
Lung Ultrasound for the Exclusion of Pneumothorax after Interventional Bronchoscopies—A Retrospective Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
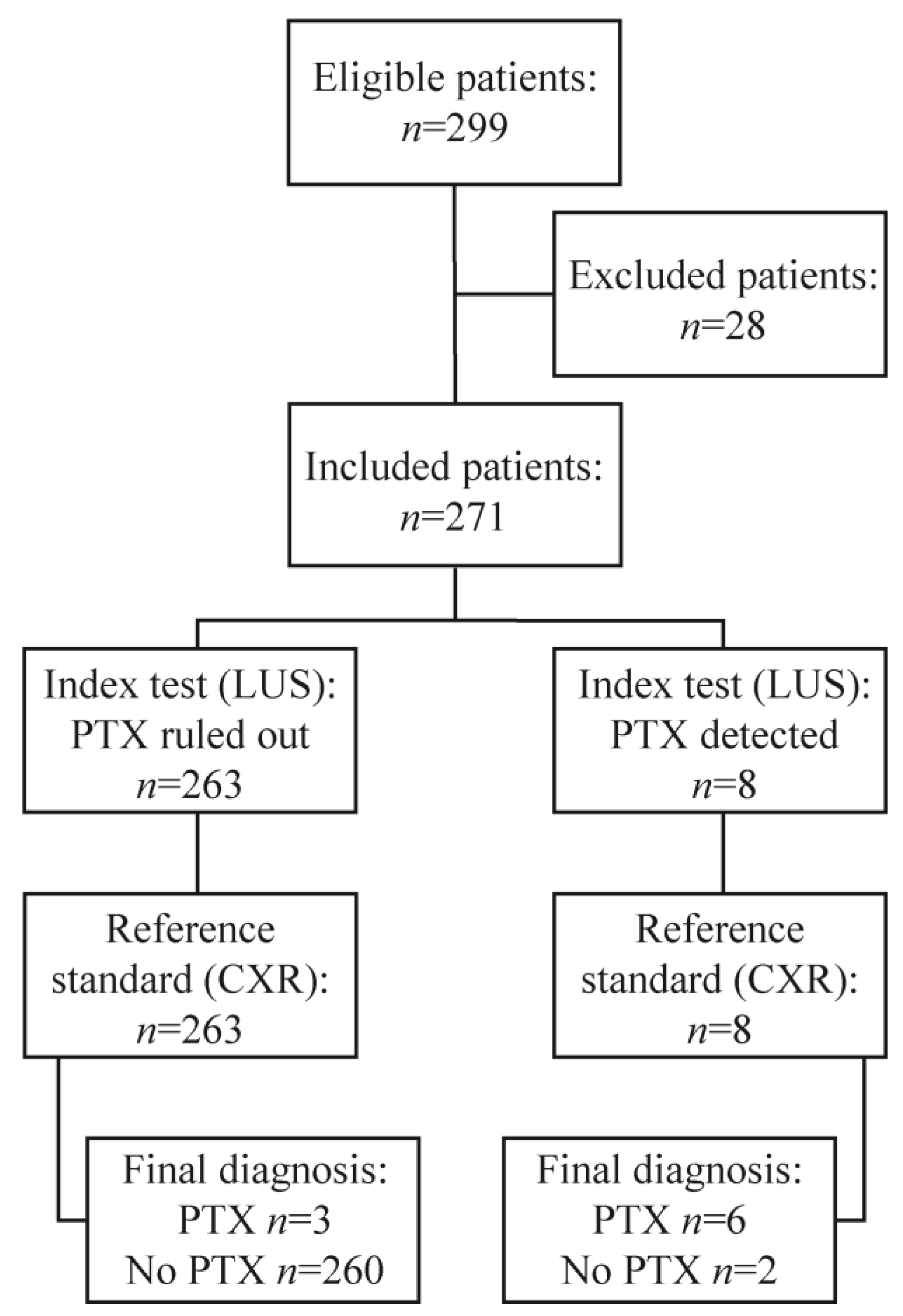
2.1. Overall Study Design and Patient Selection
2.2. Procedure and Screening for Pneumothorax
2.3. Reference Standard
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Izbicki, G.; Romem, A.; Arish, N.; Cahan, C.; Azulai, H.; Chen-Shuali, C.; Tennenhaus, E.; Bar-Yosef, Z.; Zlotkevich, E.; Rokach, A. Avoiding Routine Chest Radiography after Transbronchial Biopsy Is Safe. Respiration 2016, 92, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Izbicki, G.; Shitrit, D.; Yarmolovsky, A.; Bendayan, D.; Miller, G.; Fink, G.; Mazar, A.; Kramer, M.R. Is routine chest radiography after transbronchial biopsy necessary?: A prospective study of 350 cases. Chest 2006, 129, 1561–1564. [Google Scholar] [CrossRef]
- Kreuter, M.; Eberhardt, R.; Wenz, H.; Schmitteckert, H.; Heussel, C.-P.; Herth, F. Diagnostische Wertigkeit der transthorakalen Sonografie vergleichend zur Thoraxübersicht beim Nachweis eines postinterventionellen Pneumothorax. Ultraschall der Med. Eur. J. Ultrasound 2011, 32 (Suppl. S2), E20–E23. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Agarwal, R.; Aggarwal, A.N.; Gupta, D.; Jindal, S.K. Role of ultrasonography in the diagnosis and management of pneumothorax following transbronchial lung biopsy. J. Bronc- Interv. Pulmonol. 2015, 22, 14–19. [Google Scholar] [CrossRef]
- Dhooria, S.; Sehgal, I.S.; Aggarwal, A.N.; Behera, D.; Agarwal, R. Diagnostic Yield and Safety of Cryoprobe Transbronchial Lung Biopsy in Diffuse Parenchymal Lung Diseases: Systematic Review and Meta-Analysis. Respir Care 2016, 61, 700–712. [Google Scholar] [CrossRef]
- Ravaglia, C.; Bonifazi, M.; Wells, A.U.; Tomassetti, S.; Gurioli, C.; Piciucchi, S.; Dubini, A.; Tantalocco, P.; Sanna, S.; Negri, E.; et al. Safety and Diagnostic Yield of Transbronchial Lung Cryobiopsy in Diffuse Parenchymal Lung Diseases: A Comparative Study versus Video-Assisted Thoracoscopic Lung Biopsy and a Systematic Review of the Literature. Respiration 2016, 91, 215–227. [Google Scholar] [CrossRef]
- Gershman, E.; Fruchter, O.; Benjamin, F.; Nader, A.R.; Rosengarten, D.; Rusanov, V.; Fridel, L.; Kramer, M.R. Safety of Cryo-Transbronchial Biopsy in Diffuse Lung Diseases: Analysis of Three Hundred Cases. Respiration 2015, 90, 40–46. [Google Scholar] [CrossRef]
- Labarca, G.; Uribe, J.P.; Pacheco, C.; Folch, E.; Kheir, F.; Majid, A.; Jantz, M.A.; Mehta, H.J.; Patel, N.; Herth, F.J.F.; et al. Bronchoscopic Lung Volume Reduction with Endobronchial Zephyr Valves for Severe Emphysema: A Systematic Review and Meta-Analysis. Respiration 2019, 98, 268–278. [Google Scholar] [CrossRef] [PubMed]
- Schnell, J.; Beer, M.; Eggeling, S.; Gesierich, W.; Gottlieb, J.; Herth, F.; Hofmann, H.S.; Jany, B.; Kreuter, M.; Ley-Zaporozhan, J.; et al. Management of Spontaneous Pneumothorax and Postinterventional Pneumothorax: German S3-Guideline. Zent. Chir 2018, 143, S12–S43. [Google Scholar] [CrossRef]
- Du Rand, I.A.; Blaikley, J.; Booton, R.; Chaudhuri, N.; Gupta, V.; Khalid, S.; Mandal, S.; Martin, J.; Mills, J.; Navani, N.; et al. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: Accredited by NICE. Thorax 2013, 68 (Suppl. S1), i1–i44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gompelmann, D.; Herth, F.J.; Slebos, D.J.; Valipour, A.; Ernst, A.; Criner, G.J.; Eberhardt, R. Pneumothorax following endobronchial valve therapy and its impact on clinical outcomes in severe emphysema. Respiration 2014, 87, 485–491. [Google Scholar] [CrossRef]
- Valipour, A.; Slebos, D.J.; de Oliveira, H.G.; Eberhardt, R.; Freitag, L.; Criner, G.J.; Herth, F.J. Expert statement: Pneumothorax associated with endoscopic valve therapy for emphysema--potential mechanisms, treatment algorithm, and case examples. Respiration 2014, 87, 513–521. [Google Scholar] [CrossRef]
- Chan, K.K.; A Joo, D.; McRae, A.D.; Takwoingi, Y.; A Premji, Z.; Lang, E.; Wakai, A. Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department. Cochrane Database Syst. Rev. 2020, 7, Cd013031. [Google Scholar] [CrossRef] [PubMed]
- Eisenmann, S.; Winantea, J.; Karpf-Wissel, R.; Funke, F.; Stenzel, E.; Taube, C.; Darwiche, K. Thoracic Ultrasound for Immediate Exclusion of Pneumothorax after Interventional Bronchoscopy. J. Clin. Med. 2020, 9, 1486. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, Z. Bedside ultrasonography for diagnosis of pneumothorax. Quant. Imaging Med. Surg. 2015, 5, 618–623. [Google Scholar] [CrossRef]
- Husain, L.F.; Hagopian, L.; Wayman, D.; E Baker, W.; A Carmody, K. Sonographic diagnosis of pneumothorax. J. Emergencies, Trauma, Shock. 2012, 5, 76–81. [Google Scholar] [CrossRef]
- MacDuff, A.; Arnold, A.; Harvey, J. Management of spontaneous pneumothorax: British Thoracic Society pleural disease guideline 2010. Thorax 2010, 65 (Suppl. S2), ii18–ii31. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.; Velez, M.I.; Soni, N.J.; Proud, K.C. Delayed pneumothorax after transbronchial lung biopsy. BMJ Case Rep. 2021, 14, e240985. [Google Scholar] [CrossRef]
- Bensted, K.; McKenzie, J.; Havryk, A.; Plit, M.; Ben-Menachem, E. Lung Ultrasound After Transbronchial Biopsy for Pneumothorax Screening in Post–Lung Transplant Patients. J. Bronc- Interv. Pulmonol. 2018, 25, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Laursen, C.B.; Pietersen, P.I.; Jacobsen, N.; Falster, C.; Juul, A.D.; Davidsen, J.R. Lung ultrasound assessment for pneumothorax following transbronchial lung cryobiopsy. ERJ Open Res. 2021, 7, 00045–2021. [Google Scholar] [CrossRef] [PubMed]
- Viglietta, L.; Inchingolo, R.; Pavano, C.; Tomassetti, S.; Piciucchi, S.; Smargiassi, A.; Ravaglia, C.; Dubini, A.; Gurioli, C.; Gurioli, C.; et al. Ultrasonography for the Diagnosis of Pneumothorax after Transbronchial Lung Cryobiopsy in Diffuse Parenchymal Lung Diseases. Respiration 2017, 94, 232–236. [Google Scholar] [CrossRef]
- Honeybourne, D.; Babb, J.; Bowie, P.; Brewin, A.; Fraise, A.; Garrard, C.; Harvey, J.; Lewis, R.; Neumann, C.; Wathen, C.G.; et al. British Thoracic Society guidelines on diagnostic flexible bronchoscopy. Thorax 2001, 56 (Suppl. S1), i1-21. [Google Scholar] [CrossRef]
- Luketich, J.D.; Kiss, M.; Hershey, J.; Urso, G.K.; Wilson, J.; Bookbinder, M.; Ginsberg, R. Chest tube insertion: A prospective evaluation of pain management. Clin. J. Pain 1998, 14, 152–154. [Google Scholar] [CrossRef]
- Beres, R.A.; Goodman, L.R. Pneumothorax: Detection with upright versus decubitus radiography. Radiology 1993, 186, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Sartori, S.; Tombesi, P.; Trevisani, L.; Nielsen, I.; Tassinari, D.; Abbasciano, V. Accuracy of Transthoracic Sonography in Detection of Pneumothorax After Sonographically Guided Lung Biopsy: Prospective Comparison with Chest Radiography. Am. J. Roentgenol. 2007, 188, 37–41. [Google Scholar] [CrossRef]
- Shostak, E.; Brylka, D.; Krepp, J.; Pua, B.; Sanders, A. Bedside Sonography for Detection of Postprocedure Pneumothorax. J. Ultrasound Med. 2013, 32, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, G.; Busso, M.; Perotto, F.; De Pascale, A.; Fava, C. Ultrasound diagnosis of pneumothorax. Radiol. Med. 2006, 111, 516–525. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Final Diagnosis * | Initial CXR | Signs/Symptoms | Repeat CXR |
|---|---|---|---|
| No PTX | Negative | Negative | N/A |
| No PTX | Negative | Positive | Negative |
| No PTX | Positive | Negative | Negative |
| No PTX | Inconclusive | Positive/negative | Negative |
| PTX | Negative | Positive | Positive |
| PTX | Positive | Positive | N/A |
| PTX | Inconclusive | Positive/negative | Positive |
| Variables | Total (n = 271) | Early PTX (n = 9) | p-Value |
|---|---|---|---|
| Age (years) | 62 (14) | 60.2 (10.0) | 0.773 |
| Sex | 0.006 * | ||
| Male | 155 (57.2) | 1 (11.1) | |
| Female | 116 (42.8) | 8 (88.9) | |
| BMI (kg/m2) | 25.0 (4.8) | 22.8 (3.6) | 0.145 |
| Smoking status | 0.153 | ||
| Never-smoker | 83 (30.6) | 2 (22.2) | |
| Former smoker | 132 (48.7) | 7 (77.8) | |
| Current smoker | 56 (20.7) | 0 (0) | |
| Indication for flexible bronchoscopy | 0.254 | ||
| Suspected pulmonary malignancy | 109 (40.2) | 2 (22.2) | |
| Surveillance after lung transplant | 29 (10.7) | 1 (11.1) | |
| Lung volume reduction | 36 (13.3) | 1 (11.1) | |
| Suspected ILD other than sarcoidosis | 30 (11.1) | 3 (33.3) | |
| Suspected sarcoidosis | 26 (9.6) | 0 (0) | |
| Suspected infectious disease | 22 (8.1) | 1 (11.1) | |
| Suspected non-infectious inflammatory disease | 12 (4.4) | 0 (0) | |
| Other indications | 7 (2.6) | 1 (11.1) |
| Variables | Total (n = 271) | Early PTX (n = 9) | p-Value |
|---|---|---|---|
| Type of intervention | 0.226 | ||
| TBFB | 164 (60.5) | 3 (33.3) | |
| TBLC | 39 (14.4) | 3 (33.3) | |
| TBFB + TBLC | 32 (11.8) | 2 (22.2) | |
| EBV | 36 (13.3) | 1 (11.1) | |
| Bronchial brushing | 82 (30.3) | 2 (22.2) | 0.728 |
| Anaesthesia | 0.745 | ||
| Sedation | 163 (60.1) | 5 (55.6) | |
| General anaesthesia | 108 (39.9) | 4 (44.4) | |
| Experience level of operator | 1.00 | ||
| Senior | 257 (94.8) | 9 (100.0) | |
| Resident | 14 (5.2) | 0 (0) |
| Lung Ultrasound | Reference Standard | Total | |
|---|---|---|---|
| Pneumothorax + | Pneumothorax − | ||
| Pneumothorax + | 6 | 2 | 8 |
| Pneumothorax - | 3 | 260 | 263 |
| Total | 9 | 262 | 271 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mangold, M.S.; Rüber, F.; Steinack, C.; Gautschi, F.; Wani, J.; Grimaldi, S.; Franzen, D.P. Lung Ultrasound for the Exclusion of Pneumothorax after Interventional Bronchoscopies—A Retrospective Study. J. Clin. Med. 2023, 12, 1474. https://doi.org/10.3390/jcm12041474
Mangold MS, Rüber F, Steinack C, Gautschi F, Wani J, Grimaldi S, Franzen DP. Lung Ultrasound for the Exclusion of Pneumothorax after Interventional Bronchoscopies—A Retrospective Study. Journal of Clinical Medicine. 2023; 12(4):1474. https://doi.org/10.3390/jcm12041474
Chicago/Turabian StyleMangold, Melanie Scarlett, Fabienne Rüber, Carolin Steinack, Fiorenza Gautschi, Jasmin Wani, Sascha Grimaldi, and Daniel Peter Franzen. 2023. "Lung Ultrasound for the Exclusion of Pneumothorax after Interventional Bronchoscopies—A Retrospective Study" Journal of Clinical Medicine 12, no. 4: 1474. https://doi.org/10.3390/jcm12041474