
Early Improvements in Disease Activity Indices Predict Long-Term Clinical Remission Suggested by the Treat-to-Target Strategy in Patients with Ankylosing Spondylitis Receiving TNF-α Inhibitor Treatment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Demographic and Clinical Data
2.3. Statistical Analysis
3. Results
3.1. Baseline Demographic and Clinical Characteristics
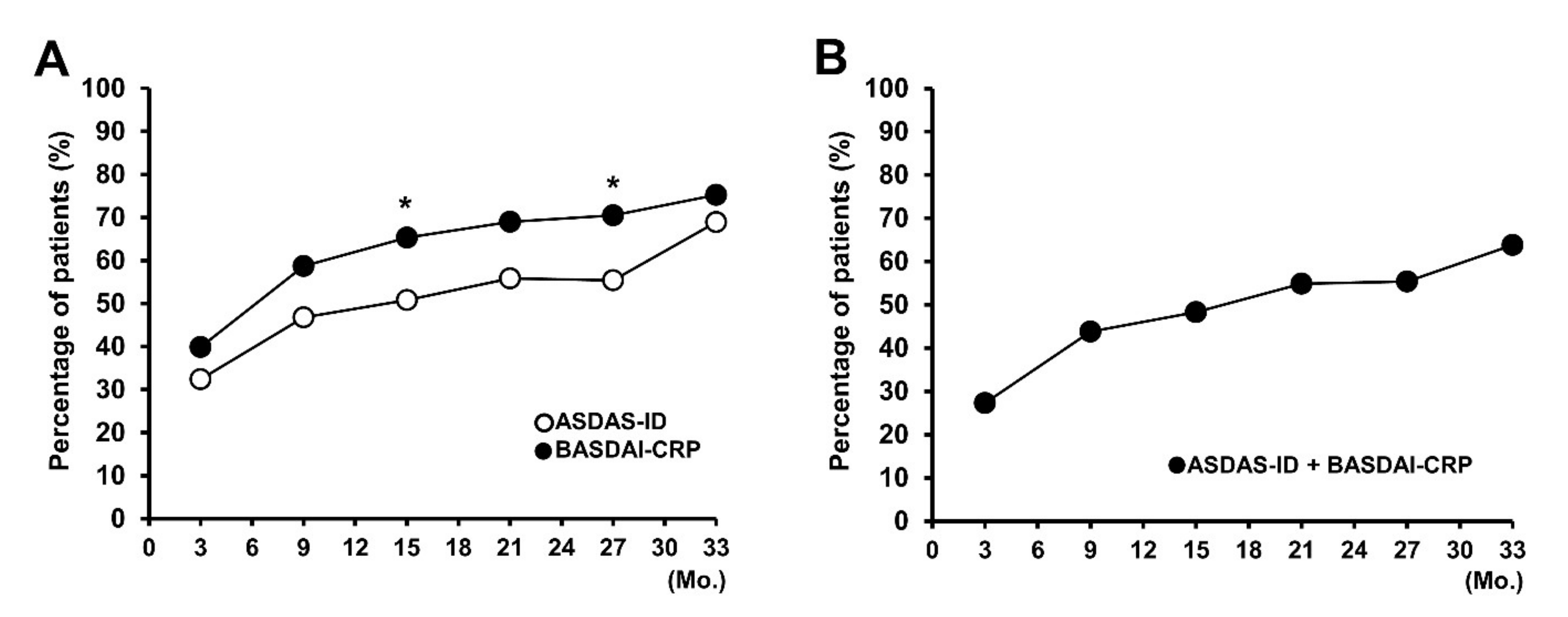
3.2. Attainment Rate of Clinical Remission Criteria during TNFi Treatment
3.3. Early Improvement in Disease Activity Indices as a Predictor of ASDAS-ID Achievement during TNFi Treatment
3.4. Early Change in Disease Activity Indices as a Predictor of BASDAI-CRP Attainment during TNFi Treatment
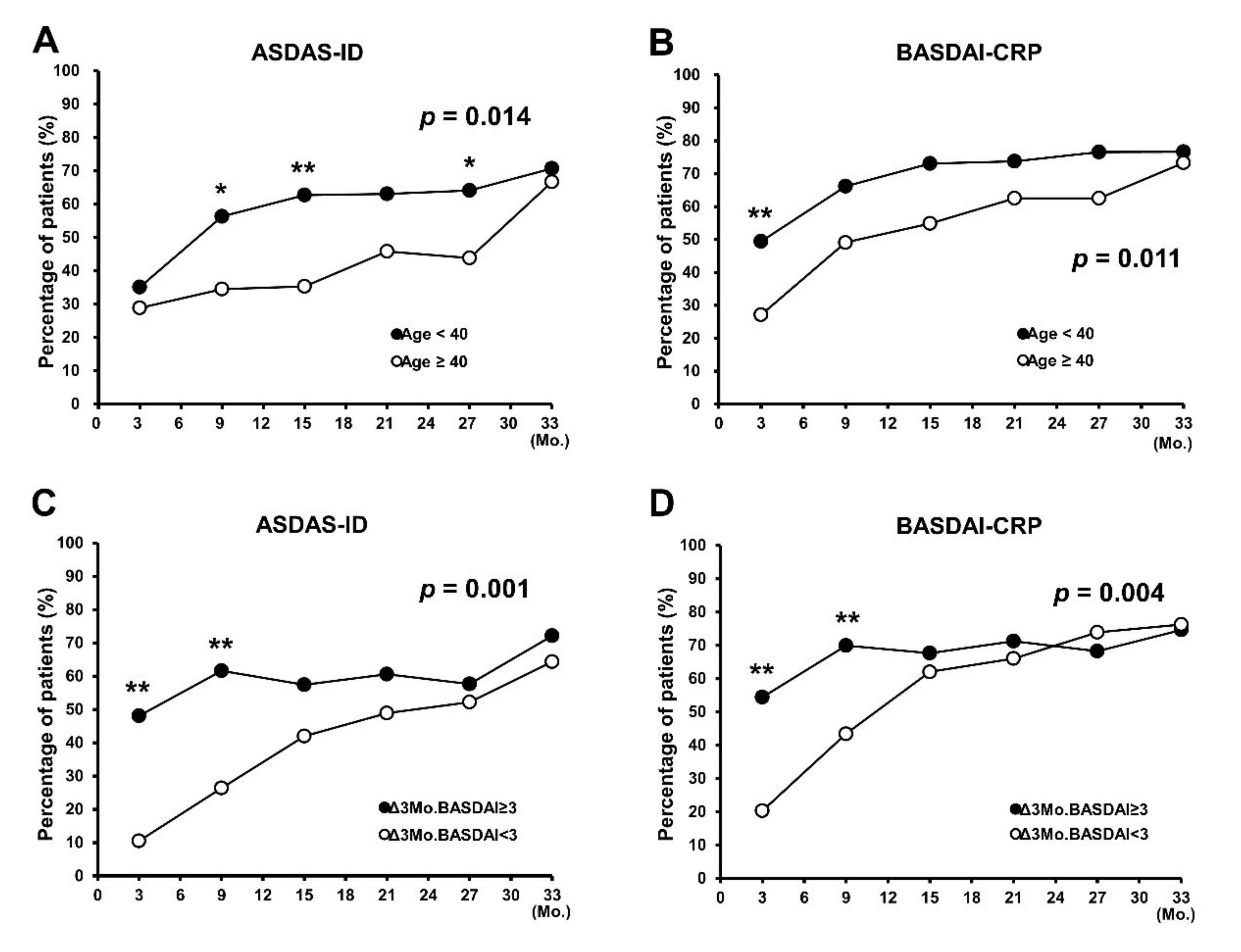
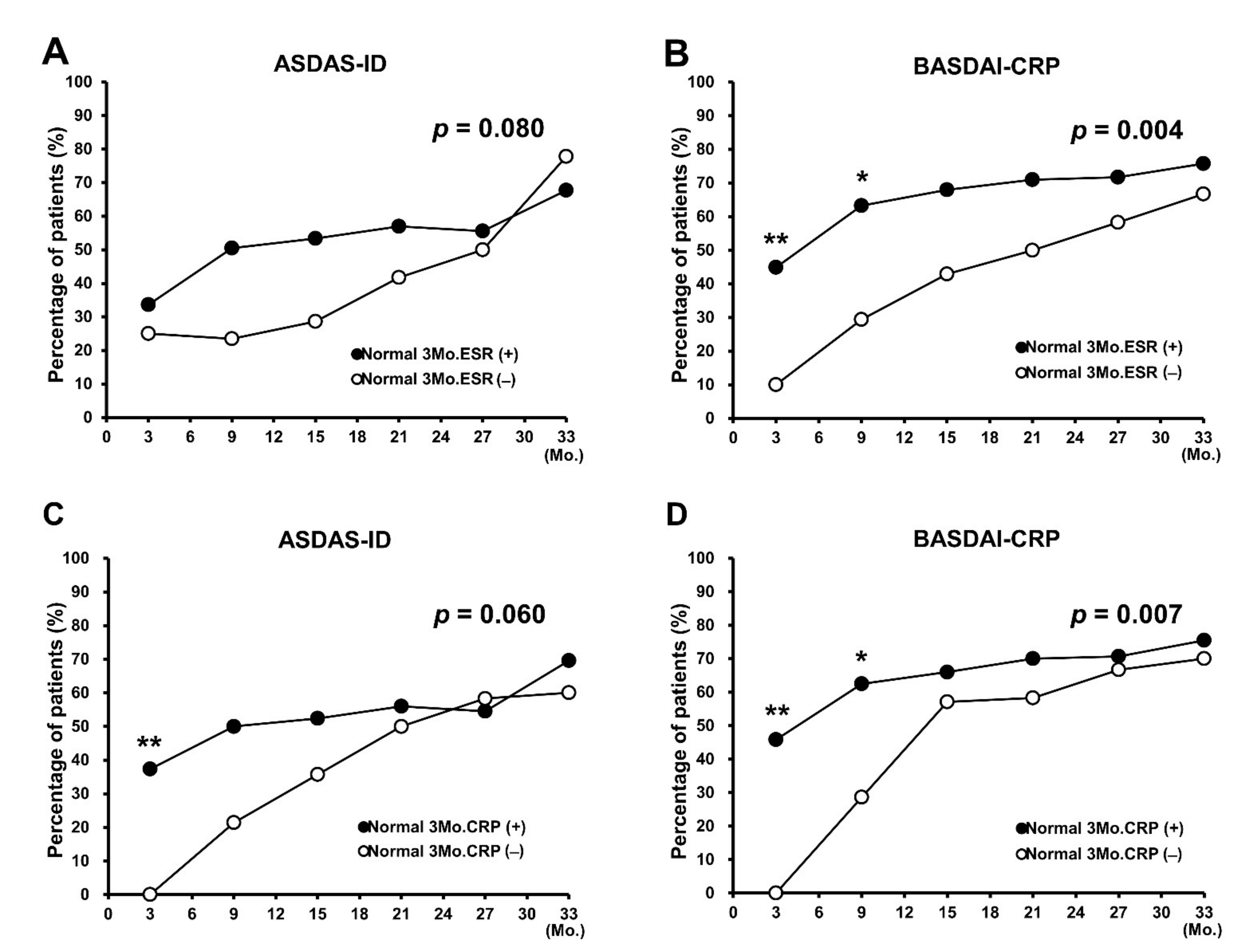
3.5. Sub-Analysis of Identified Predictors for Achievement of Clinical Remission during TNFi Treatment
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Osman, M.S.; Maksymowych, W.P. An update on the use of tumor necrosis factor alpha inhibitors in the treatment of ankylosing spondylitis. Expert Rev. Clin. Immunol. 2017, 13, 125–131. [Google Scholar] [CrossRef]
- Torgutalp, M.; Poddubnyy, D. Emerging treatment options for spondyloarthritis. Best Pract. Res. Clin. Rheumatol. 2018, 32, 472–484. [Google Scholar] [CrossRef]
- Van Der Heijde, D.; Ramiro, S.; Landewé, R.; Baraliakos, X.; Van den Bosch, F.; Sepriano, A.; Regel, A.; Ciurea, A.; Dagfinrud, H.; Dougados, M.; et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann. Rheum. Dis. 2017, 76, 978–991. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.M.; Deodhar, A.; Akl, E.A.; Lui, A.; Ermann, J.; Gensler, L.S.; Smith, J.A.; Borenstein, D.; Hiratzka, J.; Weiss, P.F.; et al. American College of Rheumatology/Spondylitis association of america/spondyloarthritis research and treatment network 2015 recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Care Res. 2016, 68, 151–166. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.M.; Deodhar, A.; Gensler, L.S.; Dubreuil, M.; Yu, D.; Khan, M.A.; Haroon, N.; Borenstein, D.; Wang, R.; Biehl, A.; et al. 2019 Update of the American College of Rheumatology/Spondylitis association of america/spondyloarthritis research and treatment network recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Care Res. 2019, 71, 1285–1299. [Google Scholar] [CrossRef] [Green Version]
- Smolen, J.S.; Braun, J.; Dougados, M.; Emery, P.; FitzGerald, O.; Helliwell, P.; Kavanaugh, A.; Kvien, T.K.; Landewé, R.; Luger, T.; et al. Treating spondyloarthritis, including ankylosing spondylitis and psoriatic arthritis, to target: Recommendations of an international task force. Ann. Rheum Dis 2014, 73, 6–16. [Google Scholar] [CrossRef]
- Smolen, J.S.; Schöls, M.; Braun, J.; Dougados, M.; FitzGerald, O.; Gladman, D.D.; Kavanaugh, A.; Landewé, R.; Mease, P.; Sieper, J.; et al. Treating axial spondyloarthritis and peripheral spondyloarthritis, especially psoriatic arthritis, to target: 2017 update of recommendations by an international task force. Ann. Rheum. Dis. 2018, 77, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.M.; Deodhar, A. Treat-to-target in axial spondyloarthritis: Gold standard or fools’ gold? Curr. Opin. Rheumatol. 2019, 31, 344–348. [Google Scholar] [CrossRef]
- Liew, J.W.; Dubreuil, M. Treat to Target in axial spondyloarthritis: Pros, cons, and future directions. Rheum. Dis. Clin. 2020, 46, 343–356. [Google Scholar] [CrossRef] [PubMed]
- Sieper, J. How to define remission in ankylosing spondylitis? Ann. Rheum. Dis. 2012, 71 (Suppl. 2), 93–95. [Google Scholar] [CrossRef] [PubMed]
- Zochling, J. Measures of symptoms and disease status in ankylosing spondylitis: Ankylosing Spondylitis Disease Activity Score (ASDAS), Ankylosing Spondylitis Quality of Life Scale (ASQoL), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI), Bath Ankylosing Spondylitis Global Score (BAS-G), Bath Ankylosing Spondylitis Metrology Index (BASMI), Dougados Functional Index (DFI), and Health Assessment Questionnaire for the Spondylarthropathies (HAQ-S). Arthritis Care Res. 2011, 63 (Suppl. 11), S47–S58. [Google Scholar]
- Sieper, J.; van der Heijde, D.; Dougados, M.; Brown, L.S.; Lavie, F.; Pangan, A.L. Early response to adalimumab predicts long-term remission through 5 years of treatment in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2012, 71, 700–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Heijde, D.; Deodhar, A.; Fleischmann, R.; Mease, P.J.; Rudwaleit, M.; Nurminen, T.; Davies, O. Early disease activity or clinical response as predictors of long-term outcomes with certolizumab pegol in axial spondyloarthritis or psoriatic arthritis. Arthritis Care Res. 2017, 69, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Vastesaeger, N.; Van Der Heijde, D.; Inman, R.D.; Wang, Y.; Deodhar, A.; Hsu, B.; Rahman, M.U.; Dijkmans, B.; Geusens, P.; Vander Cruyssen, B.; et al. Predicting the outcome of ankylosing spondylitis therapy. Ann. Rheum. Dis. 2011, 70, 973–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tužil, J.; Mlčoch, T.; Jirčíková, J.; Závada, J.; Nekvindová, L.; Svoboda, M.; Uher, M.; Křístková, Z.; Vencovský, J.; Pavelka, K.; et al. Short-term response in new users of anti-TNF predicts long-term productivity and non-disability: Analysis of Czech ATTRA ankylosing spondylitis biologic registry. Expert Opin. Biol. Ther. 2020, 20, 183–192. [Google Scholar] [CrossRef]
- Arends, S.; Brouwer, E.; van der Veer, E.; Groen, H.; Leijsma, M.K.; Houtman, P.M.; Tim, L.; Kallenberg, C.G.; Spoorenberg, A. Baseline predictors of response and discontinuation of tumor necrosis factor-alpha blocking therapy in ankylosing spondylitis: A prospective longitudinal observational cohort study. Arthritis Res. Ther. 2011, 13, R94. [Google Scholar] [CrossRef] [Green Version]
- Glintborg, B.; Ostergaard, M.; Krogh, N.S.; Dreyer, L.; Kristensen, H.L.; Hetland, M.L. Predictors of treatment response and drug continuation in 842 patients with ankylosing spondylitis treated with anti-tumour necrosis factor: Results from 8 years’ surveillance in the Danish nationwide DANBIO registry. Ann. Rheum. Dis. 2010, 69, 2002–2008. [Google Scholar] [CrossRef]
- Van der Linden, S.; Valkenburg, H.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984, 27, 361–368. [Google Scholar] [CrossRef]
- Ramiro, S.; van der Heijde, D.; van Tubergen, A.; Stolwijk, C.; Dougados, M.; van den Bosch, F.; Landewé, R. Higher disease activity leads to more structural damage in the spine in ankylosing spondylitis: 12-year longitudinal data from the OASIS cohort. Ann. Rheum. Dis.. 2014, 73, 1455–1461. [Google Scholar] [CrossRef] [Green Version]
- Machado, P.M.; Landewe, R.; Heijde, D.V. Assessment of SpondyloArthritis international S. Ankylosing Spondylitis Disease Activity Score (ASDAS): 2018 update of the nomenclature for disease activity states. Ann. Rheum. Dis. 2018, 77, 1539–1540. [Google Scholar] [CrossRef]
- Twisk, J.W. Longitudinal data analysis. A comparison between generalized estimating equations and random coefficient analysis. Eur. J. Epidemiol. 2004, 19, 769–776. [Google Scholar] [CrossRef]
- Feltkamp, T.E.; Mardjuadi, A.; Huang, F.; Chou, C.T. Spondyloarthropathies in eastern Asia. Curr. Opin. Rheumatol. 2001, 13, 285–290. [Google Scholar] [CrossRef]
- Kim, T.J.; Kim, T.H. Clinical spectrum of ankylosing spondylitis in Korea. Joint Bone Spine 2010, 77, 23–240. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; De Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ ACC/ AACVPR/ AAPA/ ABC/ ACPM/ ADA/ AGS/ APhA/ ASPC/ NLA/ PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e285–e350. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S. Treat-to-target as an approach in inflammatory arthritis. Curr. Opin. Rheumatol. 2016, 28, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Arends, S.; van der Veer, E.; Kamps, F.B.; Houtman, P.M.; Bos, R.; Bootsma, H.; Brouwer, E.; Spoorenberg, A. Patient-tailored dose reduction of TNF-alpha blocking agents in ankylosing spondylitis patients with stable low disease activity in daily clinical practice. Clin. Exp. Rheumatol. 2015, 33, 174–180. [Google Scholar] [PubMed]
- Baraliakos, X.; Brandt, J.; Listing, J.; Haibel, H.; Sörensen, H.; Rudwaleit, M.; Sieper, J.; Braun, J. Outcome of patients with active ankylosing spondylitis after two years of therapy with etanercept: Clinical and magnetic resonance imaging data. Arthritis Rheum. 2005, 53, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Schramm-Luc, A.; Schramm, J.; Siedliński, M.; Guzik, T.J.; Batko, B. Age determines response to anti-TNFα treatment in patients with ankylosing spondylitis and is related to TNFα-producing CD8+ T cells. Clin. Rheumatol. 2018, 37, 1597–1604. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Results |
|---|---|
| Patient (male, %) | 139 (122, 87.8) |
| Age, years | 37.5 ± 10.8 |
| Disease duration | 9.9 ± 7.3 |
| HLA-B27 positive | 116/124 (93.5) |
| Uveitis | 40 (28.8) |
| ASDAS-CRP | 3.7 ± 0.8 |
| BASDAI (0–10) | 5.8 ± 1.2 |
| PhGA (0–10) | 6.3 ± 1.6 |
| PtGA (0–10) | 6.6 ± 1.7 |
| Spinal pain (0–10) | 6.5 ± 1.7 |
| BASFI (0–10) | 4.4 ± 2.2 |
| BASMI10 | 4.1 ± 2.3 |
| Chest expansion | 2.8 ± 1.3 |
| ESR (mm/h) | 36.3 ± 25.1 |
| CRP (mg/dL) | 2.5 ± 2.3 |
| Syndesmophytes (≥1) | 74 (53.2) |
| Used drugs | |
| Adalimumab | 54 (38.8) |
| Etanercept | 54 (38.8) |
| Golimumab | 20 (14.4) |
| Infliximab | 11 (7.9) |
| Variable | Univariable Model, OR (95% CI) | Univariable Model Adjusted for Age and Syndemophytes * | Multivariable Model, OR (95% CI) |
|---|---|---|---|
| Age, 10 years | 0.71 (0.54–0.92) | - | 0.67 (0.49–0.93) |
| Disease duration, years | 0.97 (0.93–1.00) | - | † |
| Sex, male | 0.67 (0.28–1.60) | - | † |
| HLA-B27 (+) | 0.68 (0.25–1.84) | - | † |
| Syndesmophytes (+) | 0.55 (0.32–0.97) | - | 0.75 (0.36–1.58) |
| Uveitis (+) | 0.83 (0.45–1.54) | - | † |
| Δ3Mo.ASDAS-CRP | 1.68 (1.17–2.40) | 1.57 (1.11–2.23) | 0.66 (0.37–1.15) |
| Δ3Mo.BASDAI | 1.76 (1.36–2.27) | 1.78 (1.40–2.26) | 1.70 (1.19–2.41) |
| Δ3Mo.PhGA | 1.47 (1.26–1.72) | 1.47 (1.26–1.71) | 1.28 (0.95–1.74) |
| Δ3Mo.PtGA | 1.38 (1.19–1.61) | 1.40 (1.21–1.63) | 1.16 (0.85–1.60) |
| Δ3Mo.Pain | 1.31 (1.12–1.52) | 1.32 (1.13–1.53) | 0.89 (0.67–1.18) |
| Δ3Mo.BASFI | 1.13 (0.95–1.34) | 1.15 (0.97–1.35) | † |
| Δ3Mo.BASMI10 | 1.31 (0.95–1.80) | 1.27 (0.92–1.75) | † |
| Δ3Mo.ChE | 1.15 (0.88–1.51) | 1.09 (0.83–1.42) | † |
| Δ3Mo.ESR | 1.01 (0.99–1.02) | 1.00 (0.99–1.01) | † |
| Δ3Mo.CRP | 1.06 (0.93–1.20) | 1.05 (0.94–1.18) | † |
| Normal 3Mo.ESR | 2.04 (0.92–4.55) | 1.66 (0.73–3.76) | † |
| Normal 3Mo.CRP | 2.03 (0.97–4.27) | 1.94 (0.90–4.15) | † |
| QIC of the model | 816.657 |
| Variable | Univariable Model, OR (95% CI) | Univariable Model Adjusted for Age * | Multivariable Model, OR (95% CI) |
|---|---|---|---|
| Age, 10 years | 0.76 (0.60–0.96) | - | 0.69 (0.54–0.89) |
| Disease duration, years | 0.99 (0.95–1.02) | - | † |
| Sex, male | 0.85 (0.41–1.75) | - | † |
| HLA-B27 (+) | 0.99 (0.33–2.93) | - | † |
| Syndesmophytes (+) | 0.82 (0.48–1.39) | - | † |
| Uveitis (+) | 0.90 (0.50–1.62) | - | † |
| Δ3Mo.ASDAS-CRP | 1.41 (1.01–1.99) | 1.37 (0.97–1.92) | 0.56 (0.30–1.03) |
| Δ3Mo.BASDAI | 1.64 (1.30–2.06) | 1.66 (1.32–2.10) | 2.00 (1.45–2.76) |
| Δ3Mo.PhGA | 1.23 (1.06–1.43) | 1.23 (1.06–1.42) | 1.04 (0.79–1.37) |
| Δ3Mo.PtGA | 1.18 (1.01–1.37) | 1.19 (1.04–1.38) | 0.91 (0.68–1.23) |
| Δ3Mo.Pain | 1.24 (1.08–1.43) | 1.25 (1.09–1.45) | 1.13 (0.86–1.48) |
| Δ3Mo.BASFI | 1.03 (0.89–1.20) | 1.05 (0.91–1.22) | † |
| Δ3Mo.BASMI10 | 1.25 (0.91–1.71) | 1.25 (0.92–1.69) | † |
| Δ3Mo.ChE | 1.11 (0.84–1.46) | 1.06 (0.80–1.41) | † |
| Δ3Mo.ESR | 1.01 (1.00–1.02) | 1.00 (0.99–1.02) | † |
| Δ3Mo.CRP | 1.06 (0.95–1.19) | 1.05 (0.94–1.16) | † |
| Normal 3Mo.ESR | 3.29 (1.45–7.46) | 2.87 (1.26–6.55) | ‡ |
| Normal 3Mo.CRP | 2.73 (1.32–5.62) | 2.56 (1.22–5.34) | 3.72 (1.39–9.95) |
| QIC of the model | 799.491 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, E.J.; Lee, W.K. Early Improvements in Disease Activity Indices Predict Long-Term Clinical Remission Suggested by the Treat-to-Target Strategy in Patients with Ankylosing Spondylitis Receiving TNF-α Inhibitor Treatment. J. Clin. Med. 2021, 10, 4279. https://doi.org/10.3390/jcm10184279
Nam EJ, Lee WK. Early Improvements in Disease Activity Indices Predict Long-Term Clinical Remission Suggested by the Treat-to-Target Strategy in Patients with Ankylosing Spondylitis Receiving TNF-α Inhibitor Treatment. Journal of Clinical Medicine. 2021; 10(18):4279. https://doi.org/10.3390/jcm10184279
Chicago/Turabian StyleNam, Eon Jeong, and Won Kee Lee. 2021. "Early Improvements in Disease Activity Indices Predict Long-Term Clinical Remission Suggested by the Treat-to-Target Strategy in Patients with Ankylosing Spondylitis Receiving TNF-α Inhibitor Treatment" Journal of Clinical Medicine 10, no. 18: 4279. https://doi.org/10.3390/jcm10184279