
Diagnosis of Subclinical Keratoconus Based on Machine Learning Techniques

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
- Sixty-one eyes with healthy corneas. They had the following characteristics: (1) normal morphology, (2) negative keratoconus morphology, (3) no history of eye diseases. Each patient included only one eye;
- Twenty patients with subclinical keratoconus (SCKC): This initial stage included patients with the following conditions: (1) minor topographic signs of keratoconus and suspicious topographic findings (mild asymmetric bow tie, with or without deviation; (2) average K (mean corneal curvature) <46, 5 D; (3) minimum corneal thickness (ECM)> 490 μm; (4) no slit lamp found (no central thinning, Fleischer ring or Vogt pattern); (5) contralateral clinical keratoconus of the eye.
2.1. Patient Examination
2.2. Database Cleaning
- Normalization of N (0,1) variables: this step was not necessary in random forest and decision trees; the explanatory variables were not normalized in these methodologies. Other methodologies such as support vector machines, k-neighbors did require such normalization;
- Elimination of variables with marginal variance; this type of variable does not help to build the model;
- Elimination of variables with high correlation since highly correlated independent variables contribute noise and can lead the researcher to erroneous conclusions;
- Elimination of linear dependencies.
2.3. Techniques for Working with Unbalanced Data
- Undersampling: This involves the underrepresentation of the most frequent class or group. In this case, it was the NORMAL class. The NORMAL sample number decreased from 61 to 58 observations;
- Oversampling: Passes through the overrepresentation of the less frequent class or group. In this case, it was the SCKC class. The SCKC sample number boosted from 20 to 54 observations avoiding unbalanced data.
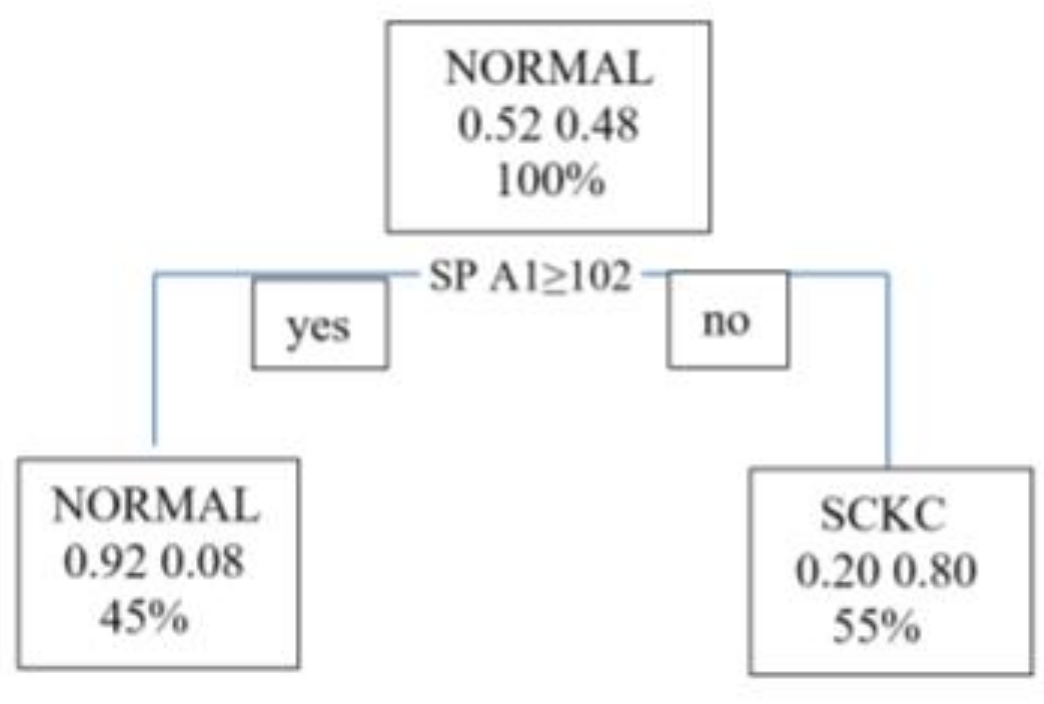
2.4. Decision Tree
2.5. Random Forest Algorithm
2.5.1. Importance of Variables in the Ranking
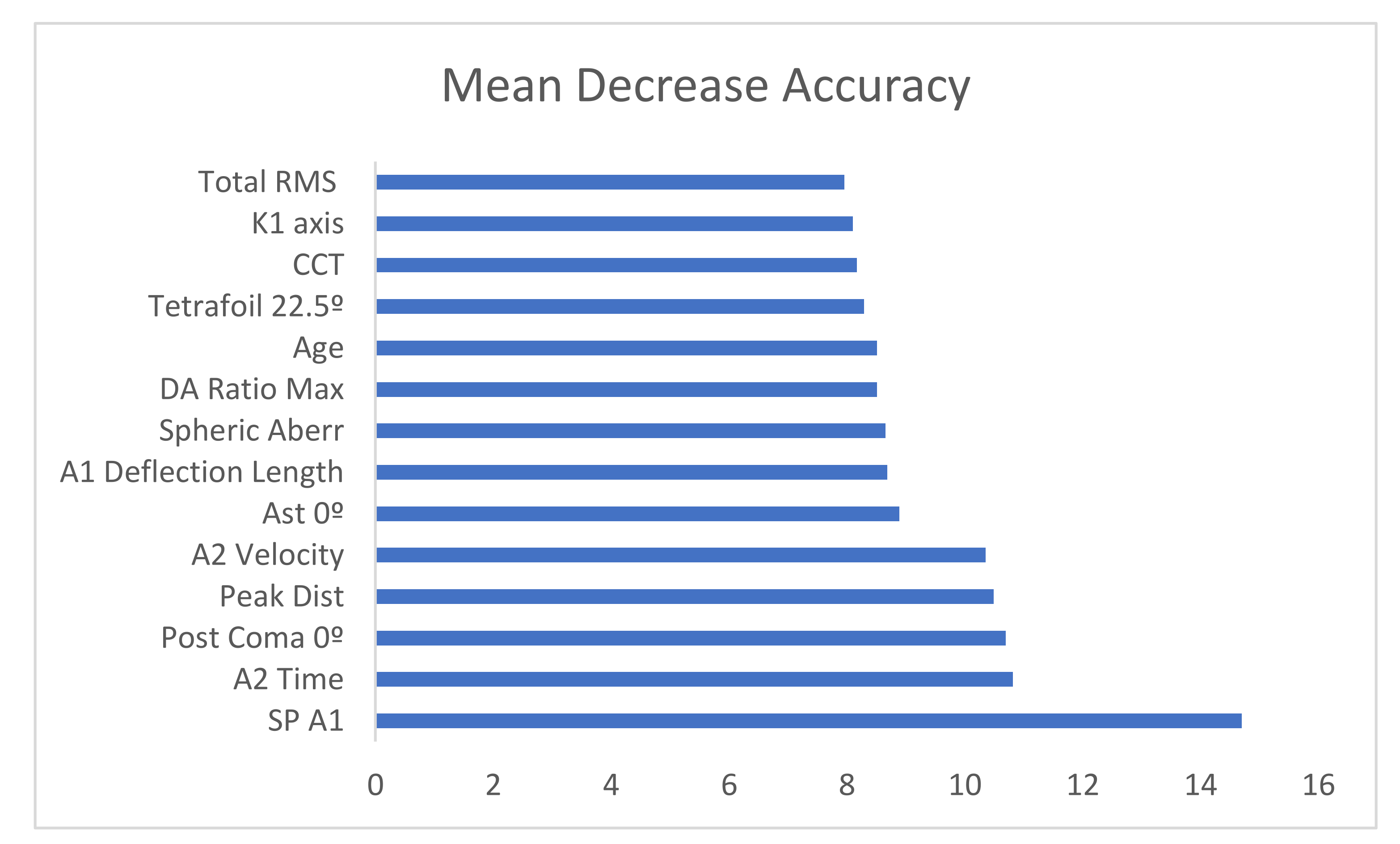
- Mean decrease accuracy: This shows the amount of accuracy the model loses when excluding each variable. The more accuracy is lost, the more influential the variable is in the ranking;
- Mean decrease in Gini: This coefficient measures how a variable contributes to the homogeneity of the nodes and leaves in the resulting model.
2.5.2. Fold Cross-Validation
2.5.3. Confusion Matrix and Metrics
- Recall/sensitivity: TP/(TP + FN)—proportion of all positive cases correctly identified as positive by the algorithm;
- Specificity: TN/(TN + FP)—proportion of all negative cases correctly predicted as negative by the algorithm;
- F1-score: combines the precision and recall metrics into a single measure. It is the harmonic mean of both metrics.
3. Results
3.1. Descriptive Statistics
3.2. Database Cleaning
- Demographic variables: age;
- General examination data: LogMAR;
- General topographic indices: K1 Axis, K1 p, K1 Axis p, K2 p, K2 Axis p, Qp, CCT;
- Aberrometric topographic indices measured by Pentacam: Total RMS, Ast 0°, Ast 45°, Coma post 0°, Trefoil 0°, Trefoil 30°, Tetrafoil 0°, Tetrafoil 22.5°, Spherical Aberration;
- Biomechanical indices measured by Corvis: A1 Deflection Length, A2 Time, A2 Deflection Length, A2 Velocity, HC Time, PeakDist, Radius, DA Ratio Max, SP A1.
3.3. Generation of the New Database
3.4. Decision Trees
3.5. Random Forest
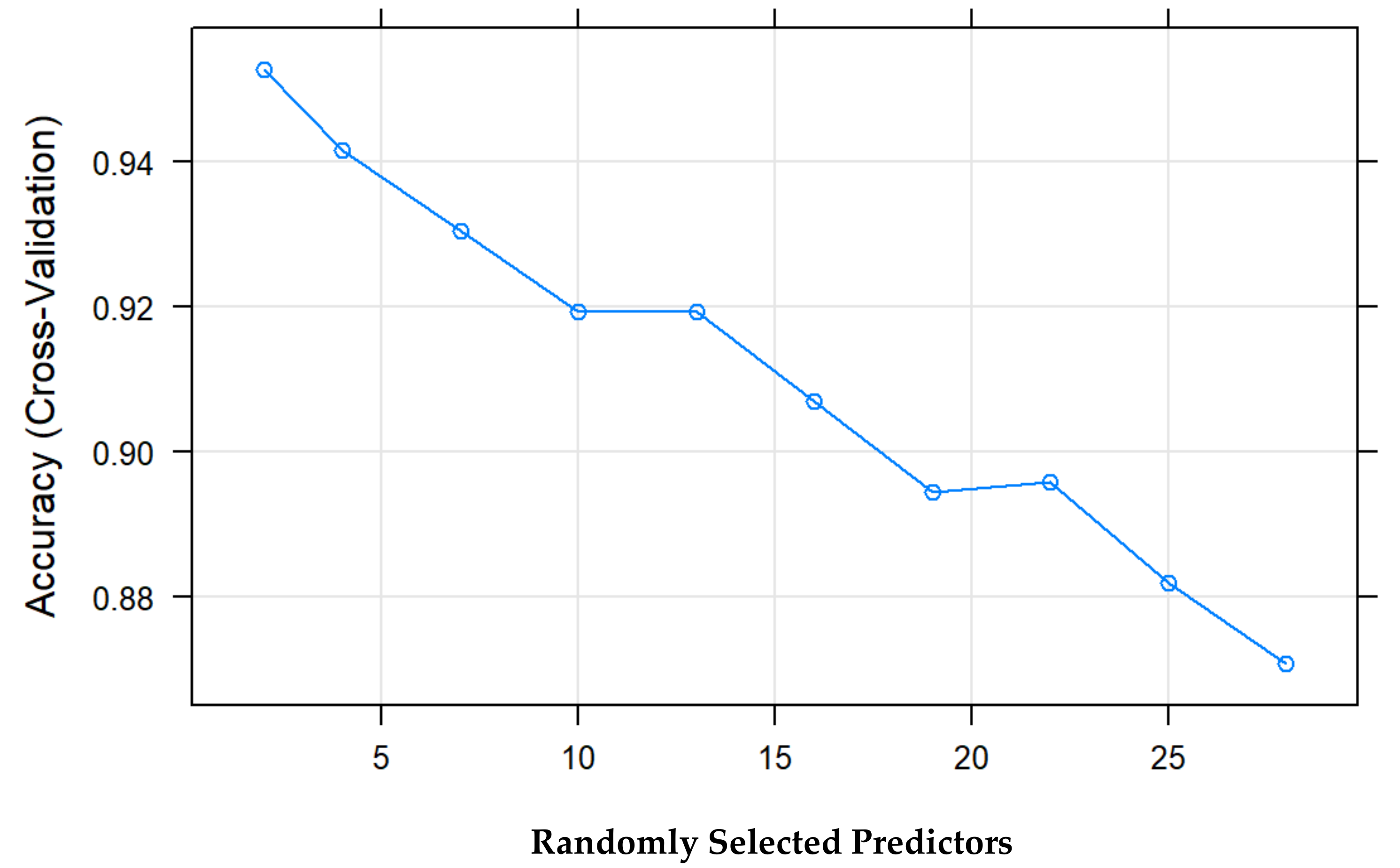
3.5.1. Number of Random Variables as Candidates in Each Branch (Mtry)
3.5.2. Number of Trees in the Forest (Ntree)
3.5.3. Importance of Variables in rf
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krachmer, J.H.; Feder, R.S.; Belin, M.W. Keratoconus and related non-inflammatory corneal thinning disorders. Surv. Ophthalmol. 1984, 28, 293–322. [Google Scholar] [CrossRef]
- Chatzis, N.; Hafezi, F. Progression of keratoconus and efficacy of pediatric corneal collagen cross-linking in children and adolescents. J. Refract. Surg. 2012, 28, 753–758. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, D.S.; Dohlman, C.H. Is keratoconus genetic? Int. Ophthalmol. Clin. 1993, 33, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Sherwin, T.; Brookes, N.H. Morphological changes in keratoconus: Pathology or pathogenesis. Clin. Exp. Ophthalmol. 2004, 32, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Ferdi, A.C.; Nguyen, V.; Gore, D.M.; Allan, B.D.; Rozema, J.J.; Watson, S.L. Keratoconus natural progression: A systematic review and meta-analysis of11 529 eyes. Ophthalmology 2019, 126, 935–945. Available online: http://tvst.arvojournals.org (accessed on 7 May 2021). [CrossRef] [PubMed]
- Maeda, N.; Klyce, S.D.; Smolek, M.K.; Thompson, H.W. Automated keratoconus screening with corneal topography analysis. Investig. Ophthalmol. Vis. Sci. 1994, 35, 2749–2757. [Google Scholar]
- Hustead, J.D. Detection of keratoconus before keratorefractive surgery. Ophthalmology 1993, 100, 975. [Google Scholar] [CrossRef]
- Rabinowitz, Y.S.; McDonnell, P.J. Computer-assisted corneal topography in keratoconus. Refract. Corneal Surg. 1989, 5, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Dastjerdi, M.H.; Hashemi, H. A quantitative corneal topography index for detection of keratoconus. J. Refract. Surg. 1998, 14, 427–436. [Google Scholar] [CrossRef]
- Holladay, J.T. Keratoconus detection using corneal topography. J. Refract. Surg. 2009, 25, S958–S962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ting, D.S.W.; Pasquale, L.R.; Peng, L.; Campbell, J.P.; Lee, A.Y.; Raman, R.; Tan, G.S.W.; Schmetterer, L.; Keane, P.A.; Wong, T.Y. Artificial intelligence and deep learning in ophthalmology. Br. J. Ophthalmol. 2019, 103, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Cheung, C.Y.; Tang, F.; Ting, D.S.W.; Tan, G.S.W.; Wong, T.Y. Artificial intelligence in diabetic eye dis-ease screening. Asia Pac. J. Ophthalmol. 2019, 8, 18–164. [Google Scholar] [CrossRef]
- Zheng, C.; Johnson, T.V.; Garg, A.; Boland, M.V. Artificial intelligence in glaucoma. Curr. Opin. Ophthalmol. 2019, 30, 97–103. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Waldstein, S.M.; Klimscha, S.; Sadeghipour, A.; Hu, X.; Gerendas, B.S.; Osborne, A.; Bogunović, H. Prediction of Individual Disease Conversion in Early AMD Using Artificial Intelligence. Investig. Ophthalmol Vis. Sci. 2018, 59, 3199–3208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, J.E.; Eaton, E. Artificial intelligence for pediatric ophthalmology. Curr. Opin. Ophthalmol. 2019, 30, 337–346. [Google Scholar] [CrossRef]
- Smolek, M.K.; Klyce, S.D. Current keratoconus detection methods compared with a neural network approach. Investig. Ophthalmol. Vis. Sci. 1997, 38, 2290–2299. [Google Scholar]
- Accardo, P.A.; Pensiero, S. Neural network-based system for early keratoconus detection from corneal topography. J. Biomed. Inform. 2002, 35, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Hwang, E.S.; Perez-Straziota, C.E.; Kim, S.W.; San-thiago, M.R.; Randleman, J.B. Distinguishing highly asymmetric keratoconus eyes using combined scheimpflug and spectral-domain OCT analysis. Ophthalmology 2018, 125, 1862–1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Rueda, A.; Jiménez-Rodríguez, D.; Castro-Luna, G. Diagnosis of Subclinical Keratoconus with a Combined Model of Biomechanical and Topographic Parameters. J. Clin. Med. 2021, 10, 2746. [Google Scholar] [CrossRef] [PubMed]
- Castro-Luna, G.; Pérez-Rueda, A. A predictive model for early diagnosis of keratoconus. BMC Ophthalmol. 2020, 20, 263. [Google Scholar] [CrossRef] [PubMed]
- Arbelaez, M.C.; Versaci, F.; Vestri, G.; Barboni, P.; Savini, G. Use of a support vector machine for keratoconus and subclinical keratoconus detection by topographic and tomographic data. Ophthalmology 2012, 119, 2231–2238. [Google Scholar] [CrossRef]
- Smadja, D.; Touboul, D.; Cohen, A.; Doveh, E.; Santhiago, M.R.; Mello, G.R.; Krueger, R.R.; Colin, J. detection of subclinical keratoconus using an automated decision tree classification. Am. J. Ophthalmol. 2013, 156, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Ambrósio, R., Jr.; Lopes, B.T.; Faria-Correia, F.; Salomão, M.Q.; Bühren, J.; Roberts, C.J.; Elsheikh, A.; Vinciguerra, R.; Vinciguerra, P. Integration of Scheimpflug-Based Corneal Tomography and Biomechanical Assessments for Enhancing Ectasia Detection. J. Refract. Surg. 2017, 33, 434–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovács, I.; Miháltz, K.; Kránitz, K.; Juhász, E.; Takács, A.; Dienes, L.; Gergely, R.; Nagy, Z.Z. Accuracy of machine learning classifiers using bilateral data from a Scheimpflug camera for identifying eyes with preclinical signs of keratoconus. J. Cataract Refract. Surg. 2016, 42, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Castro-Luna, G.M.; Martínez-Finkelshtein, A.; Ramos-López, D. Robust keratoconus detection with Bayesian network classifier for Placido-based corneal indices. Cont. Lens Anterior Eye 2020, 43, 366–372. [Google Scholar] [CrossRef]
- Issarti, I.; Consejo, A.; Jiménez-García, M.; Hershko, S.; Koppen, C.; Rozema, J.J. Computer aided diagnosis for suspect keratoconus detection. Comput. Biol. Med. 2019, 109, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Zhao, L.; Yang, X.; Wu, X.; Yang, Y.; Huang, X.; Liu, F.; Xu, J.; Lin, L.; Lin, H.; et al. Screening Candidates for Refractive Surgery with Corneal Tomographic-Based Deep Learning. JAMA Ophthalmol. 2020, 138, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Ruiz Hidalgo, I.; Rodriguez, P.; Rozema, J.J.; Ní Dhubhghaill, S.; Zakaria, N.; Tassignon, M.J.; Koppen, C. Evaluation of a Machine-Learning Classifier for Keratoconus Detection Based on Scheimpflug Tomography. Cornea 2016, 35, 827–832. [Google Scholar] [CrossRef]
- Lavric, A.; Valentin, P. KeratoDetect: Keratoconus Detection Algorithm Using Convolutional Neural Networks. Comput. Intell. Neurosci. 2019, 2019, 8162567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.R.; Ladas, J.G.; Bahadur, G.G.; Al-Hashimi, S.; Pineda, R. A Review of Machine Learning Techniques for Keratoconus Detection and Refractive Surgery Screening. Semin. Ophthalmol. 2019, 34, 317–326. [Google Scholar] [CrossRef]
- Ting, D.S.J.; Foo, V.H.; Yang, L.W.Y.; Sia, J.T.; Ang, M.; Lin, H.; Chodosh, J.; Mehta, J.S.; Ting, D.S.W. Artificial intelligence for anterior segment diseases: Emerging applications in ophthalmology. Br. J. Ophthalmol. 2021, 105, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Lopes, B.T.; Ramos, I.C.; Salomao, M.Q.; Guerra, F.P.; Schallhorn, S.C.; Schallhorn, J.M.; Vinciguerra, R.; Vinciguerra, P.; Price, F.W., Jr.; Price, M.O.; et al. Enhanced tomographic assessment to detect corneal ectasia based on artificial intelligence. Am. J. Ophthalmol. 2018, 195, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Peris-Martínez, C.; Díez-Ajenjo, M.A.; García-Domene, M.C.; Pinazo-Durán, M.D.; Luque-Cobija, M.J.; Del Buey-Sayas, M.Á.; Or-tí-Navarro, S. Evaluation of Intraocular Pressure and Other Biomechanical Parameters to Distinguish between Subclinical Keratoconus and Healthy Corneas. J. Clin. Med. 2021, 10, 1905. [Google Scholar] [CrossRef]
- Ren, S.; Xu, L.; Fan, Q.; Gu, Y.; Yang, K. Accuracy of new Corvis ST parameters for detecting subclinical and clinical keratoconus eyes in a Chinese population. Sci. Rep. 2021, 11, 4962. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.J.; Mahmoud, A.M.; Bons, J.P.; Hossain, A.; Elsheikh, A.; Vinciguerra, R.; Vinciguerra, P.; Ambrósio, R., Jr. Introduction of Two Novel Stiffness Parameters and Interpretation of Air Puff-Induced Biomechanical Deformation Parameters With a Dynamic Scheimpflug Analyzer. J. Refract. Surg. 2017, 33, 266–273. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Shen, Y.; Yan, Z.; Tian, M.; Zhao, J.; Zhou, T. Relationship Among Corneal Stiffness, Thickness, and Biomechanical Parameters Measured by Corvis ST, Pentacam and ORA in Keratoconus. Front. Physiol. 2019, 10, 740. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mean | Std. Deviation | Std. Error | Sig. | ||
|---|---|---|---|---|---|
| Age(years) | Normal | 45.85 | 20.04 | 2.57 | 0.09 |
| SCKC | 40.21 | 13.19 | 2.95 | ||
| BSCVA (decimal scale) | Normal | 0.98 | 0.05 | 0.01 | 0.97 |
| SCKC | 0.99 | 0.07 | 0.02 | ||
| Sph eq (diopters) | Normal | −1.04 | 3.16 | 0.47 | 0.52 |
| SCKC | −1.85 | 1.6 | 0.44 | ||
| KMAX (diopters) | Normal | 45.54 | 2.07 | 0.27 | 0.61 |
| SCKC | 46.15 | 2.12 | 0.47 | ||
| CCT (µm) | Normal | 529.48 | 51.08 | 6.59 | 0.17 |
| SCKC | 511.4 | 30.04 | 6.72 | ||
| IOP (mmHg) | Normal | 16.19 | 3.55 | 0.45 | 0.00 * |
| SCKC | 13.61 | 2.06 | 0.46 | ||
| HOA RMS (µm) | Normal | 0.51 | 0.25 | 0.03 | 0.31 |
| SCKC | 0.63 | 0.3 | 0.07 | ||
| Mean | Std. Deviation | Std. Error | p-Value | ||
|---|---|---|---|---|---|
| Def. Amp. Max (mm) | Normal | 1.03 | 0.1 | 0.01 | 0.01 * |
| SCKC | 1.13 | 0.11 | 0.02 | ||
| A1 Time (ms) | Normal | 7.52 | 0.39 | 0.05 | 0.00 * |
| SCKC | 7.22 | 0.22 | 0.05 | ||
| A1 Deflection Length(mm) | Normal | 2.35 | 0.31 | 0.04 | 0.24 |
| SCKC | 2.24 | 0.24 | 0.05 | ||
| A1 Velocity (m/s) | Normal | 0.14 | 0.02 | 0 | 0.00 * |
| SCKC | 0.16 | 0.02 | 0 | ||
| A2 Time (ms) | Normal | 21.6 | 1.03 | 0.13 | 0.08 |
| SCKC | 22.01 | 0.58 | 0.13 | ||
| A2 Deflection Length (mm) | Normal | 3.21 | 0.8 | 0.11 | 0.68 |
| SCKC | 3 | 0.76 | 0.17 | ||
| A2 Velocity (m/s) | Normal | −0.23 | 0.04 | 0.01 | 0.00 * |
| SCKC | −0.27 | 0.04 | 0.01 | ||
| HC Time (ms) | Normal | 17.03 | 0.66 | 0.09 | 0.88 |
| SCKC | 17.12 | 0.4 | 0.09 | ||
| Peak Dist. (mm) | Normal | 4.8 | 0.39 | 0.05 | 0.00 * |
| SCKC | 5.1 | 0.25 | 0.06 | ||
| Radius (mm) | Normal | 7.11 | 1.18 | 0.15 | 0.34 |
| SCKC | 6.75 | 0.78 | 0.18 | ||
| DA Ratio Max (2 mm) | Normal | 4.61 | 3.46 | 0.44 | 1 |
| SCKC | 4.6 | 0.5 | 0.11 | ||
| DA Ratio Max (1 mm) | Normal | 1.68 | 0.65 | 0.08 | 0.8 |
| SCKC | 1.61 | 0.06 | 0.01 | ||
| Integrated Radius (mm−1) | Normal | 8.27 | 1.38 | 0.18 | 0.1 |
| SCKC | 9.04 | 1.34 | 0.3 | ||
| ARTh | Normal | 481.87 | 189.43 | 24.46 | 0.00 * |
| SCKC | 332.46 | 67.37 | 15.46 | ||
| SP A1 | Normal | 113.54 | 18.51 | 2.39 | 0.00 * |
| SCKC | 89.61 | 15.25 | 3.41 | ||
| CBI | Normal | 0.27 | 0.32 | 0.04 | 0.01 * |
| SCKC | 0.59 | 0.38 | 0.09 | ||
| NORMAL | SCKC | |
|---|---|---|
| NORMAL | 7 | 1 |
| SCK | 7 | 13 |
| Value | |
|---|---|
| Sensitivity | 0.50 |
| Specificity | 0.93 |
| Pos Pred Value | 0.88 |
| Neg Pred Value | 0.65 |
| Precision | 0.88 |
| Recall | 0.50 |
| F1 | 0.64 |
| Prevalence | 0.50 |
| Detection Rate | 0.25 |
| Detection Prevalence | 0.29 |
| Balanced Accuracy | 0.71 |
| NORMAL | SCK | |
|---|---|---|
| NORMAL | 12 | 1 |
| SCKC | 2 | 13 |
| Value | |
|---|---|
| Sensitivity | 0.86 |
| Specificity | 0.93 |
| Pos Pred Value | 0.92 |
| Neg Pred Value | 0.87 |
| Precision | 0.92 |
| Recall | 0.86 |
| F1 | 0.89 |
| Prevalence | 0.50 |
| Detection Rate | 0.43 |
| Detection Prevalence | 0.46 |
| Balanced Accuracy | 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Luna, G.; Jiménez-Rodríguez, D.; Castaño-Fernández, A.B.; Pérez-Rueda, A. Diagnosis of Subclinical Keratoconus Based on Machine Learning Techniques. J. Clin. Med. 2021, 10, 4281. https://doi.org/10.3390/jcm10184281
Castro-Luna G, Jiménez-Rodríguez D, Castaño-Fernández AB, Pérez-Rueda A. Diagnosis of Subclinical Keratoconus Based on Machine Learning Techniques. Journal of Clinical Medicine. 2021; 10(18):4281. https://doi.org/10.3390/jcm10184281
Chicago/Turabian StyleCastro-Luna, Gracia, Diana Jiménez-Rodríguez, Ana Belén Castaño-Fernández, and Antonio Pérez-Rueda. 2021. "Diagnosis of Subclinical Keratoconus Based on Machine Learning Techniques" Journal of Clinical Medicine 10, no. 18: 4281. https://doi.org/10.3390/jcm10184281