1. Introduction
With a worldwide prevalence of approximately 500 million people affected, glucose-6-phosphate-dehydrogenase (G6PD) deficiency is an inherited enzymatic disorder causing hemolytic anemia [
1].
G6PD is a ubiquitous cytoplasmatic enzyme implicated in the regulation of carbon flow through the pentose phosphate pathway, essential for cell protection against oxidative stress. G6PD plays a crucial role in the conversion of glucose-6-phosphate into 6-phosphogluconate, a biochemical reaction associated with the simultaneous synthesis of reduced nicotinamide adenine dinucleotide phosphate (NADPH), essential for the proper functioning of glutathione reductase, an enzyme that transforms glutathione disulfide (GSSG) into reduced glutathione (GSH) [
2,
3]. Hemizygous males have uniformly deficient erythrocytes, whereas heterozygous females have mosaic populations of G6PD-deficient and normal red blood cells because of random inactivation of the X chromosome.
In red blood cells, NADPH production and, therefore, protection against oxidative stress are strongly related to G6PD activity [
2]. Consequently, in G6PD-deficient patients, the ingestion of agents with oxidant properties, such as broad bean (
Vicia faba) or some drugs (e.g., quinine derivatives, sulphonamides, and several anti-inflammatory agents), may trigger a decreased availability of GSH that may cause oxidation of hemoglobin and peroxidation of membrane lipids, thus leading to erythrocyte lysis and jaundice, which are typical clinical manifestations of hemolytic anemia [
4].
In Sardinia (Italy), a major Mediterranean island, G6PD deficiency represents a real public health issue, since over 10% of the population shows the G6PD-deficient genotype [
4].
It has been supposed that the high prevalence of this inherited enzymopathy may derive from the natural selection induced by Plasmodium falciparum malaria, endemic in Sardinia until the 1950s. In fact, G6PD deficiency, associated with increased oxidative stress in red blood cells, impairs plasmodium growth, offering protection against the development of severe malaria [
5].
Previous studies have highlighted that G6PD deficiency seems also to be associated with a decreased risk of developing several systemic and ophthalmological conditions, including cardiovascular and cerebrovascular diseases, colorectal cancer, retinal vein occlusion (RVO), and nonarteritic anterior ischemic optic neuropathy (NA-AION) [
2,
4,
6,
7]. G6PD deficiency also shows a trend for protection against severe proliferative diabetic retinopathy (PDR) [
8]. Although some hypotheses have been proposed, how exactly G6PD deficiency may be involved in protecting against the occurrence of RVO, NA-AION, and perhaps severe PDR is still not known [
4].
The retina is a highly metabolic tissue requiring tight regulation of blood perfusion and redox homeostasis for normal functioning. Cumulative oxidative stress causes damage to the retinal microvasculature and ganglion cells. Evidence from animal models indicates that endothelial Nox2, an NADPH-dependent enzyme, contributes to age-related capillary rarefaction in nervous tissue by increasing the production of reactive oxygen species [
9]. Theoretically, G6PD deficiency, characterized by decreased NADPH production and, consequently, Nox2 activity, might be associated with a better capillary network.
In the past, our knowledge and understanding of the pathophysiological mechanisms underlying retinal vascular diseases were limited to traditional angiography, an invasive imaging technique allowing only a two-dimensional en-face analysis of the retinal vasculature [
10]. The recent introduction of optical coherence tomography angiography (OCTA) in clinical practice has revolutionized our approach to retinal and optic nerve head (ONH) assessment [
11]. Indeed, this novel imaging technique generates high-resolution images of retinal and ONH plexuses [
11,
12]. Specifically, OCTA has made possible the detailed in vivo visualization of the radial peripapillary capillary (RPC) plexus, which is not feasible with traditional imaging techniques [
11,
13].
Recent research has focused on the RPC plexus, which plays a crucial role in the nourishment of retinal ganglion cells and, as a result, is involved in the pathogenesis of several retinal disorders [
14,
15,
16]. The embedded OCTA software, by automatically providing quantitative parameters (e.g., vascular density [VD]), allows for the objective evaluation of the blood flow and circulation in the RPC plexus, opening new areas of interesting research [
16].
The number of studies assessing the RPC plexus of the ONH is limited [
13]. Furthermore, we are unaware of any previous published report investigating the RPC plexus in G6PD-deficient patients. Therefore, the aim of the present study was to determine the VD values of the RPC plexus in G6PD-deficient and G6PD-normal patients and ascertain whether, or not, there were significant differences in terms of peripapillary microvascular changes between the two study groups.
2. Materials and Methods
This was a case–control study, enrolling 46 consecutive G6PD-deficient men and 23 apparently healthy G6PD-normal male controls, who were examined at the Ophthalmology Unit, Department of Medical, Surgical, and Experimental Sciences, University of Sassari, Sassari, Italy, from January to June 2017. Women were excluded due to the small number of homozygote subjects with a total lack of erythrocyte G6PD activity.
This observational study was performed according to the tenets of the Declaration of Helsinki for research involving human subjects. Institutional ethics review board approval was obtained. Each participant was given detailed information and provided written consent before inclusion.
The inclusion criteria for cases were male gender, G6PD deficiency, clear ocular media, and intra-ocular pressure (IOP) <20 mm Hg. Exclusion criteria included a history of ocular trauma, retinal and optic disc disease, uveitis, high myopia (≥6 diopters), intraocular surgery (apart from phacoemulsification performed at least 6 months before the study entry), diabetes mellitus, thalassemia trait, and kidney failure.
Apart from the presence of normal G6PD activity, the inclusion and exclusion criteria for the controls were the same as those for the cases.
Blood samples were collected from each participant. Erythrocyte G6PD activity was analyzed using a quantitative assay (G6PD/6PGD, Biomedic snc, Sassari, Italy), as described previously [
4].
All participants underwent a full ophthalmological examination and optic disc imaging. This included measurement of best-corrected visual acuity (BCVA), slit-lamp biomicroscopy with dilated indirect ophthalmoscopy, Goldmann applanation tonometry, B-scan OCT (Topcon OCT-2000), and OCTA (AngioVue XRTVue Avanti, Optovue, Fremont, CA, USA).
The OCTA scanning area was centered on the ONH. The AngioVue disc mode automatically segmented the ONH into four layers: ONH, vitreous, RPC plexus, and choroid. We assessed 4.5 × 4.5 mm OCTA scans of the RPC plexus, which extended from the inner limiting membrane (ILM) to 100 µm under the ILM, which we set as the lower boundary.
Each scan was reviewed to confirm the correct segmentation and sufficient image quality, as confirmed by the signal strength index (>55), and was repeated when necessary.
Furthermore, VD values of the RPC plexus, provided using the AngioAnalytics software embedded in the OCTA device, were recorded and compared with those of healthy eyes.
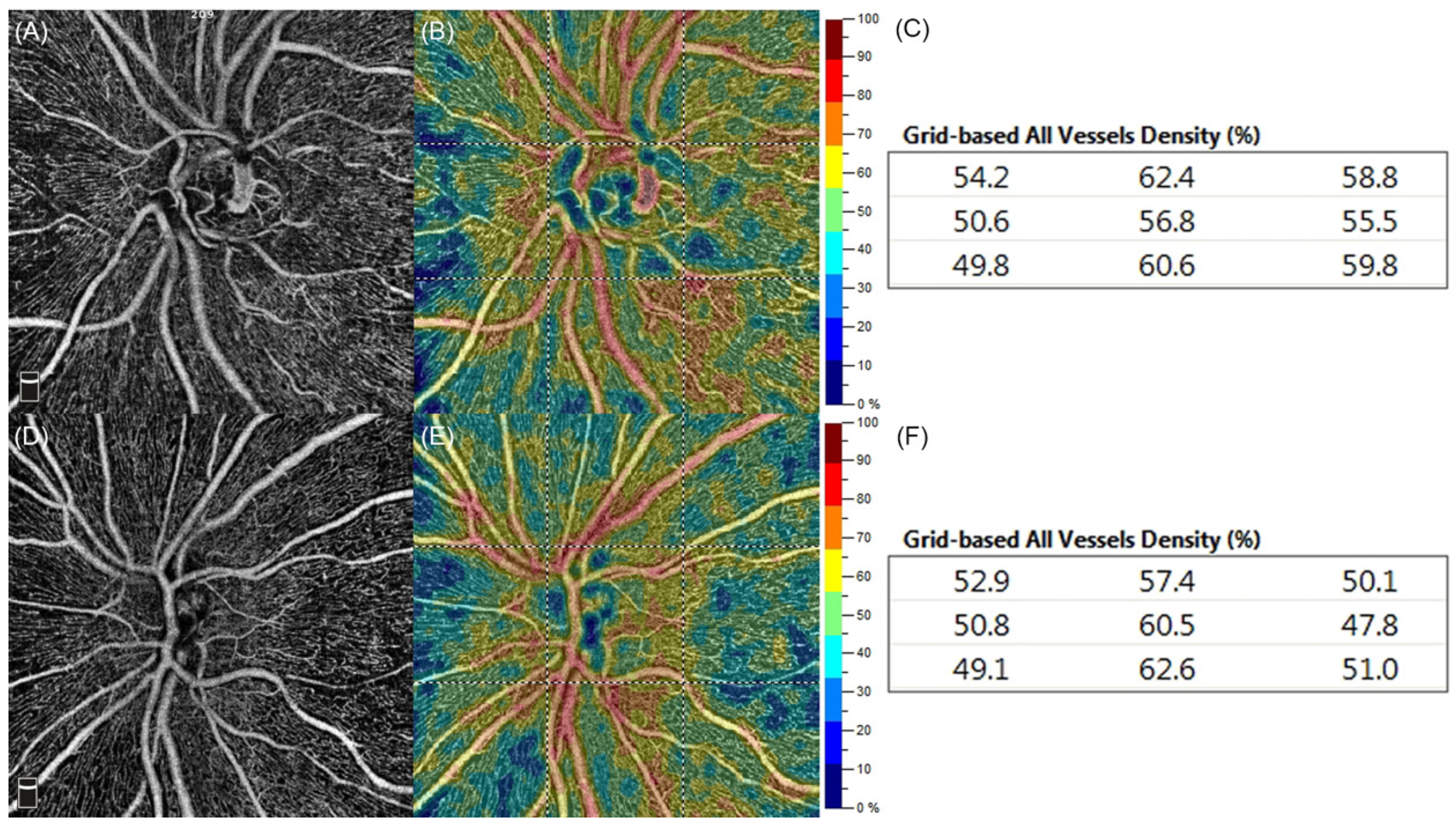
Color-coded perfusion maps were automatically generated using the flow density map software AngioAnalytics, which provided the VD values of the nine different peripapillary sectors (grid-based flow density) of the entire ONH scan. In brief, bright red stood for perfused vessel density of >50%, dark blue meant no perfusion, and intermediate perfusion densities were color-coded accordingly.
Medical conditions such as diabetes mellitus, systemic hypertension, and hypercholesterolemia were assessed. Specifically, participants were classified as hypertensive if they were receiving antihypertension drugs or if their blood pressure was >140 mm Hg systolically or >90 mm Hg diastolically (according to the WHO/International Society of Hypertension). Participants were considered to be diabetic if they were under treatment for insulin- or non-insulin-dependent diabetes mellitus, or if their fasting plasma glucose level was >126 mg/dL and/or their plasma glucose level was >200 mg/dL 2 h after a 75 g oral glucose load in a glucose tolerance test (as defined by the WHO). Hypercholesterolemia was defined by the intake of lipid-lowering drugs or a fasting plasma cholesterol level of >220 mg/dL [
4].
The statistical software package Minitab 19 for macOS (Statistical Software. [Computer software]. State College, PA, USA: Minitab, Inc.
www.minitab.com; accessed on 5 June 2022) and/or Stata 14 for Mac OS X (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, Texas, U.S.: StataCorp LP) were used to perform data processing, summaries, and analyses. Missing data were not replaced. Summary statistics, including the number of subjects (N), number of observations (Obs), mean, median, standard deviation (SD), minimum (Min), and maximum (Max), were calculated for continuous variables. Frequencies and percentages were calculated for categorical data. A Wilcoxon rank-sum test was performed between groups for each variable. A multivariate analysis of covariance (MANCOVA) test was used to examine statistical differences between groups with regards to the flow density maps of the RPC plexus. Statistical tests were two-sided at the 0.05 significance level with 95% confidence intervals.
4. Discussion
In this case–control study, we compared ONH findings in G6PD-deficient and G6PD-normal individuals. Specifically, we focused on the VD of the RPC plexus as automatically detected by OCTA. Interestingly, in G6PD-deficient subjects, the VD values of the RPC plexus were higher, reaching a statistically significant difference in the inferior temporal sector (p = 0.03).
RPCs are the innermost layer of capillaries surrounding the ONH and extending straight along the course of the retinal nerve fiber layer (RNFL) to the posterior pole [
13,
16,
17,
18,
19]. Light microscope observations have highlighted that RPCs do not derive from ONH arterioles or retinal arteries [
18]; rather, they seem to arise from deeper arterial vessels located in the ganglion cell layer or in the outer RNFL and then extend to the superficial RNFL, where they form parallel rows, with rare anastomoses and bifurcations [
13,
14].
Recent OCTA reports on the appearance of RPCs have confirmed that these capillaries have a peculiar distribution and arrangement that runs along the paths of the major temporal vessels up to 4–5 mm from the ONH, and that they form the most superficial vascular layer located within the RNFL [
16,
17,
18,
19]. RPCs, which are easy to identify via OCTA by their typical features, seem to be specialized in the nourishment of the RNFL, especially the most superficial nerve fibers, which subserve the peri-central visual field [
15].
Bjerrum scotoma is a peri-central visual field defect strongly related to selective damage to RPCs, which are more vulnerable to increased IOP than other retinal capillaries, probably because of their peculiar distribution and vascular pattern [
14,
16]. Therefore, it has been supposed that RPCs may represent the first damage site in glaucomatous eyes [
13,
16].
OCTA has revolutionized the vascular imaging approach towards the ONH, allowing for visualization and qualitative/quantitative assessment of the RPC plexus. Noteworthy recent research has focused on the study of the RPC plexus because injuries at this level seem to play a key role, not only in glaucoma, but also in retinal vascular disorders (e.g., RVO, PDR) [
15,
18].
Histopathological evidence indicates that occlusion of linear blood vessels parallel to RNFL axons, corresponding to the RPC plexus, translates into the occurrence of flame-shaped hemorrhages and cotton wool spots due to stagnant axonal flow in the RNFL [
20]. The exact pathogenetic mechanism behind RVO remains elusive; however, intraluminal thrombus formation has been associated with venous stasis, endothelial damage, and hypercoagulability. A strong correlation between RVO and typical atherosclerosis risk factors, including systemic hypertension, hypercholesterolemia, and diabetes mellitus, has widely been documented [
4,
21,
22].
In two former studies on Sardinian patients with RVO and NA-AION, the frequency of G6PD deficiency was found to be significantly lower than expected, suggesting that G6PD-deficient subjects may have a decreased risk of developing RVO and NA-AION [
4,
7]. Why and how G6PD deficiency may offer protection against RVO and NA-AION is still a matter of debate. Batetta et al. [
23] have demonstrated that G6PD-deficient patients show decreased cholesterol synthesis and esterification due to peculiar alterations in lipid metabolism, which is likely to be responsible for reduced cholesterol accumulation in the arteries of these subjects. Therefore, the slower progression of the atherosclerotic process in G6PD-deficient patients may translate into a reduced risk of atherosclerotic vascular disorders, including RVO and NA-AION. Furthermore, this theory may explain why G6PD-deficient patients show low mortality rates from cardiovascular and cerebrovascular diseases [
2].
In our study, G6PD-deficient men had significantly higher VD values of the RPC plexus than age-matched G6PD-normal controls, suggesting the presence of a denser vascular network in the former. Theoretically, this OCTA finding may represent an advantage in protection against retinal vascular disorders.
The NADPH oxidase (Nox) family catalyzes the reduction of O
2 to reactive oxygen species, coupled with NADPH oxidation. Seven isoforms of Nox (Nox1-5 and Duox1-2) have been identified so far. Among them, Nox2 is highly expressed in cells throughout the central nervous system and retina, including endothelial cells [
8,
24]. There is evidence from mouse studies that endothelial Nox2 activity increases with age in the brain and contributes to age-related capillary rarefaction [
8]. Since Nox2 is an NADPH-dependent enzyme, G6PD-deficient individuals might experience reduced endothelial Nox2 activity and reduced age-related capillary rarefaction.
The balance between the activity of nitric oxide synthase (NOS), an NAPDH-dependent enzyme, and concentrations of glutathione (GSH), a physiological NO scavenger, may play a crucial role in preventing the development of vascular disorders [
25,
26]. It is not known whether NOS and GSH are out of balance in G6PD-deficient subjects; however, experimental evidence indicates that G6PD deficiency may lead to decreased NO production [
27]. In G6PD deficiency, it is possible that the combined action of NO and GSH may be responsible for inhibiting low-density lipoprotein esterification, smooth muscle cell proliferation, and platelet aggregation, which may lead to vessel dilation and a slow-down of the atherosclerotic process.
The present study has some important limitations, principally related to the small number of eyes examined. In total, 69 male patients were enrolled, and the G6PD-deficient group was chosen to be twice as large as the control group. Furthermore, no women were included in this study due to a lack of homozygote female subjects available. Nevertheless, we are unaware of any previously published report assessing the VD of the RPC plexus in G6PD-deficient and G6PD-normal individuals.
In conclusion, our results show that G6PD-deficient men have higher VD values in the RPC plexus, although a statistically significant difference was found only in the inferior temporal sector (p = 0.03). A denser vascular network at this level, together with decreased cholesterol synthesis and esterification, may contribute to explaining why G6PD-deficient men seem to have a reduced risk of ocular vascular diseases, such as RVO and NA-AION. Further larger studies are necessary to confirm these preliminary findings and establish the potential protective role of G6PD deficiency against ocular diseases.


 ,
, 

{kind=link}