
Alveolar Nitric Oxide as a Biomarker of COVID-19 Lung Sequelae: A Pivotal Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Study Design
- -
- Inability or refusal to provide informed consent
- -
- Comorbidities that may influence FeNO values: asthma, allergic diseases, bronchiectasis, cystic fibrosis, pulmonary arterial hypertension, pre-existent interstitial lung disease, chronic rhinosinusitis, with or without nasal polyps
- -
- Ongoing treatment with oral phosphodiesterase-5 inhibitors, oral or inhaled corticosteroids.
2.2. Pulmonary Function Tests
2.3. Multiple-Flow FeNO Assessment and Analysis
2.4. Statistical Analysis
3. Results
3.1. Study Population
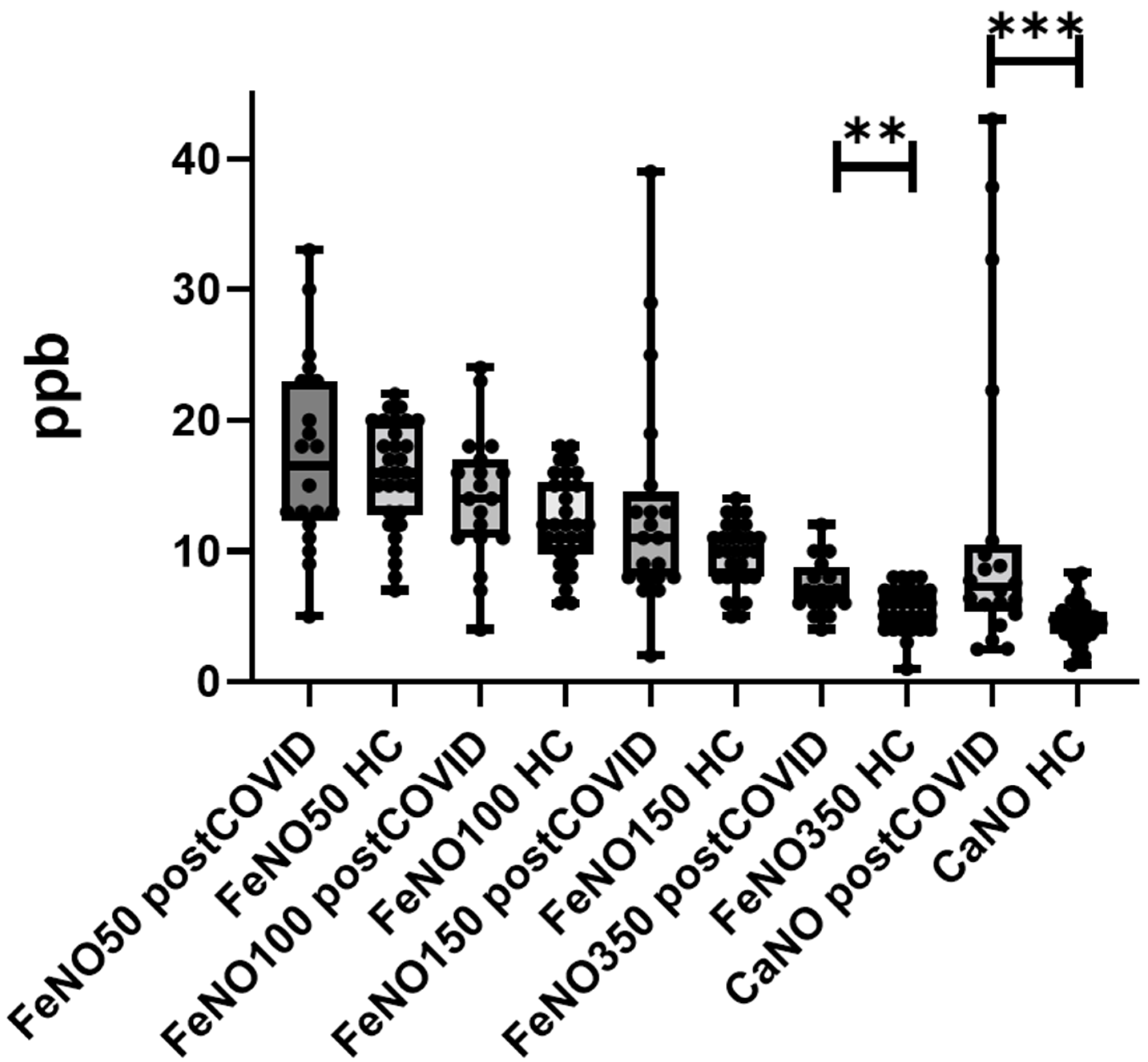
3.2. FeNO Measurements
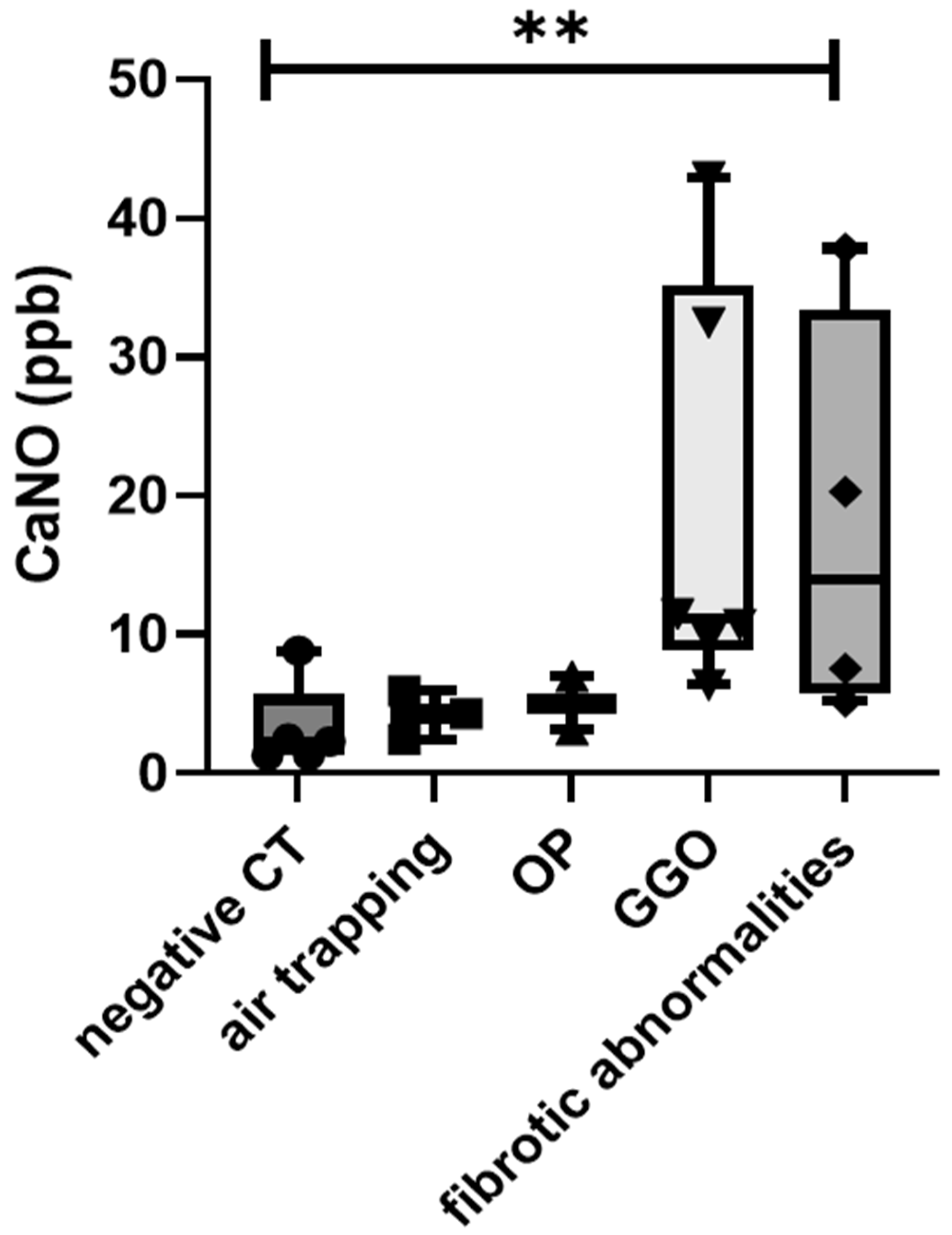
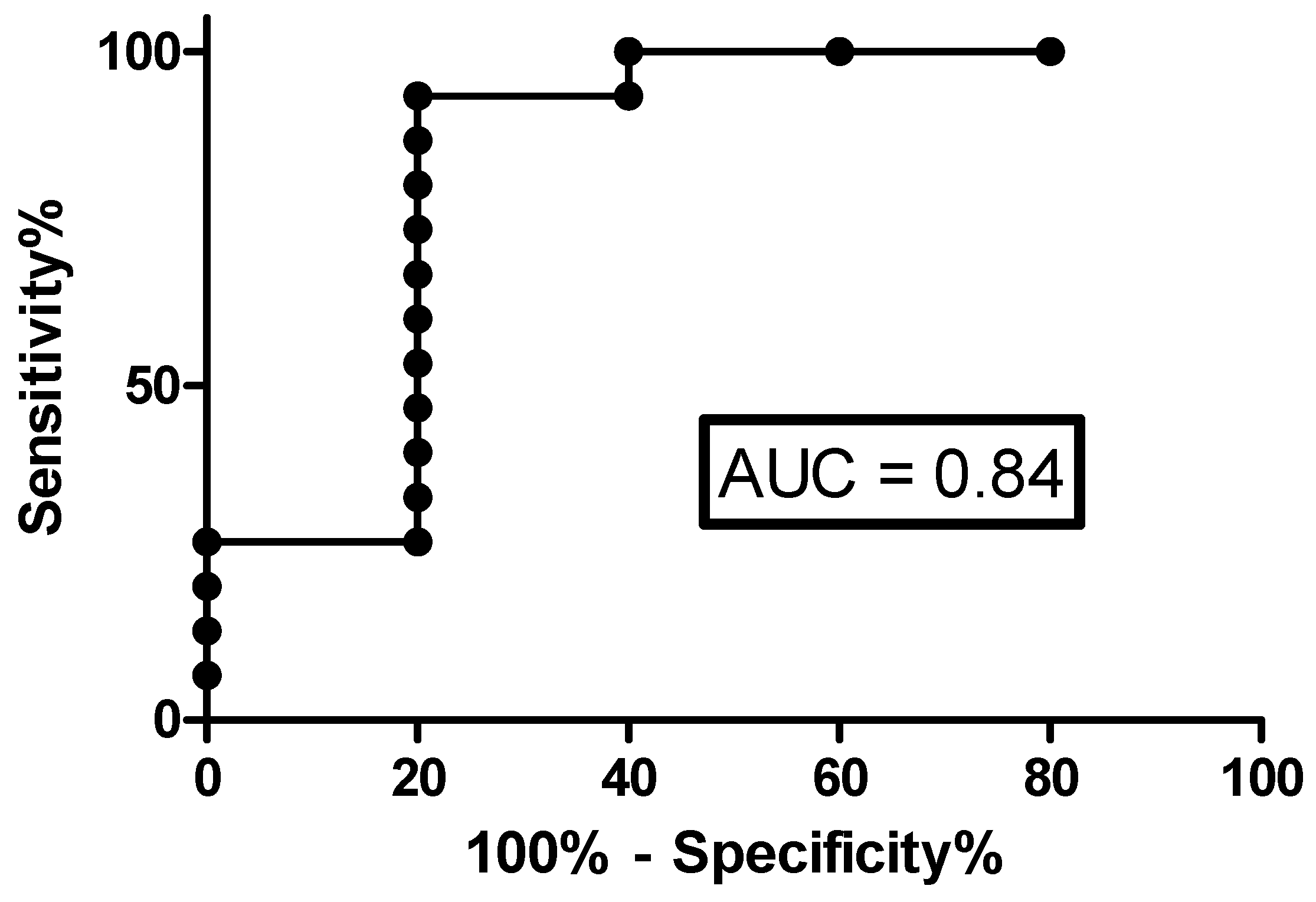
3.3. Correlations with Radiological Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Director-General’s Opening Remarks at the Media Briefing on COVID-19–11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 17 July 2021).
- Li, X.; Ma, X. Acute respiratory failure in COVID-19: Is it ‘typical’ ARDS? Crit. Care Lond Engl. 2020, 24, 198. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Izcovich, A.; Kum, E.; Pardo-Hernandez, H.; Qasim, A.; Martinez, J.P.D.; Rochwerg, B.; et al. Drug treatments for covid-19: Living systematic review and network meta-analysis. BMJ 2020, 370, m2980. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; Jarvis, H.C.; et al. ‘Long-COVID’: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2021, 76, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Burnham, E.L.; Janssen, W.J.; Riches, D.W.H.; Moss, M.; Downey, G.P. The fibroproliferative response in acute respiratory distress syndrome: Mechanisms and clinical significance. Eur. Respir. J. 2014, 43, 276–285. [Google Scholar] [CrossRef] [Green Version]
- Burnham, E.L.; Hyzy, R.C.; Paine, R.; Kelly, A.M.; Quint, L.E.; Lynch, D.; Curran-Everett, D.; Moss, M.; Standiford, T.J. Detection of Fibroproliferation by Chest High-Resolution CT Scan in Resolving ARDS. Chest 2014, 146, 1196–1204. [Google Scholar] [CrossRef] [Green Version]
- Chioma, O.; Drake, W.P. Role of Microbial Agents in Pulmonary Fibrosis. Yale J. Boil. Med. 2017, 90, 219–227. [Google Scholar]
- Furuhashi, M.; Moniwa, N.; Takizawa, H.; Ura, N.; Shimamoto, K. Potential differential effects of renin-angiotensin system inhibitors on SARS-CoV-2 infection and lung injury in COVID-19. Hypertens. Res. 2020, 43, 837–840. [Google Scholar] [CrossRef]
- Sigrist, C.J.; Bridge, A.; Le Mercier, P. A potential role for integrins in host cell entry by SARS-CoV-2. Antivir. Res. 2020, 177, 104759. [Google Scholar] [CrossRef]
- George, P.M.; Wells, A.U.; Jenkins, R.G. Pulmonary fibrosis and COVID-19: The potential role for antifibrotic therapy. Lancet Respir. Med. 2020, 8, 807–815. [Google Scholar] [CrossRef]
- Mineo, G.; Ciccarese, F.; Modolon, C.; Landini, M.P.; Valentino, M.; Zompatori, M. Post-ARDS pulmonary fibrosis in patients with H1N1 pneumonia: Role of follow-up CT. La Radiol. Med. 2012, 117, 185–200. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Fan, Y.; Alwalid, O.; Li, N.; Jia, X.; Yuan, M.; Li, Y.; Cao, Y.; Gu, J.; Wu, H.; et al. Six-month Follow-up Chest CT Findings after Severe COVID-19 Pneumonia. Radiology 2021, 299, E177–E186. [Google Scholar] [CrossRef]
- Bardakci, M.I.; Ozturk, E.N.; Ozkarafakili, M.A.; Ozkurt, H.; Yanc, U.; Sevgi, D.Y. Evaluation of long-term radiological findings, pulmonary functions, and health-related quality of life in survivors of severe COVID-19. J. Med. Virol. 2021, 93, 5574–5581. [Google Scholar] [CrossRef]
- d’Alessandro, M.; Bergantini, L.; Cameli, P.; Curatola, G.; Remediani, L.; Bennett, D.; Bianchi, F.; Perillo, F.; Volterrani, L.; Mazzei, M.A.; et al. Serial KL-6 measurements in COVID-19 patients. Intern. Emerg. Med. 2021, 16, 1541–1545. [Google Scholar] [CrossRef] [PubMed]
- Cameli, P.; Bargagli, E.; Bergantini, L.; D’Alessandro, M.; Pieroni, M.; Fontana, G.A.; Sestini, P.; Refini, R.M. Extended Exhaled Nitric Oxide Analysis in Interstitial Lung Diseases: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 6187. [Google Scholar] [CrossRef]
- Janssen, W.; Pullamsetti, S.S.; Cooke, J.; Weissmann, N.; Guenther, A.; Schermuly, R.T. The role of dimethylarginine dimethylaminohydrolase (DDAH) in pulmonary fibrosis. J. Pathol. 2013, 229, 242–249. [Google Scholar] [CrossRef]
- Romanska-Knight, H.; Polak, J.M.; Coleman, R.A.; James, R.S.; Harmer, D.W.; Allen, J.C.; Bishop, A.E. iNOS gene upregulation is associated with the early proliferative response of human lung fibroblasts to cytokine stimulation. J. Pathol. 2002, 197, 372–379. [Google Scholar] [CrossRef]
- Iyer, A.K.V.; Ramesh, V.; Castro, C.A.; Kaushik, V.; Kulkarni, Y.M.; Wright, C.A.; Venkatadri, R.; Rojanasakul, Y.; Azad, N. Nitric oxide mediates bleomycin-induced angiogenesis and pulmonary fibrosis via regulation of VEGF. J. Cell. Biochem. 2015, 116, 2484–2493. [Google Scholar] [CrossRef] [Green Version]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Crapo, R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; van der Grinten, C.M.; Gustafsson, P.; et al. General considerations for lung function testing. Eur. Respir. J. 2005, 26, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, B.L.; Brusasco, V.; Burgos, F.; Cooper, B.G.; Jensen, R.; Kendrick, A.; MacIntyre, N.R.; Thompson, B.R.; Wanger, J. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Respir. J. 2017, 49, 1600016. [Google Scholar] [CrossRef] [Green Version]
- Horváth, I.; Barnes, P.J.; Loukides, S.; Sterk, P.J.; Högman, M.; Olin, A.-C.; Amann, A.; Antus, B.; Baraldi, E.; Bikov, A.; et al. A European Respiratory Society technical standard: Exhaled biomarkers in lung disease. Eur. Respir. J. 2017, 49, 1600965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebner, L.; Funke-Chambour, M.; Von Garnier, C.; Ferretti, G.; Ghaye, B.; Beigelman-Aubry, C. Imaging in the aftermath of COVID-19: What to expect. Eur. Radiol. 2020, 31, 4390–4392. [Google Scholar] [CrossRef]
- Lee, J.-U.; Choi, I.-S.; Park, K.-O.; Lee, J.H.; Park, S.-W.; Park, C.-S.; Jang, A.-S. Expression of nitric oxide synthase, aquaporin 1 and aquaporin 5 in rat after bleomycin inhalation. Intensiv. Care Med. 2004, 30, 489–495. [Google Scholar] [CrossRef]
- Sato, Y.; Chibana, K.; Horigane, Y.; Uchida, N.; Masawa, M.; Koike, R.; Nakamura, Y.; Watanabe, T.; Shiobara, T.; Arai, R.; et al. Comparison of inducible nitric oxide synthase mRNA expression in different airway portions and association with nitric oxide parameters from patients with asthma. Clin. Exp. Allergy 2018, 49, 582–590. [Google Scholar] [CrossRef] [Green Version]
- Cameli, P.; Bargagli, E.; Refini, R.; Pieroni, M.; Bennett, D.; Rottoli, P. Exhaled nitric oxide in interstitial lung diseases. Respir. Physiol. Neurobiol. 2014, 197, 46–52. [Google Scholar] [CrossRef]
- Cameli, P.; Bargagli, E.; Bergantini, L.; Refini, R.M.; Pieroni, M.; Sestini, P.; Rottoli, P. Evaluation of multiple-flows exhaled nitric oxide in idiopathic and non-idiopathic interstitial lung disease. J. Breath Res. 2019, 13, 026008. [Google Scholar] [CrossRef] [PubMed]
- Torres-Castro, R.; Vasconcello-Castillo, L.; Alsina-Restoy, X.; Solis-Navarro, L.; Burgos, F.; Puppo, H.; Vilaró, J. Respiratory function in patients post-infection by COVID-19: A systematic review and meta-analysis. Pulmonology 2020, 27, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.; Wong, A.W.; Hague, C.J.; Murphy, D.T.; Johnston, J.C.; Ryerson, C.J.; Carlsten, C. A prospective study of 12-week respiratory outcomes in COVID-19-related hospitalisations. Thorax 2021, 76, 402–404. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Bai, W.; Yue, J.; Qin, L.; Zhang, C.; Xu, S.; Liu, X.; Ni, W.; Xie, M. Eight months follow-up study on pulmonary function, lung radiographic, and related physiological characteristics in COVID-19 survivors. Sci. Rep. 2021, 11, 13584. [Google Scholar]
- Mo, X.; Jian, W.; Su, Z.; Chen, M.; Peng, H.; Peng, P.; Lei, C.; Chen, R.; Zhong, N.; Li, S. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur. Respir. J. 2020, 55, 2001217. [Google Scholar] [CrossRef]
- Barisione, G.; Brusasco, C.; Garlaschi, A.; Baroffio, M.P.; Brusasco, V. Lung diffusing capacity for nitric oxide as a marker of fibrotic changes in idiopathic interstitial pneumonias. J. Appl. Physiol. 2016, 120, 1029–1038. [Google Scholar] [CrossRef] [Green Version]
- Barisione, G.; Garlaschi, A.; Occhipinti, M.; Baroffio, M.; Pistolesi, M.; Brusasco, V. Value of lung diffusing capacity for nitric oxide in systemic sclerosis. Physiol. Rep. 2019, 7, e14149. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Post-COVID | Healthy Controls | p-Value |
|---|---|---|---|
| N° | 20 | 22 | |
| Age (years) | 60 ± 14.3 | 58.5 ± 7.4 | 0.6648 |
| Male (%) | 13 (65) | 15 (68.2) | 0.9851 |
| Smoking status (pack/year) | 10.6 ± 5.4 | 8.4 ± 6.6 | 0.2567 |
| BMI (kg/m2) | 24.3 ± 5.4 | 23.8 ± 4.3 | 0.5598 |
| Time from onset to hospitalization (d) | 8.5 ± 4.3 | ||
| Length hospital stay (d) | 16.7 ± 14.2 | ||
| Acute respiratory failure (%) | 14 (70) | ||
| ICU admittance (%) | 4 (20) | ||
| Therapy | |||
| Steroid (%) | 14 (70) | ||
| Remdesivir (%) | 5 (25) | ||
| Anti IL-6 drugs (%) | 6 (30) | ||
| PFTs | |||
| FVC l (%) | 3.6 ± 1.2 (99 ± 21) | ||
| FEV1 l (%) | 2.7 ± 0.9 (92.8 ± 17.2) | ||
| FEV1/FVC | 76.2 ± 9.2 | ||
| RV l (%) | 2.2 ± 0.6 (99.6 ± 19.8) | ||
| TLC l (%) | 5.9 ±1.2 (95.5 ± 15) | ||
| DLCO % | 94 ± 19.3 | ||
| KCO % | 106.5 ± 21.5 | ||
| CT features | |||
| Negative (%) | 5 (25) | ||
| Air trapping (%) | 3 (15) | ||
| OP (%) | 2 (10) | ||
| GGO (%) | 6 (30) | ||
| Fibrotic abnormalities (%) | 4 (20) |
| Multiple-Flows FeNOParameters | Post-COVID | Healthy Controls | p-Value |
|---|---|---|---|
| FeNO 50 (ppb) | 17.3 ± 7.2 | 15.8 ± 4.1 | 0.6336 * |
| Min-max; 25–75 percentile (ppb) | 5–33; 12.2–23 | 7–22; 12.7–20 | Chi-square 0.53, p = 0.817 ° |
| FeNO 100 (ppb) | 14.1 ± 5.1 | 12.2 ± 3.5 | 0.1675 * |
| Min-max; 25–75 percentile (ppb) | 4–24; 11–17 | 6–18; 9.7–15.2 | Chi-square 2.49, p = 0.114 ° |
| FeNO 150 (ppb) | 13.3 ± 8.7 | 9.7 ± 2.4 | 0.2437 * |
| Min-max; 25–75 percentile (ppb) | 2–39; 8–14.5 | 5–14; 8–11.2 | Chi-square 0.65, p = 0.419 ° |
| FeNO 350 (ppb) | 7.2 ± 2.1 | 5.6 ± 1.6 | 0.0199 * |
| Min-max; 25–75 percentile (ppb) | 4–12; 6–8.7 | 1–8; 4–7 | Chi-square 4.18, p = 0.041 ° |
| J’awNO (nL/min) | 44.1 ± 31.9 | 45.3 ± 22.3 | 0.6936 * |
| Min-max; 25–75 percentile (ppb) | 2.8–129.8; 18.6–57.4 | 5.6–90.4; 28.5–54.9 | Chi-square 0.35, p = 0.551 ° |
| CaNO (ppb) | 9.7 ± 6.1 | 4.5 ± 1.6 | 0.0081 * |
| Min-max; 25–75 percentile (ppb) | 1.3–43.1; 5.8–20.6 | 1.2–8.3; 3.6–5.3 | Chi-square 7.57, p = 0.006 ° |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cameli, P.; Bargagli, E.; Bergantini, L.; d’Alessandro, M.; Giugno, B.; Gentili, F.; Sestini, P. Alveolar Nitric Oxide as a Biomarker of COVID-19 Lung Sequelae: A Pivotal Study. Antioxidants 2021, 10, 1350. https://doi.org/10.3390/antiox10091350
Cameli P, Bargagli E, Bergantini L, d’Alessandro M, Giugno B, Gentili F, Sestini P. Alveolar Nitric Oxide as a Biomarker of COVID-19 Lung Sequelae: A Pivotal Study. Antioxidants. 2021; 10(9):1350. https://doi.org/10.3390/antiox10091350
Chicago/Turabian StyleCameli, Paolo, Elena Bargagli, Laura Bergantini, Miriana d’Alessandro, Bruna Giugno, Francesco Gentili, and Piersante Sestini. 2021. "Alveolar Nitric Oxide as a Biomarker of COVID-19 Lung Sequelae: A Pivotal Study" Antioxidants 10, no. 9: 1350. https://doi.org/10.3390/antiox10091350