
Current Advances in Papillary Craniopharyngioma: State-Of-The-Art Therapies and Overview of the Literature
 , , and
, , and
Abstract
:1. Introduction
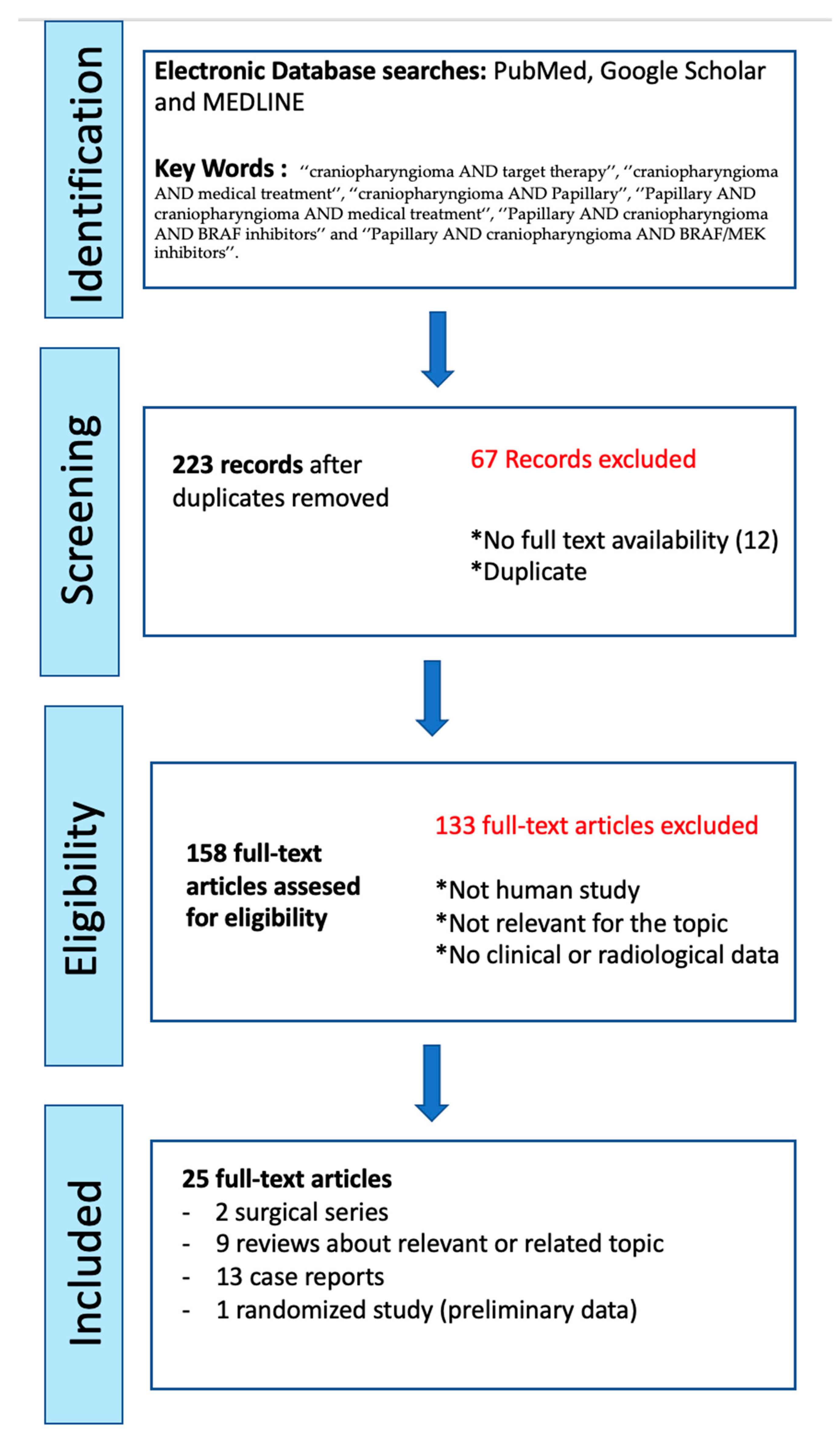
2. Materials and Methods
3. Results
4. Discussion
4.1. Radiological Features: Hypothalamic Invasion and Differential Diagnosis of ACPs/PCPs
4.2. Genetic Findings and Their Implication in Targeted Therapy
4.3. Adjuvant Treatment
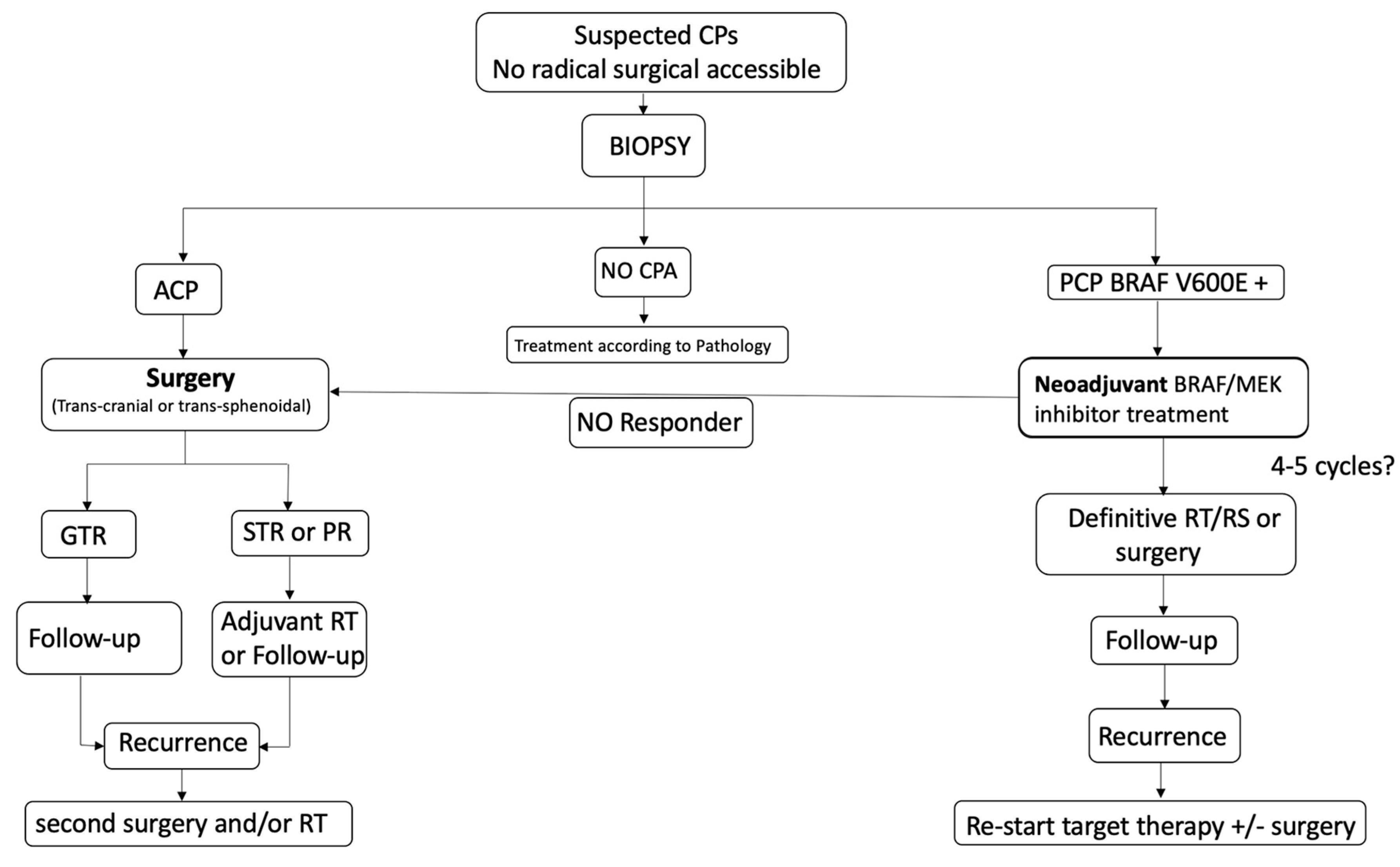
4.4. Neo-Adjuvant Treatment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CPAs | Craniopharyngiomas |
| ACPs | Adamantinomatous craniopharyngiomas |
| PCPs | Papillary craniopharyngiomas |
| PD-1/PD-L1 | programmed cell death protein 1/programmed death-ligand 1 |
References
- Müller, H.L.; Merchant, T.E.; Warmuth-Metz, M.; Martinez-Barbera, J.-P.; Puget, S. Craniopharyngioma. Nat. Rev. Dis. Prim. 2019, 5, 75. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Barbera, J.P.; Andoniadou, C.L. Biological Behaviour of Craniopharyngiomas. Neuroendocrinology 2020, 110, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Asha, M.J.; Oswari, S.; Takami, H.; Velasquez, C.; Almeida, J.P.; Gentili, F. Craniopharyngiomas: Challenges and Controversies. World Neurosurg. 2020, 142, 593–600. [Google Scholar] [CrossRef]
- Apra, C.; Enachescu, C.; Lapras, V.; Raverot, G.; Jouanneau, E. Is Gross Total Resection Reasonable in Adults with Craniopharyngiomas with Hypothalamic Involvement? World Neurosurg. 2019, 129, e803–e811. [Google Scholar] [CrossRef]
- Albano, L.; Losa, M.; Flickinger, J.; Mortini, P.; Minniti, G. Radiotherapy of Parasellar Tumours. Neuroendocrinology 2020, 110, 848–858. [Google Scholar] [CrossRef]
- Pascual, J.M.; Prieto, R.; Carrasco, R. Infundibulo-tuberal or not strictly intraventricular craniopharyngioma: Evidence for a major topographical category. Acta Neurochir. 2011, 153, 2403–2426. [Google Scholar] [CrossRef] [PubMed]
- Pascual, J.M.; Prieto, R.; Carrasco, R.; Barrios, L. Displacement of mammillary bodies by craniopharyngiomas involving the third ventricle: Surgical-MRI correlation and use in topographical diagnosis. J. Neurosurg. 2013, 119, 381–405. [Google Scholar] [CrossRef]
- Prieto, R.; Pascual, J.M.; Hofecker, V.; Winter, E.; Castro-Dufourny, I.; Carrasco, R.; Barrios, L. Craniopharyngioma adherence: A reappraisal of the evidence. Neurosurg. Rev. 2018, 43, 453–472. [Google Scholar] [CrossRef] [PubMed]
- Pascual, J.M.; Prieto, R.; Castro-Dufourny, I.; Mongardi, L.; Rosdolsky, M.; Strauss, S.; Carrasco, R.; Barrios, L. Craniopharyngiomas Primarily Involving the Hypothalamus: A Model of Neurosurgical Lesions to Elucidate the Neurobiological Basis of Psychiatric Disorders. World Neurosurg. 2018, 120, e1245–e1278. [Google Scholar] [CrossRef]
- Müller, H.L. The Diagnosis and Treatment of Craniopharyngioma. Neuroendocrinology 2020, 110, 753–766. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gutierrez, J.C.; D’Andrea, M.R.; Cahill, D.P.; Santagata, S.; Barker, F.G., 2nd; Brastianos, P.K. Diagnosis and management of craniopharyngiomas in the era of genomics and targeted therapy. Neurosurg. Focus 2016, 41, E2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iglesias, P. Targeted therapies in the medical management of craniopharyngioma. Pituitary 2022, 25, 383–392. [Google Scholar] [CrossRef]
- Tritos, N.A. Is there a role for targeted medical therapies in patients with craniopharyngiomas? Futur. Oncol. 2015, 11, 3221–3223. [Google Scholar] [CrossRef] [Green Version]
- Alexandraki, K.; Kaltsas, G.A.; Karavitaki, N.; Grossman, A.B. The Medical Therapy of Craniopharyngiomas: The Way Ahead. J. Clin. Endocrinol. Metab. 2019, 104, 5751–5764. [Google Scholar] [CrossRef]
- Calvanese, F.; Jacquesson, T.; Manet, R.; Vasiljevic, A.; Lasolle, H.; Ducray, F.; Raverot, G.; Jouanneau, E. Neoadjuvant B-RAF and MEK Inhibitor Targeted Therapy for Adult Papillary Craniopharyngiomas: A New Treatment Paradigm. Front. Endocrinol. 2022, 13, 882381. [Google Scholar] [CrossRef]
- Rostami, E.; Casar-Borota, O.; Gudjonsson, O. Molecular Targets in Craniopharyngioma. In Adult Craniopharyngiomas; Jouanneau, E., Raverot, G., Eds.; Springer Nature Switzerland AG: Cham, Switzerland, 2020; pp. 209–218. [Google Scholar]
- Himes, B.T.; Ruff, M.W.; Van Gompel, J.J.; Park, S.S.; Galanis, E.; Kaufmann, T.J.; Uhm, J.H. Recurrent papillary craniopharyngioma with BRAF V600E mutation treated with dabrafenib: Case report. J. Neurosurg. 2018, 27, 1299–1303. [Google Scholar] [CrossRef]
- Juratli, T.A.; Jones, P.S.; Wang, N.; Subramanian, M.; Aylwin, S.J.B.; Odia, Y.; Rostami, E.; Gudjonsson, O.; Shaw, B.L.; Cahill, D.P.; et al. Targeted treatment of papillary craniopharyngiomas harboring BRAF V600E mutations. Cancer 2019, 125, 2910–2914. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, A.; Mrowczynski, O.D.; Greene, A.; Ryan, S.; Chung, C.; Zacharia, B.E.; Glantz, M. Dual BRAF/MEK therapy in BRAF V600E-mutated primary brain tumors: A case series showing dramatic clinical and radiographic responses and a reduction in cutaneous toxicity. J. Neurosurg. 2019, 133, 1704–1709. [Google Scholar] [CrossRef]
- Aylwin, S.J.B.; Bodi, I.; Beaney, R. Pronounced response of papillary craniopharyngioma to treatment with vemurafenib, a BRAF inhibitor. Pituitary 2016, 19, 544–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brastianos, P.K.; Shankar, G.M.; Gill, C.; Taylor-Weiner, A.; Nayyar, N.; Panka, D.J.; Sullivan, R.J.; Frederick, D.T.; Abedalthagafi, M.; Jones, P.S.; et al. Dramatic Response of BRAF V600E Mutant Papillary Craniopharyngioma to Targeted Therapy. J. Natl. Cancer Inst. 2015, 108, djv310. [Google Scholar] [CrossRef]
- Khaddour, K.; Chicoine, M.R.; Huang, J.; Dahiya, S.; Ansstas, G. Successful Use of BRAF/MEK Inhibitors as a Neoadjuvant Approach in the Definitive Treatment of Papillary Craniopharyngioma. J. Natl. Compr. Cancer Netw. 2020, 18, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Roque, A.; Odia, Y.; Wong, E.; Rowbottom, L.; Tsao, M.; Zhang, L.; McDonald, R.; Danjoux, C.; Barnes, E.; Chan, S.; et al. BRAF-V600E mutant papillary craniopharyngioma dramatically responds to combination BRAF and MEK inhibitors. CNS Oncol. 2017, 6, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, A.L.; Guyon, D.; Sejean, K.; Feuvret, L.; Villa, C.; Berzero, G.; Bullet, V.D.; Halimi, E.; Boulin, A.; Baussart, B.; et al. Medical debulking with BRAF/MEK inhibitors in aggressive BRAF-mutant craniopharyngioma. Neuro-Oncol. Adv. 2020, 2, vdaa141. [Google Scholar] [CrossRef] [PubMed]
- Rao, M.; Bhattacharjee, M.; Shepard, S.; Hsu, S. Newly diagnosed papillary craniopharyngioma with BRAF V600E mutation treated with single-agent selective BRAF inhibitor dabrafenib: A case report. Oncotarget 2019, 10, 6038–6042. [Google Scholar] [CrossRef] [Green Version]
- La Corte, E.; Younus, I.; Pivari, F.; Selimi, A.; Ottenhausen, M.; Forbes, J.A.; Pisapia, D.J.; Dobri, G.A.; Anand, V.K.; Schwartz, T.H. BRAF V600E mutant papillary craniopharyngiomas: A single-institutional case series. Pituitary 2018, 21, 571–583. [Google Scholar] [CrossRef]
- Moreno-Torres, B.; Campos-Martín, Y.; Meléndez, B.; Martin, R.M.G.; Vicente, A.; de Lope, R.; Alen, J.F.; Mollejo, M.; Hernández-Laín, A. Craniopharyngiomas: A clinicopathological and molecular study of 52 cases—Experience in the Complejo Hospitalario de Toledo and Hospital Universitario 12 de Octubre (Madrid). Clin. Neuropathol. 2021, 40, 26–35. [Google Scholar] [CrossRef]
- Cuny, T.; Buchfelder, M.; Dufour, H.; Grossman, A.; Gatta-Cherifi, B.; Jouanneau, E.; Raverot, G.; Vasiljevic, A.; Castinetti, F. The Challenging Management of Craniopharyngiomas in Adults: Time for a Reappraisal? Cancers 2022, 14, 3831. [Google Scholar] [CrossRef]
- Cossu, G.; Jouanneau, E.; Cavallo, L.M.; Elbabaa, S.K.; Giammattei, L.; Starnoni, D.; Barges-Coll, J.; Cappabianca, P.; Benes, V.; Baskaya, M.K.; et al. Surgical management of craniopharyngiomas in adult patients: A systematic review and consensus statement on behalf of the EANS skull base section. Acta Neurochir. 2020, 162, 1159–1177. [Google Scholar] [CrossRef] [Green Version]
- Puget, S.; Garnett, M.; Wray, A.; Grill, J.; Habrand, J.-L.; Bodaert, N.; Zerah, M.; Bezerra, M.; Renier, D.; Pierre-Kahn, A.; et al. Pediatric craniopharyngiomas: Classification and treatment according to the degree of hypothalamic involvement. J. Neurosurgery Pediatr. 2007, 106, 3–12. [Google Scholar] [CrossRef]
- Hayashi, Y.; Sasagawa, Y.; Oishi, M.; Misaki, K.; Kozaka, K.; Tachibana, O.; Nakada, M. Radiological and endocrinological evaluations with grading of hypothalamic perifocal edema caused by craniopharyngiomas. Pituitary 2019, 22, 146–155. [Google Scholar] [CrossRef]
- Das, S.; Montemurro, N.; Ashfaq, M.; Ghosh, D.; Sarker, A.C.; Khan, A.H.; Dey, S.; Chaurasia, B. Resolution of Papilledema Following Ventriculoperitoneal Shunt or Endoscopic Third Ventriculostomy for Obstructive Hydrocephalus: A Pilot Study. Medicina 2022, 58, 281. [Google Scholar] [CrossRef] [PubMed]
- Van Gompel, J.J.; Nippoldt, T.B.; Higgins, D.M.; Meyer, F.B. Magnetic resonance imaging-graded hypothalamic compression in surgically treated adult craniopharyngiomas determining postoperative obesity. Neurosurg. Focus 2010, 28, E3. [Google Scholar] [CrossRef] [Green Version]
- Mortini, P.; Gagliardi, F.; Bailo, M.; Spina, A.; Parlangeli, A.; Falini, A.; Losa, M. Magnetic resonance imaging as predictor of functional outcome in craniopharyngiomas. Endocrine 2015, 51, 148–162. [Google Scholar] [CrossRef]
- Higashi, S.; Yamashita, J.; Fujisawa, H.; Yamamoto, Y.; Kadoya, M. “Moustache” Appearance in Craniopharyngiomas: Unique Magnetic Resonance Imaging and Computed Tomographic Findings of Perifocal Edema. Neurosurgery 1990, 27, 993–996. [Google Scholar] [CrossRef] [PubMed]
- Pascual, J.M.; Barrios, L.; Roda, J.M. Intraventricular craniopharyngiomas: Topographical classification and surgical approach selection based on an extensive overview. Acta Neurochir. 2004, 146, 785–802. [Google Scholar] [CrossRef]
- Pascual, J.M.; Prieto, R.; Rosdolsky, M. Craniopharyngiomas primarily affecting the hypothalamus. Handb. Clin. Neurol. 2021, 181, 75–115. [Google Scholar] [CrossRef] [PubMed]
- Müller, H.L.; Gebhardt, U.; Etavard-Gorris, N.; Korenke, E.; Warmuth-Metz, M.; Kolb, R.; Sörensen, N.; Calaminus, G. Prognosis and Sequela in Patients with Childhood Craniopharyngioma—Results of HIT-ENDO and Update on Kraniopharyngeom 2000. Klin. Padiatr. 2004, 216, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Sartoretti-Schefer, S.; Wichmann, W.; Aguzzi, A.; Valavanis, A. MR differentiation of adamantinous and squamous-papillary craniopharyngiomas. AJNR Am. J. Neur. 1997, 18, 77–87. [Google Scholar] [CrossRef]
- Yue, Q.; Yu, Y.; Shi, Z.; Wang, Y.; Zhu, W.; Du, Z.; Yao, Z.; Chen, L.; Mao, Y. Prediction of BRAF mutation status of craniopharyngioma using magnetic resonance imaging features. J. Neurosurg. 2018, 129, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Apps, J.R.; Martinez-Barbera, J.P. Pathophysiology and genetics in craniopharyngioma. In Pituitary Tumors; Honegger, J., Reincke, M., Petersenn, S., Eds.; Academic Press: Cambridge, MA, USA, 2021; pp. 53–66. [Google Scholar]
- Brastianos, P.K.; Taylor-Weiner, A.; Manley, P.E.; Jones, R.T.; Dias-Santagata, D.; Thorner, A.R.; Lawrence, M.S.; Rodriguez, F.J.; A Bernardo, L.; Schubert, L.; et al. Exome sequencing identifies BRAF mutations in papillary craniopharyngiomas. Nat. Genet. 2014, 46, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Gaston-Massuet, C.; Andoniadou, C.L.; Signore, M.; Jayakody, S.A.; Charolidi, N.; Kyeyune, R.; Vernay, B.; Jacques, T.S.; Taketo, M.M.; Le Tissier, P.; et al. Increased Wingless (Wnt) signaling in pituitary progenitor/stem cells gives rise to pituitary tumors in mice and humans. Proc. Natl. Acad. Sci. USA 2011, 108, 11482–11487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisibon, C.; Ouertani, A.; Bertolotto, C.; Ballotti, R.; Cheli, Y. Immune Checkpoints in Cancers: From Signaling to the Clinic. Cancers 2021, 13, 4573. [Google Scholar] [CrossRef] [PubMed]
- Whelan, R.; Prince, E.; Gilani, A.; Hankinson, T. The Inflammatory Milieu of Adamantinomatous Craniopharyngioma and Its Implications for Treatment. J. Clin. Med. 2020, 9, 519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coy, S.; Rashid, R.; Lin, J.-R.; Du, Z.; Donson, A.M.; Hankinson, T.C.; Foreman, N.K.; Manley, P.E.; Kieran, M.W.; A Reardon, D.; et al. Multiplexed immunofluorescence reveals potential PD-1/PD-L1 pathway vulnerabilities in craniopharyngioma. Neuro-Oncol. 2018, 20, 1101–1112. [Google Scholar] [CrossRef] [Green Version]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF gene in human cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef] [Green Version]
- Michaloglou, C.; Vredeveld, L.C.W.; Mooi, W.J.; Peeper, D.S. BRAFE600 in benign and malignant human tumours. Oncogene 2008, 27, 877–895. [Google Scholar] [CrossRef] [Green Version]
- Yuan, J.; Dong, X.; Yap, J.; Hu, J. The MAPK and AMPK signalings: Interplay and implication in targeted cancer therapy. J. Hematol. Oncol. 2020, 13, 113. [Google Scholar] [CrossRef]
- Apps, J.R.; Carreno, G.; Gonzalez-Meljem, J.M.; Haston, S.; Guiho, R.; Cooper, J.E.; Manshaei, S.; Jani, N.; Hölsken, A.; Pettorini, B.; et al. Tumour compartment transcriptomics demonstrates the activation of inflammatory and odontogenic programmes in human adamantinomatous craniopharyngioma and identifies the MAPK/ERK pathway as a novel therapeutic target. Acta Neuropathol. 2018, 135, 757–777. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Bi, W.L.; Larsen, A.G.; Al-Abdulmohsen, S.; Abedalthagafi, M.; Dunn, I.F. Craniopharyngioma: A roadmap for scientific translation. Neurosurg. Focus 2018, 44, E12. [Google Scholar] [CrossRef] [Green Version]
- Kirkland, J.L.; Tchkonia, T. Senolytic drugs: From discovery to translation. J. Intern. Med. 2020, 288, 518–536. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.-S.; Park, J.-I. Wnt signaling in cancer: Therapeutic targeting of Wnt signaling beyond β-catenin and the destruction complex. Exp. Mol. Med. 2020, 52, 183–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.I.; Akgun, E.; Bicer, A.; Ozkan, A.; Bozkurt, S.U.; Kurtkaya, O.; Koc, D.Y.; Pamir, M.N.; Kilic, T. Expression of angiogenic factors in craniopharyngiomas: Implications for tumor recurrence. Neurosurgery 2010, 66, 744–750; [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gump, J.M.; Donson, A.M.; Birks, D.K.; Amani, V.M.; Rao, K.K.; Griesinger, A.M.; Kleinschmidt-DeMasters, B.K.; Johnston, J.M.; Anderson, R.C.E.; Rosenfeld, A.; et al. Identification of targets for rational pharmacological therapy in childhood craniopharyngioma. Acta Neuropathol. Commun. 2015, 3, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heimberger, A.B.; Gatalica, Z.; Kamiya-Matsuoka, C.; Kassab, C.; Zamler, D.; Spetzler, D.; Xiu, J. Genetic and immune profiling for potential therapeutic targets in adult human craniopharyngioma. Clin. Oncol. Res. 2019, 2019, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Brastianos, P.K.; Twohy, E.; Geyer, S.M.; Gerstner, E.R.; Kaufmann, T.J.; Ruff, M.; Bota, D.A.; Reardon, D.A.; Cohen, A.L.; De La Fuente, M.I.; et al. Alliance A071601: Phase II trial of BRAF/MEK inhibition in newly diagnosed papillary craniopharyngiomas. J. Clin. Oncol. 2021, 39, 2000. [Google Scholar] [CrossRef]
- Rostami, E.; Nyström, P.W.; Libard, S.; Wikström, J.; Casar-Borota, O.; Gudjonsson, O. Recurrent papillary craniopharyngioma with BRAFV600E mutation treated with neoadjuvant-targeted therapy. Acta Neurochir. 2017, 159, 2217–2221. [Google Scholar] [CrossRef] [Green Version]
- Long, G.V.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; de Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; Grob, J.-J.; et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: A multicentre, double-blind, phase 3 randomised controlled trial. Lancet 2015, 386, 444–451. [Google Scholar] [CrossRef]
- Lewis, T.S.; Shapiro, P.S.; Ahn, N.G. Signal Transduction through MAP Kinase Cascades. Adv. Cancer Res. 1998, 74, 49–139. [Google Scholar] [CrossRef]
- Fujio, S.; A Juratli, T.; Arita, K.; Hirano, H.; Nagano, Y.; Takajo, T.; Yoshimoto, K.; Bihun, I.V.; Kaplan, A.B.; Nayyar, N.; et al. A Clinical Rule for Preoperative Prediction of BRAF Mutation Status in Craniopharyngiomas. Neurosurgery 2018, 85, 204–210. [Google Scholar] [CrossRef] [Green Version]
- Iannalfi, A.; Fragkandrea, I.; Brock, J.; Saran, F. Radiotherapy in Craniopharyngiomas. Clin. Oncol. 2013, 25, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Frio, F.; Solari, D.; Cavallo, L.M.; Cappabianca, P.; Raverot, G.; Jouanneau, E. Ommaya Reservoir System for the Treatment of Cystic Craniopharyngiomas: Surgical Results in a Series of 11 Adult Patients and Review of the Literature. World Neurosurg. 2019, 132, e869–e877. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Radiological Findings | Imaging Method | High-Risk Factor of Hypothalamic Involvement and Grading |
|---|---|---|
| Topographic location according to Pascual et al. classification [37,38] | Sagittal T1 and T2 WI | Tubero-infundibular and secondary intraventricular |
| Tumor morphology [37,38] | Sagittal and coronal T1WI-Gd | Elliptical, multilobulated tumors |
| PS morphology [37,38] | Sagittal T1 and T2 WI | Not visible or amputated/infiltrated |
| Relationship TVF/tumor [37,38] | Coronal T2WI | Middle third > upper third > bottom third |
| Hypothalamic oedema | Axial T2WI/FLAIR | Moustache appearance [36] |
| Hypothalamic oedema | Coronal T2WI/FLAIR | Grade B and C according to Hayashi et al. [32] T2WI hypothalamic changes according to Van Gompel et al.’s grading [21] |
| Irregular contrast enhancement according to Van Gompel et al.’s grading [34] | Coronal T1WI-Gd | Grade 1: Irregular contrast enhancement or hypothalamic changes on T2WI Grade 2: Irregular contrast enhancement associated with hypothalamic changes on T2WI |
| Hypothalamic involvement according to Saint-Rose and Puget’s grading [31] | Sagittal MRI | Grade 1: Hypothalamic compression Grade 2: Infiltration or unidentifiable hypothalamus |
| Hypothalamic and MB involvement according to Muller’s grading [39] | Sagittal MRI | Grade 1: No hypothalamic involvement Grade 2: Anterior hypothalamic involvement (i.e., no MB involvement) Grade 3: Anterior and posterior hypothalamic involvement including MB |
| CP adherence to hypothalamus according to Prieto et al.’s classification [8] MRI variables predicting the risk of adherence: 1. Location of Hypothalamus/TVF * 2. PS 3. Morphology | Coronal and sagittal T2WI | Level I or mild risk: Sellar/suprasellar (leptomeningeal layer) Upper third hypothalamic level, no visible PS, round or pear-like morphology Level II or moderate risk: Intraventricular (fibrovascular stem with ependyma) Lower third hypothalamic level, visible PS, round shape Level III or serious risk: Suprasellar/pseudo-ventricular (blown-like shape adherences) Upper third hypothalamic level; No visible PS; elliptical, dumbbell and multilobulated morphology Level IV or severe risk: Tubero-infundibular or secondary intraventricular (ring-like shape or wrapping paper-like adherences) Middle third hypothalamic level, No visible PS, elliptical morphology Level V or critical risk: Replacement of TVF Middle third hypothalamic level, no visible PS, elliptical and multilobulated morphology |
| Molecular or Genetic Alterations | CPs Type (% of Case) | Tumoral Compartment or Specific Tumoral Cell | Molecular or Biological Disarrangement | Possible Molecular Treatment |
|---|---|---|---|---|
| BRAFV600E | PCP (95–100%) | SOX2+/Height proliferating progenitor tumor cell | Hyperactivation MAPKK pathway | BRAF/MEKi [16] |
| CTNNB1 (Exon 3 Beta catenin gene) | ACP (70–100%) | Single or cell clusters (SOX2+) in tumor mass or at the base of epithelial protrusion | Hyperactivation WNT/beta catenin pathway leading to SASP | Senolytics [53] Wnt/β-catenin signaling inhibitors (several on-going trials) [54] |
| CTNNB1 (Exon 3 Beta catenin gene) | ACP (70–100%) | Forefront or leading edge of the tumor | Hyperactivation MAPK pathway (possible crosstalk with WNT pathway) | Trametinib or combined BRAF/MEKi [29] |
| CTNNB1 (Exon 3 Beta catenin gene) | ACP (70–100%) | Single or cell clusters (SOX2+) in tumor mass or at the base of epithelial protrusion (ACP recurrence) | SHH secretion and hyperactivation of SHH pathway IL-1 and IL-6 secretion Secretion of VEGF, FGF2, TGF beta and increased expression of PDGFR-alpha Hyperactivation of EGF/EGFR pathway (AREG, EGFR, and ERBB-3) | SHH pathway inhibitors (vismodegib) [1] IL-1R inhibitor (anakinra) Antiangiogenic drugs [55]: * bevacizumab * Selctive-PDGFR-alfa blockers (ripretinib) TKI: cetuximab, erlotinib, and lapatinib [15] |
| CTNNB1 (exon 3 Beta catenin gene) | ACP (70–100%) | Single or cell clusters (SOX2+) in tumor mass or at the base of epithelial protrusion | MMP9 and MMP12 overexpression [56] LCK, EPHA2, SRC overexpression [56] | MMP9/12 inhibitor AZD1236 dasatinib |
| PD1/PDL-1 | ACP (100%) PCP (100%) | Cyst-lining in ACP, and to basal tumor cells in PCP | Immunomodulatory action | ICI [49] |
| PIK3CA and the TSC2 mutations [57] | ACP (-) PCP (-) | _ | Hyperactivation of mTor pathway | Everolimus (mTor inhibitors) Copanlisib (pan-PIK3 inhibitor) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jannelli, G.; Calvanese, F.; Paun, L.; Raverot, G.; Jouanneau, E. Current Advances in Papillary Craniopharyngioma: State-Of-The-Art Therapies and Overview of the Literature. Brain Sci. 2023, 13, 515. https://doi.org/10.3390/brainsci13030515
Jannelli G, Calvanese F, Paun L, Raverot G, Jouanneau E. Current Advances in Papillary Craniopharyngioma: State-Of-The-Art Therapies and Overview of the Literature. Brain Sciences. 2023; 13(3):515. https://doi.org/10.3390/brainsci13030515
Chicago/Turabian StyleJannelli, Gianpaolo, Francesco Calvanese, Luca Paun, Gerald Raverot, and Emmanuel Jouanneau. 2023. "Current Advances in Papillary Craniopharyngioma: State-Of-The-Art Therapies and Overview of the Literature" Brain Sciences 13, no. 3: 515. https://doi.org/10.3390/brainsci13030515