
Modern Bronchoscopic Treatment Options for Patients with Chronic Bronchitis
Abstract
:1. Introduction
2. Bronchoscopic Treatment Options for Chronic Bronchitis and Frequent Exacerbations
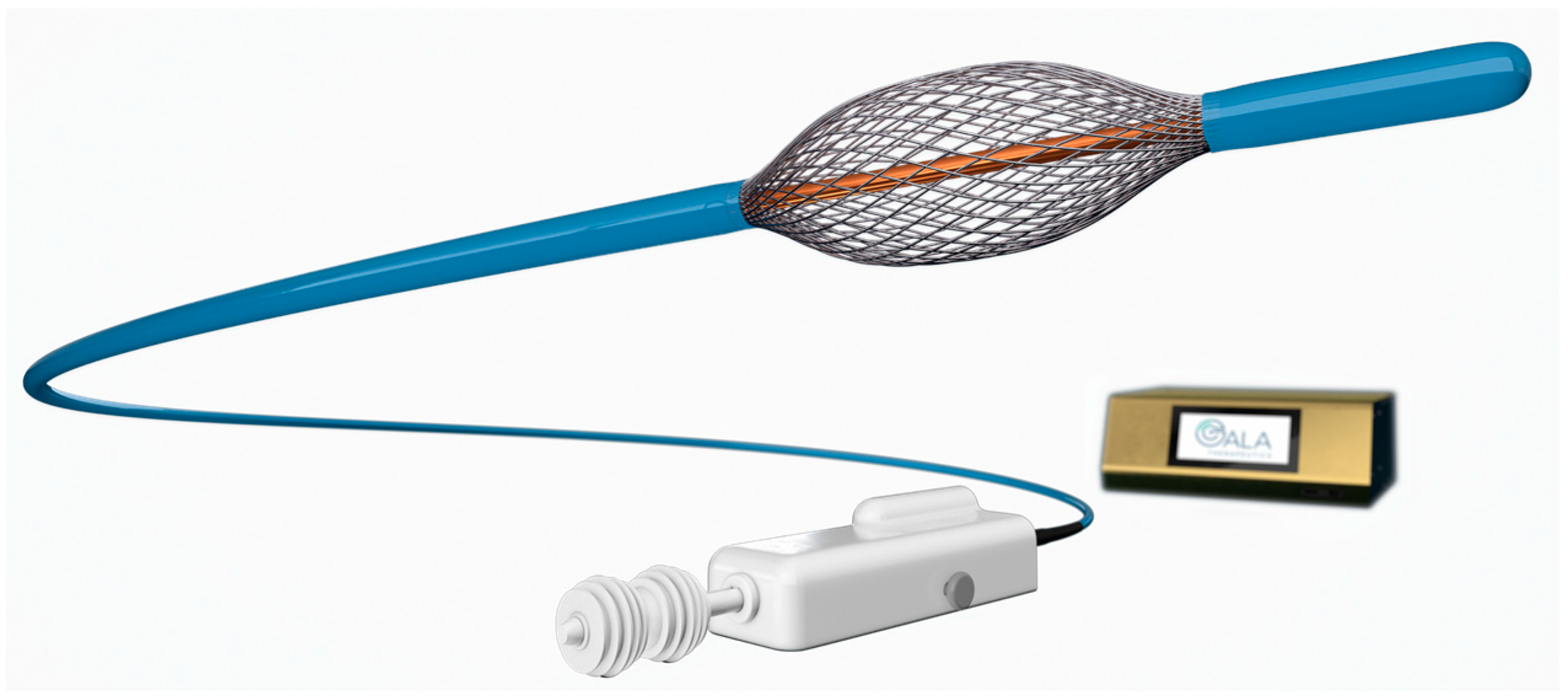
2.1. RheOx Bronchial Rheoplasty
2.2. RejuvenAir System Metered Cryospray
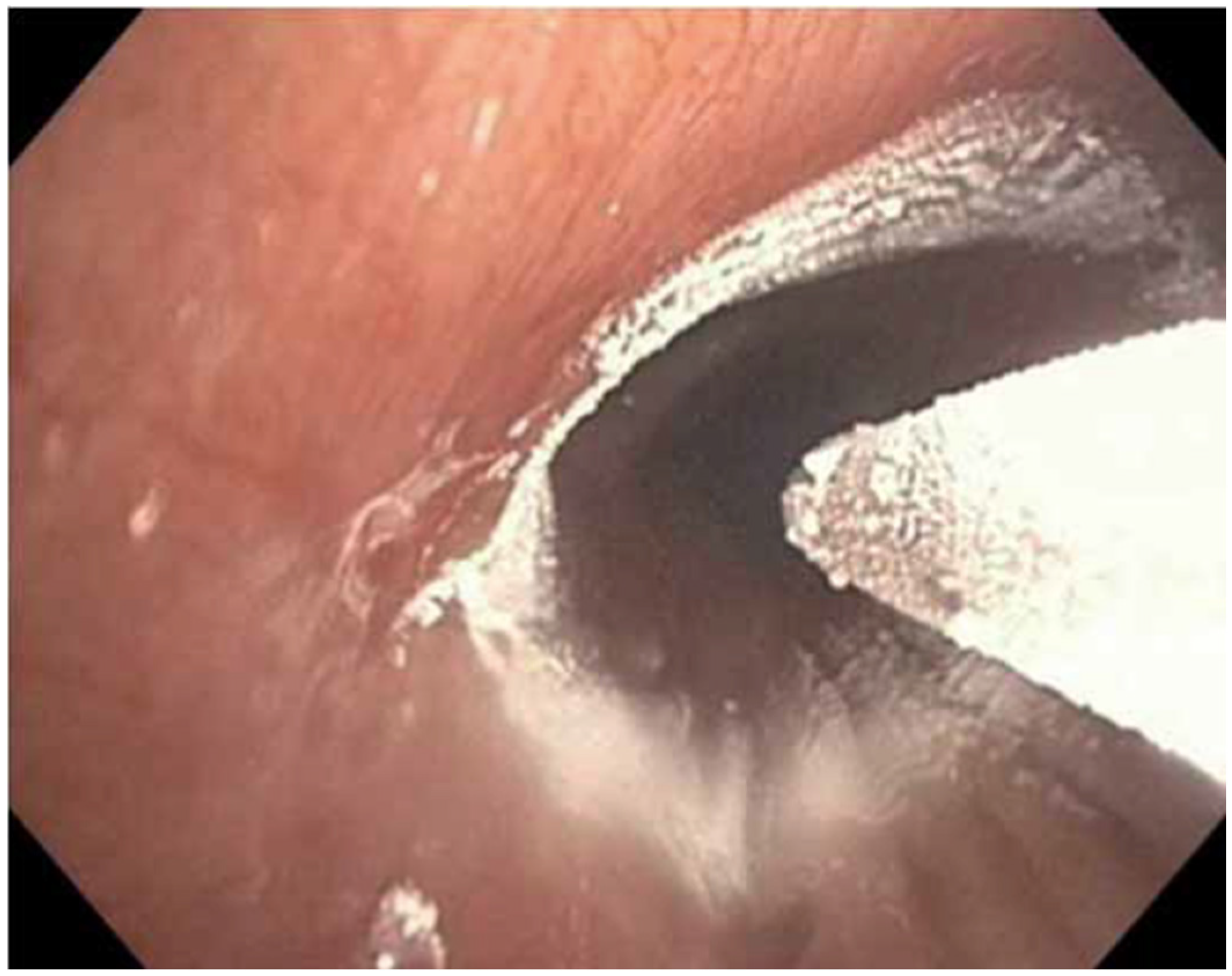
2.3. Karakoca Resector Balloon Desobstruction
2.4. Targeted Lung Denervation

{kind=link}
{kind=link}
{kind=link}
| Endpoint | Time | Group | Result | p Value | Reference |
|---|---|---|---|---|---|
| Bronchial rheoplasty | |||||
| CAT, absolute change | 6 months | −8.0 (−14.0 to −2.0) * | 0.0002 | [22] | |
| 6 months | −5.4 ± 7.6 | N/A | [23] | ||
| SGRQ, absolute change | 6 months | −7.2 (−19.8 to −3.1) * | 0.0002 | [22] | |
| 6 months | −8.0 ± 15.4 | N/A | [23] | ||
| Metered cryospray | |||||
| CAT, absolute change | 3 months | −3.8 ± 7.1 | <0.01 | [24] | |
| 12 months | −2.0 ± 7.2 | 0.12 | [24] | ||
| SGRQ, absolute change | 3 months | −6.4 ± 14.4 | 0.01 | [24] | |
| 12 months | −4.6 ± 15.1 | 0.10 | [24] | ||
| LCQ, absolute change | 3 months | 21.6 ± 32.2 | <0.01 | [24] | |
| 12 months | 9.1 ±29.0 | 0.17 | [24] | ||
| Karakoca balloon desobstruction | |||||
| FEV1, absolute (l) | baseline | 0.77 ± 0.26 | |||
| 1 month | 1.3 ± 0.5 | <0.001 | [29] | ||
| Borg scale, absolute | baseline | 8.7 ± 0.6 | |||
| 1 month | 5.1 ± 0.7 | 0.002 | [29] | ||
| 6MWT, absolute (m) | baseline | 68.7 ± 41.4 | |||
| 1 month | 387.4 ± 113.4 | <0.001 | [29] | ||
| Targeted lung denervation | |||||
| FEV1, relative change | 12 months | 20 W | 11.6 ± 32.3 | [30] | |
| 12 months | 15 W | 0.02 ± 15.1 | 20 vs. 15 W 0.324 | [30] | |
| 12 months | 40.3 ± 42.1 | <0.05 | [35] | ||
| FEV1, absolute change (mL) | 12 months | 29 W | 57.0 ± 82.0 | 0.03 | [36] |
| 12 months | 32 W | 94.2 ± 228.0 | 0.18 | [36] | |
| 6 months | TLD | 127.6 ± 201.0 | Sham vs. TLD 0.345 | [39] | |
| 12 months | TLD | 74.3 ± 213.1 | Sham vs. TLD 0.539 | [39] | |
| 2 years | TLD | −0.02 ± 0.14 | 1 vs. 2 years > 0.05 | [40] | |
| 6MWT, absolute change | 12 months | 20 W | 24.2 ± 45.6 | [30] | |
| 12 months | 15 W | −9.3 ± 70.6 | 20 vs. 15 W 0.224 | [30] | |
| 12 months | 53.7 ± 74.4 | <0.05 | [35] | ||
| CAT, absolute change | 12 months | 29 W | 0.3 ±7.8 | 0.890 | [36] |
| 12 months | 32 W | −2.9 ± 6.1 | 0.14 | [36] | |
| 6 months | TLD | −2.0 ± 6.5 | Sham vs. TLD 0.472 | [39] | |
| 12 months | TLD | −0.9 ± 6.4 | Sham vs. TLD 0.175 | [39] | |
| SGRQ, absolute change | 12 months | 20 W | −11.1 ± 9.1 | [30] | |
| 12 months | 15 W | −0.9 ± 8.6 | 20 vs. 15 W 0.045 | [30] | |
| 12 months | 29 W | −1.9 ± 12.5 | 0.617 | [36] | |
| 12 months | 32 W | −7.5 ±10.3 | 0.036 | [36] | |
| 6 months | TLD | −8.3 ± 12.6 | Sham vs. TLD 0.138 | [39] | |
| 12 months | TLD | −5.1 ± 14.4 | Sham vs. TLD 0.441 | [39] | |
| 2 years | TLD | 1.8 ± 12.7 | 1 vs. 2 years > 0.05 | [40] | |
| SGRQ, relative change | 12 months | −1.9 ± 20.8 | >0.05 | [35] | |
| Borg scale, absolute change | 12 months | 20 W | −0.3 ± 2.0 | [30] | |
| 12 months | 15 W | −0.9 ± 2.0 | 20 vs. 15 W 0.556 | [30] | |
| Borg scale, relative change | 12 months | −0.82 ± 1.83 | >0.05 | [35] | |
| mMRC, absolute change | 12 months | 20 W | −0.7 ± 0.8 | [30] | |
| 12 months | 15 W | 0.6 ± 1.3 | 20 vs. 15 W 0.085 | [30] | |
| 6 months | TLD | −0.5 ± 1.0 | Sham vs. TLD 0.337 | [39] | |
| 12 months | TLD | −0.4 ± 0.8 | Sham vs. TLD 0.279 | [39] | |
| 12 months | −0.7 ± 1.1 | >0.05 | [35] |
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). WHO Global Health Observatory. Global Health Estimates. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates (accessed on 22 December 2022).
- Iheanacho, I.; Zhang, S.; King, D.; Rizzo, M.; Ismaila, A.S. Economic Burden of Chronic Obstructive Pulmonary Disease (COPD): A Systematic Literature Review. Int. J. Chron. Obstr. Pulm. Dis. 2020, 15, 439–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease—2023 GOLD Report. Available online: https://goldcopd.org/2023-gold-report-2/ (accessed on 28 December 2022).
- Saetta, M.; Turato, G.; Baraldo, S.; Zanin, A.; Braccioni, F.; Mapp, C.E.; Maestrelli, P.; Cavallesco, G.; Papi, A.; Fabbri, L.M. Goblet cell hyperplasia and epithelial inflammation in peripheral airways of smokers with both symptoms of chronic bronchitis and chronic airflow limitation. Am. J. Respir. Crit. Care Med. 2000, 161 Pt 1, 1016–1021. [Google Scholar] [CrossRef] [PubMed]
- Kim, V.; Oros, M.; Durra, H.; Kelsen, S.; Aksoy, M.; Cornwell, W.D.; Rogers, T.J.; Criner, G.J. Chronic bronchitis and current smoking are associated with more goblet cells in moderate to severe COPD and smokers without airflow obstruction. PLoS ONE 2015, 10, e0116108. [Google Scholar] [CrossRef] [Green Version]
- Kistemaker, L.E.M.; Gosens, R. Acetylcholine beyond bronchoconstriction: Roles in inflammation and remodeling. Trends Pharmacol. Sci. 2015, 36, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Soler-Cataluña, J.J.; Calle, M.; Molina, J.; Almagro, P.; Quintano, J.A.; Riesco, J.A.; Trigueros, J.A.; Piñera, P.; Simón, A.; et al. Spanish COPD Guidelines (GesEPOC): Pharmacological Treatment of Stable COPD. Arch. Bronconeumol. 2012, 48, 247–257. [Google Scholar] [CrossRef]
- Bakeer, M.; Funk, G.-C.; Valipour, A. Chronic obstructive pulmonary disease phenotypes: Imprint on pharmacological and non-pharmacological therapy. Ann. Transl. Med. 2020, 8, 1472. [Google Scholar] [CrossRef]
- Miravitlles, M.; Calle, M.; Molina, J.; Almagro, P.; Gómez, J.T.; Trigueros, J.A.; Cosío, B.G.; Casanova, C.; López-Campos, J.L.; Riesco, J.A.; et al. Spanish COPD Guidelines (GesEPOC) 2021: Updated Pharmacological treatment of stable COPD. Arch. Bronconeumol. 2022, 58, 69–81. [Google Scholar] [CrossRef]
- Cosio, B.G.; Soriano, J.B.; López-Campos, J.L.; Calle, M.; Soler, J.J.; De-Torres, J.P.; Marín, J.M.; Martínez, C.; De Lucas, P.; Mir, I.; et al. Distribution and Outcomes of a Phenotype-Based Approach to Guide COPD Management: Results from the CHAIN Cohort. PLoS ONE 2016, 11, e0160770. [Google Scholar] [CrossRef] [Green Version]
- Koblizek, V.; Milenkovic, B.; Barczyk, A.; Tkacova, R.; Somfay, A.; Zykov, K.; Tudoric, N.; Kostov, K.; Zbozinkova, Z.; Svancara, J.; et al. Phenotypes of COPD patients with a smoking history in Central and Eastern Europe: The POPE Study. Eur. Respir. J. 2017, 49, 1601446. [Google Scholar] [CrossRef] [Green Version]
- Kim, V.; Han, M.L.K.; Vance, G.B.; Make, B.J.; Newell, J.D.; Hokanson, J.E.; Hersh, C.P.; Stinson, D.; Silverman, E.K.; Criner, G.J. The chronic bronchitic phenotype of COPD: An analysis of the COPDGene Study. Chest 2011, 140, 626–633. [Google Scholar] [CrossRef] [Green Version]
- Montes De Oca, M.; Halbert, R.J.; Lopez, M.V.; Perez-Padilla, R.; Tálamo, C.; Moreno, D.; Muiño, A.; Jardim, J.R.B.; Valdivia, G.; Pertuzé, J.; et al. The chronic bronchitis phenotype in subjects with and without COPD: The PLATINO study. Eur. Respir. J. 2012, 40, 28–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodruff, P.G.; Barr, R.G.; Bleecker, E.; Christenson, S.A.; Couper, D.; Curtis, J.L.; Gouskova, N.A.; Hansel, N.N.; Hoffman, E.A.; Kanner, R.E.; et al. Clinical Significance of Symptoms in Smokers with Preserved Pulmonary Function. N. Engl. J. Med. 2016, 374, 1811–1821. [Google Scholar] [CrossRef] [PubMed]
- Soler-Cataluña, J.J.; Martínez-García, M.Á.; Román Sánchez, P.; Salcedo, E.; Navarro, M.; Ochando, R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005, 60, 925–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dransfield, M.T.; Kunisaki, K.M.; Strand, M.J.; Anzueto, A.; Bhatt, S.P.; Bowler, R.P.; Criner, G.J.; Curtis, J.L.; Hanania, N.A.; Nath, H.; et al. Acute exacerbations and lung function loss in smokers with and without chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2017, 195, 324–330. [Google Scholar] [CrossRef] [Green Version]
- Seemungal, T.A.R.; Donaldson, G.C.; Paul, E.A.; Bestall, J.C.; Jeffries, D.J.; Wedzicha, J.A. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1998, 157, 1418–1422. [Google Scholar] [CrossRef] [PubMed]
- Dalal, A.A.; Christensen, L.; Liu, F.; Riedel, A.A. Direct costs of chronic obstructive pulmonary disease among managed care patients. Int. J. Chron. Obstr. Pulm. Dis. 2010, 5 Pt 1, 341–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipson, D.A.; Barnhart, F.; Brealey, N.; Brooks, J.; Criner, G.J.; Day, N.C.; Dransfield, M.T.; Halpin, D.M.G.; Han, M.K.; Jones, C.E.; et al. Once-Daily Single-Inhaler Triple versus Dual Therapy in Patients with COPD. N. Engl. J. Med. 2018, 378, 1671–1680. [Google Scholar] [CrossRef]
- Martinez, F.J.; Calverley, P.M.A.; Goehring, U.-M.; Brose, M.; Fabbri, L.M.; Rabe, K.F. Effect of roflumilast on exacerbations in patients with severe chronic obstructive pulmonary disease uncontrolled by combination therapy (REACT): A multicentre randomised controlled trial. Lancet 2015, 385, 857–866. [Google Scholar] [CrossRef]
- Uzun, S.; Djamin, R.S.; Kluytmans, J.A.J.W.; Mulder, P.G.H.; van’t Veer, N.E.; Ermens, A.A.M.; Pelle, A.J.; Hoogsteden, H.C.; Aerts, J.G.J.V.; Van der Eerden, M.M. Azithromycin maintenance treatment in patients with frequent exacerbations of chronic obstructive pulmonary disease (COLUMBUS): A randomised, double-blind, placebo-controlled trial. Lancet Respir. Med. 2014, 2, 361–368. [Google Scholar] [CrossRef]
- Valipour, A.; Fernandez-Bussy, S.; Ing, A.J.; Steinfort, D.P.; Snell, G.I.; Williamson, J.P.; Saghaie, T.; Irving, L.B.; Dabscheck, E.J.; Krimsky, W.S.; et al. Bronchial Rheoplasty for Treatment of Chronic Bronchitis. Twelve-Month Results from a Multicenter Clinical Trial. Am. J. Respir. Crit. Care Med. 2020, 202, 681–689. [Google Scholar] [CrossRef]
- Darwiche, K.; Zellerhoff, H.; Herth, F.; Brock, J.; Meilinger, M.; Sperk, I.; Valipour, A. Bronchial rheoplasty for chronic bronchitis: Initial results from a european registry study with RheOx®. Eur. Respir. J. 2022, 60 (Suppl. S66), 4026. [Google Scholar] [CrossRef]
- Garner, J.L.; Shaipanich, T.; Hartman, J.E.; Orton, C.M.; Caneja, C.; Klooster, K.; Thornton, J.; Sin, D.D.; Slebos, D.J.; Shah, P.L. A prospective safety and feasibility study of metered cryospray for patients with chronic bronchitis in COPD. Eur. Respir. J. 2020, 56, 2000556. [Google Scholar] [CrossRef] [PubMed]
- Krimsky, W.S.; Broussard, J.N.; Sarkar, S.A.; Harley, D.P. Bronchoscopic spray cryotherapy: Assessment of safety and depth of airway injury. J. Thorac. Cardiovasc. Surg. 2010, 139, 781–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slebos, D.J.; Breen, D.; Coad, J.; Klooster, K.; Hartman, J.; Browning, R.; Shah, P.L.; McNulty, W.H.; Al-Abdul Mohsin, M.; Irshad, K. Safety and Histological Effect of Liquid Nitrogen Metered Spray Cryotherapy in the Lung. Am. J. Respir. Crit. Care Med. 2017, 196, 1351–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartman, J.E.; Garner, J.L.; Shah, P.L.; Slebos, D.J. New bronchoscopic treatment modalities for patients with chronic bronchitis. Eur. Respir. Rev. 2021, 30, 200281. [Google Scholar] [CrossRef]
- Karakoca, Y.; Karaagac Gogus, G.; Yapicier, O. Use of Resector Balloon Desobstruction in Patients with Severe Chronic Obstructive Pulmonary Disease: A Pilot Feasibility Study on a Novel Desobstruction Technique. J. Bronchol. Interv. Pulmonol. 2015, 22, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Karakoca, Y.; Gogus, G.; Akduman, S.; Erturk, B. Follow-up outcomes of chronic obstructive pulmonary disease patients who underwent dilatation and curettage with the Karakoca resector balloon: A 188-case series over 5 years. Medicine 2018, 97, 13400. [Google Scholar] [CrossRef] [PubMed]
- Slebos, D.J.; Klooster, K.; Koegelenberg, C.F.N.; Theron, J.; Styen, D.; Valipour, A.; Mayse, M.; Bolliger, C.T. Targeted lung denervation for moderate to severe COPD: A pilot study. Thorax 2015, 70, 411–419. [Google Scholar] [CrossRef] [Green Version]
- Hummel, J.P.; Mayse, M.L.; Dimmer, S.; Johnson, P.J. Physiologic and histopathologic effects of targeted lung denervation in an animal model. J. Appl. Physiol. 2019, 126, 67–76. [Google Scholar] [CrossRef]
- Mayse, M.L.; Norman, H.S.; Peterson, A.D.; Rouw, K.T.; Johnson, P.J. Targeted lung denervation in sheep: Durability of denervation and long-term histologic effects on bronchial wall and peribronchial structures. Respir. Res. 2020, 21, 117. [Google Scholar] [CrossRef]
- Kistemaker, L.E.M.; Slebos, D.J.; Meurs, H.; Kerstjens, H.A.M.; Gosens, R. Anti-inflammatory effects of targeted lung denervation in patients with COPD. Eur. Respir. J. 2015, 46, 1489–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koegelenberg, C.F.N.; Theron, J.; Slebos, D.J.; Klooster, K.; Mayse, M.; Gosens, R. Antimuscarinic Bronchodilator Response Retained after Bronchoscopic Vagal Denervation in Chronic Obstructive Pulmonary Disease Patients. Respiration 2016, 92, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Valipour, A.; Asadi, S.; Pison, C.; Jondot, M.; Kessler, R.; Benneddif, K.; Deslee, G.; Verdier, M.; Slebos, D.J.; Mayse, M. Long-term safety of bilateral targeted lung denervation in patients with COPD. Int. J. Chron. Obstr. Pulm. Dis. 2018, 13, 2163–2172. [Google Scholar] [CrossRef] [Green Version]
- Valipour, A.; Shah, P.L.; Pison, C.; Ninane, V.; Janssens, W.; Perez, T.; Kessler, R.; Deslee, G.; Garner, J.; Abele, C.; et al. Safety and Dose Study of Targeted Lung Denervation in Moderate/Severe COPD Patients. Respiration 2019, 98, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Pison, C.; Shah, P.L.; Slebos, D.-J.; Ninane, V.; Janssens, W.; Perez, T.; Kessler, R.; Deslee, G.; Garner, J.L.; Hartman, J.E.; et al. Safety of denervation following targeted lung denervation therapy for COPD: AIRFLOW-1 3-year outcomes. Respir. Res. 2021, 22, 62. [Google Scholar] [CrossRef] [PubMed]
- Hartman, J.E.; Conway, F.; Degano, B.; Augustijn, S.W.S.; Herth, F.J.F.; Mayr, A.; Chacaroun, S.; Tonkin, J.; Valipour, A.; Slebos, D.J. Rate of lung function decline slows in the 3 years after targeted lung denervation in COPD. Respir. Med. 2021, 188, 106604. [Google Scholar] [CrossRef]
- Slebos, D.J.; Shah, P.L.; Herth, F.J.F.; Pison, C.; Schumann, C.; Hübner, R.H.; Bonta, P.; Kessler, R.; Gesierich, W.; Darwiche, K.; et al. Safety and Adverse Events after Targeted Lung Denervation for Symptomatic Moderate to Severe Chronic Obstructive Pulmonary Disease (AIRFLOW). A Multicenter Randomized Controlled Clinical Trial. Am. J. Respir. Crit. Care Med. 2019, 200, 1477–1486. [Google Scholar] [CrossRef]
- Valipour, A.; Shah, P.L.; Herth, F.J.; Pison, C.; Schumann, C.; Hübner, R.; Bonta, P.I.; Kessler, R.; Gesierich, W.; Darwiche, K.; et al. Two-Year Outcomes for the Double-Blind, Randomized, Sham-Controlled Study of Targeted Lung Denervation in Patients with Moderate to Severe COPD: AIRFLOW-2. Int. J. Chron. Obstr. Pulm. Dis. 2020, 15, 2807–2816. [Google Scholar] [CrossRef]
- Conway, F.; Tonkin, J.; Valipour, A.; Pison, C.; Schumann, C.; Bonta, P.I.; Kessler, R.; Gesierich, W.; Darwiche, K.; Lamprecht, B.; et al. Crossover Patient Outcomes for Targeted Lung Denervation in Moderate to Severe Chronic Obstructive Pulmonary Disease: AIRFLOW-2. Respiration 2022, 101, 1069–1074. [Google Scholar] [CrossRef]
- Slebos, D.J.; Degano, B.; Valipour, A.; Shah, P.L.; Deslée, G.; Sciurba, F.C. Design for a multicenter, randomized, sham-controlled study to evaluate safety and efficacy after treatment with the Nuvaira® lung denervation system in subjects with chronic obstructive pulmonary disease (AIRFLOW-3). BMC Pulm. Med. 2020, 20, 41. [Google Scholar] [CrossRef] [Green Version]
- Restrepo, R.D.; Alvarez, M.T.; Wittnebel, L.D.; Sorenson, H.; Wettstein, R.; Vines, D.L.; Sikkema-Ortiz, J.; Gardner, D.D.; Wilkins, R.L. Medication adherence issues in patients treated for COPD. Int. J. Chron. Obstr. Pulm. Dis. 2008, 3, 371–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Campos, J.L.; Gallego, E.Q.; Hernández, L.C. Status of and strategies for improving adherence to COPD treatment. Int. J. Chron. Obstr. Pulm. Dis. 2019, 14, 1503–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzanakis, N.; Koulouris, N.; Dimakou, K.; Gourgoulianis, K.; Kosmas, E.; Chasapidou, G.; Konstantinidis, A.; Kyriakopoulos, C.; Kontakiotis, T.; Rapti, A.; et al. Classification of COPD patients and compliance to recommended treatment in Greece according to GOLD 2017 report: The RELICO study. BMC Pulm. Med. 2021, 21, 216. [Google Scholar] [CrossRef] [PubMed]
- Schilling, R.; Dhillon, G.S.; Tondo, C.; Riva, S.; Grimaldi, M.; Quadrini, F.; Neuzil, P.; Chierchia, G.B.; De Asmundis, C.; Abdelaal, A.; et al. Safety, effectiveness, and quality of life following pulmonary vein isolation with a multi-electrode radiofrequency balloon catheter in paroxysmal atrial fibrillation: 1-year outcomes from SHINE. Europace 2021, 23, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, T.; Rubin, B.K. Airway Goblet Cells Secrete Pro-Inflammatory Cytokines, Chemokines, and Growth Factors. Chest 2016, 149, 714–720. [Google Scholar] [CrossRef]
- Srikanthan, K.; Kistemaker, L.; Slebos, D.-J.; Gesierich, W.; Darwiche, K.; Bonta, P.; Deslee, G.; Shah, P.; Gosens, R. Targeted lung denervation modulates the mucosal epithelial transcriptome in COPD. ERJ Open Res. 2022, 8, 00146–02022. [Google Scholar] [CrossRef]
- Hartman, J.E.; Srikanthan, K.; Caneja, C.; ten Hacken, N.H.T.; Kerstjens, H.A.M.; Shah, P.L.; Slebos, D.J. Bronchoscopic Targeted Lung Denervation in Patients with Severe Asthma: Preliminary Findings. Respiration 2022, 101, 184–189. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mayr, A.K.; Valipour, A. Modern Bronchoscopic Treatment Options for Patients with Chronic Bronchitis. J. Clin. Med. 2023, 12, 1854. https://doi.org/10.3390/jcm12051854
Mayr AK, Valipour A. Modern Bronchoscopic Treatment Options for Patients with Chronic Bronchitis. Journal of Clinical Medicine. 2023; 12(5):1854. https://doi.org/10.3390/jcm12051854
Chicago/Turabian StyleMayr, Anna Katharina, and Arschang Valipour. 2023. "Modern Bronchoscopic Treatment Options for Patients with Chronic Bronchitis" Journal of Clinical Medicine 12, no. 5: 1854. https://doi.org/10.3390/jcm12051854