
One-Year Changes in Urinary Microbial Phenolic Metabolites and the Risk of Type 2 Diabetes—A Case-Control Study

 ,
,  , , , , ,
, , , , ,  , , , , , , and
, , , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
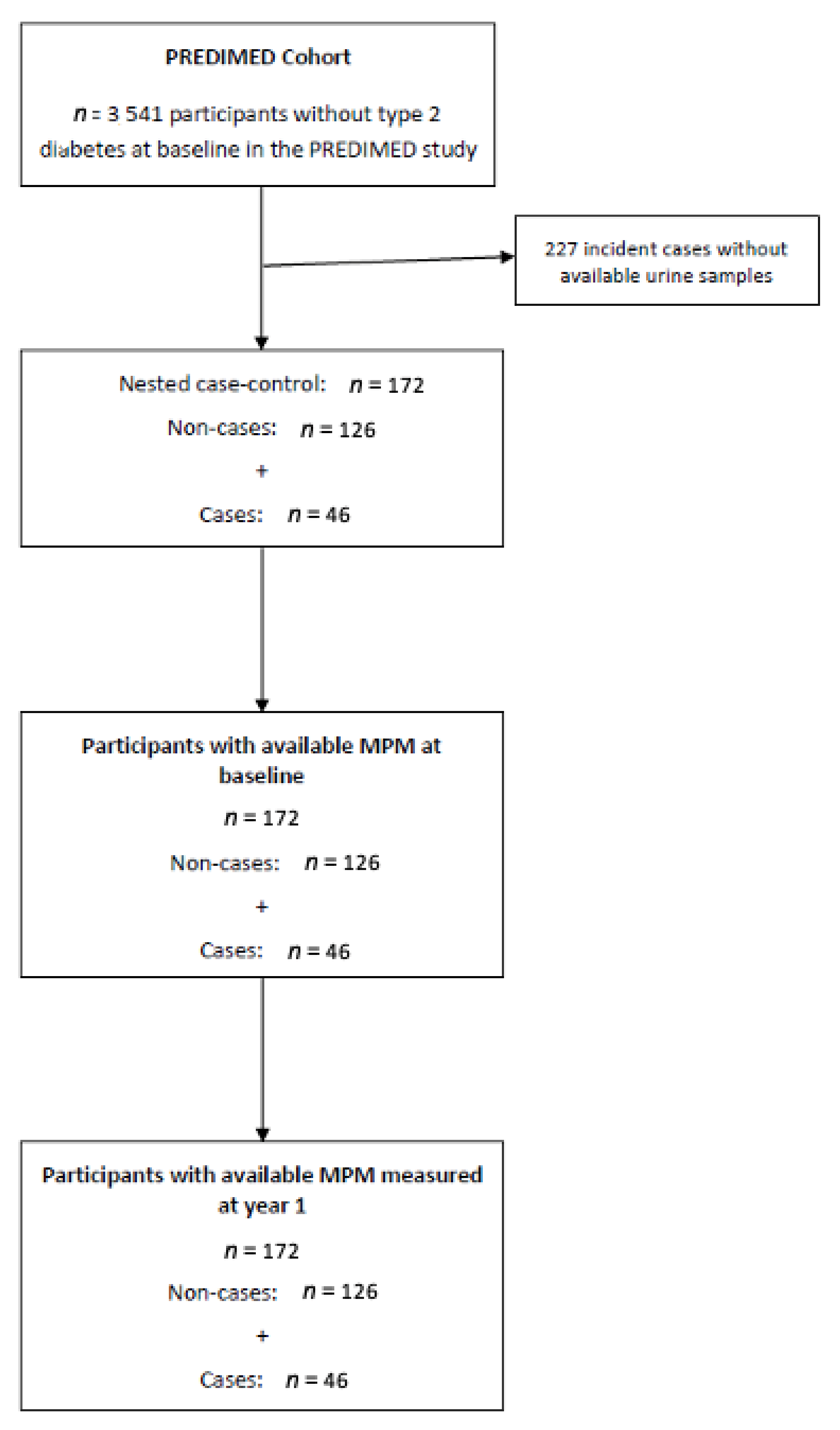
2.1. Study Design
2.2. Type 2 Diabetes Case Ascertainment
2.3. MPM Analysis
2.3.1. Samples, Standards, Solvents, and Equipment
2.3.2. MPM Extraction and Analysis
2.3.3. Creatinine Analysis
2.4. Covariates and Other Variables
2.5. Statistical Analyses
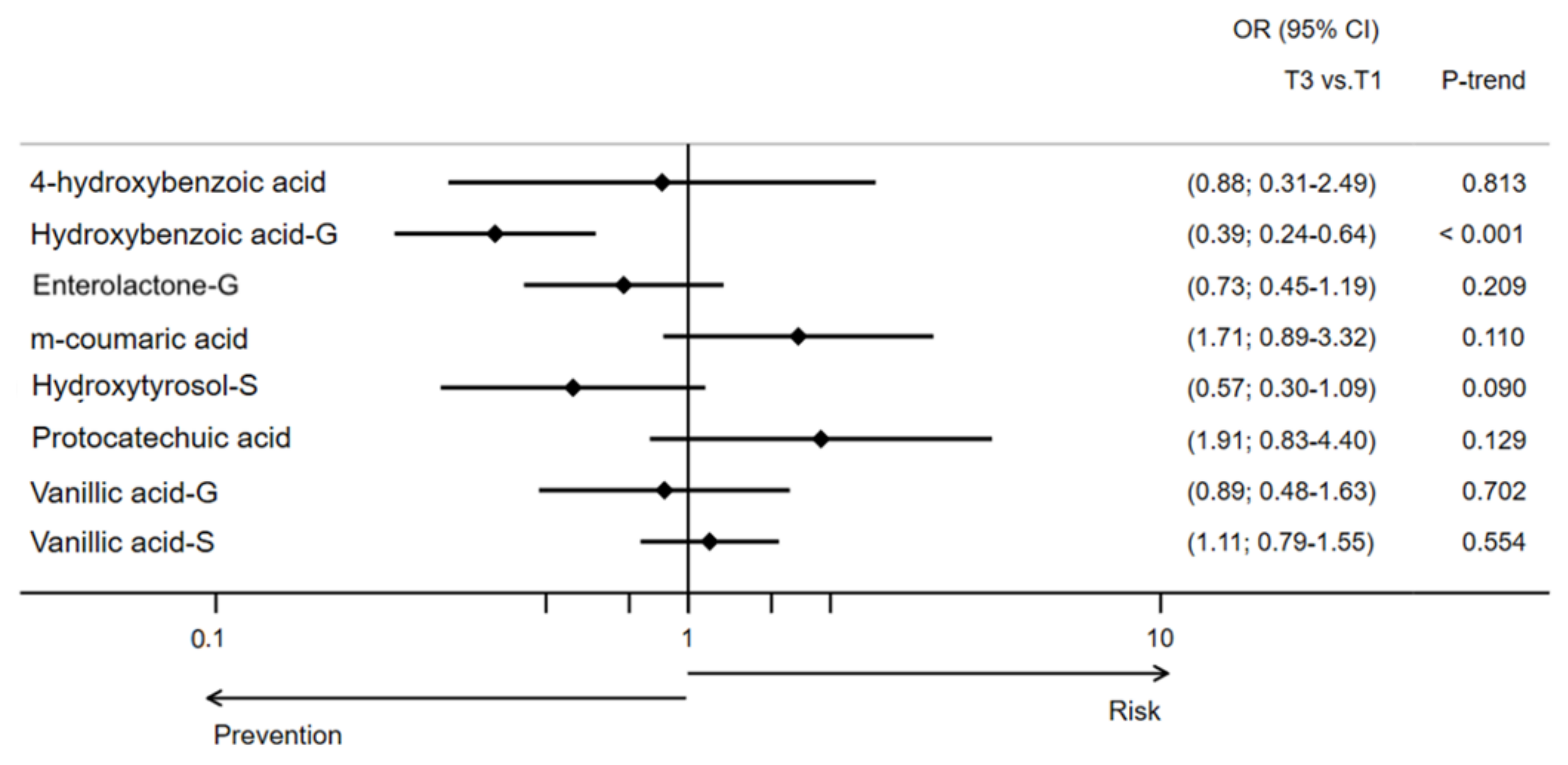
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Salas-Salvadó, J.; Bulló, M.; Estruch, R.; Ros, E.; Covas, M.-I.; Ibarrola-Jurado, N.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; et al. Prevention of diabetes with Mediterranean diets. Ann. Intern. Med. 2014, 160, 1–10. [Google Scholar] [CrossRef]
- Tresserra-Rimbau, A.; Guasch-Ferré, M.; Salas-Salvadó, J.; Toledo, E.; Corella, D.; Castañer, O.; Guo, X.; Gómez-Gracia, E.; Lapetra, J.; Arós, F.; et al. Intake of total polyphenols and some classes of polyphenols is inversely associated with diabetes in elderly people at high cardiovascular disease risk. J. Nutr. 2015, 146, 767–777. [Google Scholar] [CrossRef]
- Fraga, C.G.; Croft, K.D.; Kennedy, D.O.; Tomás-Barberán, F.A. The effects of polyphenols and other bioactives on human health. Food Funct. 2019, 10, 514–528. [Google Scholar] [CrossRef]
- Baur, J.A.; Pearson, K.J.; Price, N.L.; Jamieson, H.A.; Lerin, C.; Kalra, A.; Prabhu, V.V.; Allard, J.S.; Lopez-Lluch, G.; Lewis, K.; et al. Resveratrol improves health and survival of mice on a high-calorie diet. Nature 2006, 444, 337–342. [Google Scholar] [CrossRef]
- Tresserra-Rimbau, A.; Rimm, E.B.; Medina-Remón, A.; Martínez-González, M.A.; de la Torre, R.; Corella, D.; Salas-Salvadó, J.; Gómez-Gracia, E.; Lapetra, J.; Arós, F.; et al. Inverse association between habitual polyphenol intake and incidence of cardiovascular events in the PREDIMED study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 639–647. [Google Scholar] [CrossRef]
- Marhuenda-Muñoz, M.; Laveriano-Santos, E.P.; Tresserra-Rimbau, A.; Lamuela-Raventós, R.M.; Martínez-Huélamo, M.; Vallverdú-Queralt, A. Microbial phenolic metabolites: Which molecules actually have an effect on human health? Nutrients 2019, 11, 2725. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Ros, E.; Covas, M.I.; Fiol, M.; Warnberg, J.; Aros, F.; Ruiz-Gutierrez, V.; Lamuela-Raventos, R.M.; et al. Cohort Profile: Design and methods of the PREDIMED study. Int. J. Epidemiol. 2012, 41, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2008, 31 (Suppl. 1), S55–S60. [Google Scholar] [CrossRef] [PubMed]
- Miró-Casas, E.; Farré Albaladejo, M.; Covas, M.-I.; Rodriguez, J.O.; Menoyo Colomer, E.; Lamuela Raventós, R.M.; de la Torre, R. Capillary gas chromatography–mass spectrometry quantitative determination of hydroxytyrosol and tyrosol in human urine after olive oil intake. Anal. Biochem. 2001, 294, 63–72. [Google Scholar] [CrossRef]
- Laveriano-Santos, E.P.; Marhuenda-Muñoz, M.; Vallverdú-Queralt, A.; Martínez-Huélamo, M.; Tresserra-Rimbau, A.; Miliarakis, E.; Arancibia-Riveros, C.; Jáuregui, O.; Ruiz-León, A.M.; Castro-Baquero, S.; et al. Identification and quantification of urinary microbial phenolic metabolites by HPLC-ESI-LTQ-Orbitrap-HRMS and their relationship with dietary polyphenols in adolescents. Antioxidants 2022, 11, 1167. [Google Scholar] [CrossRef]
- Medina-Remón, A.; Barrionuevo-González, A.; Zamora-Ros, R.; Andres-Lacueva, C.; Estruch, R.; Martínez-González, M.-Á.; Diez-Espino, J.; Lamuela-Raventos, R.M. Rapid Folin–Ciocalteu method using microtiter 96-well plate cartridges for solid phase extraction to assess urinary total phenolic compounds, as a biomarker of total polyphenols intake. Anal. Chim. Acta 2009, 634, 54–60. [Google Scholar] [CrossRef]
- Hodgson, J.M.; Yee Chan, S.; Puddey, I.B.; Devine, A.; Wattanapenpaiboon, N.; Wahlqvist, M.L.; Lukito, W.; Burke, V.; Ward, N.C.; Prince, R.L.; et al. Phenolic acid metabolites as biomarkers for tea- and coffee-derived polyphenol exposure in human subjects. Br. J. Nutr. 2004, 91, 301–305. [Google Scholar] [CrossRef]
- Mir, S.; Serdaroglu, E. Quantification of hypercalciuria with the urine calcium osmolality ratio in children. Pediatr. Nephrol. 2005, 20, 1562–1565. [Google Scholar] [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing mediterranean diet adherence among older spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Ludwig, O. Blom, Gunnar: Statistical estimates and transformed beta-variables. Wiley/New York, Almquist und Wiksell/Stockholm 1958; 176 S., Kr. 20,—. Biom. Z. 1961, 3, 285. [Google Scholar] [CrossRef]
- Simes, R.J. An improved Bonferroni procedure for multiple tests of significance. Biometrika 1986, 73, 751–754. [Google Scholar] [CrossRef]
- Sun, Q.; Wedick, N.M.; Pan, A.; Townsend, M.K.; Cassidy, A.; Franke, A.A.; Rimm, E.B.; Hu, F.B.; van Dam, R.M. Gut microbiota metabolites of dietary lignans and risk of type 2 diabetes: A prospective investigation in two cohorts of u.s. women. Diabetes Care 2014, 37, 1287–1295. [Google Scholar] [CrossRef]
- Talaei, M.; Lee, B.L.; Ong, C.N.; van Dam, R.M.; Yuan, J.M.; Koh, W.P.; Pan, A. Urine phyto-oestrogen metabolites are not significantly associated with risk of type 2 diabetes: The Singapore Chinese health study. Br. J. Nutr. 2016, 115, 1607–1615. [Google Scholar] [CrossRef]
- O’Sullivan, J.F.; Morningstar, J.E.; Yang, Q.; Zheng, B.; Gao, Y.; Jeanfavre, S.; Scott, J.; Fernandez, C.; Zheng, H.; O’Connor, S.; et al. Dimethylguanidino valeric acid is a marker of liver fat and predicts diabetes. J. Clin. Investig. 2017, 127, 4394–4402. [Google Scholar] [CrossRef]
- Eriksen, A.K.; Kyrø, C.; Nørskov, N.P.; Frederiksen, K.; Bach Knudsen, K.-E.; Overvad, K.; Landberg, R.; Tjønneland, A.; Olsen, A. Pre-diagnostic plasma enterolactone concentrations are associated with lower mortality among individuals with type 2 diabetes: A case-cohort study in the Danish Diet, Cancer and Health cohort. Diabetologia 2019, 62, 959–969. [Google Scholar] [CrossRef]
- Fleschhut, J.; Kratzer, F.; Rechkemmer, G.; Kulling, S.E. Stability and biotransformation of various dietary anthocyanins in vitro. Eur. J. Nutr. 2006, 45, 7–18. [Google Scholar] [CrossRef]
- Sannino, F.; Sansone, C.; Galasso, C.; Kildgaard, S.; Tedesco, P.; Fani, R.; Marino, G.; de Pascale, D.; Ianora, A.; Parrilli, E.; et al. Pseudoalteromonas haloplanktis TAC125 produces 4-hydroxybenzoic acid that induces pyroptosis in human A459 lung adenocarcinoma cells. Sci. Rep. 2018, 8, 1190. [Google Scholar] [CrossRef]
- Ordóñez, J.L.; Pereira-Caro, G.; Ludwig, I.; Muñoz-Redondo, J.M.; Ruiz-Moreno, M.J.; Crozier, A.; Moreno-Rojas, J.M. A critical evaluation of the use of gas chromatography- and high performance liquid chromatography-mass spectrometry techniques for the analysis of microbial metabolites in human urine after consumption of orange juice. J. Chromatogr. A 2018, 1575, 100–112. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Sandhu, A.; Edirisinghe, I.; Burton-Freeman, B. An exploratory study of red raspberry (Rubus idaeus L.) (poly)phenols/metabolites in human biological samples. Food Funct. 2018, 9, 806–818. [Google Scholar] [CrossRef] [PubMed]
- Hurtado-Barroso, S.; Quifer-Rada, P.; Marhuenda-Muñoz, M.; Rinaldi de Alvarenga, J.F.J.F.; Tresserra-Rimbau, A.; Lamuela-Raventós, R.M.R.M. Increase of 4-hydroxybenzoic, a bioactive phenolic compound, after an organic intervention diet. Antioxidants 2019, 8, 340. [Google Scholar] [CrossRef] [PubMed]
- El Mohsen, M.A.; Marks, J.; Kuhnle, G.; Moore, K.; Debnam, E.; Srai, S.K.; Rice-Evans, C.; Spencer, J.P.E. Absorption, tissue distribution and excretion of pelargonidin and its metabolites following oral administration to rats. Br. J. Nutr. 2006, 95, 51–58. [Google Scholar] [CrossRef] [PubMed]
- De Ferrars, R.M.; Czank, C.; Zhang, Q.; Botting, N.P.; Kroon, P.A.; Cassidy, A.; Kay, C.D. The pharmacokinetics of anthocyanins and their metabolites in humans. Br. J. Pharmacol. 2014, 171, 3268–3282. [Google Scholar] [CrossRef]
- Wang, Y.; Hekimi, S. Understanding Ubiquinone. Trends Cell Biol. 2016, 26, 367–378. [Google Scholar] [CrossRef]
- McCarty, M.F. Can correction of sub-optimal coenzyme Q status improve b-cell function in type II diabetics? Med. Hypotheses 1999, 52, 397–400. [Google Scholar] [CrossRef]
- Fazakerley, D.J.; Chaudhuri, R.; Yang, P.; Maghzal, G.J.; Thomas, K.C.; Krycer, J.R.; Humphrey, S.J.; Parker, B.L.; Fisher-Wellman, K.H.; Meoli, C.C.; et al. Mitochondrial CoQ deficiency is a common driver of mitochondrial oxidants and insulin resistance. eLife 2018, 7, e32111. [Google Scholar] [CrossRef]
- Yoo, J.-Y.; Yum, K.-S. Effect of coenzyme q 10 on insulin resistance in Korean patients with prediabetes: A pilot single-center, randomized, double-blind, placebo-controlled study. BioMed Res. Int. 2018, 2018, 1613247. [Google Scholar] [CrossRef]
- Wolff, S.P. Diabetes mellitus and free radicals. Br. Med. Bull. 1993, 49, 642–652. [Google Scholar] [CrossRef]
- Ho, C.-C.; Chang, P.-S.; Chen, H.-W.; Lee, P.-F.; Chang, Y.-C.; Tseng, C.-Y.; Lin, P.-T. Ubiquinone supplementation with 300 mg on glycemic control and antioxidant status in athletes: A randomized, double-blinded, placebo-controlled trial. Antioxidants 2020, 9, 823. [Google Scholar] [CrossRef]
- Hodgson, J.; Watts, G.; Playford, D.; Burke, V.; Croft, K. Coenzyme Q10 improves blood pressure and glycaemic control: A controlled trial in subjects with type 2 diabetes. Eur. J. Clin. Nutr. 2002, 56, 1137–1142. [Google Scholar] [CrossRef]
- Yen, C.-H.; Chu, Y.-J.; Lee, B.-J.; Lin, Y.-C.; Lin, P.-T. Effect of liquid ubiquinol supplementation on glucose, lipids and antioxidant capacity in type 2 diabetes patients: A double-blind, randomised, placebo-controlled trial. Br. J. Nutr. 2018, 120, 57–63. [Google Scholar] [CrossRef]
- Amin, M.M.; Asaad, G.F.; Abdel Salam, R.M.; El-Abhar, H.S.; Arbid, M.S. Novel CoQ10 antidiabetic mechanisms underlie its positive effect: Modulation of insulin and adiponectine receptors, tyrosine kinase, PI3K, glucose transporters, sRAGE and visfatin in insulin resistant/diabetic rats. PLoS ONE 2014, 9, e89169. [Google Scholar] [CrossRef]
- Tresserra-Rimbau, A.; Castro-Barquero, S.; Vitelli-Storelli, F.; Becerra-Tomas, N.; Vázquez-Ruiz, Z.; Díaz-López, A.; Corella, D.; Castañer, O.; Romaguera, D.; Vioque, J.; et al. Associations between dietary polyphenols and type 2 diabetes in a cross-sectional analysis of the PREDIMED-Plus trial: Role of body mass index and sex. Antioxidants 2019, 8, 537. [Google Scholar] [CrossRef]
- Markowiak, P.; Śliżewska, K. Effects of probiotics, prebiotics, and synbiotics on human health. Nutrients 2017, 9, 1021. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of health claims related to polyphenols in olive and protection of LDL particles from oxidative damage (ID 1333, 1638, 1639, 1696, 2865), maintenance of normal blood HDL cholesterol concentrations (ID 1639), maintenance of normal blood pressure (ID 3781), “anti-inflammatory properties” (ID 1882), “contributes to the upper respiratory tract health” (ID 3468), “can help to maintain a normal function of gastrointestinal tract” (3779), and “contributes to body defences against external agents” (ID 3467) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2011, 9, 2033. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Cases (n = 46) | Controls (n = 126) | p-Value | |
|---|---|---|---|
| Women, n (%) | 26 (56.5) | 84 (66.8) | 0.220 |
| Age (years) | 65.9 ± 6.0 | 67.9 ± 5.7 | 0.039 |
| Intervention group, n (%) | 0.334 | ||
| Mediterranean Diet + EVOO | 18 (39.1) | 54 (42.9) | |
| Mediterranean Diet + nuts | 12 (26.1) | 42 (33.3) | |
| Control | 16 (34.8) | 30 (23.8) | |
| Dyslipidemia, n (%) | 38 (82.6) | 98 (77.8) | 0.491 |
| Hypertension, n (%) | 45 (97.8) | 113 (89.7) | 0.084 |
| BMI (kg/m2) | 30.9 ± 3.0 | 30.6 ± 3.9 | 0.721 |
| Energy intake (Kcal/day) | 2381 ± 544 | 2276 ± 488 | 0.226 |
| Smoking habit, n (%) | 0.682 | ||
| Current smoker | 8 (17.4) | 20 (15.9) | |
| Past smoker | 12 (26.1) | 26 (20.6) | |
| Never smoker | 26 (56.5) | 80 (63.5) | |
| Physical activity (METs-min/day) | 258.2 ± 176.3 | 218.4 ± 208.6 | 0.250 |
| Level of education, n (%) | |||
| High and medium studies | 12 (26.1) | 25 (15.8) | 0.378 |
| Fasting plasma glucose (mg/dL) | 118.8 ± 18.1 | 96.5 ± 12.8 | <0.001 |
| No. of Cases | T1 | T2 | T3 | PTrend | 1-SD Increment | |
|---|---|---|---|---|---|---|
| 58 | 57 | 57 | ||||
| 4-Hydroxybenzoic acid | Basic model | 1.00 (ref) | 0.31 [0.18–0.54] | 0.81 [0.38–1.71] | 0.579 | 0.91 [0.70–1.19] |
| Multivariable model 1 | 1.00 (ref) | 0.31 [0.19–0.53] | 0.88 [0.31–2.49] | 0.813 | 0.94 [0.70–1.26] | |
| Multivariable model 2 | 1.00 (ref) | 0.22 [0.14–0.36] | 0.67 [0.30–1.48] | 0.284 | 0.78 [0.60–1.01] | |
| Hydroxybenzoic acid glucuronide | Basic model | 1.00 (ref) | 0.54 [0.34–0.86] | 0.41 [0.26–0.65] | <0.001 | 0.63 [0.51–0.79] |
| Multivariable model 1 | 1.00 (ref) | 0.52 [0.32–0.86] | 0.39 [0.24–0.64] | <0.001 | 0.61 [0.49–0.77] | |
| Multivariable model 2 | 1.00 (ref) | 0.49 [0.13–1.84] | 0.61 [0.19–1.97] | 0.341 | 0.69 [0.44–1.09] | |
| Enterolactone glucuronide | Basic model | 1.00 (ref) | 0.97 [0.40–2.35] | 0.79 [0.54–1.14] | 0.208 | 1.08 [0.93–1.25] |
| Multivariable model 1 | 1.00 (ref) | 1.05 [0.51–2.13] | 0.73 [0.45–1.19] | 0.209 | 1.10 [0.89–1.36] | |
| Multivariable model 2 | 1.00 (ref) | 1.17 [0.79–1.73] | 0.79 [0.29–2.13] | 0.789 | 1.06 [0.73–1.54] | |
| m-coumaric acid | Basic model | 1.00 (ref) | 1.35 [0.75–2.44] | 1.78 [0.82–3.87] | 0.147 | 1.26 [0.97–1.63] |
| Multivariable model 1 | 1.00 (ref) | 1.48 [0.75–2.91] | 1.71 [0.89–3.32] | 0.110 | 1.24 [0.99–1.55] | |
| Multivariable model 2 | 1.00 (ref) | 1.46 [1.13–1.89] | 1.58 [0.91–2.73] | 0.110 | 1.11 [0.96–1.30] | |
| Hydroxytyrosol sulphate | Basic model | 1.00 (ref) | 0.54 [0.41–0.72] | 0.57 [0.22–1.50] | 0.258 | 0.93 [0.58–1.49] |
| Multivariable model 1 | 1.00 (ref) | 0.59 [0.51–0.68] | 0.57 [0.30–1.09] | 0.090 | 0.94 [0.63–1.39] | |
| Multivariable model 2 | 1.00 (ref) | 0.38 [0.17–0.86] | 0.34 [0.07–1.72] | 0.265 | 0.71 [0.31–1.65] | |
| Protocatechuic acid | Basic model | 1.00 (ref) | 1.51 [0.40–5.67] | 1.75 [0.73–4.20] | 0.208 | 1.26 [0.87–1.83] |
| Multivariable model 1 | 1.00 (ref) | 1.83 [0.54–6.15] | 1.91 [0.83–4.40] | 0.129 | 1.30 [0.91–1.87] | |
| Multivariable model 2 | 1.00 (ref) | 3.00 [0.75–12.02] | 2.08 [0.89–4.88] | 0.068 | 1.35 [0.85–2.13] | |
| Vanillic acid glucuronide | Basic model | 1.00 (ref) | 0.99 [0.48–2.04] | 0.76 [0.31–1.84] | 0.546 | 0.94 [0.60–1.48] |
| Multivariable model 1 | 1.00 (ref) | 0.95 [0.39–2.35] | 0.89 [0.48–1.63] | 0.702 | 1.04 [0.71–1.50] | |
| Multivariable model 2 | 1.00 (ref) | 1.17 [0.44–3.10] | 1.53 [0.61–3.81] | 0.399 | 1.31 [0.82–2.08] | |
| Vanillic acid sulphate | Basic model | 1.00 (ref) | 0.83 [0.74–0.93] | 1.13 [0.71–1.81] | 0.608 | 1.02 [0.75–1.38] |
| Multivariable model 1 | 1.00 (ref) | 0.87 [0.77–0.97] | 1.11 [0.79–1.55] | 0.554 | 1.01 [0.79–1.31] | |
| Multivariable model 2 | 1.00 (ref) | 0.76 [0.29–2.01] | 1.38 [0.97–1.97] | 0.046 | 1.06 [0.70–1.61] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marhuenda-Muñoz, M.; Domínguez-López, I.; Laveriano-Santos, E.P.; Parilli-Moser, I.; Razquin, C.; Ruiz-Canela, M.; Basterra-Gortari, F.J.; Corella, D.; Salas-Salvadó, J.; Fitó, M.; et al. One-Year Changes in Urinary Microbial Phenolic Metabolites and the Risk of Type 2 Diabetes—A Case-Control Study. Antioxidants 2022, 11, 1540. https://doi.org/10.3390/antiox11081540
Marhuenda-Muñoz M, Domínguez-López I, Laveriano-Santos EP, Parilli-Moser I, Razquin C, Ruiz-Canela M, Basterra-Gortari FJ, Corella D, Salas-Salvadó J, Fitó M, et al. One-Year Changes in Urinary Microbial Phenolic Metabolites and the Risk of Type 2 Diabetes—A Case-Control Study. Antioxidants. 2022; 11(8):1540. https://doi.org/10.3390/antiox11081540
Chicago/Turabian StyleMarhuenda-Muñoz, María, Inés Domínguez-López, Emily P. Laveriano-Santos, Isabella Parilli-Moser, Cristina Razquin, Miguel Ruiz-Canela, Francisco Javier Basterra-Gortari, Dolores Corella, Jordi Salas-Salvadó, Montserrat Fitó, and et al. 2022. "One-Year Changes in Urinary Microbial Phenolic Metabolites and the Risk of Type 2 Diabetes—A Case-Control Study" Antioxidants 11, no. 8: 1540. https://doi.org/10.3390/antiox11081540