
Large Amplitude Iris Fluttering Detected by Consecutive Anterior Segment Optical Coherence Tomography Images in Eyes with Intrascleral Fixation of an Intraocular Lens


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement of Iris Flutter by Anterior Segment Optical Coherence Tomography (AS-OCT)
2.3. Surgical Procedures
2.4. Statistical Analyses
3. Results
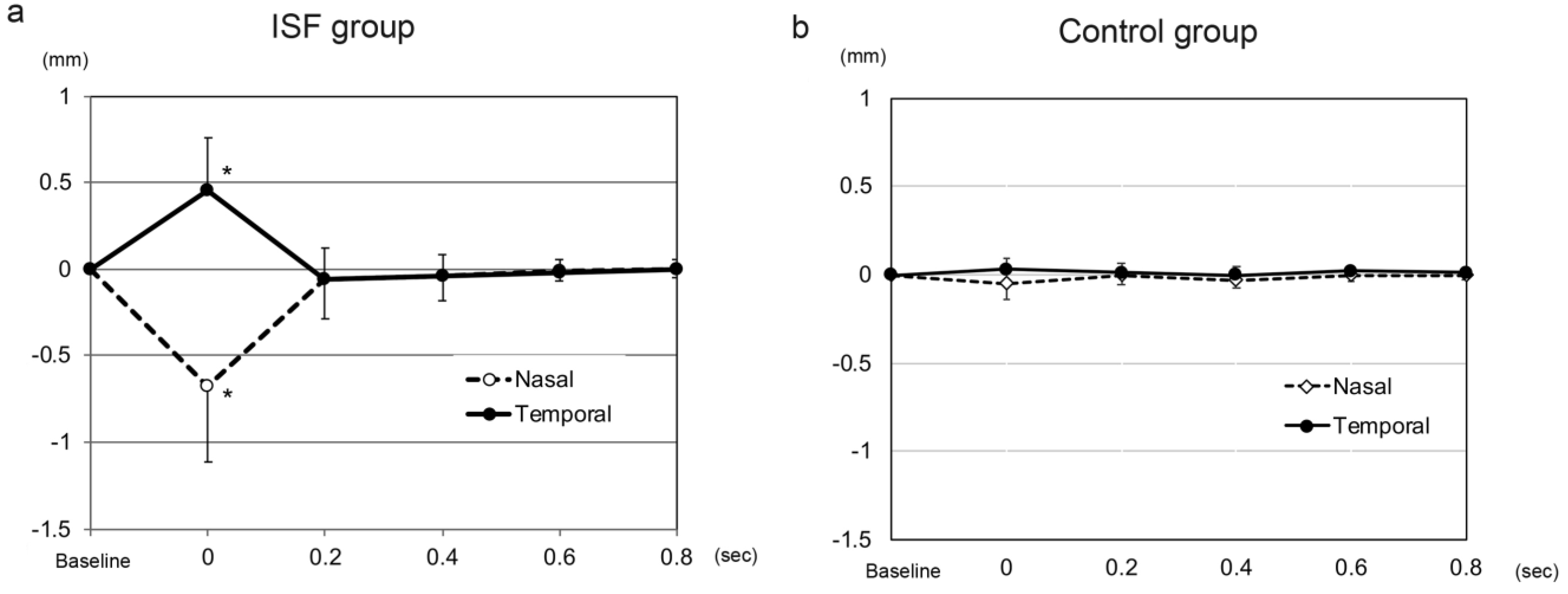
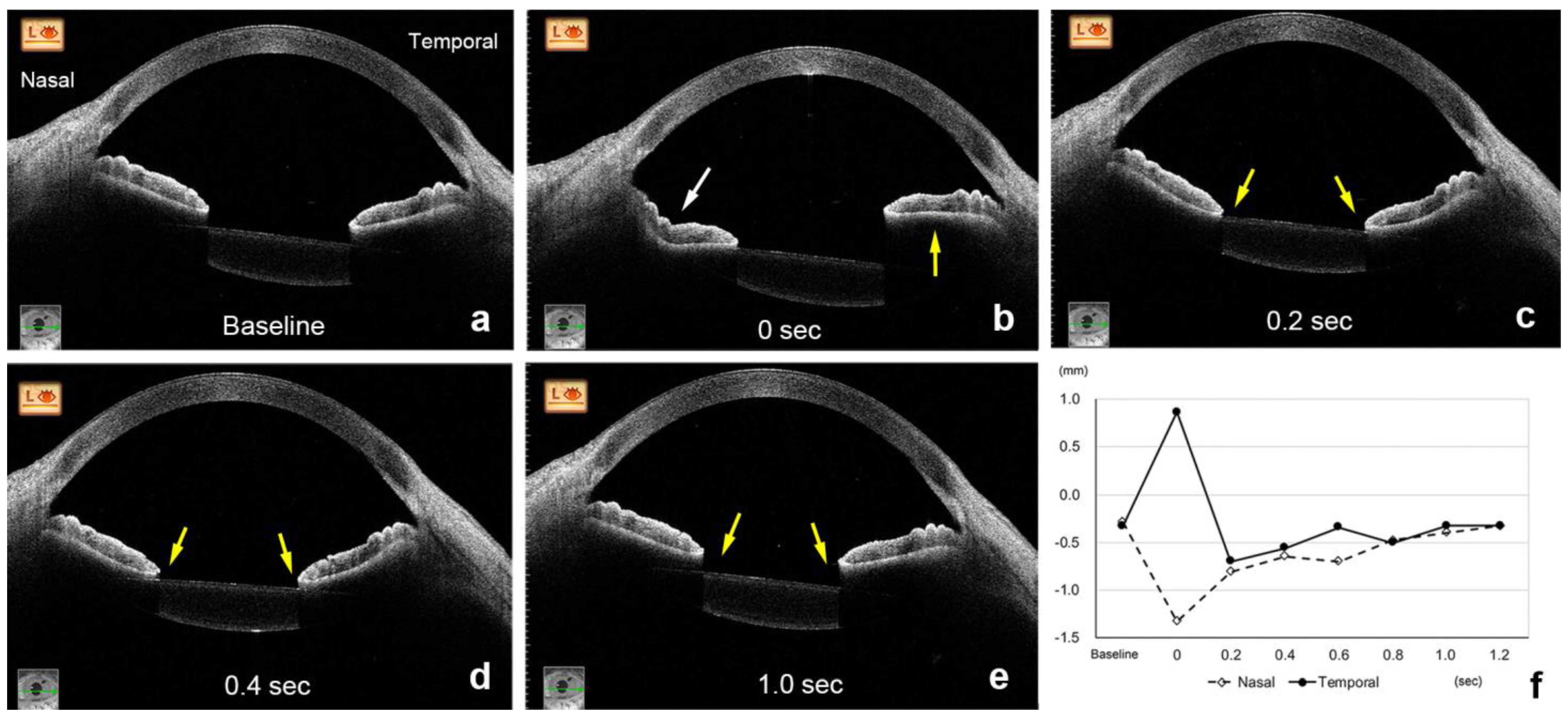
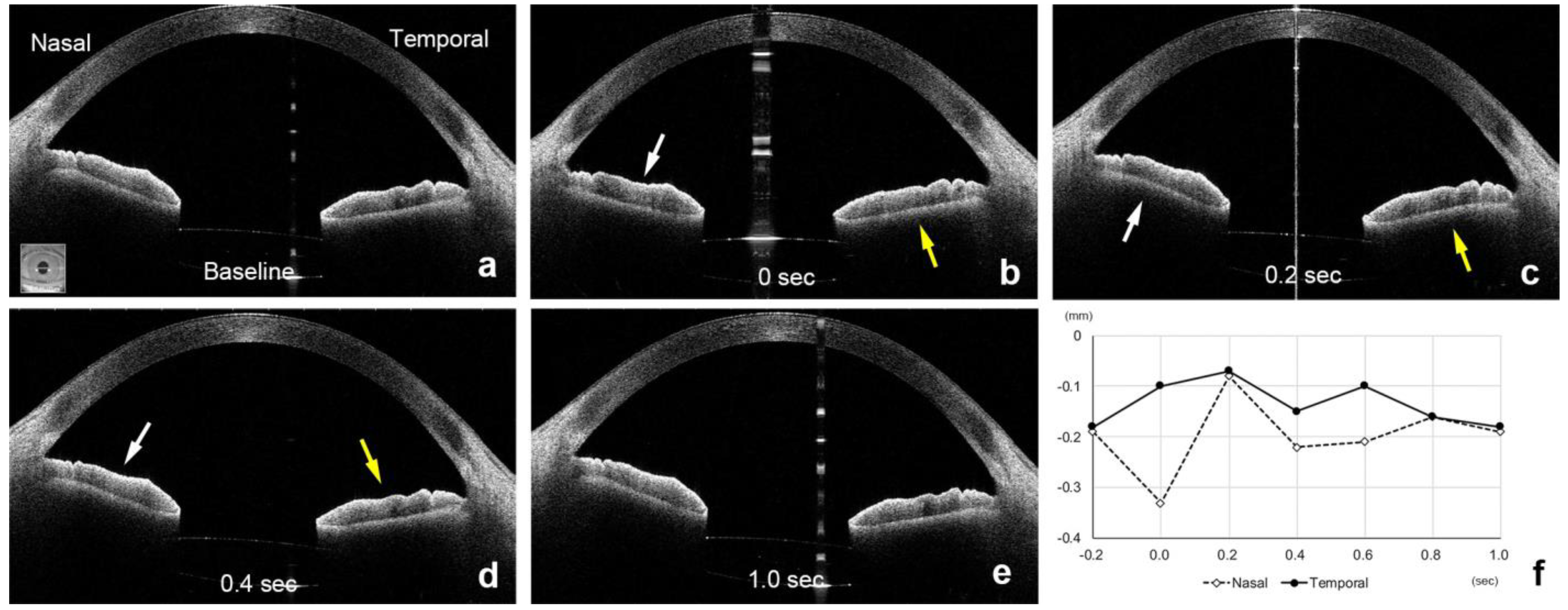
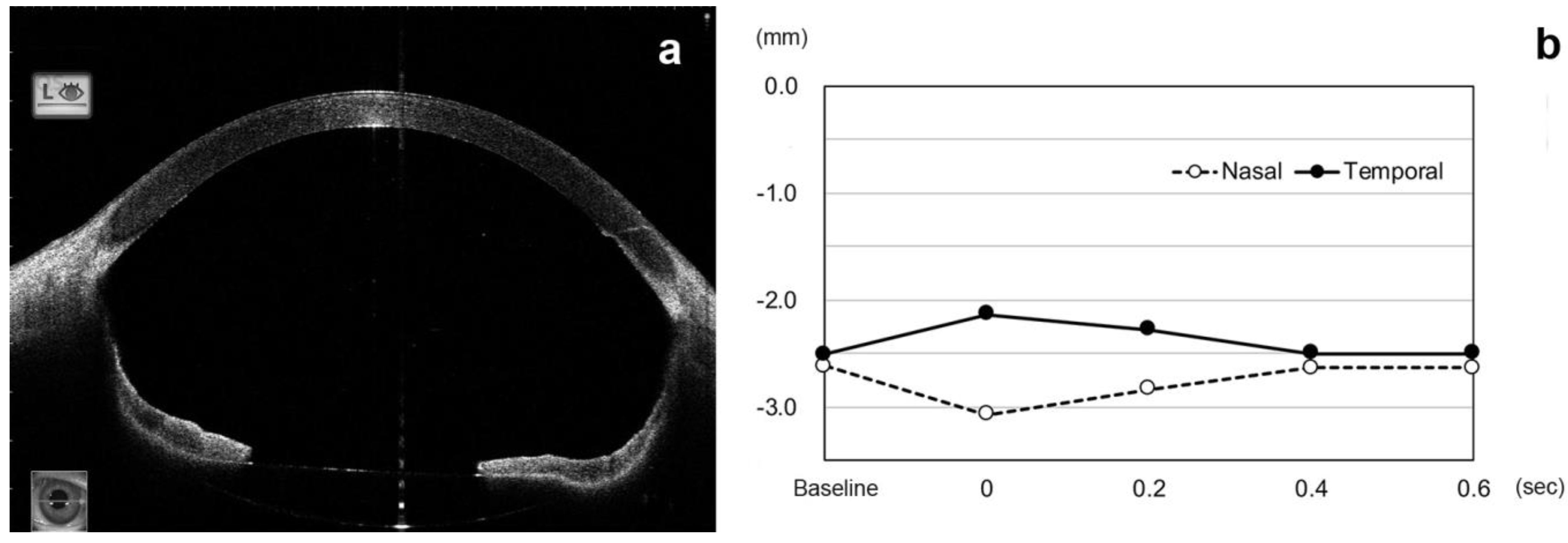
3.1. Time Course of Changes in Height of Temporal and Nasal Sectors of Iris after an Eye Movement
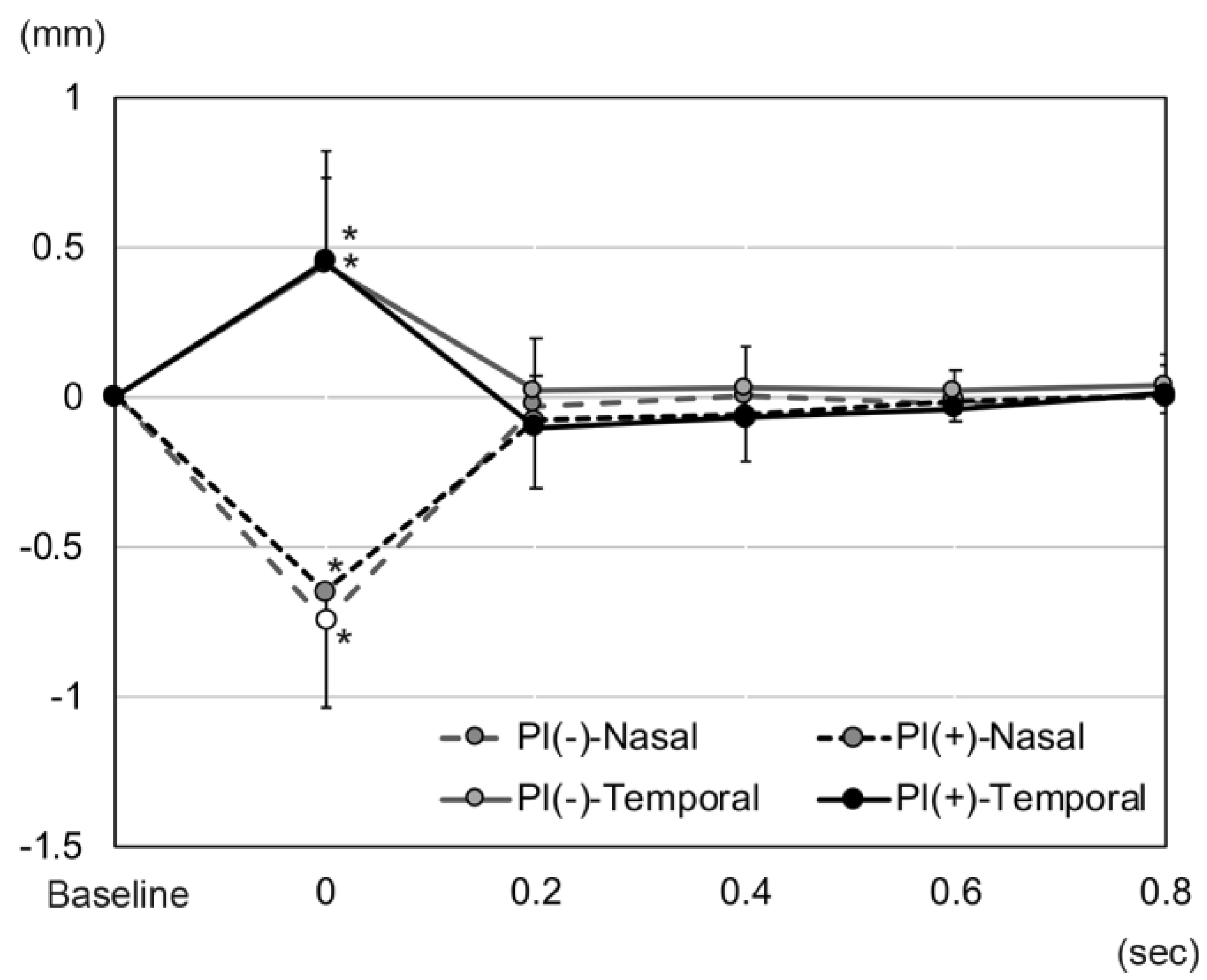
3.2. Changes in Iris Height in Eyes with and without Peripheral Iridectomy (PI)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wagoner, M.D.; Cox, T.A.; Ariyasu, R.G.; Jacobs, D.S.; Karp, C.L.; American Academy of Ophthalmology. Intraocular lens implantation in the absence of capsular support: A report by the American Academy of Ophthalmology. Ophthalmology 2003, 110, 840–859. [Google Scholar] [CrossRef]
- Monteiro, M.; Marinho, A.; Borges, S.; Ribeiro, L.; Correia, C. Scleral fixation in eyes with loss of capsule or zonule support. J. Cataract Refract. Surg. 2007, 33, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Vote, B.J.; Tranos, P.; Bunce, C.; Charteris, D.G.; Da Cruz, L. Long-term outcome of combined pars plana vitrectomy and scleral fixated sutured posterior chamber intraocular lens implantation. Am. J. Ophthalmol. 2006, 141, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Gabor, S.G.; Pavlidis, M.M. Sutureless intrascleral posterior chamber intraocular lens fixation. J. Cataract Refract. Surg. 2007, 33, 1851–1854. [Google Scholar] [CrossRef] [PubMed]
- Scharioth, G.B.; Prasad, S.; Georgalas, I.; Tatarum, C.; Pavlidism, M. Intermediate results of sutureless intrascleral posterior chamber intraocular lens fixation. J. Cataract Refract. Surg. 2010, 36, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Ohta, T.; Toshida, H.; Murakami, A. Simplified and safe method of sutureless intrascleral posterior chamber intraocular lens fixation: Y-fixation technique. J. Cataract Refract. Surg. 2014, 40, 2–7. [Google Scholar] [CrossRef]
- Yamane, S.; Inoue, M.; Arakawa, A.; Kadonosono, K. Sutureless 27-gauge needle-guided intrascleral intraocular lens implantation with lamellar scleral dissection. Ophthalmology 2014, 121, 61–66. [Google Scholar] [CrossRef]
- Yamane, S.; Sato, S.; Maruyama-Inoue, M.; Kadonosono, K. Flanged Intrascleral Intraocular Lens Fixation with Double-Needle Technique. Ophthalmology 2017, 124, 1136–1142. [Google Scholar] [CrossRef]
- Kujime, Y.; Akimoto, M. Repair of angle recession prevents pupillary capture of intrasclerally fixed intraocular lenses. Int. Ophthalmol. 2019, 39, 1163–1168. [Google Scholar] [CrossRef]
- Bang, S.P.; Joo, C.K.; Jun, J.H. Reverse pupillary block after implantation of a scleral-sutured posterior chamber intraocular lens: A retrospective, open study. BMC Ophthalmol. 2017, 17, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.I.; Kim, K. Tram-Track Suture Technique for Pupillary Capture of a Scleral Fixated Intraocular Lens. Case Rep. Ophthalmol. 2016, 7, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Higashide, T.; Shimizu, F.; Nishimura, A.; Sugiyama, K. Anterior segment optical coherence tomography findings of reverse pupillary block after scleral-fixated sutured posterior chamber intraocular lens implantation. J. Cataract Refract. Surg. 2009, 35, 1540–1547. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.F.; Pimenta, F.; Alves, M.A.; Oliveira, M.S.N. Flow dynamics of vitreous humour during saccadic eye movements. J. Mech. Behav. Biomed. Mater. 2020, 110, 103860. [Google Scholar] [CrossRef] [PubMed]
- Abouali, O.; Modareszadeh, A.; Ghaffariyeh, A.; Tu, J. Numerical simulation of the fluid dynamics in vitreous cavity due to saccadic eye movement. Med. Eng. Phys. 2012, 34, 681–692. [Google Scholar] [CrossRef]
- Abouali, O.; Modareszadeh, A.; Ghaffarieh, A.; Tu, J. Investigation of saccadic eye movement effects on the fluid dynamic in the anterior chamber. J. Biomech. Eng. 2012, 134, 021002. [Google Scholar] [CrossRef]
- Modarreszadeh, S.; Abouali, O.; Ghaffariehm, A.; Ahmadim, G. Physiology of aqueous humor dynamic in the anterior chamber due to rapid eye movement. Physiol. Behav. 2014, 135, 112–118. [Google Scholar] [CrossRef]
- Fitt, A.D.; Gonzalez, G. Fluid Mechanics of the Human Eye: Aqueous Humour Flow in The Anterior Chamber. Bull. Math. Biol. 2006, 68, 53–71. [Google Scholar] [CrossRef]
- Radhakrishnan, S.; Yarovoy, D. Development in anterior segment imaging for glaucoma. Curr. Opin. Ophthalmol. 2014, 25, 98–103. [Google Scholar] [CrossRef]
- Angmo, D.; Nongpiur, M.E.; Sharma, R.; Sidhu, T.; Sihota, R.; Dada, T. Clinical utility of anterior segment swept-source optical coherence tomography in glaucoma. Oman J. Ophthalmol. 2016, 9, 3–10. [Google Scholar] [CrossRef]
- Zarei, M.; KhaliliPour, E.; Ebrahimiadib, N.; Riazi-Esfahani, H. Quantitative Analysis of the Iris Surface Smoothness by Anterior Segment Optical Coherence Tomography in Fuchs Uveitis. Ocul. Immunol. Inflamm. 2022, 30, 697–702. [Google Scholar] [CrossRef]
- Zarei, M.; Mahmoudi, T.; Riazi-Esfahani, H.; Mousavi, B.; Ebrahimiadib, N.; Yaseri, M.; Khalili Pour, E.; Arabalibeik, H. Automated measurement of iris surface smoothness using anterior segment optical coherence tomography. Sci. Rep. 2021, 11, 8505. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Wang, K.; Zhang, X.; Xing, X. Biometric indicators of anterior segment parameters before and after laser peripheral iridotomy by swept-source optical coherent tomography. BMC. Ophthalmol. 2022, 22, 222. [Google Scholar] [CrossRef] [PubMed]
- Ikegawa, W.; Suzuki, T.; Namiguchi, K.; Mizoue, S.; Shiraishi, A.; Ohashi, Y. Changes in Anterior Segment Morphology of Iris Bombe before and after Laser Peripheral Iridotomy in Patients with Uveitic Secondary Glaucoma. J. Ophthalmol. 2016, 2016, 8496201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panda, S.K.; Tan, R.K.Y.; Tun, T.A.; Buist, M.L.; Nongpiur, M.; Baskaran, M.; Aung, T.; Girard, M.J.A. Changes in Iris Stiffness and Permeability in Primary Angle Closure Glaucoma. Investig. Ophthalmol. Vis. Sci. 2021, 62, 29. [Google Scholar] [CrossRef]
- Ye, S.; Bao, C.; Chen, Y.; Shen, M.; Lu, F.; Zhang, S.; Zhu, D. Identification of Peripheral Anterior Synechia by Corneal Deformation Using Air-Puff Dynamic Anterior Segment Optical Coherence Tomography. Front. Bioeng. Biotechnol. 2022, 10, 856531. [Google Scholar] [CrossRef]
- Khodabande, A.; Mohammadi, M.; Riazi-Esfahani, H.; Karami, S.; Mirghorbani, M.; Modjtahedi, B.S. Changes in anterior segment optical coherence tomography following pars plana vitrectomy without tamponade. Int. J. Retin. Vitr. 2021, 7, 15. [Google Scholar] [CrossRef]
- Singh, H.; Modabber, M.; Safran, S.G.; Ahmed, I.I. Laser iridotomy to treat uveitis-glaucoma-hyphema syndrome secondary to reverse pupillary block in sulcus-placed intraocular lenses: Case series. J. Cataract Refract. Surg. 2015, 41, 2215–2223. [Google Scholar] [CrossRef]
- Bharathi, M.; Balakrishnan, D.; Senthil, S. “Pseudophakic Reverse Pupillary Block” Following Yamane Technique Scleral-fixated Intraocular Lens. J. Glaucoma 2020, 29, e68–e70. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ISF | Control | p-Value | |
|---|---|---|---|
| Eyes | 29 | 15 | |
| Age | 66.2 ± 17.7 | 65.1 ± 8.0 | 0.435 * |
| Sex (M/W) | 22/7 | 7/8 | 0.056 ** |
| Laterality (R/L) | 14/15 | 9/6 | 0.338 ** |
| Axial length (mm) | 25.32 ± 1.73 | 24.75 ± 2.05 | 0.202 * |
| Nasal height of iris (mm) | −0.20 ± 0.16 | −0.06 ± 0.17 | 0.007 * |
| Temporal height of iris (mm) | −0.23 ± 0.13 | −0.08 ± 0.16 | 0.006 * |
| ACD (mm) | 5.82 ± 0.58 | 5.25 ± 0.31 | <0.001 * |
| Peripheral iridectomy | 20 | 0 |
| PI (+) | PI (−) | p-Value | |
|---|---|---|---|
| Eyes | 20 | 9 | - |
| Age | 66.9 ± 18.9 | 64.6 ± 15.4 | 0.594 * |
| Sex (M/W) | 15/5 | 7/2 | 0.631 ** |
| Laterality (R/L) | 11/9 | 3/6 | 0.250 ** |
| Axial length (mm) | 25.52 ± 1.82 | 24.87 ± 1.48 | 0.390 * |
| Nasal height of iris (mm) | −0.24 ± 0.13 | −0.14 ± 0.20 | 0.317 * |
| Temporal height of iris (mm) | −0.25 ± 0.11 | −0.17 ± 0.15 | 0.116 * |
| ACD (mm) | 5.67 ± 0.46 | 6.17 ± 0.69 | 0.030 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, M.; Koto, T.; Hirakata, A. Large Amplitude Iris Fluttering Detected by Consecutive Anterior Segment Optical Coherence Tomography Images in Eyes with Intrascleral Fixation of an Intraocular Lens. J. Clin. Med. 2022, 11, 4596. https://doi.org/10.3390/jcm11154596
Inoue M, Koto T, Hirakata A. Large Amplitude Iris Fluttering Detected by Consecutive Anterior Segment Optical Coherence Tomography Images in Eyes with Intrascleral Fixation of an Intraocular Lens. Journal of Clinical Medicine. 2022; 11(15):4596. https://doi.org/10.3390/jcm11154596
Chicago/Turabian StyleInoue, Makoto, Takashi Koto, and Akito Hirakata. 2022. "Large Amplitude Iris Fluttering Detected by Consecutive Anterior Segment Optical Coherence Tomography Images in Eyes with Intrascleral Fixation of an Intraocular Lens" Journal of Clinical Medicine 11, no. 15: 4596. https://doi.org/10.3390/jcm11154596