
Effect of Chronic Ankle Instability on the Biomechanical Organization of Gait Initiation: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Selection Process
2.4. Data Collection Process and Data Extraction
2.5. Risk of Bias and Methodological Quality Assessment
3. Results
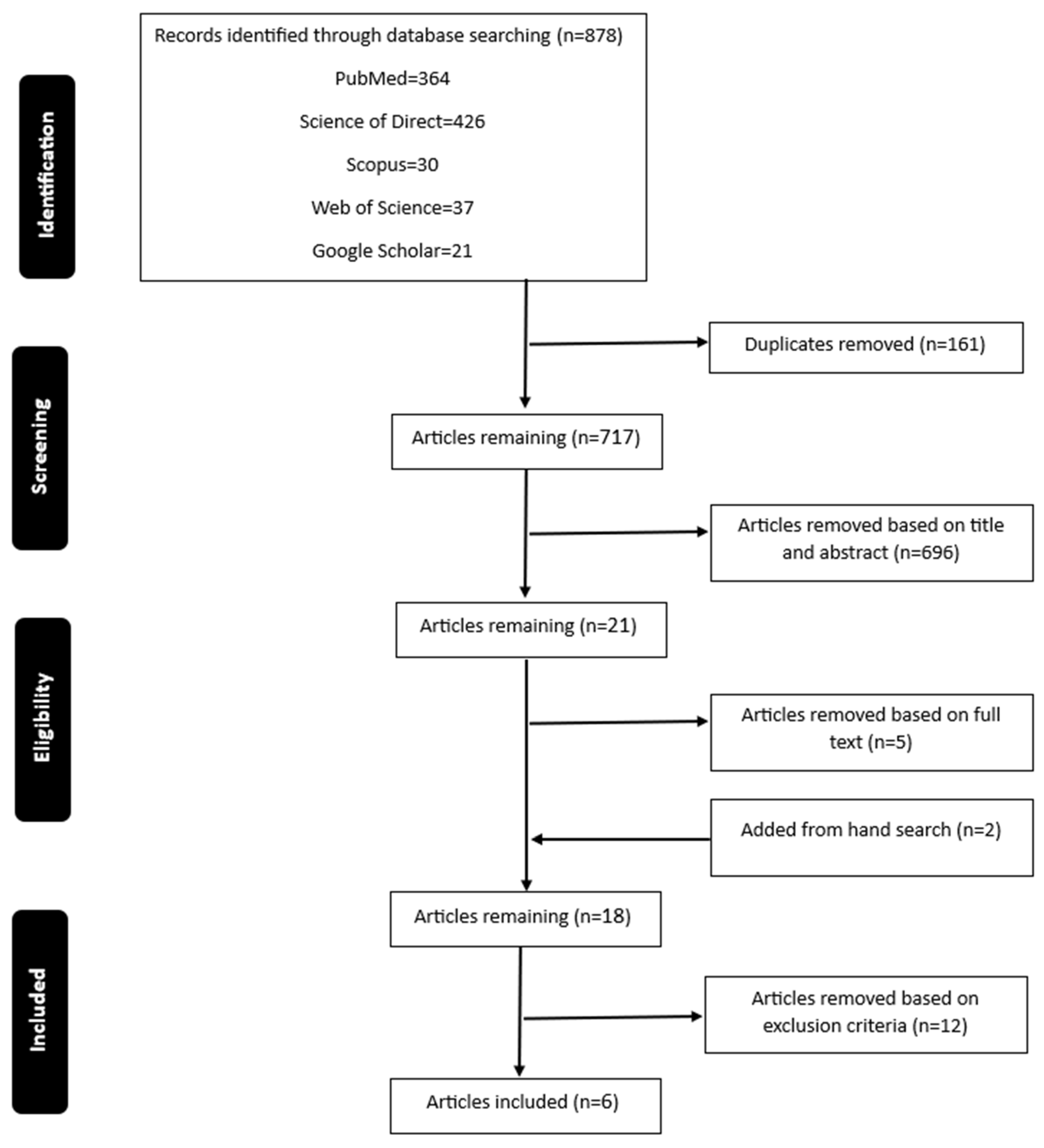
3.1. Study Selection and Characteristics
3.2. Quality Assessment
3.3. Results of Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swenson, D.M.; Collins, C.L.; Fields, S.K.; Comstock, R.D. Epidemiology of US High School Sports-Related Ligamentous Ankle Injuries, 2005/06–2010/11. Clin. J. Sport Med. 2013, 23, 190–196. [Google Scholar] [CrossRef]
- Waterman, B.R.; Owens, B.D.; Davey, S.; Zacchilli, M.A.; Belmont, P.J., Jr. The Epidemiology of Ankle Sprains in the United States. JBJS 2010, 92, 2279–2284. [Google Scholar] [CrossRef]
- Mohamadi, S.; Ebrahimi, I.; Salavati, M.; Dadgoo, M.; Jafarpisheh, A.S.; Rezaeian, Z.S. Attentional Demands of Postural Control in Chronic Ankle Instability, Copers and Healthy Controls: A Controlled Cross-sectional Study. Gait Posture 2020, 79, 183–188. [Google Scholar] [CrossRef]
- Son, S.J.; Kim, H.; Seeley, M.K.; Hopkins, J.T. Movement Strategies among Groups of Chronic Ankle Instability, Coper, and Control. Med. Sci. Sports Exerc. 2017, 49, 1649–1661. [Google Scholar] [CrossRef]
- Suttmiller, A.M.B.; Cavallario, J.M.; Baez, S.E.; Martinez, J.C.; McCann, R.S. Perceived Instability, Pain, and Psychological Factors for Prediction of Function and Disability in Individuals with Chronic Ankle Instability. J. Athl. Train. 2022, 57, 1048–1054. [Google Scholar] [CrossRef]
- Watabe, T.; Takabayashi, T.; Tokunaga, Y.; Yoshida, T.; Kubo, M. Copers adopt an altered movement pattern compared to individuals with chronic ankle instability and control groups in unexpected single-leg landing and cutting task. J. Electromyogr. Kinesiol. 2021, 57, 102529. [Google Scholar] [CrossRef]
- Koldenhoven, R.M.; Feger, M.A.; Fraser, J.J.; Hertel, J. Variability in center of pressure position and muscle activation during walking with chronic ankle instability. J. Electromyogr. Kinesiol. 2018, 38, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Hertel, J.; Corbett, R.O. An Updated Model of Chronic Ankle Instability. J. Athl. Train. 2019, 54, 572–588. [Google Scholar] [CrossRef]
- Herb, C.C.; Hertel, J. Current concepts on the pathophysiology and management of recurrent ankle sprains and chronic ankle instability. Cur. Phys. Med. Rehabil. Rep. 2014, 2, 25–34. [Google Scholar] [CrossRef]
- Thompson, C.; Schabrun, S.; Romero, R.; Bialocerkowski, A.; Marshall, P. Factors contributing to chronic ankle instability: A protocol for a systematic review of systematic reviews. Syst. Rev. 2016, 5, 94. [Google Scholar] [CrossRef]
- Hou, Z.-C.; Miao, X.; Ao, Y.-F.; Hu, Y.-L.; Jiao, C.; Guo, Q.-W.; Xie, X.; Zhao, F.; Pi, Y.-B.; Li, N.; et al. Characteristics and predictors of muscle strength deficit in mechanical ankle instability. BMC Musculoskelet. Disord. 2020, 21, 730. [Google Scholar] [CrossRef] [PubMed]
- Wenning, M.; Gehring, D.; Mauch, M.; Schmal, H.; Ritzmann, R.; Paul, J. Functional deficits in chronic mechanical ankle instability. J. Orthop. Surg. Res. 2020, 15, 304. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, G.M.; Kaminski, T.W.; Douex, A.T. Neuromuscular control and ankle instability. PM R 2009, 1, 359–365. [Google Scholar] [CrossRef]
- Kipp, K.; Palmieri-Smith, R.M. Differences in kinematic control of ankle joint motions in people with chronic ankle instability. Clin. Biomech. 2013, 28, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Moisan, G.; Mainville, C.; Descarreaux, M.; Cantin, V. Lower limb biomechanics in individuals with chronic ankle instability during gait: A case-control study. J. Foot Ankle Res. 2021, 14, 36. [Google Scholar] [CrossRef]
- Balasukumaran, T.; Gottlieb, U.; Springer, S. Muscle activation patterns during backward walking in people with chronic ankle instability. BMC Musculoskelet. Disord. 2020, 21, 489. [Google Scholar] [CrossRef]
- Balasukumaran, T.; Gottlieb, U.; Springer, S. Spatiotemporal gait characteristics and ankle kinematics of backward walking in people with chronic ankle instability. Sci. Rep. 2020, 10, 11515. [Google Scholar] [CrossRef]
- Kim, H.; Palmieri-Smith, R.; Kipp, K. Muscle force contributions to ankle joint contact forces during an unanticipated cutting task in people with chronic ankle instability. J. Biomech. 2021, 124, 110566. [Google Scholar] [CrossRef]
- Doherty, C.; Delahunt, E.; Caulfield, B.; Hertel, J.; Ryan, J.; Bleakley, C. The Incidence and Prevalence of Ankle Sprain Injury: A Systematic Review and Meta-Analysis of Prospective Epidemiological Studies. Sports Med. 2014, 44, 123–140. [Google Scholar] [CrossRef]
- Delval, A.; Bayot, M.; Lapoulvereyrie, R.; Defebvre, L.; Vermersch, P.; Tard, C. Role of the peripheral nervous system for an appropriate postural preparation during gait initiation in patients with a chronic inflammatory demyelinating polyneuropathy: A pilot study. Gait Posture 2021, 90, 29–35. [Google Scholar] [CrossRef]
- Fraser, J.J.; Hart, J.M.; Saliba, S.F.; Park, J.S.; Tumperi, M.; Hertel, J. Multisegmented ankle-foot kinematics during gait initiation in ankle sprains and chronic ankle instability. Clin. Biomech. 2019, 68, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimabadi, Z.; Naimi, S.S.; Rahimi, A.; Sadeghi, H.; Hosseini, S.M.; Baghban, A.A.; Arsalan, S.A. The alteration of neuromuscular control strategies during gait initiation in individuals with chronic ankle instability. Iran. Red Crescent Med. J. 2017, 19, e44534. [Google Scholar] [CrossRef]
- Yiou, E.; Caderby, T.; Delafontaine, A.; Fourcade, P.; Honeine, J.L. Balance control during gait initiation: State-of-the-art and research perspectives. World J. Orthop. 2017, 8, 815–828. [Google Scholar] [CrossRef]
- Lu, C.; Amundsen Huffmaster, S.L.; Harvey, J.C.; MacKinnon, C.D. Anticipatory postural adjustment patterns during gait initiation across the adult lifespan. Gait Posture 2017, 57, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Yiou, E.; Caderby, T.; Hussein, T. Adaptability of anticipatory postural adjustments associated with voluntary movement. World J. Orthop. 2012, 3, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimabadi, Z.; Naimi, S.S.; Rahimi, A.; Sadeghi, H.; Hosseini, S.M.; Baghban, A.A.; Arslan, S.A. Investigating the anticipatory postural adjustment phase of gait initiation in different directions in chronic ankle instability patients. J. Bodyw. Mo. Ther. 2018, 22, 40–45. [Google Scholar] [CrossRef]
- Caderby, T.; Yiou, E.; Peyrot, N.; Begon, M.; Dalleau, G. Influence of gait speed on the control of mediolateral dynamic stability during gait initiation. J. Biomech. 2014, 47, 417–423. [Google Scholar] [CrossRef] [PubMed]
- McIlroy, W.E.; Maki, B.E. The control of lateral stability during rapid stepping reactions evoked by antero-posterior perturbation: Does anticipatory control play a role? Gait Posture 1999, 9, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimabadi, Z.; Naimi, S.S.; Rahimi, A.; Yousefi, M.; Wikstrom, E.A. Postural phase duration during self-generated and triggered gait initiation in patients with chronic ankle instability. Sci. Sports 2023, 38, 182–188. [Google Scholar] [CrossRef]
- Hass, C.J.; Bishop, M.D.; Doidge, D.; Wikstrom, E.A. Chronic ankle instability alters central organization of movement. Am. J. Sports Med. 2010, 38, 829–834. [Google Scholar] [CrossRef]
- Honeine, J.-L.; Schieppati, M.; Crisafulli, O.; Do, M.-C. The Neuro-Mechanical Processes That Underlie Goal-Directed Medio-Lateral APA during Gait Initiation. Front. Hum. Neurosci. 2016, 10, 445. [Google Scholar] [CrossRef] [PubMed]
- Yiou, E.; Artico, R.; Teyssedre, C.A.; Labaune, O.; Fourcade, P. Anticipatory Postural Control of Stability during Gait Initiation Over Obstacles of Different Height and Distance Made Under Reaction-Time and Self-Initiated Instructions. Front. Hum. Neurosci. 2016, 10, 449. [Google Scholar] [CrossRef] [PubMed]
- Crenna, P.; Frigo, C. A motor programme for the initiation of forward-oriented movements in humans. J. Physiol. 1991, 437, 635–653. [Google Scholar] [CrossRef]
- Feger, M.A.; Donovan, L.; Hart, J.M.; Hertel, J. Lower extremity muscle activation in patients with or without chronic ankle instability during walking. J. Athl. Train. 2015, 50, 350–357. [Google Scholar] [CrossRef]
- Kim, H.; Palmieri-Smith, R.; Kipp, K. Time-frequency analysis of muscle activation patterns in people with chronic ankle instability during Landing and cutting tasks. Gait Posture 2020, 82, 203–208. [Google Scholar] [CrossRef]
- Kim, H.; Palmieri-Smith, R.; Kipp, K. Muscle Synergies in People with Chronic Ankle Instability during Anticipated and Unanticipated Cutting Tasks. J. Athl. Train. 2023, 58, 58,143–152. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Uygur, M.; Kaminski Thomas, W. Effect of Ankle Instability on Gait Parameters: A Systematic Review. Athl. Train. Sports Health Care 2012, 4, 275–281. [Google Scholar] [CrossRef]
- Moisan, G.; Descarreaux, M.; Cantin, V. Effects of chronic ankle instability on kinetics, kinematics and muscle activity during walking and running: A systematic review. Gait Posture 2017, 52, 381–399. [Google Scholar] [CrossRef] [PubMed]
- Labanca, L.; Mosca, M.; Ghislieri, M.; Agostini, V.; Knaflitz, M.; Benedetti, M.G. Muscle activations during functional tasks in individuals with chronic ankle instability: A systematic review of electromyographical studies. Gait Posture 2021, 90, 340–373. [Google Scholar] [CrossRef]
- Lin, C.I.; Khajooei, M.; Engel, T.; Nair, A.; Heikkila, M.; Kaplick, H.; Mayer, F. The effect of chronic ankle instability on muscle activations in lower extremities. PLoS ONE 2021, 16, e0247581. [Google Scholar] [CrossRef]
- Yousefi, M.; Sadeghi, H.; Ilbiegi, S.; Ebrahimabadi, Z.; Kakavand, M.; Wikstrom, E.A. Center of pressure excursion and muscle activation during gait initiation in individuals with and without chronic ankle instability. J. Biomech. 2020, 108, 109904. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ Clin. Res. Ed. 2021, 372, n71. [Google Scholar]
- Chiou, S.Y.; Hurry, M.; Reed, T.; Quek, J.X.; Strutton, P.H. Cortical contributions to anticipatory postural adjustments in the trunk. J. Physiol. 2018, 596, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.V.; Lou, J.S.; Kraakevik, J.A.; Horak, F.B. The supplementary motor area contributes to the timing of the anticipatory postural adjustment during step initiation in participants with and without Parkinson’s disease. Neuroscience 2009, 164, 877–885. [Google Scholar] [CrossRef]
- Brenière, Y.; Cuong Do, M.; Bouisset, S. Are dynamic phenomena prior to stepping essential to walking? J. Mot. Behav. 1987, 19, 62–76. [Google Scholar] [CrossRef]
- Lepers, R.; Brenière, Y. The role of anticipatory postural adjustments and gravity in gait initiation. Exp. Brain. Res. 1995, 107, 118–124. [Google Scholar] [CrossRef]
- Elble, R.J.; Cousins, R.; Leffler, K.; Hughes, L. Gait initiation by patients with lower-half parkinsonism. Brain 1996, 119 Pt 5, 1705–1716. [Google Scholar] [CrossRef]
- Kirker, S.G.B.; Simpson, D.S.; Jenner, J.R.; Wing, A.M. Stepping before standing: Hip muscle function in stepping and standing balance after stroke. J. Neurol. Neurosurg. Psychiatry 2000, 68, 458. [Google Scholar] [CrossRef]
- King, D.L.; Zatsiorsky, V.M. Periods of extreme ankle displacement during one-legged standing. Gait Posture 2002, 15, 172–179. [Google Scholar] [CrossRef]
- Hof, A.L.; van Bockel, R.M.; Schoppen, T.; Postema, K. Control of lateral balance in walking. Experimental findings in normal subjects and above-knee amputees. Gait Posture 2007, 25, 250–258. [Google Scholar] [CrossRef]
- Arnold, B.L.; Linens, S.W.; de la Motte, S.J.; Ross, S.E. Concentric evertor strength differences and functional ankle instability: A meta-analysis. J. Athl. Train. 2009, 44, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Wikstrom, E.A.; Anderson, R.B. Alterations in gait initiation are present in those with posttraumatic ankle osteoarthritis: A pilot study. J. Appl. Biomech. 2013, 29, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Lyon, I.N.; Day, B.L. Control of frontal plane body motion in human stepping. Exp. Brain Res. 1997, 115, 345–356. [Google Scholar] [CrossRef]
- Rogers, M.W.; Hedman, L.D.; Johnson, M.E.; Cain, T.D.; Hanke, T.A. Lateral stability during forward-induced stepping for dynamic balance recovery in young and older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Delafontaine, A.; Vialleron, T.; Diakhaté, D.G.; Fourcade, P.; Yiou, E. Effects of experimentally induced cervical spine mobility alteration on the postural organisation of gait initiation. Sci. Rep. 2022, 12, 6055. [Google Scholar] [CrossRef] [PubMed]
- Aruin, A.S. Enhancing Anticipatory Postural Adjustments: A Novel Approach to Balance Rehabilitation. J. Nov. Physiother. 2016, 6, e144. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Yamanaka, M.; Kasahara, S.; Fukushima, J. Relationship between improvements in motor performance and changes in anticipatory postural adjustments during whole-body reaching training. Hum. Mov. Sci. 2014, 37, 69–86. [Google Scholar] [CrossRef]
- Yiou, E.; Fourcade, P.; Artico, R.; Caderby, T. Influence of temporal pressure constraint on the biomechanical organization of gait initiation made with or without an obstacle to clear. Exp. Brain Res. 2016, 234, 1363–1375. [Google Scholar] [CrossRef]


{kind=link}
| Study | Study Design | Participants | Protocol | Outcome Measures | Key Findings |
|---|---|---|---|---|---|
| Ebrahimabadi et al., 2017 [22] | Cross-sectional study | 22 CAI (F:22, 22.4 ± 1.5 yrs) 22 healthy (F:22, 22.7 ± 1.8 yrs) | Triggered GI at maximum speed with both the injured and non-injured limb. | Displacement and velocity of the COP during APA and execution phases. | Peak ML COP displacement toward the swing leg in the APA phase of GI was reduced in CAI. Forward COP velocity was increased in CAI in the execution phase of GI. |
| Ebrahimabadi et al., 2018 [26] | Pilot cross-sectional study | 20 CAI (21.4 ± 1.3 yrs) 20 healthy (21.7 ± 1.5 yrs) | Triggered GI at maximum speed in 3 directions (forward, 30° medial, and 30° lateral) with both the injured and non-injured limb. | COP and COM kinematics. | AP COM velocity at the end of APA did not differ between CAI and controls. Peak ML COP shift and vertical COM velocity during APA were decreased in CAI. |
| Ebrahimabadi et al., 2022 [29] | Cross-sectional study | 25 CAI (F:20/M:5, 22.01 ± 1.08 yrs) 25 healthy (F:21/M:4, 22.90 ± 1.61 yrs) | Triggered and self-generated GI at maximum speed in 3 directions (forward, 30° medial, and 30° lateral) with the non-injured limb. | Reaction time and APA phase durations, COP displacement, and COM velocity during the APA phase. | Longer reaction time and shorter APA duration (7%) in CAI. No difference in COP displacement and COM velocity between CAI and controls. |
| Fraser et al., 2019 [21] | Cross-sectional study | 22 Control (F:13/M:9, 19.6 ± 0.9 yrs) 17 LAS (F:9/M:8, 21.0 ± 2.3 yrs) 21 Coper (F:13/M:8, 20.8 ± 2.9 yrs) 20 CAI (F:15/M:5, 19.8 ± 1.3 yrs) | GI at a self-selected speed with the injured limb. | Three-dimensional kinematics of the hallux, forefoot, midfoot, and rearfoot. | Rearfoot inversion during the end of step execution phase increased by 5.3° in CAI. |
| Hass et al., 2010 [30] | Cross-sectional study | 20 CAI (F:15/M:5, 20.5 ± 61.0 yrs) 20 Control (F:16, M:4, 20.85 ± 61.6 yrs) | Triggered GI at a self-selected speed with both the injured and non-injured limb. | Displacement and velocity of the COP during the APA and execution phases. | Resultant COP displacement in the APA phase and ML COP displacement in the execution phase were reduced in CAI when gait was initiated with the non-injured limb. |
| Yousefi et al., 2020 [41] | Cross-sectional study | 17 CAI (M:17, 24.31 ± 0.81 yrs) 17 Control (M:17, 23.40 ± 1.70 yrs) | Triggered gait initiation at a self-selected speed with the injured limb. | Reaction time and APA duration, COP excursion, muscle activation. | Longer reaction time phase and shorter APA duration in CAI. No difference in AP and ML normalized peak COP excursions in the APA phase. Earlier soleus activation in the injured limb in CAI. |
| Quality items | Ebrahimabadi et al., 2022 [29] | Yousefi et al., 2020 [41] | Fraser et al., 2019 [21] | Ebrahimabadi et al., 2018 [26] | Ebrahimabadi et al., 2017 [22] | Hass et al., 2010 [30] | |
|---|---|---|---|---|---|---|---|
| Reporting | Q1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Q2 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Q3 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Q4 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Q5 | 2 | 2 | 2 | 2 | 2 | 2 | |
| Q6 | 0 | 1 | 1 | 1 | 0 | 1 | |
| Q7 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Q8 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Q9 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Q10 | 1 | 1 | 1 | 1 | 1 | 1 | |
| External Validity | Q11 | 1 | 0 | 0 | 0 | 1 | 0 |
| Q12 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Q13 | 1 | 0 | 1 | 0 | 1 | 0 | |
| Internal Validity–Bias | Q14 | 0 | 0 | 0 | 0 | 0 | 0 |
| Q15 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Q16 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Q17 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Q18 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Q19 | 0 | 0 | 1 | 0 | 0 | 0 | |
| Q20 | 0 | 0 | 1 | 0 | 0 | 0 | |
| Internal Validity–Confounding | Q21 | 1 | 0 | 1 | 0 | 0 | 1 |
| Q22 | 0 | 0 | 0 | 0 | 1 | 0 | |
| Q23 | 0 | 0 | 0 | 0 | 1 | 0 | |
| Q24 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Q25 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Q26 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Power | Q27 | 0 | 0 | 0 | 1 | 1 | 0 |
| Total | 11 | 9 | 13 | 10 | 13 | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yousefi, M.; Zivari, S.; Yiou, E.; Caderby, T. Effect of Chronic Ankle Instability on the Biomechanical Organization of Gait Initiation: A Systematic Review. Brain Sci. 2023, 13, 1596. https://doi.org/10.3390/brainsci13111596
Yousefi M, Zivari S, Yiou E, Caderby T. Effect of Chronic Ankle Instability on the Biomechanical Organization of Gait Initiation: A Systematic Review. Brain Sciences. 2023; 13(11):1596. https://doi.org/10.3390/brainsci13111596
Chicago/Turabian StyleYousefi, Mohammad, Shaghayegh Zivari, Eric Yiou, and Teddy Caderby. 2023. "Effect of Chronic Ankle Instability on the Biomechanical Organization of Gait Initiation: A Systematic Review" Brain Sciences 13, no. 11: 1596. https://doi.org/10.3390/brainsci13111596