

Total Antioxidant Capacity in Obese and Non-Obese Subjects and Its Association with Anthropo-Metabolic Markers: Systematic Review and Meta-Analysis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Information Sources and Search Strategy
2.3. Eligibility Criteria
2.4. Data Extraction
2.5. Assessment of Risk of Bias
2.6. Data Analysis
3. Results
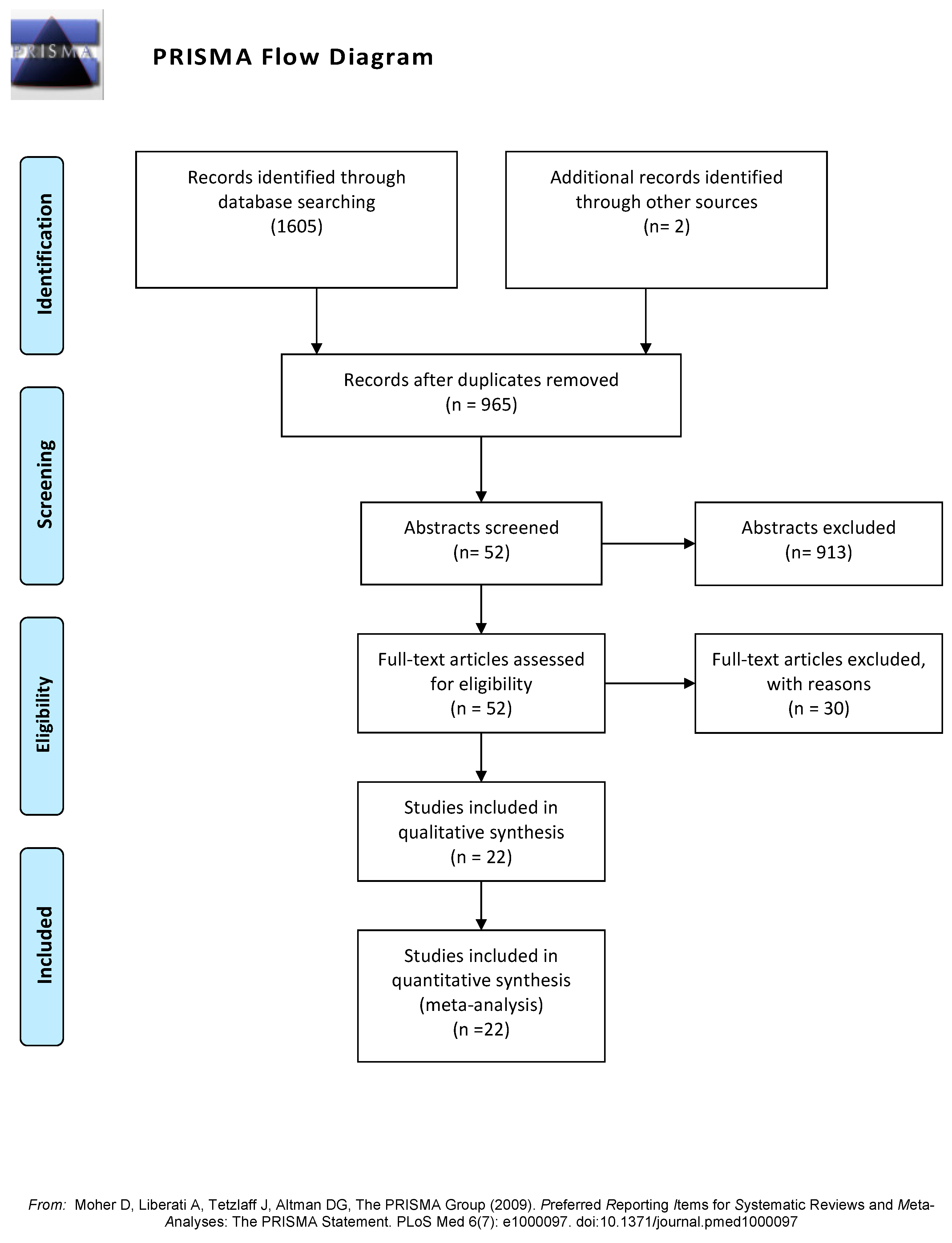
3.1. Study Selection

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year of Publication) | Country of the Sample | Sample Size (n) | Proportion of SO:NW | Mean Age (Years) at Inclusion | Mean BMI | Proportion of Male:Female | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| SO | NW | Total | SO | NW | SO | NW | ||||
| Amirkhizi (2010) [25] | Iran | 25 | 79 | 104 | 0.24:0.76 | 39 | 27 | 33.6 | 23.4 | 0:1 |
| Asghari (2021) [26] | Iran | 140 | 90 | 230 | 0.61:0.39 | 41 | 40.2 | 32.3 | 23.6 | 0.58:0.42 |
| Aslan (2017) [27] | Turkey | 27 | 26 | 53 | 0.51:0.49 | 30 | 28 | 36.31 | 36.31 | 0.58:0.42 |
| Aysegül (2014) * [28] | Turkey | 38 | 51 | 89 | 0.43:0.57 | 9.42 | 9.29 | 27.63 | 17.42 | 0.52:0.48 |
| Chen (2014) & [11] | China | 31 | 30 | 61 | 0.51:0.49 | 44.9 | 44.03 | 28.9 | 22.7 | 1:0 |
| Chrysohoou (2007) [10] | Greece | 540 | 1226 | 1766 | 0.31:0.69 | 50 | 41 | - | - | 0.40:0.60 |
| Dambal (2011) [29] | India | 50 | 50 | 100 | 0.5:0.5 | - | - | - | - | 0.40:0.60 |
| Dursun (2016) [30] | Turkey | 20 | 20 | 40 | 0.5:0.5 | 27.9 | 26.11 | 34.08 | 22.15 | 0:1 |
| Eren (2014) [12] | Turkey | 95 | 56 | 151 | 0.63:0.37 | 13.34 | 13.95 | 31.14 | 18.85 | 0.43:0.57 |
| Faienza (2012) † [31] | Italy | 55 | 30 | 85 | 0.65:0.35 | 11.4 | 10.4 | 2.22 | 0.37 | 0.51:0.49 |
| García-Sánchez (2020) [32] | Mexico | 33 | 23 | 56 | 0.59:0.41 | 56.45 | 68.7 | - | - | 0.25:0.75 |
| Hadžović-Džuvo (2015) [33] | Herzegovina and Bosnia | 23 | 36 | 59 | 0.39:0.61 | - | - | - | - | 0:1 |
| Karaouzene (2011) [34] | Algeria | 85 | 120 | 205 | 0.41:0.59 | 48 | 46 | 33.2 | 23.5 | 1:0 |
| Lejawa (2021) [13] | Poland | 49 | 49 | 98 | 0.5:0.5 | 30.5 | 30.9 | 32.6 | 23.36 | 1: 0 |
| Mahasneh (2016) [35] | USA | 35 | 46 | 81 | 0.43:0.57 | - | - | - | - | 0:1 |
| Matusik (2015) * † [36] | Poland | 78 | 82 | 160 | 0.49:0.51 | 13.96 | 13.72 | 2.96 | 0.38 | 0.52:0.48 |
| Park (2016) & [37] | Korea | 33 | 45 | 78 | 0.42:0.58 | 65.3 | 66.6 | 26.3 | 22.5 | 0.55:0.45 |
| Pirgon (2013) [38] | Turkey | 46 | 29 | 75 | 0.61:0.39 | 12.5 | 12.7 | 30.63 | 18.36 | 0.48:0.52 |
| Rowicka (2017) + [39] | Polonia | 62 | 21 | 83 | 0.75:0.25 | 7.5 | 6.4 | 23.5 | 19.5 | 0.39:0.61 |
| Skalicky (2008) [40] | Czech Republic | 40 | 48 | 88 | 0.45:0.55 | 50 | 52.12 | 35.3 | 21.86 | 0.52:0.48 |
| Sonoli (2015) [41] | India | 70 | 35 | 105 | 0.67:0.33 | 23.1 | 22.9 | 31.38 | 23.07 | 0.5:0.5 |
| Vehapoglu (2016) * [42] | Turkey | 90 | 80 | 170 | 0.53:0.47 | 7.4 | 7.2 | 25.78 | 16.75 | 0.47:0.53 |
| Reason for Non-Inclusion | Number of Articles |
|---|---|
| The inclusion of overweight subjects within the SO group | 5 |
| The inclusion of overweight subjects within the NW group | 4 |
| All included patients had type 2 diabetes | 4 |
| The sample size was lower than 20 by group | 4 |
| No comparison of SO versus NW, instead there was a comparison of metabolic syndrome versus non-metabolic syndrome | 4 |
| Studies performed in patients with polycystic ovary syndrome | 2 |
| Article written in Turkish | 1 |
| Duplicated publication, data were published previously | 1 |
| Low score on the Newcastle–Ottawa scale | 1 |
| TAC was measured in seminal fluid | 1 |
| The sample size was lower than 20 by group and Newcastle–Ottawa score was 5. | 1 |
| The study groups were prediabetes versus normal fasting glycemia; thus, patients were not classified as SO and NW | 1 |
| No comparison of TAC in SO versus NW, instead authors compare men versus women | 1 |

3.2. Risk of Bias of the Included Studies
3.3. Synthesis of the Studies
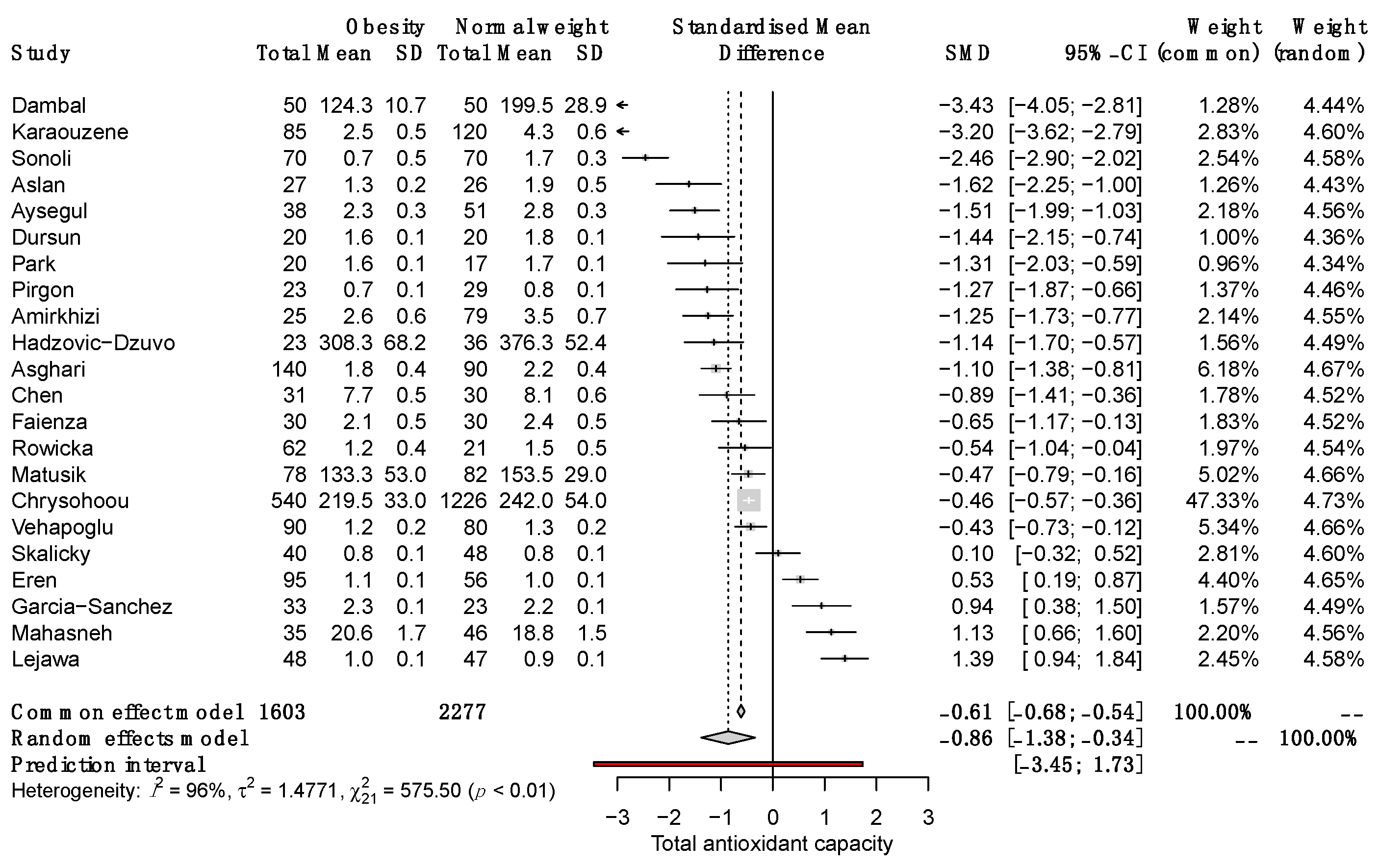
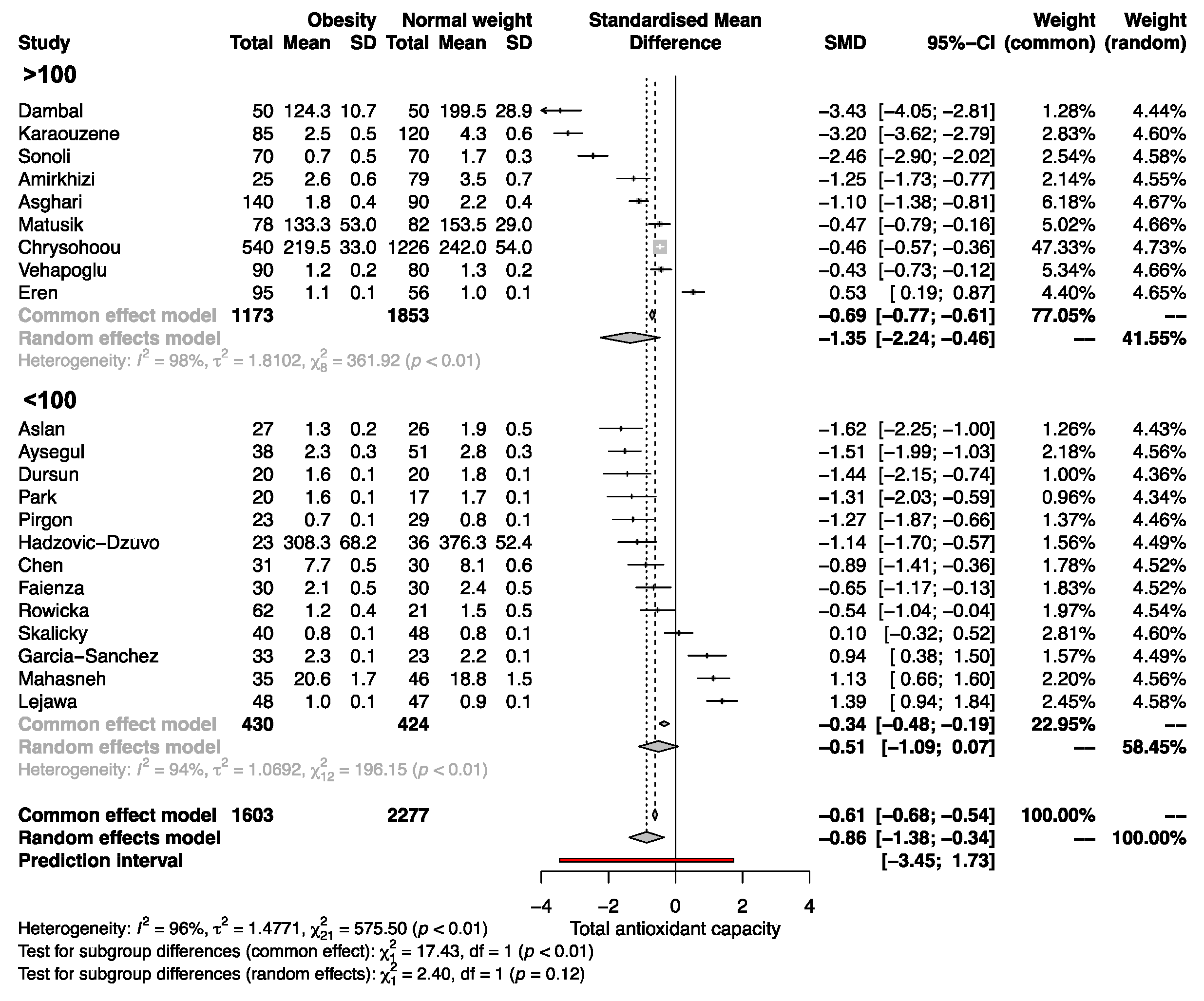
3.4. Differences in Total Antioxidant Capacity among SO and NW
3.5. Correlations of TAC with Anthropometric and Metabolic Parameters
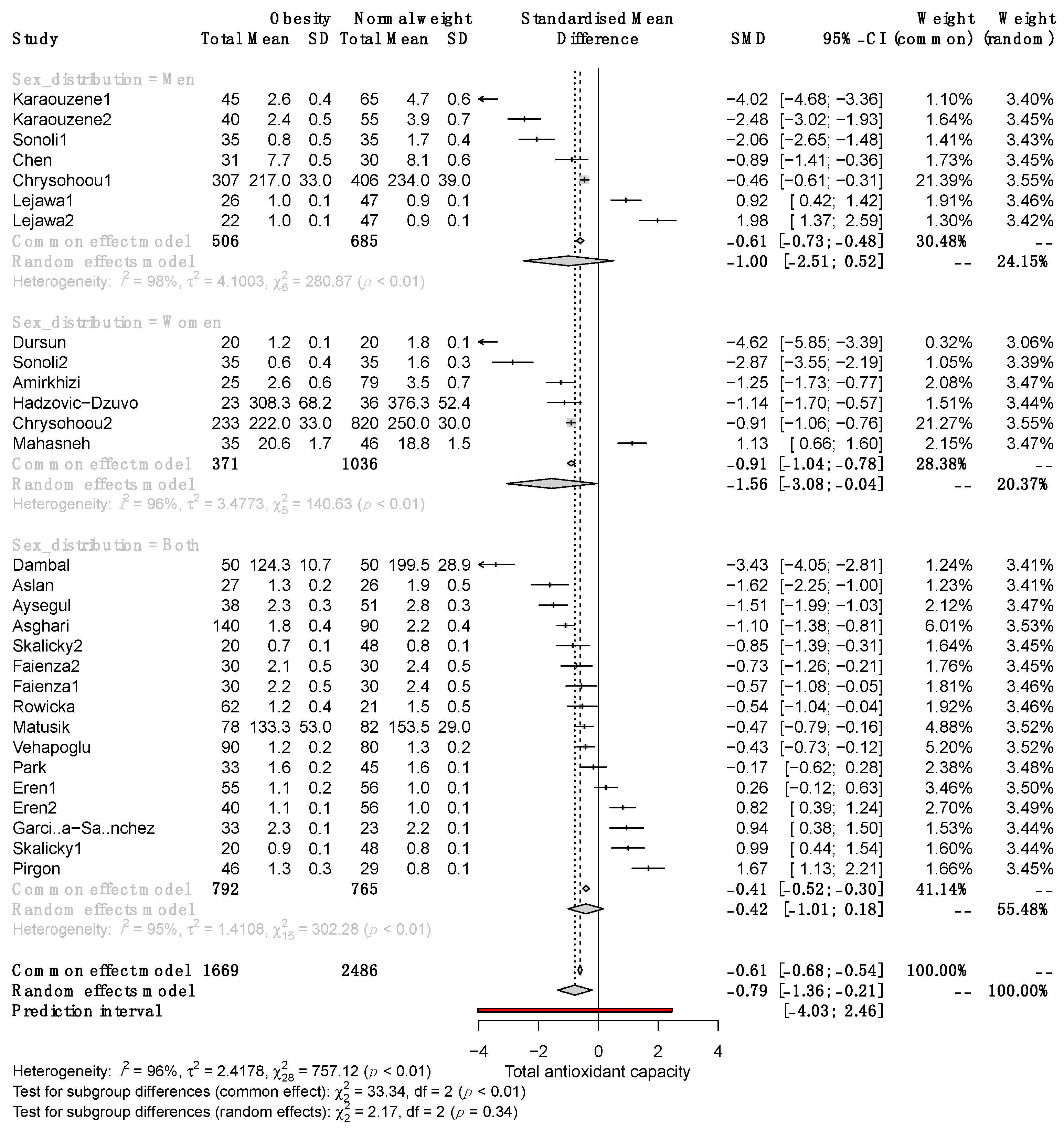
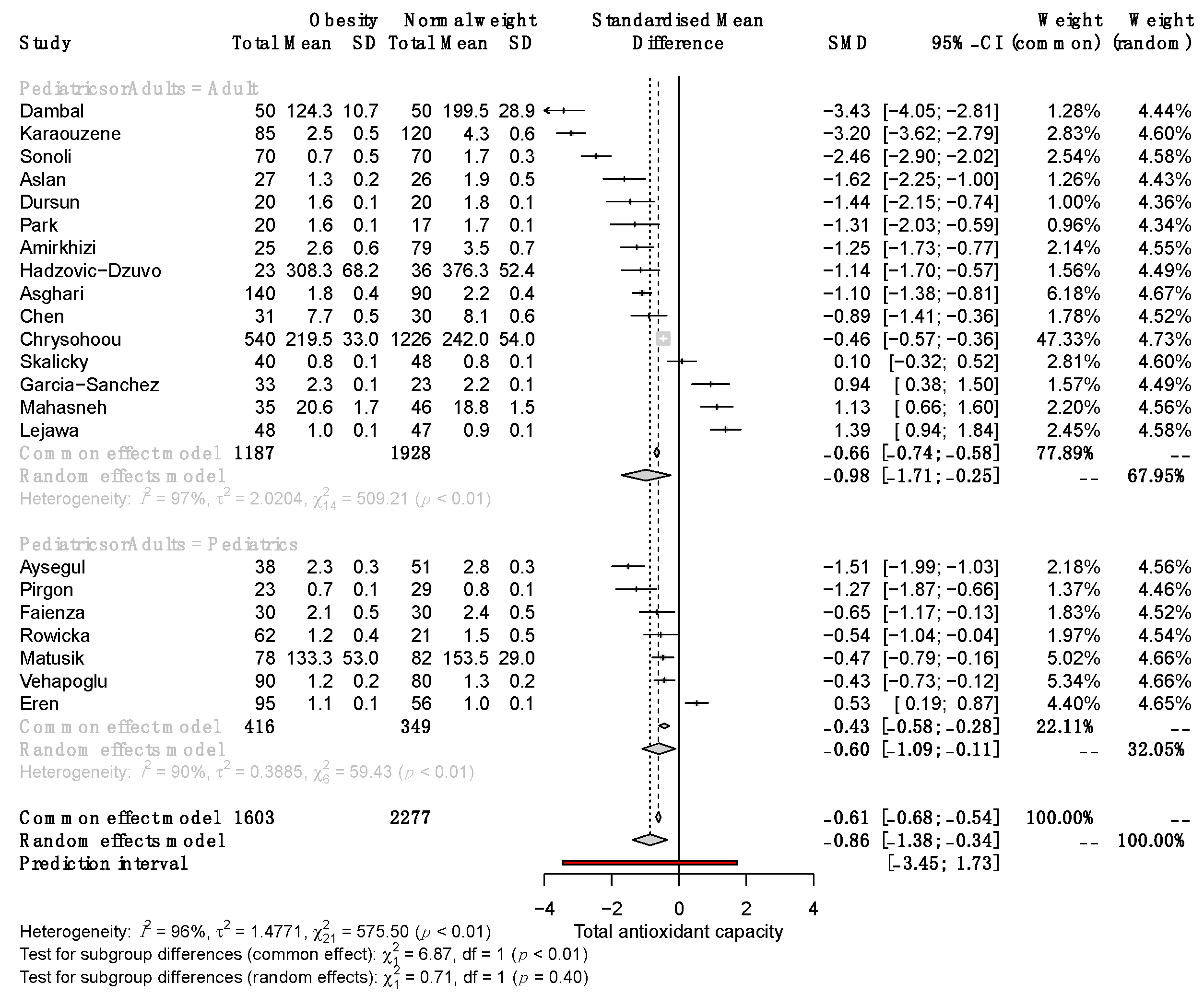
3.6. Subgroup Analysis by Sex, Age, Methods Used for Determining Serum TAC, and Study Sample Size
3.7. Other Oxidative-Stress-Related Parameters and Their Correlation with Anthropo-Metabolic Parameters
3.8. Heterogeneity, Variability Analysis, and Publication Bias
4. Discussion
4.1. Main Findings
4.2. Clinical Implications
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cervantes Gracia, K.; Llanas-Cornejo, D.; Husi, H. CVD and Oxidative Stress. J. Clin. Med. 2017, 6, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajam, Y.A.; Rani, R.; Ganie, S.Y.; Sheikh, T.A.; Javaid, D.; Qadri, S.S.; Pramodh, S.; Alsulimani, A.; Alkhanani, M.F.; Harakeh, S.; et al. Oxidative Stress in Human Pathology and Aging: Molecular Mechanisms and Perspectives. Cells 2022, 11, 552. [Google Scholar] [CrossRef] [PubMed]
- Ito, F.; Sono, Y.; Ito, T. Measurement and Clinical Significance of Lipid Peroxidation as a Biomarker of Oxidative Stress: Oxidative Stress in Diabetes, Atherosclerosis, and Chronic Inflammation. Antioxidants 2019, 8, 72. [Google Scholar] [CrossRef] [Green Version]
- Birben, E.; Sahiner, U.M.; Sackesen, C.; Erzurum, S.; Kalayci, O. Oxidative Stress and Antioxidant Defense. World Allergy Organ J. 2012, 5, 9–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubio, C.P.; Hernández-Ruiz, J.; Martinez-Subiela, S.; Tvarijonaviciute, A.; Ceron, J.J. Spectrophotometric assays for total antioxidant capacity (TAC) in dog serum: An update. BMC Vet. Res. 2016, 12, 166. [Google Scholar] [CrossRef] [Green Version]
- Bartosz, G. Non-enzymatic antioxidant capacity assays: Limitations of use in biomedicine. Free Radic. Res. 2010, 44, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Solis-Paredes, J.M.; Montoya-Estrada, A.; Cruz-Rico, A.; Reyes-Muñoz, E.; Perez-Duran, J.; Espino y Sosa, S.; Garcia-Salgado, V.R.; Sevilla-Montoya, R.; Martinez-Portilla, R.J.; Estrada-Gutierrez, G.; et al. Plasma Total Antioxidant Capacity and Carbonylated Proteins Are Increased in Pregnant Women with Severe COVID-19. Viruses 2022, 14, 723. [Google Scholar] [CrossRef]
- Yaghoubi, N.; Youssefi, M.; Jabbari Azad, F.; Farzad, F.; Yavari, Z.; Zahedi Avval, F. Total antioxidant capacity as a marker of severity of COVID-19 infection: Possible prognostic and therapeutic clinical application. J. Med. Virol. 2022, 94, 1558. [Google Scholar] [CrossRef]
- Pieme, C.A.; Tatangmo, J.A.; Simo, G.; Biapa Nya, P.C.; Ama Moor, V.J.; Moukette Moukette, B.; Tankeu Nzufo, F.; Njinkio Nono, B.L.; Sobngwi, E. Relationship between hyperglycemia, antioxidant capacity and some enzymatic and non-enzymatic antioxidants in African patients with type 2 diabetes. BMC Res. Notes 2017, 10, 141. [Google Scholar] [CrossRef] [Green Version]
- Chrysohoou, C.; Panagiotakos, D.B.; Pitsavos, C.; Skoumas, I.; Papademetriou, L.; Economou, M.; Stefanadis, C. The implication of obesity on total antioxidant capacity in apparently healthy men and women: The ATTICA study. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Sun, L.; Gao, H.; Ren, L.; Liu, N.; Song, G. Visfatin and oxidative stress influence endothelial progenitor cells in obese populations. Endocr. Res. 2015, 40, 83–87. [Google Scholar] [CrossRef]
- Eren, E.; Abuhandan, M.; Solmaz, A.; Taşkın, A. Serum paraoxonase/arylesterase activity and oxidative stress status in children with metabolic syndrome. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 163–168. [Google Scholar] [CrossRef]
- Lejawa, M.; Osadnik, K.; Osadnik, T.; Pawlas, N. Association of Metabolically Healthy and Unhealthy Obesity Phenotypes with Oxidative Stress Parameters and Telomere Length in Healthy Young Adult Men. Analysis of the MAGNETIC Study. Antioxidants 2021, 10, 1350. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, T.I.A.; Martinez, A.R.; Jørgensen, T.S.H. Epidemiology of Obesity. In From Obesity to Diabetes; Handbook of Experimental Pharmacology; Eckel, J., Clément, K., Eds.; Springer: Cham, Switzerland, 2022; Volume 274, pp. 3–27. [Google Scholar]
- Thomas-Valdés, S.; Tostes, M.D.G.V.; Anunciação, P.C.; da Silva, B.P.; Sant’Ana HM, P. Association between vitamin deficiency and metabolic disorders related to obesity. Crit. Rev. Food Sci. Nutr. 2017, 57, 3332–3343. [Google Scholar] [CrossRef]
- Engin, A. Fat Cell and Fatty Acid Turnover in Obesity. In Obesity and Lipotoxicity; Advances in Experimental Medicine and Biology; Springer: Cham, Switzerland, 2017; Volume 960, pp. 135–160. [Google Scholar]
- Engin, A. Endothelial Dysfunction in Obesity. In Obesity and Lipotoxicity; Advances in Experimental Medicine and Biology; Springer: Cham, Switzerland, 2017; Volume 960, pp. 345–379. [Google Scholar]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol.-Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity: Implications for metabolic syndrome, diabetes, hypertension, dyslipidemia, atherosclerosis, and cancer. Obes. Res. Clin. Pract. 2013, 7, e330–e341. [Google Scholar] [CrossRef] [PubMed]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021, 156, 787–788. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2021. Available online: http://www.evidencebasedpublichealth.de/download/Newcastle_Ottowa_Scale_Pope_Bruce.pdf (accessed on 21 October 2022).
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Fixed-Effect Versus Random-Effects Models. In Introduction to Meta-Analysis; John Wiley & Sons Ltd.: Chichester, UK, 2009; Volume 2, pp. 77–86. [Google Scholar]
- Borenstein, M.; Higgins, J.P.T.; Hedges, L.V.; Rothstein, H.R. Basics of meta-analysis: I2 is not an absolute measure of heterogeneity. Res. Synth. Methods 2017, 8, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Amirkhizi, F.; Siassi, F.; Djalali, M.; Foroushani, A.R. Evaluation of oxidative stress and total antioxidant capacity in women with general and abdominal adiposity. Obes. Res. Clin. Pract. 2010, 4, e209–e216. [Google Scholar] [CrossRef]
- Asghari, S.; Hamedi-Shahraki, S.; Amirkhizi, F. Vitamin D status and systemic redox biomarkers in adults with obesity. Clin. Nutr. ESPEN 2021, 45, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Aslan, M.; Duzenli, U.; Esen, R.; Soyoral, Y.U. Serum prolidase enzyme activity in obese subjects and its relationship with oxidative stress markers. Clin. Chim. Acta 2017, 473, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Demir, A.D.; Erenberk, U.; Özgen, I.T.; Özkaya, E.; Türkmen, A.V.; Dündaröz, M.R.; Erel, Ö. Total antioxidant and oxidant status in obese children without insulin resistance. Dicle Med. J. 2014, 41, 257–261. [Google Scholar] [CrossRef]
- Dambal, S.S.; Indumati, V.; Kumari, S. Role of oxidative stress in obesity with and insight into type II diabetes mellitus. JCDR. 2011, 5, 52–54. [Google Scholar]
- Dursun, E.; Akalin, F.A.; Genc, T.; Cinar, N.; Erel, O.; Yildiz, B.O. Oxidative stress and periodontal disease in obesity. Medicine 2016, 95, e3136. [Google Scholar] [CrossRef]
- Faienza, M.F.; Francavilla, R.; Goffredo, R.; Ventura, A.; Marzano, F.; Panzarino, G.; Marinelli, G.; Cavallo, L.; Di Bitonto, G. Oxidative Stress in Obesity and Metabolic Syndrome in Children and Adolescents. Horm. Res. Paediatr. 2012, 78, 158–164. [Google Scholar] [CrossRef]
- García-Sánchez, A.; Gámez-Nava, J.I.; Díaz-de la Cruz, E.N.; Cardona-Muñoz, E.G.; Becerra-Alvarado, I.N.; Aceves-Aceves, J.A.; Sánchez-Rodríguez, E.N.; Miranda-Díaz, A.G. The Effect of Visceral Abdominal Fat Volume on Oxidative Stress and Proinflammatory Cytokines in Subjects with Normal Weight, Overweight and Obesity. Diabetes Metab. Syndr. Obes. 2020, 13, 1077–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadžović-Džuvo, A.; Valjevac, A.; Lepara, O.; Čustović, S.; Vatreš, A.; Agačević, A.; Rahmanović, S.; Zukić, S. Obesity is associated with decreased total antioxidant capacity in apparently healthy postmenopausal women. Folia Medica Fac. Med. Univ. Saraev. 2015, 50, 101–106. [Google Scholar]
- Karaouzene, N.; Merzouk, H.; Aribi, M.; Merzouk, S.A.; Berrouiguet, A.Y.; Tessier, C.; Narce, M. Effects of the association of aging and obesity on lipids, lipoproteins and oxidative stress biomarkers: A comparison of older with young men. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 792–799. [Google Scholar] [CrossRef]
- Mahasneh, A.A.; Zhang, Y.; Zhao, H.; Ambrosone, C.B.; Hong, C.C. Lifestyle predictors of oxidant and antioxidant enzyme activities and total antioxidant capacity in healthy women: A cross-sectional study. J. Physiol. Biochem. 2016, 72, 745–762. [Google Scholar] [CrossRef]
- Matusik, P.; Prokopowicz, Z.; Norek, B.; Olszanecka-Glinianowicz, M.; Chudek, J.; Malecka-Tendera, E. Oxidative/Antioxidative Status in Obese and Sport Trained Children: A Comparative Study. BioMed. Res. Int. 2015, 2015, 315747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.H.; Lee, E.; Park, E. Effect of Pumpkin, Corn Silk, Adzuki Bean, and Their Mixture on Weight Control and Antioxidant Activities in High Fat Diet-Induced Obesity Rats. J. Korean Soc. Food Sci. Nutr. 2016, 45, 1239–1248. [Google Scholar] [CrossRef]
- Pirgon, O.; Hüseyin, B.; Ferhat, Ç.; Hüseyin, K.; Nuri, D.B. Association Between Insulin Resistance and Oxidative Stress Parameters in Obese Adolescents with Non-Alcoholic Fatty Liver Disease. J. Clin. Res. Pediatr. Endocrinol. 2013, 5, 33–39. [Google Scholar] [PubMed]
- Rowicka, G.; Dyląg, H.; Ambroszkiewicz, J.; Riahi, A.; Weker, H.; Chełchowska, M. Total Oxidant and Antioxidant Status in Prepubertal Children with Obesity. Oxid. Med. Cell. Longev. 2017, 2017, 5621989. [Google Scholar] [CrossRef] [Green Version]
- Skalicky, J.; Muzakova, V.; Kandar, R.; Meloun, M.; Rousar, T.; Palicka, V. Evaluation of oxidative stress and inflammation in obese adults with metabolic syndrome. Clin. Chem. Lab. Med. 2008, 46, 495–505. [Google Scholar] [CrossRef]
- Sonoli, S.S.; Kothiwale, V.A.; Malleshappa, A. A Cross Sectional Study to assess Oxidative Stress, Ceruloplasmin and Physical Activity Status in Healthy Obese Young Adults. Indian J. Public Health Res. Dev. 2015, 6, 214. [Google Scholar] [CrossRef]
- Vehapoglu, A.; Turkmen, S.; Goknar, N.; Özer, Ö.F. Reduced antioxidant capacity and increased subclinical inflammation markers in prepubescent obese children and their relationship with nutritional markers and metabolic parameters. Redox Rep. 2016, 21, 271–280. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 7, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [Green Version]
- Talegawkar, S.A.; Beretta, G.; Yeum, K.J.; Johnson, E.J.; Carithers, T.C.; Taylor, H.A., Jr.; Russell, R.M.; Tucker, K.L. Total Antioxidant Performance Is Associated with Diet and Serum Antioxidants in Participants of the Diet and Physical Activity Substudy of the Jackson Heart Study. J. Nutr. 2009, 139, 1964–1971. [Google Scholar] [CrossRef] [Green Version]
- Fabbrini, E.; Serafini, M.; Colic Baric, I.; Hazen, S.L.; Klein, S. Effect of Plasma Uric Acid on Antioxidant Capacity, Oxidative Stress, and Insulin Sensitivity in Obese Subjects. Diabetes 2014, 63, 976–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asbaghi, O.; Ghanavati, M.; Ashtary-Larky, D.; Bagheri, R.; Rezaei Kelishadi, M.; Nazarian, B.; Nordvall, M.; Wong, A.; Dutheil, F.; Suzuki, K.; et al. Effects of Folic Acid Supplementation on Oxidative Stress Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antioxidants 2021, 10, 871. [Google Scholar] [CrossRef] [PubMed]
- Nälsén, C.; Öhrvall, M.; Kamal-Eldin, A.; Vessby, B. Plasma antioxidant capacity among middle-aged men: The contribution of uric acid. Scand J. Clin. Lab. Investig. 2006, 66, 239–248. [Google Scholar] [CrossRef]
- Rospleszcz, S.; Dermyshi, D.; Müller-Peltzer, K.; Strauch, K.; Bamberg, F.; Peters, A. Association of serum uric acid with visceral, subcutaneous and hepatic fat quantified by magnetic resonance imaging. Sci. Rep. 2020, 10, 442. [Google Scholar] [CrossRef] [Green Version]
- Sautin, Y.Y.; Johnson, R.J. Uric acid: The oxidant-antioxidant paradox. Nucleosides Nucleotides Nucleic Acids 2008, 27, 608–619. [Google Scholar] [CrossRef] [Green Version]
- Yang, R.; Le, G.; Li, A.; Zheng, J.; Shi, Y. Effect of antioxidant capacity on blood lipid metabolism and lipoprotein lipase activity of rats fed a high-fat diet. Nutrition 2006, 22, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, A.; Korac, A.; Buzadzic, B.; Otasevic, V.; Stancic, A.; Daiber, A.; Korac, B. Redox implications in adipose tissue (dys)function—A new look at old acquaintances. Redox Biol. 2015, 6, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Marseglia, L.; Manti, S.; D’Angelo, G.; Nicotera, A.; Parisi, E.; Di Rosa, G.; Gitto, E.; Arrigo, T. Oxidative stress in obesity: A critical component in human diseases. Int. J. Mol. Sci. 2014, 16, 378–400. [Google Scholar] [CrossRef] [Green Version]
- Masschelin, P.M.; Cox, A.R.; Chernis, N.; Hartig, S.M. The Impact of Oxidative Stress on Adipose Tissue Energy Balance. Front. Physiol. 2020, 10, 448358. [Google Scholar] [CrossRef]




| Study | Selection | Comparability | Exposure | Stars | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Is the Case Definition Adequate? | Representativeness of the Cases | Selection of Controls | Definition of Controls | Comparability of Cases and Controls on the Basis of the Design or Analysis (Age/Other) | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Non-Response Rate | ||
| Asghari [26] | 2021 | * | * | * | * | * | * | * | * | * | 9 |
| Chen [11] | 2014 | * | * | * | * | * | * | * | * | * | 9 |
| Dambal [29] | 2011 | * | - | * | * | - | - | * | * | * | 6 |
| Dursun [30] | 2016 | * | - | * | - | * | * | * | * | * | 7 |
| Eren [12] | 2014 | * | * | * | * | * | * | * | * | * | 9 |
| Faienza [31] | 2012 | * | * | * | * | * | * | * | * | * | 9 |
| Karaouzene [34] | 2010 | * | * | * | * | * | * | * | * | * | 9 |
| Lejawa [13] | 2021 | * | * | * | * | * | * | * | * | * | 9 |
| Matusik [36] | 2015 | * | * | * | * | * | * | * | * | * | 9 |
| Aslan [28] | 2017 | * | * | * | * | * | * | * | * | * | 9 |
| Park [37] | 2016 | * | * | * | * | * | * | * | * | * | 9 |
| Pirgon [38] | 2013 | * | * | * | * | * | * | * | * | * | 9 |
| Rowwicka [39] | 2017 | * | * | * | * | * | - | * | * | * | 8 |
| Skalicky [40] | 2008 | * | * | * | * | * | * | * | * | * | 9 |
| Sonoli [41] | 2015 | * | * | * | * | * | - | * | * | * | 9 |
| Amirkhizi [25] | 2010 | * | * | * | * | * | - | * | * | * | 8 |
| Chrysohoou [10] | 2007 | * | * | * | * | * | - | * | * | * | 8 |
| García Sánchez [32] | 2020 | * | * | * | * | * | * | * | * | * | 9 |
| Hadžović-Džuvo [33] | 2015 | * | * | * | * | * | - | * | * | * | 8 |
| Mahasneh [35] | 2016 | * | * | * | * | * | * | * | * | * | 9 |
| Vehapoglu [42] | 2016 | * | * | * | * | * | - | * | * | * | 8 |
| Ayşegül [28] | 2014 | * | * | * | * | - | - | * | * | * | 7 |
| Parameter | n | Pooled Correlations (Random Effects Model) | I2 |
|---|---|---|---|
| Age | 718 | 0.01 (−0.11; 0.13) | 61% |
| Weight | 1870 | −0.17 (−0.27; −0.06) | 78% |
| Waist circumference | 1929 | −0.10 (−0.32; 0.13) | 84% |
| Hip circumference | 1766 | −0.11 (−0.21; −0.01) | 77% |
| Waist-to-hip ratio | 2805 | −0.03 (−0.18; 0.12) | 87% |
| BMI | 3166 | 0.03 (−0.11;0.17) | 89% |
| Adipose-visceral index | 520 | 0.29 (0.03; 0.51) | 86% |
| Total cholesterol | 678 | 0.13 (−0.03; 0.27) | 71% |
| C-reactive protein | 351 | 0.19 (−0.15; 0.49) | 91% |
| HDL-c | 678 | −0.16 (−0.31; 0.01) | 74% |
| LDL-c | 678 | 0.11 (−0.00; 0.21) | 48% |
| Triglycerides | 678 | 0.25 (0.02; 0.45) | 85% |
| Aspartate aminotransferase | 173 | 0.41 (0.28; 0.53) | 0% |
| Alanine aminotransferase | 173 | 0.38 (0.25; 0.50) | 0% |
| Fasting plasma glucose | 678 | 0.05 (−0.03; 0.12) | 0% |
| HOMA-IR | 245 | 0.32 (−0.63; 0.89) | 98% |
| Insulin | 245 | 0.28 (−0.61; 0.86) | 98% |
| Uric acid | 520 | 0.53 (0.26; 0.72) | 90% |
| Diastolic blood pressure | 595 | 0.05 (−0.14; 0.24) | 78% |
| Systolic blood pressure | 595 | 0.13 (−0.15; 0.38) | 89% |
| Ceruloplasmin | 140 | −0.12 (−0.28; 0.05) | 0% |
| Total | 19,201 |
| Covariate | Estimate | 95% CI | p-Value | R2 (%) * | |
|---|---|---|---|---|---|
| Sex female | 0.0986 | 1.5050 | 1.7023 | 0.9040 | 100.0 |
| Asian continent | 1.4377 | −0.4697 | 3.3451 | 0.1396 | |
| European continent | 1.8341 | −0.0275 | 3.6957 | 0.0535 | |
| BMI | −0.0315 | −0.1857 | 0.1227 | 0.6890 | |
| Age | −0.0003 | 0.0150 | 0.0144 | 0.9698 | |
| Altitude | −0.0001 | −0.0029 | 0.0001 | 0.7924 | |
| Method of TAC quantification: reduction of Cu+2 to Cu+1 | −68.0922 | −83.3645 | −52.8199 | <0.0001 ** | |
| Method of TAC quantification: Enzymatic reaction of peroxides and peroxidases (TBM) | −0.5555 | 1.4932 | −2.6042 | 0.5951 | |
| Intercept | −0.9830 | −5.3560 | 3.3901 | 0.6595 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anaya-Morua, W.; Villafan-Bernal, J.R.; Ramírez-Moreno, E.; García-Ortiz, H.; Martínez-Portilla, R.J.; Contreras-Cubas, C.; Martínez-Hernández, A.; Centeno-Cruz, F.; Pedroza-Montoya, F.E.; Orozco, L.; et al. Total Antioxidant Capacity in Obese and Non-Obese Subjects and Its Association with Anthropo-Metabolic Markers: Systematic Review and Meta-Analysis. Antioxidants 2023, 12, 1512. https://doi.org/10.3390/antiox12081512
Anaya-Morua W, Villafan-Bernal JR, Ramírez-Moreno E, García-Ortiz H, Martínez-Portilla RJ, Contreras-Cubas C, Martínez-Hernández A, Centeno-Cruz F, Pedroza-Montoya FE, Orozco L, et al. Total Antioxidant Capacity in Obese and Non-Obese Subjects and Its Association with Anthropo-Metabolic Markers: Systematic Review and Meta-Analysis. Antioxidants. 2023; 12(8):1512. https://doi.org/10.3390/antiox12081512
Chicago/Turabian StyleAnaya-Morua, Wendoline, José Rafael Villafan-Bernal, Esther Ramírez-Moreno, Humberto García-Ortiz, Raigam Jafet Martínez-Portilla, Cecilia Contreras-Cubas, Angélica Martínez-Hernández, Federico Centeno-Cruz, Florencia Estefana Pedroza-Montoya, Lorena Orozco, and et al. 2023. "Total Antioxidant Capacity in Obese and Non-Obese Subjects and Its Association with Anthropo-Metabolic Markers: Systematic Review and Meta-Analysis" Antioxidants 12, no. 8: 1512. https://doi.org/10.3390/antiox12081512