
Outbreaks of COVID-19 in Nursing Homes: A Cross-Sectional Survey of 74 Nursing Homes in a French Area

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context and Design
2.2. Content of the Survey
2.2.1. COVID-19 Cases and Populations of Analysis
2.2.2. Outbreaks
2.3. Statistical Analyses
2.4. Ethics, Patient and Public Involvement
3. Results
3.1. Nursing Homes Characteristics and Measures to Control the Epidemic
3.2. COVID-19 among Residents and Staff Members
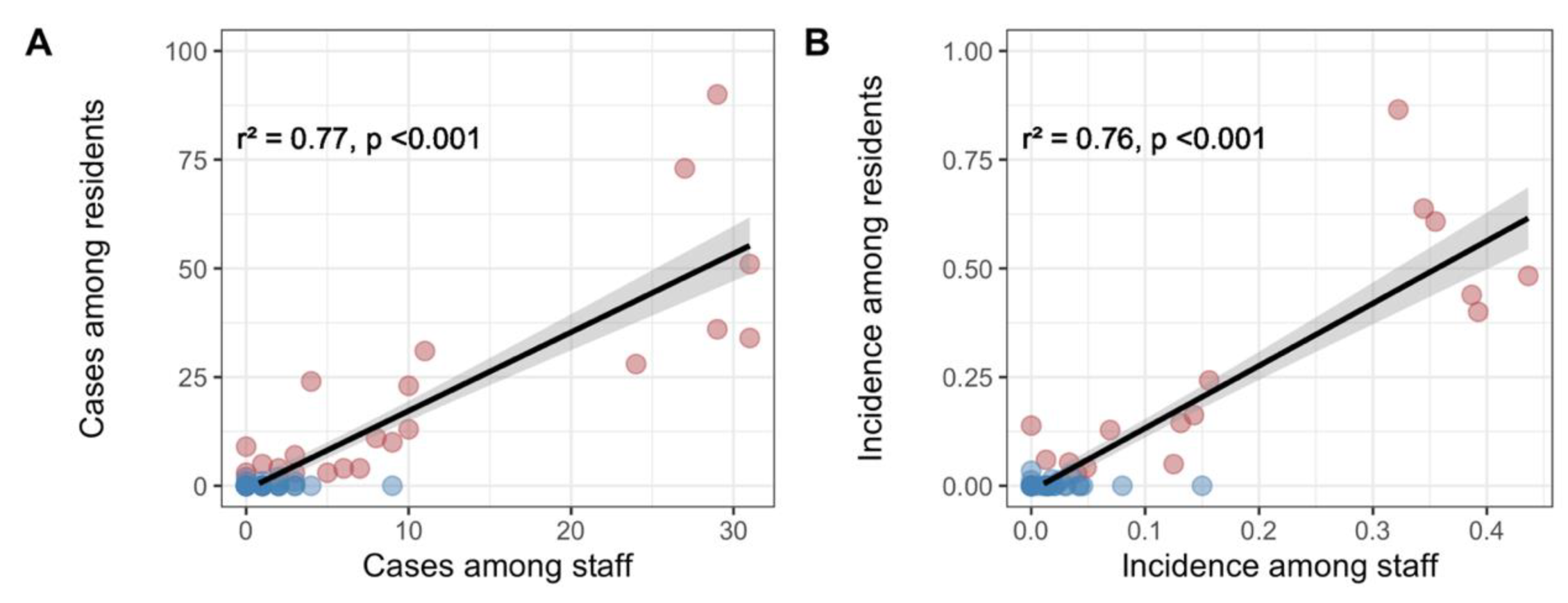
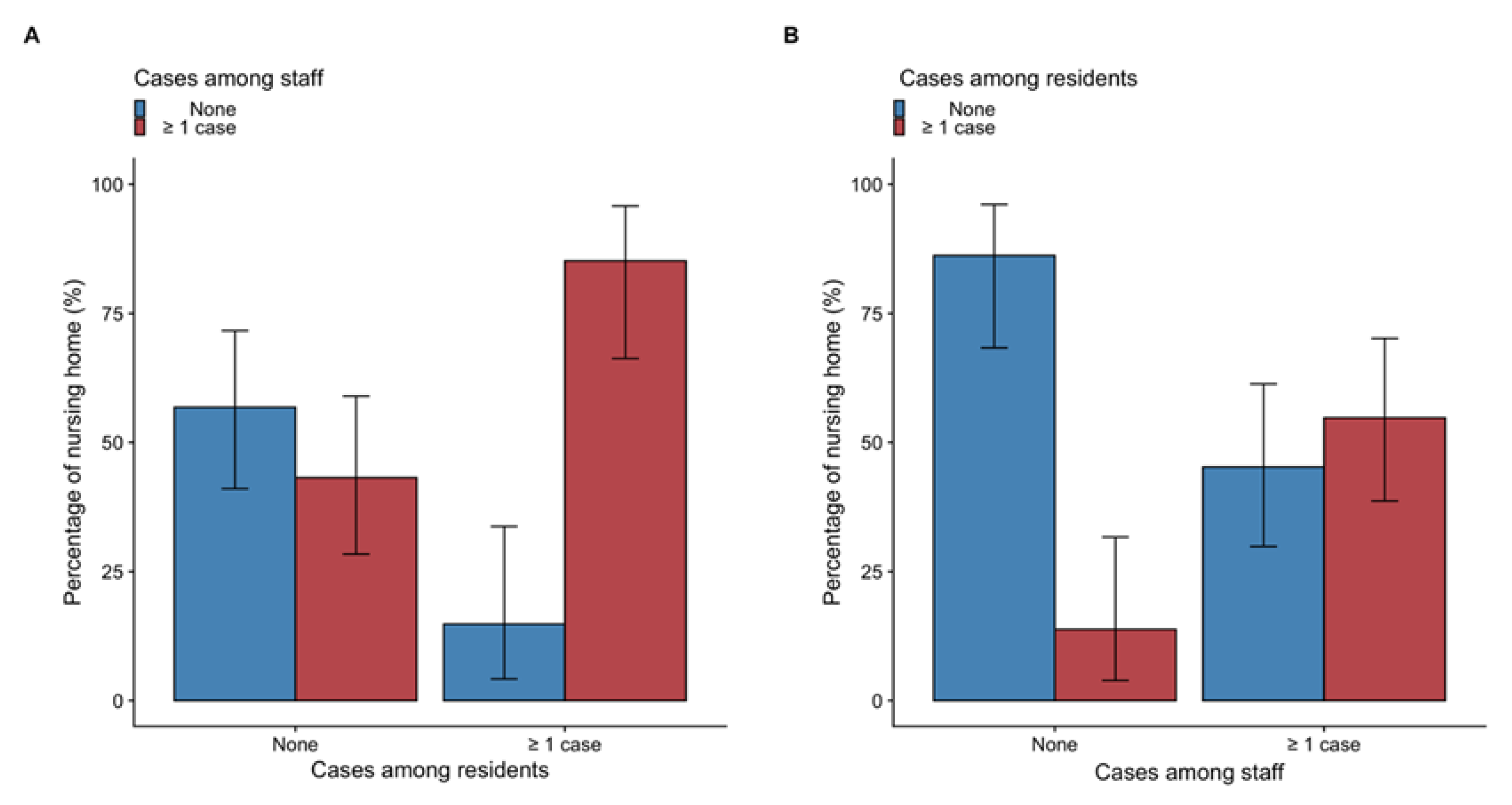
3.3. Relationship between Infections among Staff Members and Residents
3.4. Nursing Homes Organization and Occurrence of Outbreaks among Residents
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Approval
References
- Vestergaard, L.S.; Nielsen, J.; Richter, L.; Schmid, D.; Bustos, N.; Braeye, T.; Denissov, G.; Veideman, T.; Luomala, O.; Möttönen, T.; et al. Excess All-Cause Mortality during the COVID-19 Pandemic in Europe—Preliminary Pooled Estimates from the EuroMOMO Network, March to April 2020. Eurosurveillance 2020, 25, 2001214. [Google Scholar] [CrossRef]
- Salje, H.; Tran Kiem, C.; Lefrancq, N.; Courtejoie, N.; Bosetti, P.; Paireau, J.; Andronico, A.; Hozé, N.; Richet, J.; Dubost, C.-L.; et al. Estimating the Burden of SARS-CoV-2 in France. Science 2020, 369, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Burton, J.K.; Bayne, G.; Evans, C.; Garbe, F.; Gorman, D.; Honhold, N.; McCormick, D.; Othieno, R.; Stevenson, J.E.; Swietlik, S.; et al. Evolution and Effects of COVID-19 Outbreaks in Care Homes: A Population Analysis in 189 Care Homes in One Geographical Region of the UK. Lancet Healthy Longev. 2020, 1, e21–e31. [Google Scholar] [CrossRef]
- Brandén, M.; Aradhya, S.; Kolk, M.; Härkönen, J.; Drefahl, S.; Malmberg, B.; Rostila, M.; Cederström, A.; Andersson, G.; Mussino, E. Residential Context and COVID-19 Mortality among Adults Aged 70 Years and Older in Stockholm: A Population-Based, Observational Study Using Individual-Level Data. Lancet Healthy Longev. 2020, 1, e80–e88. [Google Scholar] [CrossRef]
- Shah, A.S.V.; Wood, R.; Gribben, C.; Caldwell, D.; Bishop, J.; Weir, A.; Kennedy, S.; Reid, M.; Smith-Palmer, A.; Goldberg, D.; et al. Risk of Hospital Admission with Coronavirus Disease 2019 in Healthcare Workers and Their Households: Nationwide Linkage Cohort Study. BMJ 2020, 371, m3582. [Google Scholar] [CrossRef]
- Blain, H.; Rolland, Y.; Schols, J.M.G.A.; Cherubini, A.; Miot, S.; O’Neill, D.; Martin, F.C.; Guérin, O.; Gavazzi, G.; Bousquet, J.; et al. August 2020 Interim EuGMS Guidance to Prepare European Long-Term Care Facilities for COVID-19. Eur. Geriatr. Med. 2020, 11, 899–913. [Google Scholar] [CrossRef]
- Telford, C.T. Preventing COVID-19 Outbreaks in Long-Term Care Facilities through Preemptive Testing of Residents and Staff Members—Fulton County, Georgia, March–May 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1296. [Google Scholar] [CrossRef]
- SPF COVID-19: Point Epidémiologique du 2 Juillet 2020. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/infection-a-coronavirus/documents/bulletin-national/covid-19-point-epidemiologique-du-2-juillet-2020 (accessed on 1 December 2020).
- Danis, K.; Epaulard, O.; Bénet, T.; Gaymard, A.; Campoy, S.; Botelho-Nevers, E.; Bouscambert-Duchamp, M.; Spaccaferri, G.; Ader, F.; Mailles, A.; et al. Cluster of Coronavirus Disease 2019 (COVID-19) in the French Alps, February 2020. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 825–832. [Google Scholar] [CrossRef] [Green Version]
- Le Vu, S.; Jones, G.; Anna, F.; Rose, T.; Richard, J.-B.; Bernard-Stoecklin, S.; Goyard, S.; Demeret, C.; Helynck, O.; Escriou, N.; et al. Prevalence of SARS-CoV-2 Antibodies in France: Results from Nationwide Serological Surveillance. Nat. Commun. 2021, 12, 3025. [Google Scholar] [CrossRef]
- Vitrat, V.; Maillard, A.; Raybaud, A.; Wackenheim, C.; Chanzy, B.; Nguyen, S.; Valran, A.; Bosch, A.; Noret, M.; Delory, T. Effect of Professional and Extra-Professional Exposure on Seroprevalence of SARS-CoV-2 Infection among Healthcare Workers of the French Alps: A Multicentric Cross-Sectional Study. Vaccines 2021, 9, 824. [Google Scholar] [CrossRef]
- French Government Instruction (DGCS/SD3/DSS/SD1 N°2013/418) Related to the Assessment of Loss of Autonomy of Residents Living in Nursing Homes. 2013. Available online: http://affairesjuridiques.aphp.fr/textes/circulaire-interministerielle-n-dgcssd3dsssd12013418-du-6-decembre2013-relative-a-la-mise-en-oeuvre-du-decret-n-2013-22-du-8-janvier-2013-relatif-a-levaluation-et-a-la-vali/?pdf=612743 (accessed on 1 December 2020).
- Aguilova, L.; Sauzéon, H.; Balland, É.; Consel, C.; N’Kaoua, B. AGGIR scale: A contribution to specifying the needs of disabled elders. Rev. Neurol. (Paris) 2014, 170, 216–221. [Google Scholar] [CrossRef]
- Vetel, J.M.; Leroux, R.; Ducoudray, J.M. AGGIR. Practical use. Geriatric Autonomy Group Resources Needs. Soins. Gerontol. 1998, 13, 23–27. [Google Scholar]
- WHO COVID-19 Case Definition. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Surveillance_Case_Definition-2020.1 (accessed on 9 December 2020).
- Graham, N.S.N.; Junghans, C.; Downes, R.; Sendall, C.; Lai, H.; McKirdy, A.; Elliott, P.; Howard, R.; Wingfield, D.; Priestman, M.; et al. SARS-CoV-2 Infection, Clinical Features and Outcome of COVID-19 in United Kingdom Nursing Homes. J. Infect. 2020, 81, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Annweiler, C.; Sacco, G.; Salles, N.; Aquino, J.-P.; Gautier, J.; Berrut, G.; Guérin, O.; Gavazzi, G. National French Survey of COVID-19 Symptoms in People Aged 70 and Over. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020. [Google Scholar] [CrossRef]
- Yanes-Lane, M.; Winters, N.; Fregonese, F.; Bastos, M.; Perlman-Arrow, S.; Campbell, J.R.; Menzies, D. Proportion of Asymptomatic Infection among COVID-19 Positive Persons and Their Transmission Potential: A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0241536. [Google Scholar] [CrossRef]
- Mehta, H.B.; Li, S.; Goodwin, J.S. Risk Factors Associated With SARS-CoV-2 Infections, Hospitalization, and Mortality Among US Nursing Home Residents. JAMA Netw. Open 2021, 4, e216315. [Google Scholar] [CrossRef]
- Sablerolles, R.S.G.; Lafeber, M.; van Kempen, J.A.L.; van de Loo, B.P.A.; Boersma, E.; Rietdijk, W.J.R.; Polinder-Bos, H.A.; Mooijaart, S.P.; van der Kuy, H.; Versmissen, J.; et al. Association between Clinical Frailty Scale Score and Hospital Mortality in Adult Patients with COVID-19 (COMET): An International, Multicentre, Retrospective, Observational Cohort Study. Lancet Healthy Longev. 2021, 2, e163–e170. [Google Scholar] [CrossRef]
- Lombardo, F.L.; Bacigalupo, I.; Salvi, E.; Lacorte, E.; Piscopo, P.; Mayer, F.; Ancidoni, A.; Remoli, G.; Bellomo, G.; Losito, G.; et al. The Italian National Survey on Coronavirus Disease 2019 Epidemic Spread in Nursing Homes. Int. J. Geriatr. Psychiatry 2021, 36, 873–882. [Google Scholar] [CrossRef]
- Boëlle, P.-Y.; Delory, T.; Maynadier, X.; Janssen, C.; Piarroux, R.; Pichenot, M.; Lemaire, X.; Baclet, N.; Weyrich, P.; Melliez, H.; et al. Trajectories of Hospitalization in COVID-19 Patients: An Observational Study in France. J. Clin. Med. 2020, 9, 3148. [Google Scholar] [CrossRef]
- Canouï-Poitrine, F.; Rachas, A.; Thomas, M.; Carcaillon-Bentata, L.; Fontaine, R.; Gavazzi, G.; Laurent, M.; Robine, J.-M. Magnitude, Change over Time, Demographic Characteristics and Geographic Distribution of Excess Deaths among Nursing Home Residents during the First Wave of COVID-19 in France: A Nationwide Cohort Study. Age Ageing 2021, afab098. [Google Scholar] [CrossRef]
- SPF Influenza Activity in France, Season 2018–2019. BEH 2019, 28, 552–563.
- Poltavskiy, E.; Alishahi Tabriz, A.; Romano, P.S.; Bang, H.; Kshirsagar, A.V. Predicting COVID-19 at Skilled Nursing Facilities in California: Do the Stars Align? BMJ Open Qual. 2021, 10, e001099. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Li, Y.; Fang, F. Is There a Link between Nursing Home Reported Quality and COVID-19 Cases? Evidence from California Skilled Nursing Facilities. J. Am. Med. Dir. Assoc. 2020, 21, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Tulloch, J.S.P.; Green, R.; Tunnah, C.; Coffey, E.; Ashton, M.; Ghebrehewet, S. COVID-19 Outbreaks in Care Homes during the First Wave: Are Care Quality Commission Ratings a Good Predictor of at-Risk Homes? J. Hosp. Infect. 2021, 111, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Abrams, H.R.; Loomer, L.; Gandhi, A.; Grabowski, D.C. Characteristics of U.S. Nursing Homes with COVID-19 Cases. J. Am. Geriatr. Soc. 2020, 68, 1653–1656. [Google Scholar] [CrossRef]
- Chen, A.T.; Yun, H.; Ryskina, K.L.; Jung, H.-Y. Nursing Home Characteristics Associated With Resident COVID-19 Morbidity in Communities With High Infection Rates. JAMA Netw. Open 2021, 4, e211555. [Google Scholar] [CrossRef] [PubMed]
- Janssen, C.; Maillard, A.; Bodelet, C.; Claudel, A.-L.; Gaillat, J.; Delory, T. Hesitancy towards COVID-19 Vaccination among Healthcare Workers: A Multi-Centric Survey in France. Vaccines 2021, 9, 547. [Google Scholar] [CrossRef]
- Fritch, W.M.; Agnew, J.; Rosman, L.; Cadorette, M.A.; Barnett, D.J. Application of the Haddon Matrix to COVID-19 Prevention and Containment in Nursing Homes. J. Am. Geriatr. Soc. 2021. [Google Scholar] [CrossRef] [PubMed]
- CDC Infection Prevention and Control Assessment Tool for Nursing Homes Preparing for COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/assessment-tool-for-nursing-homes.html (accessed on 18 August 2021).
- Miller, K.E.M.; Gorges, R.J.; Konetzka, R.T.; Van Houtven, C.H. The Metrics Matter: Improving Comparisons of COVID-19 Outbreaks in Nursing Homes. J. Am. Med. Dir. Assoc. 2021, 22, 955–959.e3. [Google Scholar] [CrossRef]
- Cai, S.; Yan, D.; Intrator, O. COVID-19 Cases and Death in Nursing Homes: The Role of Racial and Ethnic Composition of Facilities and Their Communities. J. Am. Med. Dir. Assoc. 2021, 22, 1345–1351. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| NHs’ Characteristics, n (%) or Median [IQR] | All NH n = 74 | Outbreak-Free NH n = 51 | Outbreak NH * n = 22 |
|---|---|---|---|
| Presence of coordinating physician | 63 (85.1%) | 43 (82.7%) | 20 (90.9%) |
| Private nursing home | 26 (35.1%) | 14 (26.9%) | 12 (54.5%) |
| NHs’ status | |||
| Private associative NHs | 18 (24.7%) | 13 (25.0%) | 5 (23.8%) |
| Private commercial NHs | 5 (6.8%%) | 1 (1.9%) | 4 (19.0%) |
| Public hospital NHs | 28 (38.4%) | 22 (42.3%) | 6 (28.6%) |
| Public territorial NHs | 20 (27.4%) | 16 (30.8%) | 4 (19.0%) |
| Others | 2 (2.7%) | 0 (0.0%) | 2 (9.5%) |
| Agreement with an infection control team | 71 (95.9%) | 50 (96.2%) | 21 (95.5%) |
| Number of residents a | 74.5 [60.2, 83.5] | 71.0 [54.8, 82.5] | 77.5 [72.0, 83.5] |
| Number of dementia places | 14.0 [0.0, 24.0] | 12.5 [0.0, 22.0] | 14.0 [2.0, 26.0] |
| Twin bedrooms ≥ 1 | 22 (30.1%) | 15 (29.4%) | 7 (31.8%) |
| Turnover rate b | 2.5 [0.0, 6.4] | 2.5 [0.0, 7.2] | 2.0 [0.0, 4.8] |
| Morbidity score, as per GMP c | 780.0 [746.8, 819.0] | 783.0 [746.8, 818.8] | 776.5 [751.0, 820.8] |
| Dependence score, as per PMP d | 227.0 [206.0, 244.0] | 230.0 [206.2, 248.8] | 219.0 [201.0, 239.5] |
| Number of staff e | 65.0 [48.0, 78.5] | 64.0 [48.0, 76.5] | 67.5 [54.5, 80.8] |
| Number of fulltime caregiver per 100 residents e | |||
| Nurse | 4.4 [3.6, 6.0] | 4.3 [3.2, 6.0] | 4.9 [4.0, 6.0] |
| Assistant nurse | 16.0 [11.5, 21.8] | 16.0 [9.4, 22.0] | 16.0 [12.0, 19.8] |
| Other caregivers | 10.0 [7.0, 15.0] | 10.5 [7.1, 16.0] | 10.0 [7.0, 13.0] |
| Use of interim manpower | 49 (68.1%) | 36 (72.0%) | 13 (59.1%) |
| Use of other sources of on-demand manpower | 57 (78.1%) | 38 (74.5%) | 19 (86.4%) |
| Preventive measures implemented | |||
| Days between national decision and visits’ ban | 0 days [−2.5, 1.5] | 0.5 days [−2.8, 2.0] | 0 days [−2.0, 1.0] |
| Days between national lockdown and systematic face mask wear | −6.0 days [−15.2, 0.2] | −6.5 days [−17.5, 1.0] | −5.0 days [−13.2, 0.0] |
| Replacement of the facial mask every 4 h | 44 (59.5%) | 31 (59.6%) | 13 (59.1%) |
| Individual lockdown of residents’ in their room | 62 (86.1%) | 42 (82.4%) | 20 (95.2%) |
| Corrective measures implemented | |||
| Intervention of the infection control team | 65 (91.5%) | 43 (87.8%) | 22 (100.0%) |
| Systematic screening of all staff using RT-PCR for COVID-19 | 46 (63.0%) | 28 (54.9%) | 18 (81.8%) |
| All NH n = 74 | Outbreak-Free NH n = 51 | Outbreak NH * n = 22 | p-Value | |
|---|---|---|---|---|
| Residents | ||||
| Number of residents | 5891 | 4096 | 1795 | |
| Incidence of COVID-19 among residents | 482 (8.2%) | 9 (0.2%) | 473 (26.4%) | <0.001 |
| Hospitalization rate | 588 (10.0%) | 247 (6.0%) | 341 (19.0%) | <0.001 |
| Mortality rate | 503 (8.5%) | 250 (6.1%) | 253 (14.1%) | <0.001 |
| Staff | ||||
| Number of staff | 4652 | 3304 | 1348 | |
| Incidence of COVID-19 among staff members | 296 (6.4%) | 46 (1.4%) | 250 (18.5%) | <0.001 |
| Facilities with ≥1cases among staff members | 42 (56.8%) | 23 (44.2%) | 19 (86.4%) | <0.001 |
| Characteristics | Outbreak-Free NH | Outbreak NH | Univariate | Bivariate | ||||
|---|---|---|---|---|---|---|---|---|
| n = 51 | n = 22 | OR | 95% CI | p-Value | aOR * | 95% | p-Value | |
| Cases ≥ 1 among the staff | 23 (46.0) | 19 (90.5) | 11.23 | 2.35–53.63 | 0.002 | - | - | - |
| NHs’ characteristics | ||||||||
| Presence of coordinating physician | 43 (82.7) | 20 (90.9) | 1.90 | 0.37–9.80 | 0.441 | - | - | - |
| High number of residents (>80) | 15 (28.8) | 7 (31.8) | 1.20 | 0.40–3.57 | 0.743 | 0.87 | 0.26–2.89 | 0.817 |
| Presence of dementia places | 35 (70.0) | 16 (72.7) | 0.99 | 0.32–3.08 | 0.987 | 0.61 | 0.16–2.33 | 0.473 |
| Twin bedrooms ≥ 1 | 15 (29.4) | 7 (31.8) | 1.17 | 0.39–3.47 | 0.782 | 0.88 | 0.26–2.97 | 0.843 |
| High turnover rate (>2%) | 35 (70.0) | 13 (59.1) | 0.62 | 0.22–1.76 | 0.368 | 0.33 | 0.09–1.28 | 0.110 |
| High dependence level (GMP a score > 80) | 24 (52.2) | 8 (40.0) | 0.61 | 0.21–1.77 | 0.365 | 0.72 | 0.22–2.37 | 0.592 |
| High morbidity level (PMP b score > 225) | 23 (54.8) | 8 (42.1) | 0.60 | 0.20–1.80 | 0.362 | 0.65 | 0.20–2.16 | 0.481 |
| High total number of staff (>60) | 26 (55.3) | 13 (65.0) | 1.50 | 0.51–4.43 | 0.463 | 0.93 | 0.28–3.16 | 0.911 |
| High number of fulltime caregiver (>40 per 100 residents) | 32 (72.7) | 10 (62.5) | 0.63 | 0.19–2.10 | 0.447 | 0.55 | 0.15–2.05 | 0.376 |
| Use of interim manpower | 36 (72.0) | 13 (59.1) | 0.58 | 0.20–1.65 | 0.307 | 0.41 | 0.11–1.47 | 0.172 |
| Use of other sources of on-demand manpower | 38 (74.5) | 19 (86.4) | 2.23 | 0.56–8.77 | 0.253 | 1.29 | 0.28–6.05 | 0.744 |
| Preventive measures implemented | ||||||||
| Early ban of visits (before the national decision) | 15 (32.6) | 8 (38.1) | 1.23 | 0.42–3.61 | 0.706 | 0.66 | 0.20–2.24 | 0.506 |
| Early systematic facial mask wearing (before the national lockdown) | 34 (68.0) | 15 (68.2) | 0.97 | 0.33–2.88 | 0.962 | 1.01 | 0.30–3.36 | 0.987 |
| Replacement of the face mask every 4 h | 31 (59.6) | 13 (59.1) | 0.96 | 0.35–2.67 | 0.942 | 1.26 | 0.40–3.99 | 0.698 |
| Confining residents’ in their room | 42 (82.4) | 20 (95.2) | 4.50 | 0.53–38.04 | 0.167 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piet, E.; Maillard, A.; Mallaval, F.O.; Dusseau, J.Y.; Galas-Haddad, M.; Ducki, S.; Creton, H.; Lallemant, M.; Forestier, E.; Gavazzi, G.; et al. Outbreaks of COVID-19 in Nursing Homes: A Cross-Sectional Survey of 74 Nursing Homes in a French Area. J. Clin. Med. 2021, 10, 4280. https://doi.org/10.3390/jcm10184280
Piet E, Maillard A, Mallaval FO, Dusseau JY, Galas-Haddad M, Ducki S, Creton H, Lallemant M, Forestier E, Gavazzi G, et al. Outbreaks of COVID-19 in Nursing Homes: A Cross-Sectional Survey of 74 Nursing Homes in a French Area. Journal of Clinical Medicine. 2021; 10(18):4280. https://doi.org/10.3390/jcm10184280
Chicago/Turabian StylePiet, Emilie, Alexis Maillard, Franck Olivier Mallaval, Jean Yves Dusseau, Murielle Galas-Haddad, Sébastien Ducki, Hélène Creton, Marc Lallemant, Emmanuel Forestier, Gaëtan Gavazzi, and et al. 2021. "Outbreaks of COVID-19 in Nursing Homes: A Cross-Sectional Survey of 74 Nursing Homes in a French Area" Journal of Clinical Medicine 10, no. 18: 4280. https://doi.org/10.3390/jcm10184280