Forceps. Journal of Clinical Medicine. 2022; 11(16):4700. https://doi.org/10.3390/jcm11164700
Chicago/Turabian StyleRüber, Fabienne, Gilles Wiederkehr, Carolin Steinack, Sylvia Höller, Peter Karl Bode, Fabian Kölbener, and Daniel Peter Franzen. 2022. "Endobronchial Ultrasound-Guided Transbronchial Forceps Biopsy: A Retrospective Bicentric Study Using the Olympus 1.5 mm Mini-Forceps" Journal of Clinical Medicine 11, no. 16: 4700. https://doi.org/10.3390/jcm11164700