
Correlation between Choroidal Vascularity Index and Outer Retina in Patients with Diabetic Retinopathy


Abstract
:1. Introduction
2. Materials and Methods
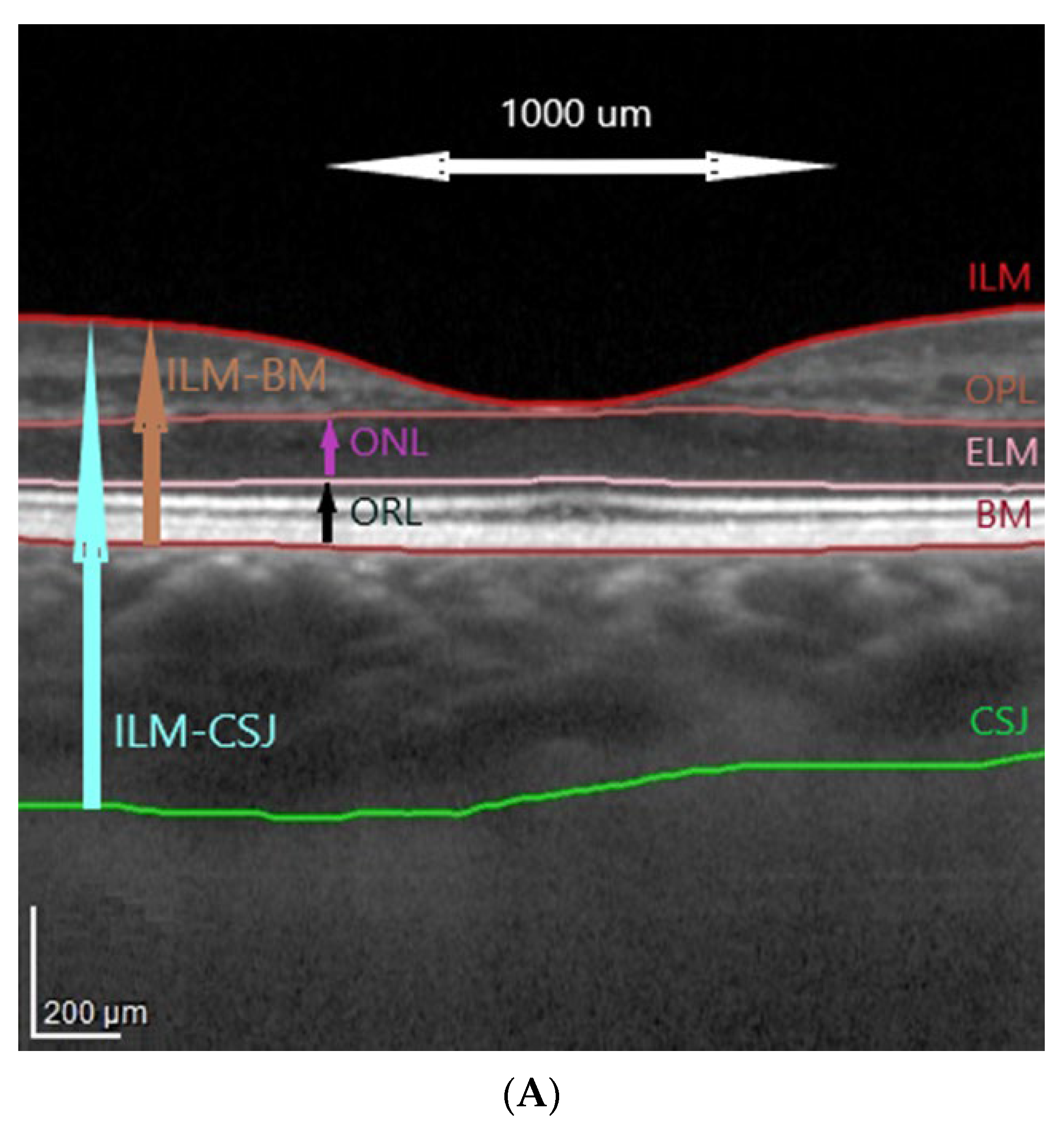
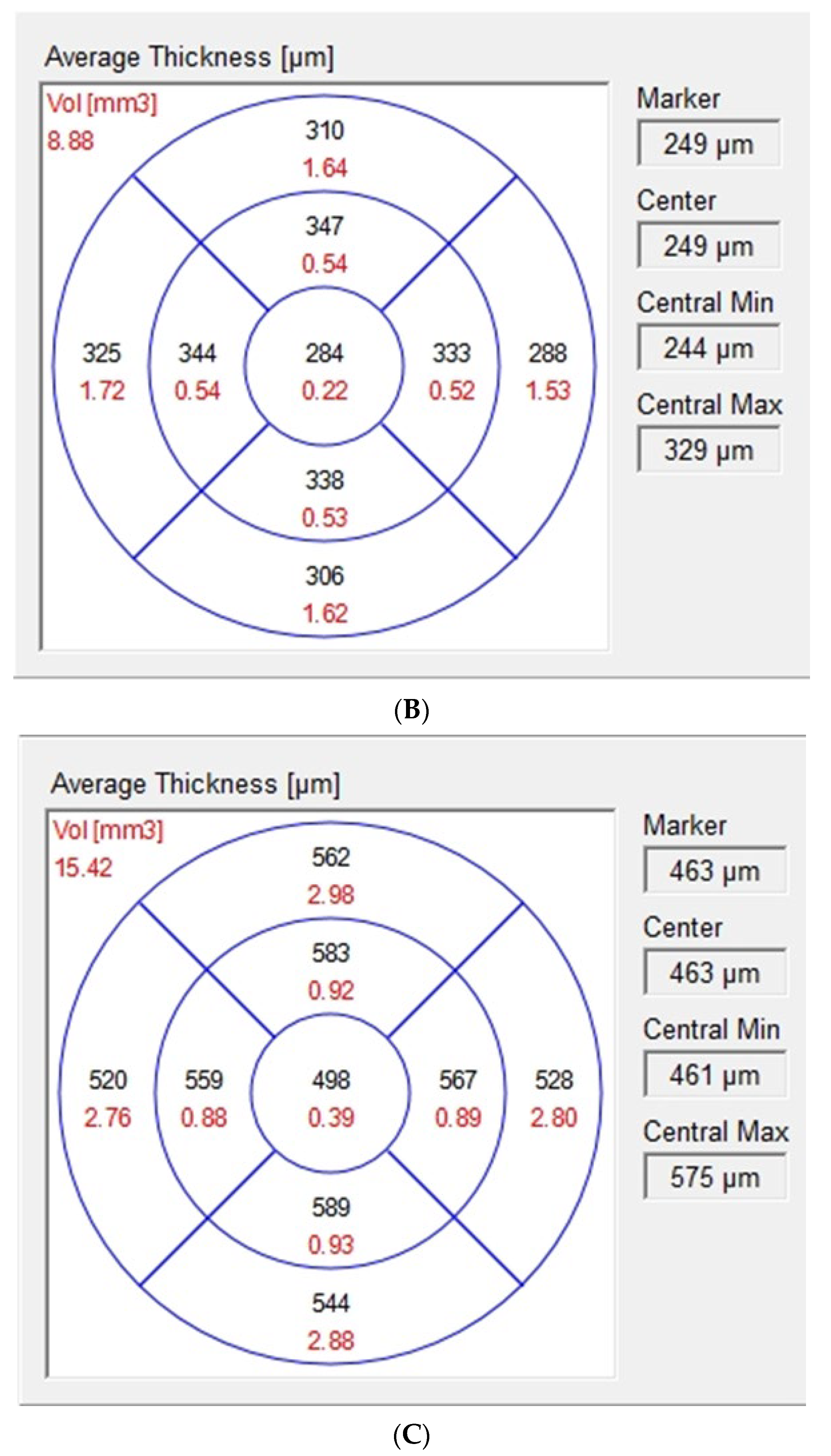
2.1. Optical Coherence Tomography Images Acquisition and Analysis
2.2. Binarization of Subfoveal Choroidal Images
2.3. Fluorescein Angiograms Acquisition and Analysis
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Between-Group Comparison of Outer Retinal and Choroidal Parameters
3.3. Intra-Group Correlations and Regressions between Outer Retinal and Choroidal Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Linsenmeier, R.A.; Padnick-Silver, L. Metabolic dependence of photoreceptors on the choroid in the normal and detached retina. Investig. Ophthalmol. Vis. Sci. 2000, 41, 3117–3123. [Google Scholar]
- Scarinci, F.; Nesper, P.L.; Fawzi, A.A. Deep Retinal Capillary Nonperfusion Is Associated with Photoreceptor Disruption in Diabetic Macular Ischemia. Am. J. Ophthalmol. 2016, 168, 129–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, J.; McLeod, S.; Merges, C.A.; Lutty, G.A. Choriocapillaris degeneration and related pathologic changes in human diabetic eyes. Arch. Ophthalmol. 1998, 116, 589–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parravano, M.; Ziccardi, L.; Borrelli, E.; Costanzo, E.; Frontoni, S.; Picconi, F.; Parisi, V.; Sacconi, R.; Di Renzo, A.; Varano, M.; et al. Outer retina dysfunction and choriocapillaris impairment in type 1 diabetes. Sci. Rep. 2021, 11, 15183. [Google Scholar] [CrossRef]
- Borrelli, E.; Palmieri, M.; Viggiano, P.; Ferro, G.; Mastropasqua, R. Photoreceptor damage in diabetic choroidopathy. Retina 2020, 40, 1062–1069. [Google Scholar] [CrossRef]
- Querques, G.; Lattanzio, R.; Querques, L.; Del Turco, C.; Forte, R.; Pierro, L.; Souied, E.H.; Bandello, F. Enhanced depth imaging optical coherence tomography in type 2 diabetes. Investig. Ophthalmol. Vis. Sci. 2012, 53, 6017–6024. [Google Scholar] [CrossRef] [Green Version]
- Maheshwary, A.S.; Oster, S.F.; Yuson, R.M.; Cheng, L.; Mojana, F.; Freeman, W.R. The association between percent disruption of the photoreceptor inner segment-outer segment junction and visual acuity in diabetic macular edema. Am. J. Ophthalmol. 2010, 150, 63–67.e1. [Google Scholar] [CrossRef] [Green Version]
- Alasil, T.; Keane, P.A.; Updike, J.F.; Dustin, L.; Ouyang, Y.; Walsh, A.C.; Sadda, S.R. Relationship between optical coherence tomography retinal parameters and visual acuity in diabetic macular edema. Ophthalmology 2010, 117, 2379–2386. [Google Scholar] [CrossRef]
- Otani, T.; Yamaguchi, Y.; Kishi, S. Correlation between visual acuity and foveal microstructural changes in diabetic macular edema. Retina 2010, 30, 774–780. [Google Scholar] [CrossRef]
- Murakami, T.; Nishijima, K.; Sakamoto, A.; Ota, M.; Horii, T.; Yoshimura, N. Association of pathomorphology, photoreceptor status, and retinal thickness with visual acuity in diabetic retinopathy. Am. J. Ophthalmol. 2011, 151, 310–317. [Google Scholar] [CrossRef]
- Wong, R.L.; Lee, J.W.; Yau, G.S.; Wong, I.Y. Relationship between Outer Retinal Layers Thickness and Visual Acuity in Diabetic Macular Edema. Biomed. Res. Int. 2015, 2015, 981471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sim, D.A.; Keane, P.A.; Fung, S.; Karampelas, M.; Sadda, S.R.; Fruttiger, M.; Patel, P.J.; Tufail, A.; Egan, C.A. Quantitative analysis of diabetic macular ischemia using optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2014, 55, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Kim, J.T.; Jung, D.W.; Joe, S.G.; Yoon, Y.H. The relationship between foveal ischemia and spectral-domain optical coherence tomography findings in ischemic diabetic macular edema. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1080–1085. [Google Scholar] [CrossRef] [Green Version]
- Yuodelis, C.; Hendrickson, A. A qualitative and quantitative analysis of the human fovea during development. Vision Res. 1986, 26, 847–855. [Google Scholar] [CrossRef]
- Forooghian, F.; Stetson, P.F.; Meyer, S.A.; Chew, E.Y.; Wong, W.T.; Cukras, C.; Meyerle, C.B.; Ferris, F.L. Relationship between photoreceptor outer segment length and visual acuity in diabetic macular edema. Retina 2010, 30, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Damian, I.; Nicoara, S.D. Optical Coherence Tomography Biomarkers of the Outer Blood-Retina Barrier in Patients with Diabetic Macular Oedema. J. Diabetes Res. 2020, 2020, 8880586. [Google Scholar] [CrossRef]
- Wang, X.N.; Li, S.T.; Li, W.; Hua, Y.J.; Wu, Q. The thickness and volume of the choroid, outer retinal layers and retinal pigment epithelium layer changes in patients with diabetic retinopathy. Int. J. Ophthalmol. 2018, 11, 1957–1962. [Google Scholar]
- Pelosini, L.; Hull, C.C.; Boyce, J.F.; McHugh, D.; Stanford, M.R.; Marshall, J. Optical coherence tomography may be used to predict visual acuity in patients with macular edema. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2741–2748. [Google Scholar] [CrossRef] [Green Version]
- Lutty, G.A. Diabetic choroidopathy. Vision Res. 2017, 139, 161–167. [Google Scholar] [CrossRef]
- Melancia, D.; Vicente, A.; Cunha, J.P.; Abegão Pinto, L.; Ferreira, J. Diabetic choroidopathy: A review of the current literature. Graefes. Arch. Clin. Exp. Ophthalmol. 2016, 254, 1453–1461. [Google Scholar] [CrossRef]
- Sun, Z.; Yang, D.; Tang, Z.; Ng, D.S.; Cheung, C.Y. Optical coherence tomography angiography in diabetic retinopathy: An updated review. Eye 2021, 35, 149–161. [Google Scholar] [CrossRef]
- Brinks, J.; van Dijk, E.H.C.; Klaassen, I.; Schlingemann, R.O.; Kielbasa, S.M.; Emri, E.; Quax, P.H.A.; Bergen, A.A.; Meijer, O.C.; Boon, C.J.F. Exploring the choroidal vascular labyrinth and its molecular and structural roles in health and disease. Prog. Retin. Eye Res. 2022, 87, 100994. [Google Scholar] [CrossRef] [PubMed]
- Sidorczuk, P.; Pieklarz, B.; Konopinska, J.; Saeed, E.; Mariak, Z.; Dmuchowska, D. Foveal avascular zone does not correspond to choroidal characteristics in patients with diabetic retinopathy: A single-center cross-sectional analysis. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 2893–2903. [Google Scholar] [CrossRef] [PubMed]
- Ţălu, Ş.; Nicoara, S.D. Malfunction of outer retinal barrier and choroid in the occurrence and progression of diabetic macular edema. World J. Diabetes 2021, 12, 437–452. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Moss, S.E.; Cruickshanks, K.J. The Wisconsin Epidemiologic Study of Diabetic Retinopathy: XVII. The 14-year incidence and progression of diabetic retinopathy and associated risk factors in type 1 diabetes. Ophthalmology 1998, 105, 1801–1815. [Google Scholar] [CrossRef]
- Daruich, A.; Matet, A.; Moulin, A.; Kowalczuk, L.; Nicolas, M.; Sellam, A.; Rotschild, P.-R.; Omri, S.; Gelize, E.; Jonet, L.; et al. Mechanisms of macular edema: Beyond the surface. Prog. Retin. Eye Res. 2018, 63, 20–68. [Google Scholar] [CrossRef]
- Xu, H.Z.; Le, Y.Z. Significance of outer blood-retina barrier breakdown in diabetes and ischemia. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2160–2164. [Google Scholar] [CrossRef]
- Rangasamy, S.; McGuire, P.G.; Franco Nitta, C.; Monickaraj, F.; Oruganti, S.R.; Das, A. Chemokine mediated monocyte trafficking into the retina: Role of inflammation in alteration of the blood-retinal barrier in diabetic retinopathy. PLoS ONE 2014, 9, e108508. [Google Scholar] [CrossRef]
- Marques, I.P.; Alves, D.; Santos, T.; Mendes, L.; Santos, A.R.; Lobo, C.; Durbin, M.; Cunha-Vaz, J. Multimodal Imaging of the Initial Stages of Diabetic Retinopathy: Different Disease Pathways in Different Patients. Diabetes 2019, 68, 648–653. [Google Scholar] [CrossRef] [Green Version]
- Murakami, T.; Yoshimura, N. Structural changes in individual retinal layers in diabetic macular edema. J. Diabetes Res 2013, 2013, 920713. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, R.; Ding, J.; Sen, P.; Rousselot, A.; Chan, A.; Nivison-Smith, L.; Wei, X.; Mahajan, S.; Kim, R.; Mishra, C.; et al. Exploring choroidal angioarchitecture in health and disease using choroidal vascularity index. Prog. Retin. Eye Res. 2020, 77, 100829. [Google Scholar] [CrossRef] [PubMed]
- Sonoda, S.; Sakamoto, T.; Yamashita, T.; Uchino, E.; Kawano, H.; Yoshihara, N.; Terasaki, H.; Shirasawa, M.; Tomita, M.; Ishibashi, T. Luminal and stromal areas of choroid determined by binarization method of optical coherence tomographic images. Am. J. Ophthalmol. 2015, 159, 1123–1131.e1. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Salman, M.; Tan, K.A.; Karampelas, M.; Sim, D.A.; Keane, P.A.; Pavesio, C. Choroidal Vascularity Index (CVI)--A Novel Optical Coherence Tomography Parameter for Monitoring Patients with Panuveitis? PLoS ONE 2016, 11, e0146344. [Google Scholar] [CrossRef] [PubMed]
- Campos, A.; Campos, E.J.; Martins, J.; Ambrósio, A.F.; Silva, R. Viewing the choroid: Where we stand, challenges and contradictions in diabetic retinopathy and diabetic macular oedema. Acta Ophthalmol. 2017, 95, 446–459. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.R.; Vupparaboina, K.K.; Goud, A.; Dansingani, K.K.; Chhablani, J. Choroidal imaging biomarkers. Surv. Ophthalmol. 2019, 64, 312–333. [Google Scholar] [CrossRef]
- Iovino, C.; Pellegrini, M.; Bernabei, F.; Borrelli, E.; Sacconi, R.; Govetto, A.; Vaggo, A.; Di Zazzo, A.; Forlini, M.; Finocchio, L.; et al. Choroidal Vascularity Index: An In-Depth Analysis of This Novel Optical Coherence Tomography Parameter. J. Clin. Med. 2020, 9, 595. [Google Scholar] [CrossRef] [Green Version]
- Esmaeelpour, M.; Považay, B.; Hermann, B.; Hofer, B.; Kajic, V.; Hale, S.L.; North, R.V.; Drexler, W.; Sheen, N.J.L. Mapping choroidal and retinal thickness variation in type 2 diabetes using three-dimensional 1060-nm optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2011, 52, 5311–5316. [Google Scholar] [CrossRef]
- Esmaeelpour, M.; Brunner, S.; Ansari-Shahrezaei, S.; Shahrezaei, S.A.; Nemetz, S.; Povazay, B.; Kajic, V.; Drexler, W.; Binder, S. Choroidal thinning in diabetes type 1 detected by 3-dimensional 1060 nm optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2012, 53, 6803–6809. [Google Scholar] [CrossRef] [Green Version]
- Endo, H.; Kase, S.; Takahashi, M.; Yokoi, M.; Isozaki, C.; Katsuta, S.; Kase, M. Alteration of layer thickness in the choroid of diabetic patients. Clin. Exp. Ophthalmol. 2018, 46, 926–933. [Google Scholar] [CrossRef]
- Tan, K.A.; Laude, A.; Yip, V.; Loo, E.; Wong, E.P.; Agrawal, R. Choroidal vascularity index—A novel optical coherence tomography parameter for disease monitoring in diabetes mellitus? Acta Ophthalmol. 2016, 94, e612–e616. [Google Scholar] [CrossRef]
- Kim, M.; Ha, M.J.; Choi, S.Y.; Park, Y.H. Choroidal vascularity index in type-2 diabetes analyzed by swept-source optical coherence tomography. Sci. Rep. 2018, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Gupta, C.; Tan, R.; Mishra, C.; Khandelwal, N.; Raman, R.; Kim, R.; Agrawal, R.; Sen, P. Choroidal structural analysis in eyes with diabetic retinopathy and diabetic macular edema-A novel OCT based imaging biomarker. PLoS ONE 2018, 13, e0207435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markan, A.; Agarwal, A.; Arora, A.; Bazgain, K.; Rana, V.; Gupta, V. Novel imaging biomarkers in diabetic retinopathy and diabetic macular edema. Ther. Adv. Ophthalmol. 2020, 12, 2515841420950513. [Google Scholar] [CrossRef] [PubMed]
- Ozkaya, A.; Alkin, Z.; Karakucuk, Y.; Karatas, G.; Fazil, K.; Gurkan Erdogan, M.; Parente, I.; Taskapili, M. Thickness of the retinal photoreceptor outer segment layer in healthy volunteers and in patients with diabetes mellitus without retinopathy, diabetic retinopathy, or diabetic macular edema. Saudi J. Ophthalmol. 2017, 31, 69–75. [Google Scholar] [CrossRef]
- Virgili, G.; Menchini, F.; Casazza, G.; Hogg, R.; Das, R.R.; Wang, X.; Michelessi, M. Optical coherence tomography (OCT) for detection of macular oedema in patients with diabetic retinopathy. Cochrane Database Syst. Rev. 2015, 1, CD008081. [Google Scholar] [CrossRef] [Green Version]
- Dmuchowska, D.A.; Sidorczuk, P.; Pieklarz, B.; Konopińska, J.; Mariak, Z.; Obuchowska, I. Quantitative Assessment of Choroidal Parameters in Patients with Various Types of Diabetic Macular Oedema: A Single-Centre Cross-Sectional Analysis. Biology 2021, 10, 725. [Google Scholar] [CrossRef]
- Sonoda, S.; Sakamoto, T.; Yamashita, T.; Shirasawa, M.; Uchino, E.; Terasaki, H.; Tomita, M. Choroidal structure in normal eyes and after photodynamic therapy determined by binarization of optical coherence tomographic images. Investig. Ophthalmol. Vis. Sci. 2014, 55, 3893–3899. [Google Scholar] [CrossRef]
- Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—An extension of the modified Airlie House classification. ETDRS report number 10. Ophthalmology 1991, 98 (Suppl. 5), 786–806. [Google Scholar] [CrossRef]
- Early Treatment Diabetic Retinopathy Study Research Group. Classification of diabetic retinopathy from fluorescein angiograms. ETDRS report number 11. Ophthalmology 1991, 98 (Suppl. 5), 807–822. [Google Scholar] [CrossRef]
- Heinze, G.; Dunkler, D. Five myths about variable selection. Transpl. Int. 2017, 30, 6–10. [Google Scholar] [CrossRef]
- Wang, W.; Liu, S.; Qiu, Z.; He, M.; Wang, L.; Li, Y.; Huang, W. Choroidal Thickness in Diabetes and Diabetic Retinopathy: A Swept Source OCT Study. Investig. Ophthalmol. Vis. Sci. 2020, 61, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietrowska, K.; Dmuchowska, D.A.; Krasnicki, P.; Bujalska, A.; Samczuk, P.; Parfieniuk, E.; Kowalczyk, T.; Wojnar, M.; Mariak, Z.; Kretowski, A.; et al. An exploratory LC-MS-based metabolomics study reveals differences in aqueous humor composition between diabetic and non-diabetic patients with cataract. Electrophoresis 2018, 39, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Krasnicki, P.; Dmuchowska, D.A.; Proniewska-Skretek, E.; Dobrzycki, S.; Mariak, Z. Ocular haemodynamics in patients with type 2 diabetes and coronary artery disease. Br. J. Ophthalmol. 2014, 98, 675–678. [Google Scholar] [CrossRef] [PubMed]
- Damian, I.; Roman, G.; Nicoară, S.D. Analysis of the Choroid and Its Relationship with the Outer Retina in Patients with Diabetes Mellitus Using Binarization Techniques Based on Spectral-Domain Optical Coherence Tomography. J. Clin. Med. 2021, 10, 210. [Google Scholar] [CrossRef]
- Karahan, E.; Zengin, M.O.; Tuncer, I. Correlation of choroidal thickness with outer and inner retinal layers. Ophthalmic Surg. Lasers Imaging Retin. 2013, 44, 544–548. [Google Scholar] [CrossRef]
- Gerendas, B.S.; Waldstein, S.M.; Simader, C.; Deak, G.; Hajnajeeb, B.; Zhang, L.; Bogunovic, H.; Abramoff, M.D.; Kundi, M.; Sonka, M.; et al. Three-dimensional automated choroidal volume assessment on standard spectral-domain optical coherence tomography and correlation with the level of diabetic macular edema. Am. J. Ophthalmol. 2014, 158, 1039–1048. [Google Scholar] [CrossRef] [Green Version]
- Marmor, M.F. Mechanisms of fluid accumulation in retinal edema. Doc. Ophthalmol. 1999, 97, 239–249. [Google Scholar] [CrossRef]
- Santos, A.R.; Santos, T.; Alves, D.; Marques, I.P.; Lobo, C.; Cunha-Vaz, J. Characterization of Initial Stages of Diabetic Macular Edema. Ophthalmic Res. 2019, 62, 203–210. [Google Scholar] [CrossRef]
- Cunha-Vaz, J.; Ribeiro, L.; Lobo, C. Phenotypes and biomarkers of diabetic retinopathy. Prog. Retin. Eye Res. 2014, 41, 90–111. [Google Scholar] [CrossRef]
- Dmuchowska, D.A.; Krasnicki, P.; Mariak, Z. Can optical coherence tomography replace fluorescein angiography in detection of ischemic diabetic maculopathy? Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 731–738. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Overall | Group | p | |||
|---|---|---|---|---|---|
| DR + DME+ | DR + DME− | Controls | |||
| Number of patients | 191 | 49 | 90 | 52 | |
| Number of eyes | 286 | 76 | 134 | 76 | |
| Age, years, mean ± SD | 59.24 ± 14.43 | 61.50 ± 11.92 | 60.03 ± 13.19 | 55.73 ± 17.87 | 0.103 |
| Sex, female, n (%) | 100 (52.4) | 25 (51.0) | 47 (52.2) | 28 (53.8) | 0.960 |
| Spherical equivalent, mean ± SD | 0.32 ± 1.10 | 0.43 ± 1.07 | 0.23 ± 0.99 | 0.39 ± 1.28 | 0.371 |
| DR severity, n (%) | |||||
| NPDR | 135 (47.2) | 50 (65.8) | 85 (63.4) | - | 0.766 1 |
| PDR | 75 (26.2) | 26 (34.2) | 49 (36.6) | - | |
| PRP, n (%) | |||||
| No | 138 (48.3) | 48 (63.2) | 90 (67.2) | - | 0.650 1 |
| Yes | 72 (25.2) | 28 (36.8) | 44 (32.8) | - | |
| DR + DME+ | DR + DME− | Controls | p | Post Hoc | |||
|---|---|---|---|---|---|---|---|
| DR + DME+ vs. DR + DME− | DR + DME− vs. Controls | DR + DME+ vs. Controls | |||||
| Choroidal parameters | |||||||
| CVI | 0.62 ± 0.05 | 0.63 ± 0.05 | 0.65 ± 0.05 | 0.001 | 0.576 | 0.089 | <0.001 |
| LA (mm2) | 0.24 ± 0.05 | 0.25 ± 0.08 | 0.25 ± 0.06 | 0.266 | |||
| SCA (mm2) | 0.15 ± 0.03 | 0.14 ± 0.04 | 0.14 ± 0.03 | 0.204 | |||
| TCA (mm2) | 0.39 ± 0.08 | 0.40 ± 0.01 | 0.39 ± 0.08 | 0.773 | |||
| Choroid (µm) | 250.75 ± 45.61 | 265.34 ± 60.91 | 303.64 ± 72.77 | <0.001 | 0.218 | <0.001 | <0.001 |
| Central macular thickness (1 mm diameter) | |||||||
| ORL (µm) | 92.58 ± 24.10 | 84.20 ± 4.97 | 87.64 ± 3.52 | <0.001 | <0.001 | 0.157 | 0.052 |
| ONL (µm) | 141.70 ± 85.70 | 82.38 ± 18.03 | 92.13 ± 10.81 | <0.001 | <0.001 | 0.306 | <0.001 |
| Correlation: | DR + DME+ | DR + DME− | Controls | |||
|---|---|---|---|---|---|---|
| Rho | p | Rho | p | Rho | p | |
| ORL central macular thickness (1 mm diameter) | ||||||
| Choroidal central macular thickness (µm) | 0.23 | 0.160 | 0.34 | 0.003 | 0.27 | 0.069 |
| CVI | −0.01 | 0.953 | 0.49 | <0.001 | 0.12 | 0.426 |
| LA (mm2) | 0.23 | 0.171 | 0.41 | <0.001 | 0.19 | 0.191 |
| SA (mm2) | 0.17 | 0.314 | 0.12 | 0.293 | 0.05 | 0.719 |
| TCA (mm2) | 0.18 | 0.285 | 0.32 | 0.005 | 0.17 | 0.242 |
| ONL central macular thickness (1 mm diameter) | ||||||
| Choroidal central macular thickness (µm) | −0.07 | 0.683 | 0.01 | 0.932 | −0.27 | 0.058 |
| CVI | 0.35 | 0.031 | 0.25 | 0.027 | 0.14 | 0.336 |
| LA (mm2) | 0.08 | 0.641 | 0.09 | 0.430 | −0.02 | 0.871 |
| SA (mm2) | −0.22 | 0.191 | −0.20 | 0.077 | −0.16 | 0.289 |
| TCA (mm2) | −0.03 | 0.856 | −0.01 | 0.981 | −0.09 | 0.558 |
| ORL Central Macular Thickness (1 mm Diameter) | ONL Central Macular Thickness (1 mm Diameter) | |||||||
|---|---|---|---|---|---|---|---|---|
| β | SE | p | R2/R2 adj. | β | SE | p | R2/R2 adj. | |
| Choroidal central macular thickness (µm) | 0.03 | 0.01 | 0.019 | 0.14/0.08 | 0.03 | 0.04 | 0.395 | 0.23/0.18 |
| CVI | 43.70 | 9.93 | <0.001 | 0.26/0.21 | 67.03 | 36.32 | 0.069 | 0.26/0.21 |
| LA (mm2) | 18.73 | 6.22 | 0.004 | 0.17/0.11 | 7.94 | 21.92 | 0.718 | 0.23/0.17 |
| SA (mm2) | 12.29 | 12.54 | 0.330 | −34.52 | 41.74 | 0.411 | 0.23/0.18 | |
| TCA (mm2) | 10.20 | 4.32 | 0.021 | 0.13/0.07 | −0.70 | 14.91 | 0.963 | 0.23/0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sidorczuk, P.; Obuchowska, I.; Konopinska, J.; Dmuchowska, D.A. Correlation between Choroidal Vascularity Index and Outer Retina in Patients with Diabetic Retinopathy. J. Clin. Med. 2022, 11, 3882. https://doi.org/10.3390/jcm11133882
Sidorczuk P, Obuchowska I, Konopinska J, Dmuchowska DA. Correlation between Choroidal Vascularity Index and Outer Retina in Patients with Diabetic Retinopathy. Journal of Clinical Medicine. 2022; 11(13):3882. https://doi.org/10.3390/jcm11133882
Chicago/Turabian StyleSidorczuk, Patryk, Iwona Obuchowska, Joanna Konopinska, and Diana A. Dmuchowska. 2022. "Correlation between Choroidal Vascularity Index and Outer Retina in Patients with Diabetic Retinopathy" Journal of Clinical Medicine 11, no. 13: 3882. https://doi.org/10.3390/jcm11133882