
Navigated Transcranial Magnetic Stimulation Motor Mapping and Diffusion Tensor Imaging Tractography for Diencephalic Tumor in Pediatric Patients
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Material and Methods
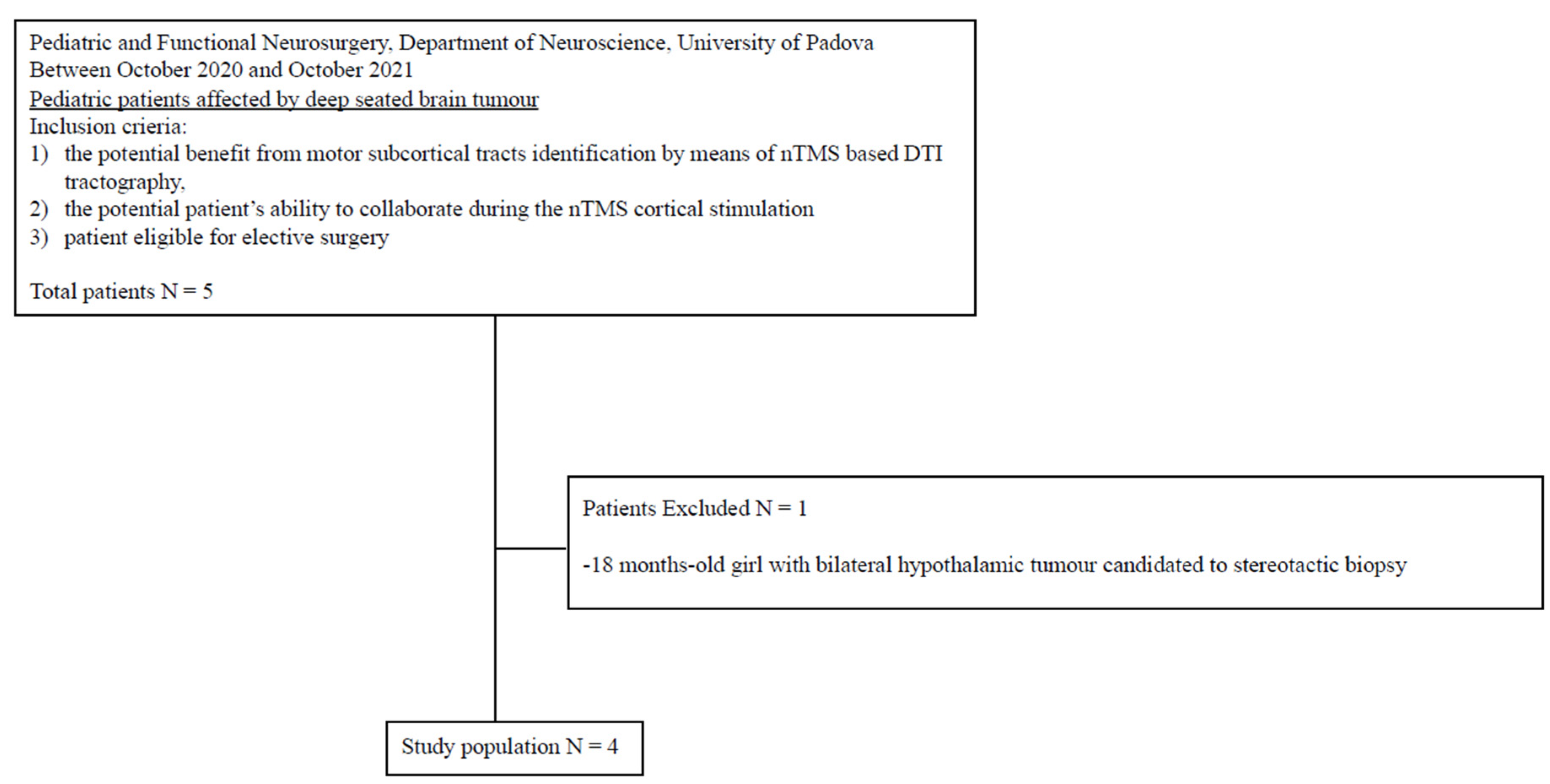
2.1. Patient Selection
2.2. Patient Informed Consent and Ethical Approval
2.3. MRI Acquisition
2.4. nTMS Motor Mapping
2.5. Tractography
3. Results
3.1. Patient Sample
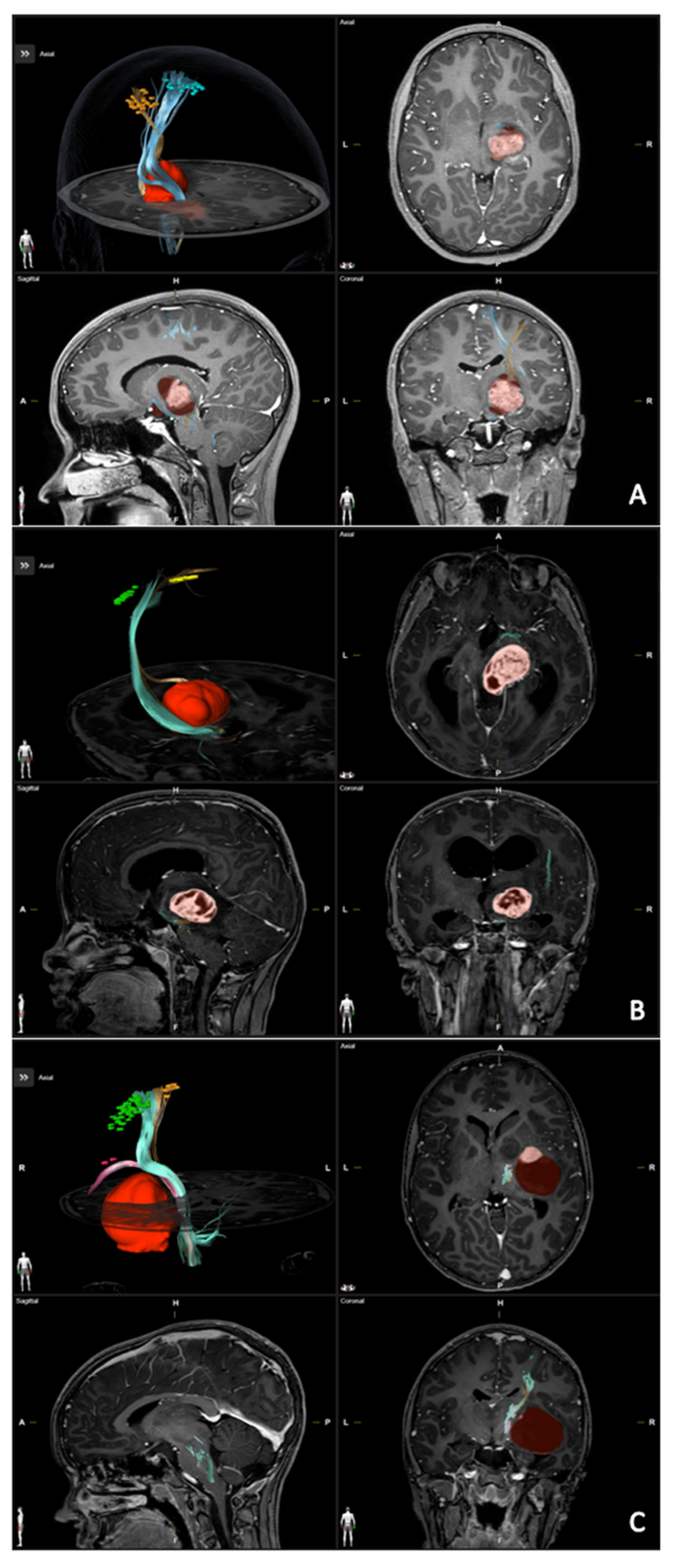
3.2. nTMS and Tractography
3.3. Surgery and Outcome
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Picht, T.; Schmidt, S.; Brandt, S.; Frey, D.; Hannula, H.; Neuvonen, T.; Karhu, J.; Vajkoczy, P.; Suess, O. Preoperative functional mapping for rolandic brain tumor surgery: Comparison of navigated transcranial magnetic stimulation to direct cortical stimulation. Neurosurgery 2011, 69, 581–588. [Google Scholar] [CrossRef]
- Tarapore, P.E.; Findlay, A.M.; Honma, S.M.; Mizuiri, D.; Houde, J.F.; Berger, M.S.; Nagarajan, S.S. Language mapping with navigated repetitive TMS: Proof of technique and validation. NeuroImage 2013, 82, 260–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sollmann, N.; Wildschuetz, N.; Kelm, A.; Conway, N.; Moser, T.; Bulubas, L.; Kirschke, J.S.; Meyer, B.; Krieg, S.M. Associations between clinical outcome and navigated transcranial magnetic stimulation characteristics in patients with motor-eloquent brain lesions: A combined navigated transcranial magnetic stimulation-diffusion tensor imaging fiber tracking approach. J. Neurosurg. 2018, 128, 800–810. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, T.; Grittner, U.; Acker, G.; Schwarzer, V.; Kulchytska, N.; Vajkoczy, P.; Picht, T. Risk stratification in motor area-related glioma surgery based on navigated transcranial magnetic stimulation data. J. Neurosurg. 2017, 126, 1227–1237. [Google Scholar] [CrossRef] [Green Version]
- Picht, T.; Frey, D.; Thieme, S.; Kliesch, S.; Vajkoczy, P. Presurgical navigated TMS motor cortex mapping improves outcome in glioblastoma surgery: A controlled observational study. J. Neurooncol. 2016, 126, 535–543. [Google Scholar] [CrossRef]
- Tarapore, P.E.; Picht, T.; Bulubas, L.; Shin, Y.; Kulchytska, N.; Meyer, B.; Berger, M.S.; Nagarajan, S.S.; Krieg, S.M. Safety and tolerability of navigated TMS for preoperative mapping in neurosurgical patients. Clin. Neurophysiol. 2016, 127, 1895–1900. [Google Scholar] [CrossRef]
- Krings, T.; Foltys, H.; Reinges, M.H.T.; Kemeny, S.; Rohde, V.; Spetzger, U.; Gilsbach, J.M.; Thron, A. Navigated Transcranial Magnetic Stimulation for Presurgical Planning Correlation with Functional MRI. Minim. Invasive Neurosurg. 2001, 44, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Vitikainen, A.M.; Salli, E.; Lioumis, P.; Mäkelä, J.P.; Metsähonkala, L. Applicability of nTMS in locating the motor cortical representation areas in patients with epilepsy. Acta Neurochir. 2013, 155, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Krieg, S.M.; Sollmann, N.; Hauck, T.; Ille, S.; Meyer, B.; Ringel, F. Repeated mapping of cortical language sites by preoperative navigated transcranial magnetic stimulation compared to repeated intraoperative DCS mapping in awake craniotomy. BMC Neurosci. 2014, 15, 20. [Google Scholar] [CrossRef] [Green Version]
- Ille, S.; Sollmann, N.; Hauck, T.; Maurer, S.; Tanigawa, N.; Obermueller, T.; Negwer, C.; Droese, D.; Boeckh-Behrens, T.; Meyer, B.; et al. Impairment of preoperative language mapping by lesion location: A functional magnetic resonance imaging, navigated transcranial magnetic stimulation, and direct cortical stimulation study. J. Neurosurg. 2015, 123, 314–324. [Google Scholar] [CrossRef] [Green Version]
- Jeltema, H.R.; Ohlerth, A.K.; de Wit, A.; Wagemakers, M.; Rofes, A.; Bastiaanse, R.; Drost, G. Comparing navigated transcranial magnetic stimulation mapping and “gold standard” direct cortical stimulation mapping in neurosurgery: A systematic review. Neurosurg. Rev. 2021, 44, 1903–1920. [Google Scholar] [CrossRef] [PubMed]
- Krieg, S.M.; Lioumis, P.; Mäkelä, J.P.; Wilenius, J.; Karhu, J.; Hannula, H.; Savolainen, P.; Lucas, C.W.; Seidel, K.; Laakso, A.; et al. Protocol for motor and language mapping by navigated TMS in patients and healthy volunteers; workshop report. Acta Neurochir. 2017, 159, 1187–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picht, T.; Krieg, S.M.; Sollmann, N.; Rösler, J.; Niraula, B.; Neuvonen, T.; Savolainen, P.; Lioumis, P.; Mäkelä, J.P.; Deletis, V.; et al. A comparison of language mapping by preoperative navigated transcranial magnetic stimulation and direct cortical stimulation during awake surgery. Neurosurgery 2013, 72, 808–819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ille, S.; Sollmann, N.; Hauck, T.; Maurer, S.; Tanigawa, N.; Obermueller, T.; Negwer, C.; Droese, D.; Zimmer, C.; Meyer, B.; et al. Combined noninvasive language mapping by navigated transcranial magnetic stimulation and functional MRI and its comparison with direct cortical stimulation. J. Neurosurg. 2015, 123, 212–225. [Google Scholar] [CrossRef] [Green Version]
- Haddad, A.F.; Young, J.S.; Berger, M.S.; Tarapore, P.E. Preoperative Applications of Navigated Transcranial Magnetic Stimulation. Front. Neurol. 2021, 11, 628903. [Google Scholar] [CrossRef]
- Sollmann, N.; Zhang, H.; Schramm, S.; Ille, S.; Negwer, C.; Kreiser, K.; Meyer, B.; Krieg, S.M. Function-specific Tractography of Language Pathways Based on nTMS Mapping in Patients with Supratentorial Lesions. Clin. Neuroradiol. 2020, 30, 123–135. [Google Scholar] [CrossRef]
- Sollmann, N.; Negwer, C.; Ille, S.; Maurer, S.; Hauck, T.; Kirschke, J.S.; Ringel, F.; Meyer, B.; Krieg, S.M. Feasibility of nTMS-based DTI fiber tracking of language pathways in neurosurgical patients using a fractional anisotropy threshold. J. Neurosci. Methods 2016, 267, 45–54. [Google Scholar] [CrossRef]
- Raffa, G.; Bährend, I.; Schneider, H.; Faust, K.; Germanò, A.; Vajkoczy, P.; Picht, T. A novel technique for region and linguistic specific nTMS-based DTI fiber tracking of language pathways in brain tumor patients. Front. Neurosci. 2016, 10, 552. [Google Scholar] [CrossRef] [Green Version]
- Raffa, G.; Conti, A.; Scibilia, A.; Sindorio, C.; Quattropani, M.C.; Visocchi, M.; Germanò, A.; Tomasello, F. Functional reconstruction of motor and language pathways based on navigated transcranial magnetic stimulation and DTI fiber tracking for the preoperative planning of low grade glioma surgery: A new tool for preservation and restoration of eloquent networks. Acta Neurochir. Suppl. 2017, 124, 251–261. [Google Scholar]
- Frey, D.; Strack, V.; Wiener, E.; Jussen, D.; Vajkoczy, P.; Picht, T. A new approach for corticospinal tract reconstruction based on navigated transcranial stimulation and standardized fractional anisotropy values. NeuroImage 2012, 62, 1600–1609. [Google Scholar] [CrossRef]
- Rosenstock, T.; Giampiccolo, D.; Schneider, H.; Runge, S.J.; Bährend, I.; Vajkoczy, P.; Picht, T. Specific DTI seeding and diffusivity-analysis improve the quality and prognostic value of TMS-based deterministic DTI of the pyramidal tract. NeuroImage Clin. 2017, 16, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Zdunczyk, A.; Roth, F.; Picht, T.; Vajkoczy, P. Functional DTI tractography in brainstem cavernoma surgery. J. Neurosurg. 2021, 135, 712–721. [Google Scholar] [CrossRef]
- Baro, V.; Caliri, S.; Sartori, L.; Facchini, S.; Guarrera, B.; Zangrossi, P.; Anglani, M.; Denaro, L.; d’Avella, D.; Ferreri, F.; et al. Preoperative repetitive navigated TMS and functional white matter tractography in a bilingual patient with a brain tumor in wernike area. Brain Sci. 2021, 11, 557. [Google Scholar] [CrossRef]
- Lehtinen, H.; Mäkelä, J.P.; Mäkelä, T.; Lioumis, P.; Metsähonkala, L.; Hokkanen, L.; Wilenius, J.; Gaily, E. Language mapping with navigated transcranial magnetic stimulation in pediatric and adult patients undergoing epilepsy surgery: Comparison with extraoperative direct cortical stimulation. Epilepsia Open 2018, 3, 224–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selassie, G.R.-H.; Pegenius, G.; Karlsson, T.; Viggedal, G.; Hallböök, T.; Elam, M. Cortical mapping of receptive language processing in children using navigated transcranial magnetic stimulation. Epilepsy Behav. 2020, 103, 106836. [Google Scholar] [CrossRef]
- Schramm, S.; Mehta, A.; Auguste, K.I.; Tarapore, P.E. Navigated transcranial magnetic stimulation mapping of the motor cortex for preoperative diagnostics in pediatric epilepsy. J. Neurosurg. Pediatr. 2021, 28, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, T.; Picht, T.; Schneider, H.; Vajkoczy, P.; Thomale, U.W. Pediatric navigated transcranial magnetic stimulation motor and language mapping combined with diffusion tensor imaging tractography: Clinical experience. J. Neurosurg. Pediatr. 2020, 26, 583–593. [Google Scholar] [CrossRef]
- Coburger, J.; Karhu, J.; Bittl, M.; Hopf, N.J. First preoperative functional mapping via navigated transcranial magnetic stimulation in a 3-year-old boy: Case report. J. Neurosurg. Pediatr. 2012, 9, 660–664. [Google Scholar] [CrossRef]
- Rosenstock, T.; Picht, T.; Schneider, H.; Koch, A.; Thomale, U.W. Left perisylvian tumor surgery aided by TMS language mapping in a 6-year-old boy: Case report. Child’s Nerv. Syst. 2019, 35, 175–181. [Google Scholar] [CrossRef]
- Udaka, Y.T.; Packer, R.J. Pediatric Brain Tumors. Neurol. Clin. 2018, 36, 533–556. [Google Scholar] [CrossRef]
- Shurtleff, H.; Warner, M.; Poliakov, A.; Bournival, B.; Shaw, D.W.; Ishak, G.; Yang, T.; Karandikar, M.; Saneto, R.P.; Browd, S.R.; et al. Functional magnetic resonance imaging for presurgical evaluation of very young pediatric patients with epilepsy. J. Neurosurg. Pediatr. 2010, 5, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Ogg, R.J.; Laningham, F.H.; Clarke, D.; Einhaus, S.; Zou, P.; Tobias, M.E.; Boop, F.A. Passive range of motion functional magnetic resonance imaging localizing sensorimotor cortex in sedated children: Clinical article. J. Neurosurg. Pediatr. 2009, 4, 317–322. [Google Scholar] [CrossRef]
- Bernal, B.; Grossman, S.; Gonzalez, R.; Altman, N. FMRI Under Sedation: What Is the Best Choice in Children? J. Clin. Med. Res. 2012, 4, 363–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhri, A.F.; Patel, R.M.; Siddiqui, A.; Whitehead, M.T.; Wheless, J.W. Cortical activation through passive-motion functional MRI. Am. J. Neuroradiol. 2015, 36, 1675–1681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Francesco, M.W.; Robertson, S.A.; Karunanayaka, P.; Holland, S.K. BOLD fMRI in infants under sedation: Comparing the impact of pentobarbital and propofol on auditory and language activation. J. Magn. Reson. Imaging 2013, 38, 1184–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gemma, M.; Scola, E.; Baldoli, C.; Mucchetti, M.; Pontesilli, S.; De Vitis, A.; Falini, A.; Beretta, L. Auditory functional magnetic resonance in awake (nonsedated) and propofol-sedated children. Paediatr. Anaesth. 2016, 26, 521–530. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Abbruzzese, G.; Assini, A.; Buccolieri, A.; Schieppati, M.; Trompetto, C. Comparison of intracortical inhibition and facilitation in distaland proximal arm muscles in humans. J. Physiol. 1999, 514, 895–903. [Google Scholar] [CrossRef]
- Weiss Lucas, C.; Tursunova, I.; Neuschmelting, V.; Nettekoven, C.; Oros-Peusquens, A.M.; Stoffels, G.; Faymonville, A.M.; Jon, S.N.; Langen, K.J.; Lockau, H.; et al. Functional MRI vs. navigated TMS to optimize M1 seed volume delineation for DTI tractography. A prospective study in patients with brain tumours adjacent to the corticospinal tract. NeuroImage Clin. 2017, 13, 297–309. [Google Scholar] [CrossRef] [Green Version]
- Bae, E.H.; Schrader, L.M.; Machii, K.; Alonso-Alonso, M.; Riviello, J.J.; Pascual-Leone, A.; Rotenberg, A. Safety and tolerability of repetitive transcranial magnetic stimulation in patients with epilepsy: A review of the literature. Epilepsy Behav. 2007, 10, 521–528. [Google Scholar] [CrossRef]
- Schrader, L.M.; Stern, J.M.; Koski, L.; Nuwer, M.R.; Engel, J. Seizure incidence during single- and paired-pulse transcranial magnetic stimulation (TMS) in individuals with epilepsy. Clin. Neurophysiol. 2004, 115, 2728–2737. [Google Scholar] [CrossRef] [PubMed]
- Oberman, L.M.; Pascual-Leone, A. Report of seizure induced by continuous theta burst stimulation. Brain Stimul. 2009, 2, 246–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunny Tharayil, B.; Gangadhar, B.N.; Thirthalli, J.; Anand, L. Seizure With Single-Pulse Transcranial Magnetic Stimulation in a 35-Year-Old Otherwise-Healthy Patient With Bipolar Disorder. J. ECT 2005, 21, 188–189. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.K.; Knösche, T.R.; Turner, R. White matter integrity, fiber count, and other fallacies: The do’s and don’ts of diffusion MRI. NeuroImage 2013, 73, 239–254. [Google Scholar] [CrossRef]
- Baro, V.; Landi, A.; Brigadoi, S.; Castellaro, M.; Moretto, M.; Anglani, M.; Ermani, M.; Causin, F.; Zanoletti, E.; Denaro, L.; et al. Preoperative Prediction of Facial Nerve in Patients with Vestibular Schwannomas: The Role of Diffusion Tensor Imaging—A Systematic Review. World Neurosurg. 2019, 125, 24–31. [Google Scholar] [CrossRef]
- Castellaro, M.; Moretto, M.; Baro, V.; Brigadoi, S.; Zanoletti, E.; Anglani, M.; Denaro, L.; Dell’Acqua, R.; Landi, A.; Causin, F.; et al. Multishell Diffusion MRI-Based Tractography of the Facial Nerve in Vestibular Schwannoma. AJNR Am. J. Neuroradiol. 2020, 41, 1480–1486. [Google Scholar] [CrossRef]
- Forster, M.T.; Hoecker, A.C.; Kang, J.S.; Quick, J.; Seifert, V.; Hattingen, E.; Hilker, R.; Weise, L.M. Does navigated transcranial stimulation increase the accuracy of tractography? A prospective clinical trial based on intraoperative motor evoked potential monitoring during deep brain stimulation. Neurosurgery 2015, 76, 766–775. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | |
|---|---|---|---|---|
| Preoperative Data | ||||
| Sex | F | F | F | M |
| Age | 12 | 13 | 11 | 9 |
| Tumor location | Right thalamopeduncular | Right thalamopeduncular | Right thalamic | Left thalamic with temporomesial and frontal invasion |
| Tumor volume (cm3) | 12.3 | 19.0 | 36.7 | 42.3 |
| Clinical Presentation | Headache and vomiting | Left hemiparesis and VII deficit, hydrocephalus | Headache and vomiting | Headache and vomiting |
| Motor status MRC grade (UL/IL) | M5/M5 | M3/M3 | M5/M5 | M5/M5 |
| Length of Symptoms (months) | 12 | 7 | 3 | 0.2 |
| Antiseizure medications | None | None | None | None |
| Other | - | NF1 | NF1 | - |
| nTMS Data | |||
| Duration of the session (min) | 73 | 102 | 55 |
| Adverse event | None | None | None |
| RMT upper limb | 43% | 46% | 35% |
| RMT lower limb | 58% | 60% | 58% |
| RMT mouth | Not detected | Not detected | 45% |
| No. stimuli upper limb | 66 | 71 | 97 |
| No. stimuli lower limb | 67 | 75 | 68 |
| No. stimuli mouth | - | - | 48 |
| No. stimuli evoking a MEP for upper limb | 25 | 27 | 45 |
| No. stimuli evoking a MEP for lower limb | 15 | 10 | 38 |
| No. stimuli evoking a MEP mouth | - | - | 10 |
| DTI tractography | |||
| CST identification and localization | Lateral displacement. Bundle for hand: anteriorly and bundle for foot: posteriorly | Anterior displacement of hand bundle, posterolateral displacement of the leg bundle | Medial displacement with bundle for mouth markedly shifted anteriorly |
| FA | Hand: 0.13; foot: 0.16 | Hand: 0.15; foot: 0.08 | Hand: 0.23; foot: 0.24; mouth: 0.29 |
| DTT (mm) | 3 | 3 | 4 |
| Fiber integrity | Displaced but intact | Displaced but intact | Displaced but intact |
| Intraoperative Data | |||
| Approach | Trans-sylvian | Trans-temporal | Trans-temporal |
| IONM | Reduction > 50% | Reduction > 50% | Unchanged |
| Complications | None | None | None |
| Pathology | Pilocytic Astrocytoma | Pilocytic Astrocytoma | Pilocytic Astrocytoma |
| Postoperative data | |||
| Complications | MCA stroke | None | None |
| Residual tumor volume (cm3) | 0.13 (1.1%) | 0.75 (3.9%) | 0 |
| Motor status MRC (UL/IL) | M1/M3 | M2/M2 | M5/M5 |
| Adjuvant therapy | None | None | None |
| Motor status MRC (UL/IL) at follow-up | M5/M5 | M4/M4 | M5/M5 |
| Recurrency | None | None | None |
| Length of follow-up | 20 | 16 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baro, V.; Sartori, L.; Caliri, S.L.; Furlanis, G.M.; D’Amico, A.; Meneghini, G.; Facchini, S.; Ferreri, F.; Corbetta, M.; Denaro, L.; et al. Navigated Transcranial Magnetic Stimulation Motor Mapping and Diffusion Tensor Imaging Tractography for Diencephalic Tumor in Pediatric Patients. Brain Sci. 2023, 13, 234. https://doi.org/10.3390/brainsci13020234
Baro V, Sartori L, Caliri SL, Furlanis GM, D’Amico A, Meneghini G, Facchini S, Ferreri F, Corbetta M, Denaro L, et al. Navigated Transcranial Magnetic Stimulation Motor Mapping and Diffusion Tensor Imaging Tractography for Diencephalic Tumor in Pediatric Patients. Brain Sciences. 2023; 13(2):234. https://doi.org/10.3390/brainsci13020234
Chicago/Turabian StyleBaro, Valentina, Luca Sartori, Samuel Luciano Caliri, Giulia Melinda Furlanis, Alberto D’Amico, Giulia Meneghini, Silvia Facchini, Florinda Ferreri, Maurizio Corbetta, Luca Denaro, and et al. 2023. "Navigated Transcranial Magnetic Stimulation Motor Mapping and Diffusion Tensor Imaging Tractography for Diencephalic Tumor in Pediatric Patients" Brain Sciences 13, no. 2: 234. https://doi.org/10.3390/brainsci13020234