
Benefits of Natural Antioxidants on Oral Health

 , , , , , , , ,
, , , , , , , ,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
1.1. Green Tea
1.2. Curcumin
1.3. Resveratrol
1.4. Vitamins
1.5. Aloe Vera
1.6. Propolis
2. Materials and Methods
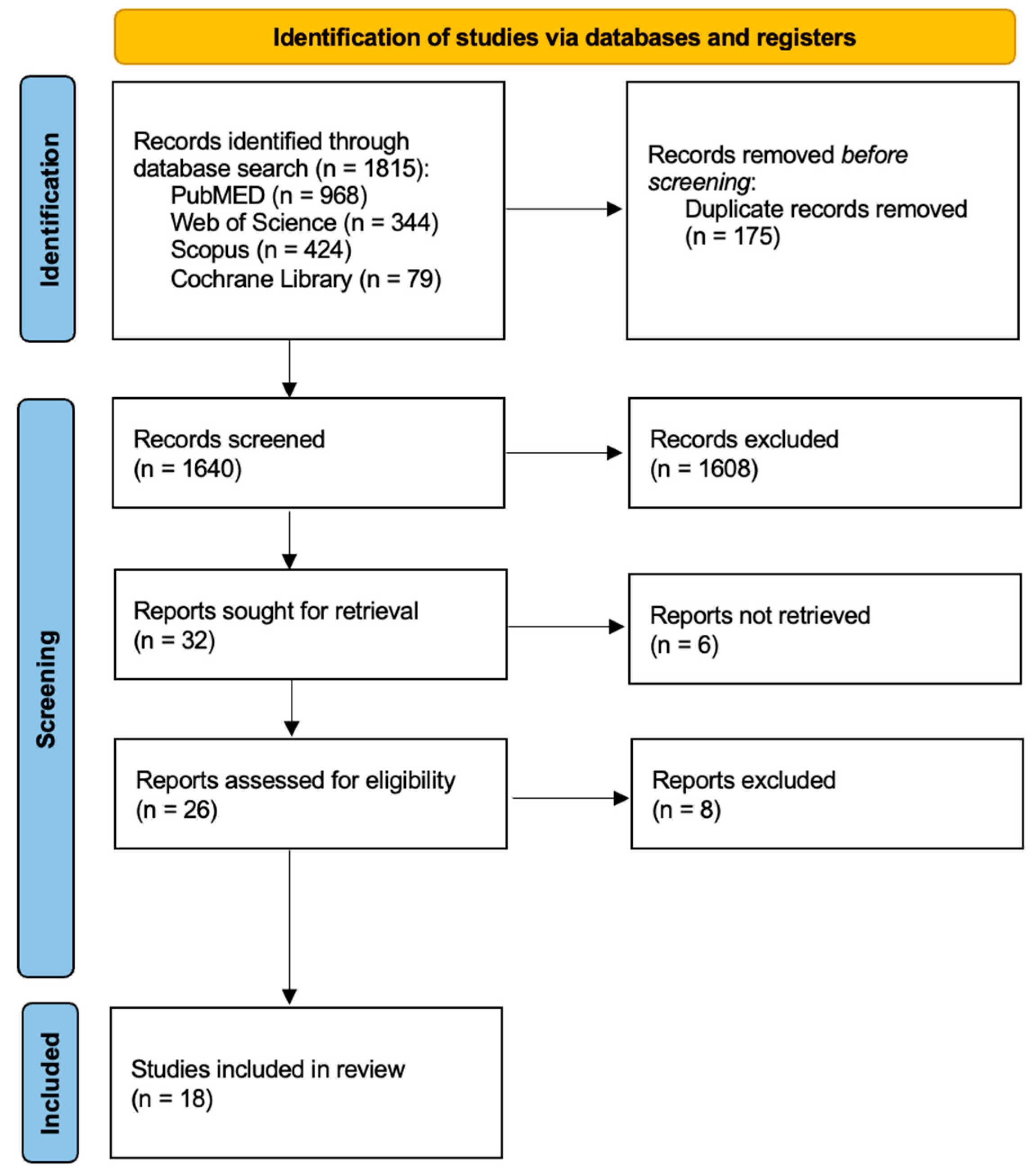
2.1. Search Processing
2.2. Inclusion Criteria
3. Results
4. Discussion
4.1. Periodontal Health
4.2. Mucositis
4.3. Oral Submucosa Fibrosis
4.4. Candidiasis
4.5. Caries
4.6. Oral Lichen Planus
4.7. Oral Potentially Malignant Disorders
5. Limits
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ROS | Reactive Oxygen Species |
| GT | Green tea |
| CUM | Curcumin |
| RSV | Resveratrol |
| PFs | Polyphenols |
| EGCG | Epigallocatechin-3-gallate |
| EGC | Epigallocatechin |
| TNF-alpha | Tumour necrosis factor alpha |
| AHH | Arryl hydrocarbon hydroxylase |
| DTD | DT-diaphorase |
| GST | glutathione-S-transferase |
| UDP-GT | UDP-glucuronyl transferase |
| CGFs | Platelet-containing growth factor concentrates |
| PVL | Panton–Valentine’s leucocidin |
| IU | International units |
| SBI | Sulcus bleeding index |
| PD | Probing depth |
| CAL | Clinical attachment level |
| PI | Plaque index |
| GI | Gingival index |
| BOP | Bleeding on probing |
| OHI | Oral hygiene index |
| PPD | Probing pocked depth |
| IL-1 | Interleukin 1 |
| CELC | Vitamin C, vitamin E, lysozyme, and carbazochrome |
| GBR | Guided bone regeneration |
| GSE | Grape seed extract |
| SRP | Scaling and root planing |
| RAL | Relative attachment level |
| OLP | Oral lichen planus |
| OPMDs | Oral potentially malignant disorders |
| OSF | Oral submucous fibrosis |
| CAPE | Caffeic-acid-phenethyl-ester |
| DCs | Diene conjugates |
| MDA | Malonic dialdehyde |
| CP | Chronic periodontitis |
| IL-6 | Interleukin 6 |
| PGE2 | Prostalgandin E2 |
| gCP | Generalised chronic periodontitis |
| WHO | World Health Organization |
| PM | Peri-implant mucositis |
| CFU/mL | Colony-forming units per millilitre |
References
- Lennicke, C.; Cochemé, H.M. Redox Metabolism: ROS as Specific Molecular Regulators of Cell Signaling and Function. Mol. Cell 2021, 81, 3691–3707. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, H.; Aulehla, A. Revisiting the Role of Metabolism during Development. Development 2018, 145, dev131110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antunes, F.; Brito, P.M. Quantitative Biology of Hydrogen Peroxide Signaling. Redox Biol. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ch, R.; Rey, G.; Ray, S.; Jha, P.K.; Driscoll, P.C.; Dos Santos, M.S.; Malik, D.M.; Lach, R.; Weljie, A.M.; MacRae, J.I.; et al. Rhythmic Glucose Metabolism Regulates the Redox Circadian Clockwork in Human Red Blood Cells. Nat. Commun. 2021, 12, 377. [Google Scholar] [CrossRef] [PubMed]
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martín, C. Pathophysiology of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef]
- Kempf, A.; Song, S.M.; Talbot, C.B.; Miesenböck, G. A Potassium Channel β-Subunit Couples Mitochondrial Electron Transport to Sleep. Nature 2019, 568, 230–234. [Google Scholar] [CrossRef]
- Holmström, K.M.; Finkel, T. Cellular Mechanisms and Physiological Consequences of Redox-Dependent Signalling. Nat. Rev. Mol. Cell Biol. 2014, 15, 411–421. [Google Scholar] [CrossRef]
- Tossetta, G.; Fantone, S.; Giannubilo, S.R.; Marzioni, D. The Multifaced Actions of Curcumin in Pregnancy Outcome. Antioxidants 2021, 10, 126. [Google Scholar] [CrossRef]
- Caponio, G.R.; Noviello, M.; Calabrese, F.M.; Gambacorta, G.; Giannelli, G.; De Angelis, M. Effects of Grape Pomace Polyphenols and In Vitro Gastrointestinal Digestion on Antimicrobial Activity: Recovery of Bioactive Compounds. Antioxidants 2022, 11, 567. [Google Scholar] [CrossRef]
- Dominguez-Bello, M.G.; Godoy-Vitorino, F.; Knight, R.; Blaser, M.J. Role of the Microbiome in Human Development. Gut 2019, 68, 1108–1114. [Google Scholar] [CrossRef] [Green Version]
- Gao, L.; Xu, T.; Huang, G.; Jiang, S.; Gu, Y.; Chen, F. Oral Microbiomes: More and More Importance in Oral Cavity and Whole Body. Protein Cell 2018, 9, 488–500. [Google Scholar] [CrossRef] [Green Version]
- Altomare, R.; Cacciabaudo, F.; Damiano, G.; Palumbo, V.D.; Gioviale, M.C.; Bellavia, M.; Tomasello, G.; Lo Monte, A.I. The Mediterranean Diet: A History of Health. Iran. J. Public Health 2013, 42, 449–457. [Google Scholar]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Almas, K. The Role of Nutrition in Periodontal Health: An Update. Nutrients 2016, 8, 530. [Google Scholar] [CrossRef] [Green Version]
- Arora, I.; Sharma, M.; Tollefsbol, T.O. Combinatorial Epigenetics Impact of Polyphenols and Phytochemicals in Cancer Prevention and Therapy. Int. J. Mol. Sci. 2019, 20, 4567. [Google Scholar] [CrossRef] [Green Version]
- Carlos-Reyes, Á.; López-González, J.S.; Meneses-Flores, M.; Gallardo-Rincón, D.; Ruíz-García, E.; Marchat, L.A.; Astudillo-de la Vega, H.; Hernández de la Cruz, O.N.; López-Camarillo, C. Dietary Compounds as Epigenetic Modulating Agents in Cancer. Front. Genet. 2019, 10, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, D.M.; Nannapaneni, S.; Patel, M.R.; Shi, Q.; Liu, Y.; Chen, Z.; Chen, A.Y.; El-Deiry, M.W.; Beitler, J.J.; Steuer, C.E.; et al. Phase Ib Study of Chemoprevention with Green Tea Polyphenon E and Erlotinib in Patients with Advanced Premalignant Lesions (APL) of the Head and Neck. Clin. Cancer Res. 2020, 26, 5860–5868. [Google Scholar] [CrossRef]
- Sur, S.; Panda, C.K. Molecular Aspects of Cancer Chemopreventive and Therapeutic Efficacies of Tea and Tea Polyphenols. Nutrition 2017, 43–44, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Narotzki, B.; Reznick, A.Z.; Aizenbud, D.; Levy, Y. Green Tea: A Promising Natural Product in Oral Health. Arch. Oral Biol. 2012, 57, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Dipalma, G.; Cirulli, N.; Cantore, S.; Saini, R.S.; Altini, V.; Santacroce, L.; Ballini, A.; Saini, R. Microbiological Results of Improvement in Periodontal Condition by Administration of Oral Probiotics. J. Biol. Regul. Homeost. Agents 2018, 32, 1323–1328. [Google Scholar]
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; Mancini, A.; et al. COVID-19 Infection in Children and Infants: Current Status on Therapies and Vaccines. Children 2022, 9, 249. [Google Scholar] [CrossRef]
- Koh, Y.W.; Choi, E.C.; Kang, S.U.; Hwang, H.S.; Lee, M.H.; Pyun, J.; Park, R.; Lee, Y.; Kim, C.-H. Green Tea (-)-Epigallocatechin-3-Gallate Inhibits HGF-Induced Progression in Oral Cavity Cancer through Suppression of HGF/c-Met. J. Nutr. Biochem. 2011, 22, 1074–1083. [Google Scholar] [CrossRef] [PubMed]
- Zigmundo, G.C.d.O.; Schuch, L.F.; Schmidt, T.R.; Silveira, F.M.; Martins, M.A.T.; Carrard, V.C.; Martins, M.D.; Wagner, V.P. 4-Nitroquinoline-1-Oxide (4NQO) Induced Oral Carcinogenesis: A Systematic Literature Review. Pathol. Res. Pract. 2022, 236, 153970. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, P.; Suchalatha, S.; Babu, P.V.A.; Devi, R.S.; Narayan, S.; Sabitha, K.E.; Shyamala Devi, C.S. Chemopreventive and Therapeutic Modulation of Green Tea Polyphenols on Drug Metabolizing Enzymes in 4-Nitroquinoline 1-Oxide Induced Oral Cancer. Chem. Biol. Interact. 2008, 172, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Dundar, S.; Bozoglan, A.; Bulmus, O.; Tekin, S.; Yildirim, T.T.; Kirtay, M.; Toy, V.E.; Gul, M.; Bozoglan, M.Y. Effects of Restraint Stress and High-Fat Diet on Osseointegration of Titanium Implants: An Experimental Study. Braz. Oral Res. 2020, 34, e008. [Google Scholar] [CrossRef]
- Keuroghlian, A.; Barroso, A.D.V.; Kirikian, G.; Bezouglaia, O.; Tintut, Y.; Tetradis, S.; Moy, P.; Pirih, F.; Aghaloo, T. The Effects of Hyperlipidemia on Implant Osseointegration in the Mouse Femur. J. Oral Implantol. 2015, 41, e7–e11. [Google Scholar] [CrossRef] [Green Version]
- Cheung, B.; Sikand, G.; Dineen, E.H.; Malik, S.; Barseghian El-Farra, A. Lipid-Lowering Nutraceuticals for an Integrative Approach to Dyslipidemia. J. Clin. Med. 2023, 12, 3414. [Google Scholar] [CrossRef]
- Dai, C.; Lin, J.; Li, H.; Shen, Z.; Wang, Y.; Velkov, T.; Shen, J. The Natural Product Curcumin as an Antibacterial Agent: Current Achievements and Problems. Antioxidants 2022, 11, 459. [Google Scholar] [CrossRef]
- Chen, H.; Xie, S.; Gao, J.; He, L.; Luo, W.; Tang, Y.; Weir, M.D.; Oates, T.W.; Xu, H.H.K.; Yang, D. Flavonoid Baicalein Suppresses Oral Biofilms and Protects Enamel Hardness to Combat Dental Caries. Int. J. Mol. Sci. 2022, 23, 10593. [Google Scholar] [CrossRef]
- Kumbar, V.M.; Peram, M.R.; Kugaji, M.S.; Shah, T.; Patil, S.P.; Muddapur, U.M.; Bhat, K.G. Effect of Curcumin on Growth, Biofilm Formation and Virulence Factor Gene Expression of Porphyromonas Gingivalis. Odontology 2021, 109, 18–28. [Google Scholar] [CrossRef]
- Gupta, S.C.; Patchva, S.; Aggarwal, B.B. Therapeutic Roles of Curcumin: Lessons Learned from Clinical Trials. AAPS J. 2012, 15, 195–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuloria, S.; Mehta, J.; Chandel, A.; Sekar, M.; Rani, N.N.I.M.; Begum, M.Y.; Subramaniyan, V.; Chidambaram, K.; Thangavelu, L.; Nordin, R.; et al. A Comprehensive Review on the Therapeutic Potential of Curcuma Longa Linn. in Relation to Its Major Active Constituent Curcumin. Front. Pharmacol. 2022, 13. [Google Scholar] [CrossRef]
- Yallapu, M.M.; Jaggi, M.; Chauhan, S.C. Curcumin Nanoformulations: A Future Nanomedicine for Cancer. Drug Discov. Today 2012, 17, 71–80. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.X.; Li, C.M.; Huang, C.Z. Curcumin Modified Silver Nanoparticles for Highly Efficient Inhibition of Respiratory Syncytial Virus Infection. Nanoscale 2016, 8, 3040–3048. [Google Scholar] [CrossRef]
- Dance-Barnes, S.T.; Kock, N.D.; Moore, J.E.; Lin, E.Y.; Mosley, L.J.; D’Agostino, R.B.; McCoy, T.P.; Townsend, A.J.; Miller, M.S. Lung Tumor Promotion by Curcumin. Carcinogenesis 2009, 30, 1016–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laparra, J.M.; Sanz, Y. Interactions of Gut Microbiota with Functional Food Components and Nutraceuticals. Pharmacol. Res. 2010, 61, 219–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Avantario, P.; Azzollini, D.; Buongiorno, S.; Viapiano, F.; Campanelli, M.; Ciocia, A.M.; De Leonardis, N.; et al. Effects of Resveratrol, Curcumin and Quercetin Supplementation on Bone Metabolism—A Systematic Review. Nutrients 2022, 14, 3519. [Google Scholar] [CrossRef]
- Viapiano, F.; Viapiano, F.; Viapiano, F. Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report. Children 2022, 9, 1046. [Google Scholar] [CrossRef]
- Ornstrup, M.J.; Harsløf, T.; Sørensen, L.; Stenkjær, L.; Langdahl, B.L.; Pedersen, S.B. Resveratrol Increases Osteoblast Differentiation In Vitro Independently of Inflammation. Calcif. Tissue Int. 2016, 99, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Knop, F.K.; Konings, E.; Timmers, S.; Schrauwen, P.; Holst, J.J.; Blaak, E.E. Thirty Days of Resveratrol Supplementation Does Not Affect Postprandial Incretin Hormone Responses, but Suppresses Postprandial Glucagon in Obese Subjects. Diabet. Med. 2013, 30, 1214–1218. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Gambino, R.; Ponzo, V.; Cioffi, I.; Goitre, I.; Evangelista, A.; Ciccone, G.; Cassader, M.; Procopio, M. Effects of Resveratrol on Bone Health in Type 2 Diabetic Patients. A Double-Blind Randomized-Controlled Trial. Nutr. Diabetes 2018, 8, 51. [Google Scholar] [CrossRef] [Green Version]
- Asis, M.; Hemmati, N.; Moradi, S.; Nagulapalli Venkata, K.C.; Mohammadi, E.; Farzaei, M.H.; Bishayee, A. Effects of Resveratrol Supplementation on Bone Biomarkers: A Systematic Review and Meta-Analysis. Ann. N. Y. Acad. Sci. 2019, 1457, 92–103. [Google Scholar] [CrossRef]
- Borsani, E.; Bonazza, V.; Buffoli, B.; Nocini, P.F.; Albanese, M.; Zotti, F.; Inchingolo, F.; Rezzani, R.; Rodella, L.F. Beneficial Effects of Concentrated Growth Factors and Resveratrol on Human Osteoblasts In Vitro Treated with Bisphosphonates. BioMed Res. Int. 2018, 2018, 4597321. [Google Scholar] [CrossRef] [Green Version]
- Zhai, J.-L.; Weng, X.-S.; Wu, Z.-H.; Guo, S.-G. Effect of Resveratrol on Preventing Steroid-Induced Osteonecrosis in a Rabbit Model. Chin. Med. J. 2016, 129, 824–830. [Google Scholar] [CrossRef]
- Simonet, W.S.; Lacey, D.L.; Dunstan, C.R.; Kelley, M.; Chang, M.S.; Lüthy, R.; Nguyen, H.Q.; Wooden, S.; Bennett, L.; Boone, T.; et al. Osteoprotegerin: A Novel Secreted Protein Involved in the Regulation of Bone Density. Cell 1997, 89, 309–319. [Google Scholar] [CrossRef] [Green Version]
- Palermo, A.; Giannotti, L.; Di Chiara Stanca, B.; Ferrante, F.; Gnoni, A.; Nitti, P.; Calabriso, N.; Demitri, C.; Damiano, F.; Batani, T.; et al. Use of CGF in Oral and Implant Surgery: From Laboratory Evidence to Clinical Evaluation. Int. J. Mol. Sci. 2022, 23, 15164. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Xhajanka, E.; Scarano, A.; Lorusso, F.; Farronato, M.; Tartaglia, G.M.; Isacco, C.G.; et al. SARS-CoV-2 Disease Adjuvant Therapies and Supplements Breakthrough for the Infection Prevention. Microorganisms 2021, 9, 525. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.-C.; Tsai, Y.-F.; Tsai, H.-I.; Yu, H.-P. Anti-Inflammatory and Organ-Protective Effects of Resveratrol in Trauma-Hemorrhagic Injury. Mediat. Inflamm. 2015, 2015, 643763. [Google Scholar] [CrossRef] [Green Version]
- Kugaji, M.S.; Kumbar, V.M.; Peram, M.R.; Patil, S.; Bhat, K.G.; Diwan, P.V. Effect of Resveratrol on Biofilm Formation and Virulence Factor Gene Expression of Porphyromonas Gingivalis in Periodontal Disease. APMIS 2019, 127, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Anand David, A.V.; Arulmoli, R.; Parasuraman, S. Overviews of Biological Importance of Quercetin: A Bioactive Flavonoid. Pharmacogn. Rev. 2016, 10, 84–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abouelmagd, S.A.; Sun, B.; Chang, A.C.; Ku, Y.J.; Yeo, Y. Release Kinetics Study of Poorly Water-Soluble Drugs from Nanoparticles: Are We Doing It Right? Mol. Pharm. 2015, 12, 997–1003. [Google Scholar] [CrossRef] [Green Version]
- Chang, W.-S.; Tsai, C.-W.; Yang, J.-S.; Hsu, Y.-M.; Shih, L.-C.; Chiu, H.-Y.; Bau, D.-T.; Tsai, F.-J. Resveratrol Inhibited the Metastatic Behaviors of Cisplatin-Resistant Human Oral Cancer Cells via Phosphorylation of ERK/p-38 and Suppression of MMP-2/9. J. Food Biochem. 2021, 45, e13666. [Google Scholar] [CrossRef] [PubMed]
- Bottino, M.C.; Arthur, R.A.; Waeiss, R.A.; Kamocki, K.; Gregson, K.S.; Gregory, R.L. Biodegradable Nanofibrous Drug Delivery Systems: Effects of Metronidazole and Ciprofloxacin on Periodontopathogens and Commensal Oral Bacteria. Clin. Oral Investig. 2014, 18, 2151–2158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alamanda, M.; Denthumdas, S.K.; Wadgave, U.; Pharne, P.M.; Patil, S.J.; Kondreddi, S.; Deshpande, P.; Koppikar, R.S. Comparative Evaluation of Ciprofloxacin Levels in GCF and Plasma of Chronic Periodontitis Patients: Quasi Experimental Study. J. Clin. Diagn. Res. 2016, 10, ZC47-50. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.M.; Malcangi, G.; Ferrante, L.; Del Vecchio, G.; Viapiano, F.; Mancini, A.; Inchingolo, F.; Inchingolo, A.D.; Di Venere, D.; Dipalma, G.; et al. Damage from Carbonated Soft Drinks on Enamel: A Systematic Review. Nutrients 2023, 15, 1785. [Google Scholar] [CrossRef]
- Inchingolo, A.M.; Malcangi, G.; Ferrara, I.; Patano, A.; Viapiano, F.; Netti, A.; Azzollini, D.; Ciocia, A.M.; de Ruvo, E.; Campanelli, M.; et al. MRONJ Treatment Strategies: A Systematic Review and Two Case Reports. Appl. Sci. 2023, 13, 4370. [Google Scholar] [CrossRef]
- Carazo, A.; Macáková, K.; Matoušová, K.; Krčmová, L.K.; Protti, M.; Mladěnka, P. Vitamin A Update: Forms, Sources, Kinetics, Detection, Function, Deficiency, Therapeutic Use and Toxicity. Nutrients 2021, 13, 1703. [Google Scholar] [CrossRef]
- Chawla, J.; Kvarnberg, D. Hydrosoluble Vitamins. Handb. Clin. Neurol. 2014, 120, 891–914. [Google Scholar] [CrossRef]
- Neiva, R.F.; Al-Shammari, K.; Nociti, F.H.; Soehren, S.; Wang, H.-L. Effects of Vitamin-B Complex Supplementation on Periodontal Wound Healing. J. Periodontol. 2005, 76, 1084–1091. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Inchingolo, A.M.; Piras, F.; Malcangi, G.; Patano, A.; Di Pede, C.; Netti, A.; Ciocia, A.M.; Corriero, A.; Semjonova, A.; et al. A Systematic Review of Positional Plagiocephaly Prevention Methods for Patients in Development. Appl. Sci. 2022, 12, 11172. [Google Scholar] [CrossRef]
- Abdullah, M.; Jamil, R.T.; Attia, F.N. Vitamin C (Ascorbic Acid). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Zohoori, V.; Duckworth, R.M. The Impact of Nutrition and Diet on Oral Health; Monographs in Oral Science; Karger Publishers: Basel, Switzerland, 2020; Volume 28, ISBN 978-3-318-06516-9. [Google Scholar]
- Grenier, D.; Morin, M.-P.; Fournier-Larente, J.; Chen, H. Vitamin D Inhibits the Growth of and Virulence Factor Gene Expression by Porphyromonas Gingivalis and Blocks Activation of the Nuclear Factor Kappa B Transcription Factor in Monocytes. J. Periodontal. Res. 2016, 51, 359–365. [Google Scholar] [CrossRef]
- Inchingolo, F.; Martelli, F.S.; Gargiulo Isacco, C.; Borsani, E.; Cantore, S.; Corcioli, F.; Boddi, A.; Nguyễn, K.C.D.; De Vito, D.; Aityan, S.K.; et al. Chronic Periodontitis and Immunity, Towards the Implementation of a Personalized Medicine: A Translational Research on Gene Single Nucleotide Polymorphisms (SNPs) Linked to Chronic Oral Dysbiosis in 96 Caucasian Patients. Biomedicines 2020, 8, 115. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.-T.; Nestel, F.P.; Bourdeau, V.; Nagai, Y.; Wang, Q.; Liao, J.; Tavera-Mendoza, L.; Lin, R.; Hanrahan, J.W.; Mader, S.; et al. Cutting Edge: 1,25-Dihydroxyvitamin D3 Is a Direct Inducer of Antimicrobial Peptide Gene Expression. J. Immunol. 2004, 173, 2909–2912. [Google Scholar] [CrossRef] [Green Version]
- Stein, S.H.; Livada, R.; Tipton, D.A. Re-Evaluating the Role of Vitamin D in the Periodontium. J. Periodontal Res. 2014, 49, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. [Google Scholar] [CrossRef] [PubMed]
- Hokugo, A.; Christensen, R.; Chung, E.M.; Sung, E.C.; Felsenfeld, A.L.; Sayre, J.W.; Garrett, N.; Adams, J.S.; Nishimura, I. Increased Prevalence of Bisphosphonate-Related Osteonecrosis of the Jaw with Vitamin D Deficiency in Rats. J. Bone Miner. Res. 2010, 25, 1337–1349. [Google Scholar] [CrossRef] [Green Version]
- Yanık, S.; Aras, M.H.; Erkılıç, S.; Bozdağ, Z.; Demir, T.; Çetiner, S. Histopathological Features of Bisphosphonates Related Osteonecrosis of the Jaw in Rats with and without Vitamin d Supplementation. Arch. Oral Biol. 2016, 65, 59–65. [Google Scholar] [CrossRef]
- Chiang, K.-C.; Yeh, C.-N.; Chen, S.-C.; Shen, S.-C.; Hsu, J.-T.; Yeh, T.-S.; Pang, J.-H.S.; Su, L.-J.; Takano, M.; Kittaka, A.; et al. MART-10, a New Generation of Vitamin D Analog, Is More Potent than 1α,25-Dihydroxyvitamin D(3) in Inhibiting Cell Proliferation and Inducing Apoptosis in ER+ MCF-7 Breast Cancer Cells. Evid. Based Complement Altern. Med. 2012, 2012, 310872. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, S.; Raza, S.T.; Ahmed, F.; Ahmad, A.; Abbas, S.; Mahdi, F. The Role of Vitamin E in Human Health and Some Diseases. Sultan Qaboos Univ. Med. J. 2014, 14, e157–e165. [Google Scholar]
- Mangaiyarkarasi, S.P.; Manigandan, T.; Elumalai, M.; Cholan, P.K.; Kaur, R.P. Benefits of Aloe Vera in Dentistry. J. Pharm. Bioallied Sci. 2015, 7, S255–S259. [Google Scholar] [CrossRef]
- Khurshid, Z.; Naseem, M.; Zafar, M.S.; Najeeb, S.; Zohaib, S. Propolis: A Natural Biomaterial for Dental and Oral Healthcare. J. Dent. Res. Dent. Clin. Dent. Prospect. 2017, 11, 265–274. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasti, J.; Wasti, A.; Singh, R. Efficacy of Antioxidants Therapy on Progression of Periodontal Disease—A Randomized Control Trial. Indian J. Dent. Res. 2021, 32, 187–191. [Google Scholar] [CrossRef] [PubMed]
- El-Sharkawy, H.; Elmeadawy, S.; Elshinnawi, U.; Anees, M. Is Dietary Melatonin Supplementation a Viable Adjunctive Therapy for Chronic Periodontitis?-A Randomized Controlled Clinical Trial. J. Periodontal Res. 2019, 54, 190–197. [Google Scholar] [CrossRef]
- Melnychuk, H.M.; Semeniuk, H.D.; Kashivska, R.S.; Shovkova, N.I.; Melnyk, N.S. Regulation of Antioxidant Enzymes in Patients after Periodontal Treatment with Natural Agents. Wiad Lek 2022, 75, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Shasmitha, R.S.; Gurunathan, D.; Mani, G. Evaluation of Antioxidant-Essential Toothpaste as a Treatment for Gingivitis in Orthodontic Patients. Drug Invent. Today 2019, 12, 151–154. [Google Scholar]
- Sukmawati, A.N.; Wijayanti, P.; Karina, V.M.; Lastianny, S.P. 10% Propolis as a Subgingival Irrigation Agent after Gingival Curettage: A Comparative Study. J. Int. Oral Health 2021, 13, 571. [Google Scholar] [CrossRef]
- Hong, J.-Y.; Lee, J.-S.; Choi, S.-H.; Shin, H.-S.; Park, J.-C.; Shin, S.-I.; Chung, J.-H. A Randomized, Double-Blind, Placebo-Controlled Multicenter Study for Evaluating the Effects of Fixed-Dose Combinations of Vitamin C, Vitamin E, Lysozyme, and Carbazochrome on Gingival Inflammation in Chronic Periodontitis Patients. BMC Oral Health 2019, 19, 40. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Shang, Q.; Yang, D.; Peng, J.; Zhao, H.; Xu, H.; Chen, Q. Abnormal Micronutrient Intake Is Associated with the Risk of Periodontitis: A Dose-Response Association Study Based on NHANES 2009–2014. Nutrients 2022, 14, 2466. [Google Scholar] [CrossRef]
- Li, X.; Tang, L.; Lin, Y.F.; Xie, G.F. Role of Vitamin C in Wound Healing after Dental Implant Surgery in Patients Treated with Bone Grafts and Patients with Chronic Periodontitis. Clin. Implant. Dent. Relat. Res. 2018, 20, 793–798. [Google Scholar] [CrossRef]
- Das, M.; Das, A.C.; Panda, S.; Greco Lucchina, A.; Mohanty, R.; Manfredi, B.; Rovati, M.; Giacomello, M.S.; Colletti, L.; Mortellaro, C.; et al. Clinical Efficacy of Grape Seed Extract as an Adjuvant to Scaling and Root Planing in Treatment of Periodontal Pockets. J. Biol. Regul. Homeost. Agents 2021, 35, 89–96. [Google Scholar] [CrossRef]
- Mehta, P.; Bhavasar, R.; Ajith, N.A.; Bhavsar, R.P.; Bahammam, M.A.; Bakri, M.M.H.; Alzahrani, K.J.; Alghamdi, A.A.; Halawani, I.F.; Bhandi, S.; et al. Assessing the Effect of Curcumin on the Oral Mucosal Cytomorphometry and Candidal Species Specificity in Tobacco Users: A Pilot Study. Healthcare 2022, 10, 1507. [Google Scholar] [CrossRef]
- Cespedes, D.; Mendez, J.; Villasanti, U. Carica Papaya Mouthrinse as an Inhibitor of Streptococcus Mutans: Randomized Controlled Clinical Trial. Am. J. Dent. 2021, 34, 273–276. [Google Scholar] [PubMed]
- Kia, S.J.; Basirat, M.; Mortezaie, T.; Moosavi, M.-S. Comparison of Oral Nano-Curcumin with Oral Prednisolone on Oral Lichen Planus: A Randomized Double-Blinded Clinical Trial. BMC Complement. Med. Ther. 2020, 20, 328. [Google Scholar] [CrossRef] [PubMed]
- Neetha, M.C.; Panchaksharappa, M.G.; Pattabhiramasastry, S.; Shivaprasad, N.V.; Venkatesh, U.G. Chemopreventive Synergism between Green Tea Extract and Curcumin in Patients with Potentially Malignant Oral Disorders: A Double-Blind, Randomized Preliminary Study. J. Contemp. Dent. Pract. 2020, 21, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Agha-Hosseini, F.; Pourpasha, M.; Amanlou, M.; Moosavi, M.-S. Mouthwash Containing Vitamin E, Triamcinolon, and Hyaluronic Acid Compared to Triamcinolone Mouthwash Alone in Patients With Radiotherapy-Induced Oral Mucositis: Randomized Clinical Trial. Front. Oncol. 2021, 11, 614877. [Google Scholar] [CrossRef] [PubMed]
- González-Serrano, J.; López-Pintor, R.M.; Serrano, J.; Torres, J.; Hernández, G.; Sanz, M. Short-Term Efficacy of a Gel Containing Propolis Extract, Nanovitamin C and Nanovitamin E on Peri-Implant Mucositis: A Double-Blind, Randomized, Clinical Trial. J. Periodontal Res. 2021, 56, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Salehi, M.; Saeedi, M.; Ghorbani, A.; Ghodrati, P.; Moosazadeh, M.; Rostamkalaei, S.; Hatkehlouei, M.B.; Molania, T. The Effect of Propolis Tablet on Oral Mucositis Caused by Chemotherapy|Gazi Medical Journal. GMJ 2018, 29, 196–201. [Google Scholar] [CrossRef] [Green Version]
- Nerkar Rajbhoj, A.; Kulkarni, T.M.; Shete, A.; Shete, M.; Gore, R.; Sapkal, R. A Comparative Study to Evaluate Efficacy of Curcumin and Aloe Vera Gel along with Oral Physiotherapy in the Management of Oral Submucous Fibrosis: A Randomized Clinical Trial. Asian Pac. J. Cancer Prev. 2021, 22, 107–112. [Google Scholar] [CrossRef]
- Tahir, M.; Abbas, A.; Nawaz, F.U.H.; Raza, M.; Rafique, A.; Niazi, M.S.B. Efficacy Of Antioxidant With Aloe Vera Gel Versus Intra-Lesional Steroids in the Management of Oral Submucous Fibrosis—A Prospective Comparative Study. Pak. Armed Forces Med. J. 2021, 71, S526-29. [Google Scholar] [CrossRef]
- Chapple, I.L.C. Potential Mechanisms Underpinning the Nutritional Modulation of Periodontal Inflammation. J. Am. Dent. Assoc. 2009, 140, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Van Der Velden, U.; Kuzmanova, D.; Chapple, I.L.C. Micronutritional Approaches to Periodontal Therapy: Micronutritrients and Periodontal Therapy. J. Clin. Periodontol. 2011, 38, 142–158. [Google Scholar] [CrossRef]
- Dawson, D.R.; Branch-Mays, G.; Gonzalez, O.A.; Ebersole, J.L. Dietary Modulation of the Inflammatory Cascade: Dietary Modulation of the Inflammatory Cascade. Periodontology 2000 2014, 64, 161–197. [Google Scholar] [CrossRef]
- Tenovuo, J. Clinical Applications of Antimicrobial Host Proteins Lactoperoxidase, Lysozyme and Lactoferrin in Xerostomia: Efficacy and Safety. Oral Dis. 2002, 8, 23–29. [Google Scholar] [CrossRef]
- Sendo, T.; Itoh, Y.; Aki, K.; Oka, M.; Oishi, R. Carbazochrome Sodium Sulfonate (AC-17) Reverses Endothelial Barrier Dysfunction through Inhibition of Phosphatidylinositol Hydrolysis in Cultured Porcine Endothelial Cells. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2003, 368, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Cabezas-Wallscheid, N.; Buettner, F.; Sommerkamp, P.; Klimmeck, D.; Ladel, L.; Thalheimer, F.B.; Pastor-Flores, D.; Roma, L.P.; Renders, S.; Zeisberger, P.; et al. Vitamin A-Retinoic Acid Signaling Regulates Hematopoietic Stem Cell Dormancy. Cell 2017, 169, 807–823.e19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dommisch, H.; Kuzmanova, D.; Jönsson, D.; Grant, M.; Chapple, I. Effect of Micronutrient Malnutrition on Periodontal Disease and Periodontal Therapy. Periodontol 2000 2018, 78, 129–153. [Google Scholar] [CrossRef]
- Doshi, P.; Adsule, P.; Banerjee, K.; Oulkar, D. Phenolic Compounds, Antioxidant Activity and Insulinotropic Effect of Extracts Prepared from Grape (Vitis vinifera L.) Byproducts. J. Food Sci. Technol. 2015, 52, 181–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.G.; Zhang, X.Y.; Wu, Y.J.; Tian, X. Anti-Inflammatory Effect and Mechanism of Proanthocyanidins from Grape Seeds. Acta Pharmacol. Sin. 2001, 22, 1117–1120. [Google Scholar]
- Furiga, A.; Lonvaud-Funel, A.; Badet, C. In Vitro Study of Antioxidant Capacity and Antibacterial Activity on Oral Anaerobes of a Grape Seed Extract. Food Chem. 2009, 113, 1037–1040. [Google Scholar] [CrossRef]
- Nuttall, S.L.; Kendall, M.J.; Bombardelli, E.; Morazzoni, P. An Evaluation of the Antioxidant Activity of a Standardized Grape Seed Extract, Leucoselect®. J. Clin. Pharm. Ther. 1998, 23, 385–389. [Google Scholar] [CrossRef]
- Baydar, N.G.; Özkan, G.; Sağdiç, O. Total Phenolic Contents and Antibacterial Activities of Grape (Vitis vinifera L.) Extracts. Food Control 2004, 15, 335–339. [Google Scholar] [CrossRef]
- Canakci, C.F.; Cicek, Y.; Yildirim, A.; Sezer, U.; Canakci, V. Increased Levels of 8-Hydroxydeoxyguanosine and Malondialdehyde and Its Relationship with Antioxidant Enzymes in Saliva of Periodontitis Patients. Eur. J. Dent. 2009, 3, 100–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inchingolo, A.D.; Cazzolla, A.P.; Di Cosola, M.; Greco Lucchina, A.; Santacroce, L.; Charitos, I.A.; Topi, S.; Malcangi, G.; Hazballa, D.; Scarano, A.; et al. The Integumentary System and Its Microbiota between Health and Disease. J. Biol. Regul. Homeost. Agents 2021, 35, 303–321. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Elner, S.G.; Bian, Z.-M.; Till, G.O.; Petty, H.R.; Elner, V.M. Pro-Inflammatory Cytokines Increase Reactive Oxygen Species through Mitochondria and NADPH Oxidase in Cultured RPE Cells. Exp. Eye Res. 2007, 85, 462–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, M.; Siddiqui, M.R.; Tran, K.; Reddy, S.P.; Malik, A.B. Reactive Oxygen Species in Inflammation and Tissue Injury. Antioxid. Redox Signal. 2014, 20, 1126–1167. [Google Scholar] [CrossRef] [Green Version]
- Lobo, V.; Patil, A.; Phatak, A.; Chandra, N. Free Radicals, Antioxidants and Functional Foods: Impact on Human Health. Phcog. Rev. 2010, 4, 118. [Google Scholar] [CrossRef] [Green Version]
- Bin-Jumah, M.N.; Nadeem, M.S.; Gilani, S.J.; Mubeen, B.; Ullah, I.; Alzarea, S.I.; Ghoneim, M.M.; Alshehri, S.; Al-Abbasi, F.A.; Kazmi, I. Lycopene: A Natural Arsenal in the War against Oxidative Stress and Cardiovascular Diseases. Antioxidants 2022, 11, 232. [Google Scholar] [CrossRef]
- Tripathi, P.; Blaggana, V.; Upadhyay, P.; Jindal, M.; Gupta, S.; Nishat, S. Antioxidant Therapy (Lycopene and Green Tea Extract) in Periodontal Disease: A Promising Paradigm. J. Indian Soc. Periodontol. 2019, 23, 25. [Google Scholar] [CrossRef]
- Ferlazzo, N.; Andolina, G.; Cannata, A.; Costanzo, M.G.; Rizzo, V.; Currò, M.; Ientile, R.; Caccamo, D. Is Melatonin the Cornucopia of the 21st Century? Antioxidants 2020, 9, 1088. [Google Scholar] [CrossRef]
- Vila, T.; Sultan, A.S.; Montelongo-Jauregui, D.; Jabra-Rizk, M.A. Oral Candidiasis: A Disease of Opportunity. J. Fungi 2020, 6, 15. [Google Scholar] [CrossRef] [Green Version]
- Akpan, A.; Morgan, R. Oral Candidiasis. Postgrad. Med. J. 2002, 78, 455–459. [Google Scholar] [CrossRef] [Green Version]
- Chattopadhyay, I.; Verma, M.; Panda, M. Role of Oral Microbiome Signatures in Diagnosis and Prognosis of Oral Cancer. Technol. Cancer Res. Treat. 2019, 18, 1533033819867354. [Google Scholar] [CrossRef] [Green Version]
- Inchingolo, A.D.; Malcangi, G.; Semjonova, A.; Inchingolo, A.M.; Patano, A.; Coloccia, G.; Ceci, S.; Marinelli, G.; Di Pede, C.; Ciocia, A.M.; et al. Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature. Children 2022, 9, 1014. [Google Scholar] [CrossRef]
- da Silva, J.A.T.; Rashid, Z.; Nhut, D.T.; Sivakumar, D.; Gera, A.; Souza, M.T.; Tennant, P. Papaya (Carica papaya L.) Biology and Biotechnology. Tree For. Sci. Biotechnol. 2007, 1, 47–76. [Google Scholar]
- Singh, S.P.; Kumar, S.; Mathan, S.V.; Tomar, M.S.; Singh, R.K.; Verma, P.K.; Kumar, A.; Kumar, S.; Singh, R.P.; Acharya, A. Therapeutic Application of Carica Papaya Leaf Extract in the Management of Human Diseases. Daru 2020, 28, 735–744. [Google Scholar] [CrossRef]
- Santana, L.F.; Inada, A.C.; do Espirito Santo, B.L.S.; Filiú, W.F.O.; Pott, A.; Alves, F.M.; Guimarães, R.d.C.A.; Freitas, K.d.C.; Hiane, P.A. Nutraceutical Potential of Carica Papaya in Metabolic Syndrome. Nutrients 2019, 11, 1608. [Google Scholar] [CrossRef] [Green Version]
- Lavanya, N.; Jayanthi, P.; Rao, U.K.; Ranganathan, K. Oral Lichen Planus: An Update on Pathogenesis and Treatment. J. Oral Maxillofac. Pathol. 2011, 15, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Cassol-Spanemberg, J.; Rodríguez-de Rivera-Campillo, M.-E.; Otero-Rey, E.-M.; Estrugo-Devesa, A.; Jané-Salas, E.; López-López, J. Oral Lichen Planus and Its Relationship with Systemic Diseases. A Review of Evidence. J. Clin. Exp. Den.t 2018, 10, e938–e944. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Ao, M.; Dong, B.; Jiang, Y.; Yu, L.; Chen, Z.; Hu, C.; Xu, R. Anti-Inflammatory Effects of Curcumin in the Inflammatory Diseases: Status, Limitations and Countermeasures. Drug Des. Dev. Ther. 2021, 15, 4503–4525. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, H.; Baharvand, M.; Mehdipour, M. Oral Potentially Malignant Disorders: An Overview of More than 20 Entities. J. Dent. Res. Dent. Clin. Dent. Prospect. 2014, 8, 6–14. [Google Scholar] [CrossRef]
- Mohammed, A.; Fox, J.T.; Miller, M.S. Cancer Chemoprevention: Preclinical In Vivo Alternate Dosing Strategies to Reduce Drug Toxicities. Toxicol. Sci. 2019, 170, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotecha, R.; Takami, A.; Espinoza, J.L. Dietary Phytochemicals and Cancer Chemoprevention: A Review of the Clinical Evidence. Oncotarget 2016, 7, 52517–52529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.-J.; Cheng, T.-C.; Yen, Y.; Fang, C.-L.; Liao, Y.-C.; Kuo, C.-C.; Tu, S.-H.; Lin, L.-C.; Chang, H.-W.; Chen, L.-C.; et al. Tea Polyphenol Epigallocatechin-3-Gallate Inhibits Cell Proliferation in a Patient-Derived Triple-Negative Breast Cancer Xenograft Mouse Model via Inhibition of Proline-Dehydrogenase-Induced Effects. J. Food Drug Anal. 2021, 29, 113–127. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Articles screening strategy | KEYWORDS: A: “natural”; B: “antioxidant”; C: “oral”; D: “health”; E: “disease” |
| Boolean Indicators: (“A” AND “B”) AND ((“C” AND “D”) OR (“C” AND “E”)) | |
| Timespan: from January 2018 up to 30 April 2023. | |
| Electronic Databases: PubMed, Web of Science, Scopus, and Cochrane Library |
| Author (Year) | Study Design | Number of Patients | Average Age (Years) | Materials and Methods | Pathology | Outcomes |
|---|---|---|---|---|---|---|
| Wasti et al., 2021 [74] | RCT | 48 healthy patients (24 test group; 24 control group) | Unspecified | SRP and oral hygiene instructions. The test group was given a prescription for CLIK®, which contained GT extract (300 mg) and natural lycopene. Post-operative clinical parameter determination and uric acid estimation were performed 45 days later. Saliva was collected at baseline and the 45th day. | Gingivitis | Modified plaque index (PI) ↑,sulcular bleeding index ↑, and salivary uric acid levels ↑ in the test group. The test group’s gingival health improved more than the control group’s (improved antioxidant profile). |
| El-Sharkawy et al., 2019 [75] | RCT | 74 patients with chronic periodontitis (CP) and primary insomnia (test group: 21 M, 17 F; control group: 20 M, 17 F) | Mean age: 45.6 in test group; 46.7 in control group | Patients in the test group received SRP and took 10 mg oral melatonin capsules once daily before bedtime for 2 months. The patients in the control group received SRP and took a placebo. The authors measured clinical attachment level (CAL) gain after 3 and 6 months of therapy. | Periodontitis | At 3 and 6 months, the melatonin group had ↓ probing depth (PD) and CAL compared to those of the placebo group. After 3 and 6 months, the melatonin group showed better PD↓ and CAL↑. No statistically significant differences in plaque index, gingival index, and bleeding upon probing (BOP%) between the two groups were found. |
| Melnychuk et al., 2022 [76] | Observational study | 161 patients; 125 had periodontitis; 36 had intact periodontium | 19–45 | Exogenous and endogenous use of biologically active supplement based on blue-green microalgae Spirulina platensis, a paste made of spirulina powder and silica enterosorbent mixed with 0.05% solution of chlorhexidine bigluconate to a gel-like consistency, and Spirulina tablets were taken twice daily for four weeks. | Periodontitis | All patients had raised levels of malonic dialdehyde, diene conjugates, catalase activity, transferrin iron saturation, and ceruloplasmin activity, which were all reliably and long-lastingly regulated by the treatment. All indicators deviated marginally from the norm during the year, and periodontitis was stabilised. |
| Shasmitha et al., 2019 [77] | Clincial trial | 42 orthodontic patients with generalised chronic gingivitis | 14–30 | Patients were assessed for gingivitis using GI, PD, blood on probing, and OHI. A modified Brass brushing technique using total care herbal toothpaste was demonstrated at the second session and the patients’ gingival condition was once more evaluated. | Gingivitis | The pre-treatment and post-treatment GI and OHI index scores were calculated with a 3-week time difference. Both scores were marginally higher than the respective pre-treatment GI and pre-OHI index scores, but neither was statistically significant. |
| Sukmawati AN et al., 2021 [78] | Comparative Study | 6 patients | Unspecified | Group A received 10% propolis after curettage, while Group B received 1% tetracycline. PPD, BOP, and IL-1 concentration were measured at baseline on day 0, before curettage, and 21 days following curettage. | Periodontal disease | In patients with CP, 10% propolis as a subgingival irrigation agent improved the clinical parameters of periodontal tissue and concentration of IL-1 more effectively than 1% tetracycline did. |
| Hong JY et al., 2019 [79] | RCT | 112 patients | 19–80 | Patients randomly received combinations of vitamin C and E, lysozyme, and carbazochrome (CELC) or the placebo for the first four weeks. Then, it the mean change in the GI was measured, followed by that in the PI, PD, and CAL at 4 and 8 weeks. | Periodontal disease | After 4 weeks and 8 weeks, the GI in the test group considerably ↓. When compared to a placebo, CELC significantly reduced gingival inflammation. |
| Li W et al., 2022 [80] | cross-sectional study | 8959 patients | Mean age: 52.4 | The US National Health and Nutrition Examination Survey (NHANES, 2009–2014) database was used to identify participants who underwent a periodontal examination and reported their micronutrient intake levels. | Periodontal disease | With adequate intake of the micronutrients (vitamin A, vitamin B1, vitamin B2, and vitamin E), the risk of periodontitis was decreased. A high consumption of vitamin B1 (1.8 mg/day for men and 1.3 mg/day for women), vitamin C (90 mg/day for men), and copper (1.1 mg/day combined) all raised the incidence of periodontitis. |
| Li X. et al., 2018 [81] | RCT | 128 patients | Mean age: 44.9 | Group A received dental implants supported by the guided bone regeneration (GBR) technique; group B received dental implants with Bio-Oss Collagen; group C received dental implants, containing patients with CP; and group D received dental implants without any bone grafting or periodontal disease. Each group was split into a control subgroup and an experimental subgroup that received vitamin C. | Periodontal disease | Supplementing with vitamin C helps patients with CP and those receiving GBR or Bio-Oss Collagen grafts heal more quickly after receiving dental implants. |
| Das M. et al., 2021 [82] | RCT | 72 patients | Mean age: 39.2 ± 8.6 | Randomly, two groups of patients with periodontal pockets were formed; the test group received an intra-pocket administration of grape seed extract (GSE) along with SRP, and the control group received SRP alone. At baseline and three months, clinical measurements including the PI, GI, PPD, and relative attachment level (RAL) were taken. | Periodontal disease | At the end of 3 months, the test group showed PD↓ and RAL↓; there was no discernible difference between PI and GI. It might be advantageous to control periodontal pockets via the intra-pocket application of GSE and SRP. |
| Mehta et al., (2022) [83] | Prospective study | 120 (60 cases: 36 M 24 F-60 controls:31 M 29 F) | 18–40 | CUM gel was applied 3 times a day for 2 months; cytomorphometric analysis using CHROMagar was performed | Candidiasis in tobacco users | CUM reduces both the number of micronuclei and also Candida colonies. |
| Cespedes et al., (2021) [84] | Double-blinded RCT | 40 (20 cases-20 controls) | Unspecified | Comparison between Carica papaya and chlorhexidine mouthwash | Caries | Carica papaya has anti S. mutans action which is comparable to that of chlorhexidine |
| Kia et al., (2020) [85] | Double-blinded RCT | 57 (29 case-28 controls) | 51,86 (CUM-cases) 53.67 (prednisolone-controls) | Comparison between administration of 80 mg CUM in the Nano-Micellar Soft gel capsule and 10 mg Prednisolone in capsules | Oral lichen planus (OLP) | CUM may represent an alternative therapy in patients in which corticosteroids are contraindicated; it is effective in preventing the recurrence of OLP lesions. |
| Neetha (2020) [86] | Double-blinded Randomised preliminary study | 60 (20 GT; 20 CUM; 20 combination) | 45.5 (16–82) | Topical + systemic administration for 3 months of GT extract (800 mg/day), CUM (950 mg/day) or both combined. Evaluation of biomarkers Ki67, cyclin D1 and p53 at time 0 and at 12 weeks was performed | Oral potentially malignant disorders (OPMDs) | The combination of CUM and GT extract has synergistic action, causing clinical benefits and the downregulation of molecular biomarkers after 12 weeks. |
| Farzaneh Agha-Hosseini et al,. 2021 [87] | RCT | 60 patients | least 18 years old (no maximum age limit) | Combined mouthwash was prepared with 0.1% triamcinolone, 0.2% vitamin E and 0.2% hyaluronic acid | Oral mucositis caused by radiotherapy | The reduction in inflammation and pain was significantly higher in the intervention group. |
| José Gonzalez-Serrano et al., 2021 [88] | double-blind RCT | 46 patients | around 60 years old | Gel containing propolis extract, nanovitamin C and nanovitamin E | Oeri-implant mucositis (PM) | Full PM resolution was observed in the intervention group. |
| Maede Salehi et al., 2018 [89] | double-blind clinical trial | 50 patients | 26–70 | 2 tablets of 50 mg propolis daily | Oral mucositis caused by chemotherapy | The intervention group achieved a significant difference in the healing of oral mucositis. |
| Ashwini Nerkar Rajbhoj et al., 2021 [90] | RCT | 60 patients | 15–55 | CUM gel and aloe vera gel with oral physiotherapy | Oral submucous fibrosis (OSF) | Both types of gel improved the symptoms but aloe vera gel achieved a statistically significant result in remedying burning. |
| Maometto Tahir et al., 2021 [91] | Prospective comparative study | 28 patients | Mean age: 26.14 ± 5.33 | Comparison between alpha lipoic acid with aloe vera gel and hydrocortisone | OSF | Comparison between the alpha lipoic acid with aloe vera gel group versus the hydrocortisone group showed almost similar results. |
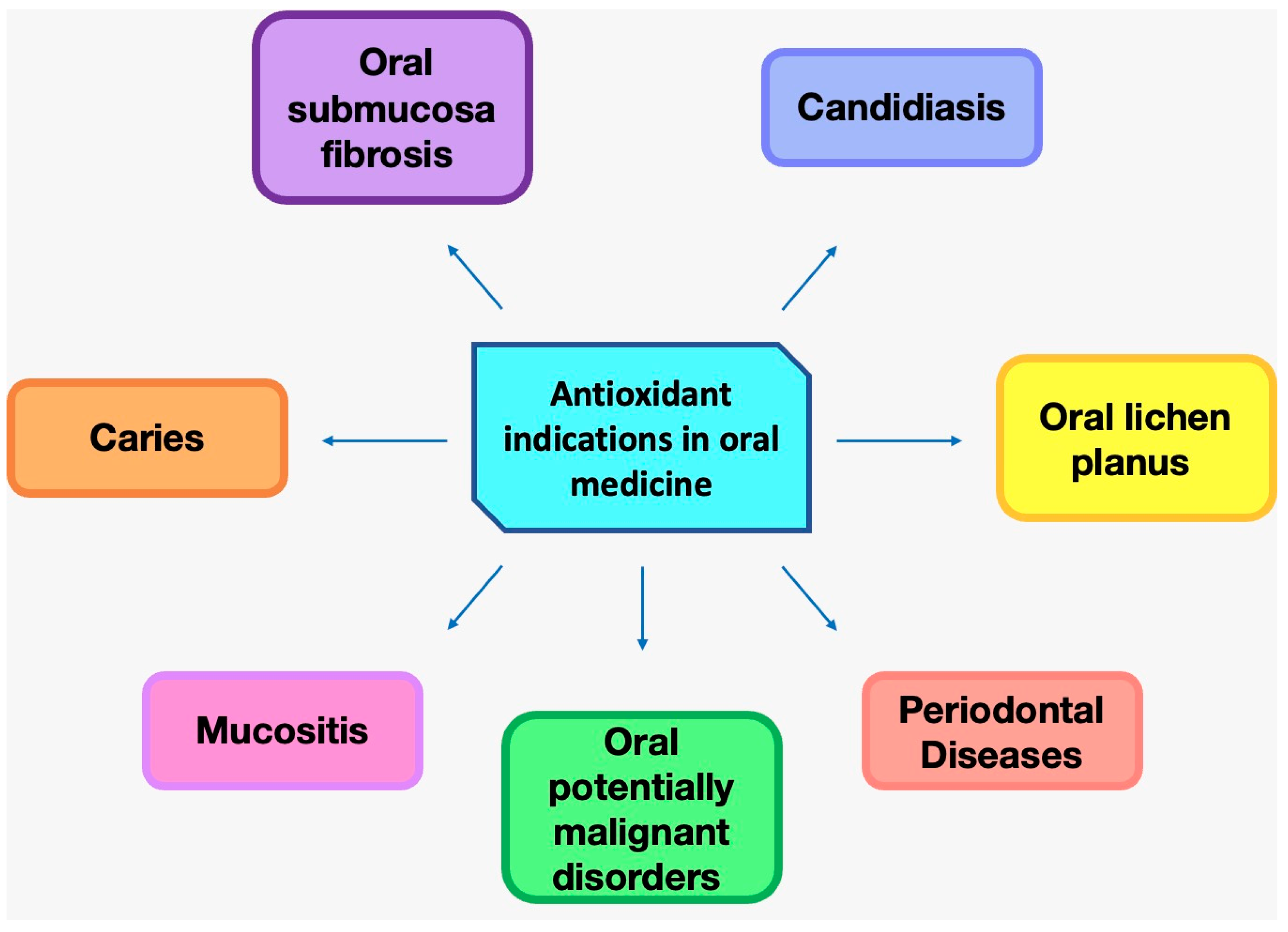
| Oral Disease | Nutraceutical/Food Substance |
|---|---|
| Periodontal disease | Propolis, vitamin C, vitamin E, vitamin A, vitamin B2, copper, sage essential oil, grape seed, green tea, uric acid, menthol and thymol essential oils, ferulic acid and phloretin, and melatonin |
| Mucositis | Vitamin E, triamcinolone and hyaluronic acid, propolis, and vitamin C |
| Oral submucosal fibrosis | Curcumin and aloe vera |
| Oral candidiasis | Curcumin |
| Caries | Papaya |
| Lichen planus | Curcumin |
| Malignant oral cavity disorders | Green tea and curcumin |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malcangi, G.; Patano, A.; Ciocia, A.M.; Netti, A.; Viapiano, F.; Palumbo, I.; Trilli, I.; Guglielmo, M.; Inchingolo, A.D.; Dipalma, G.; et al. Benefits of Natural Antioxidants on Oral Health. Antioxidants 2023, 12, 1309. https://doi.org/10.3390/antiox12061309
Malcangi G, Patano A, Ciocia AM, Netti A, Viapiano F, Palumbo I, Trilli I, Guglielmo M, Inchingolo AD, Dipalma G, et al. Benefits of Natural Antioxidants on Oral Health. Antioxidants. 2023; 12(6):1309. https://doi.org/10.3390/antiox12061309
Chicago/Turabian StyleMalcangi, Giuseppina, Assunta Patano, Anna Maria Ciocia, Anna Netti, Fabio Viapiano, Irene Palumbo, Irma Trilli, Mariafrancesca Guglielmo, Alessio Danilo Inchingolo, Gianna Dipalma, and et al. 2023. "Benefits of Natural Antioxidants on Oral Health" Antioxidants 12, no. 6: 1309. https://doi.org/10.3390/antiox12061309