
Effect of Laterally Moving Tactile Stimuli to Sole on Anticipatory Postural Adjustment of Gait Initiation in Healthy Males
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
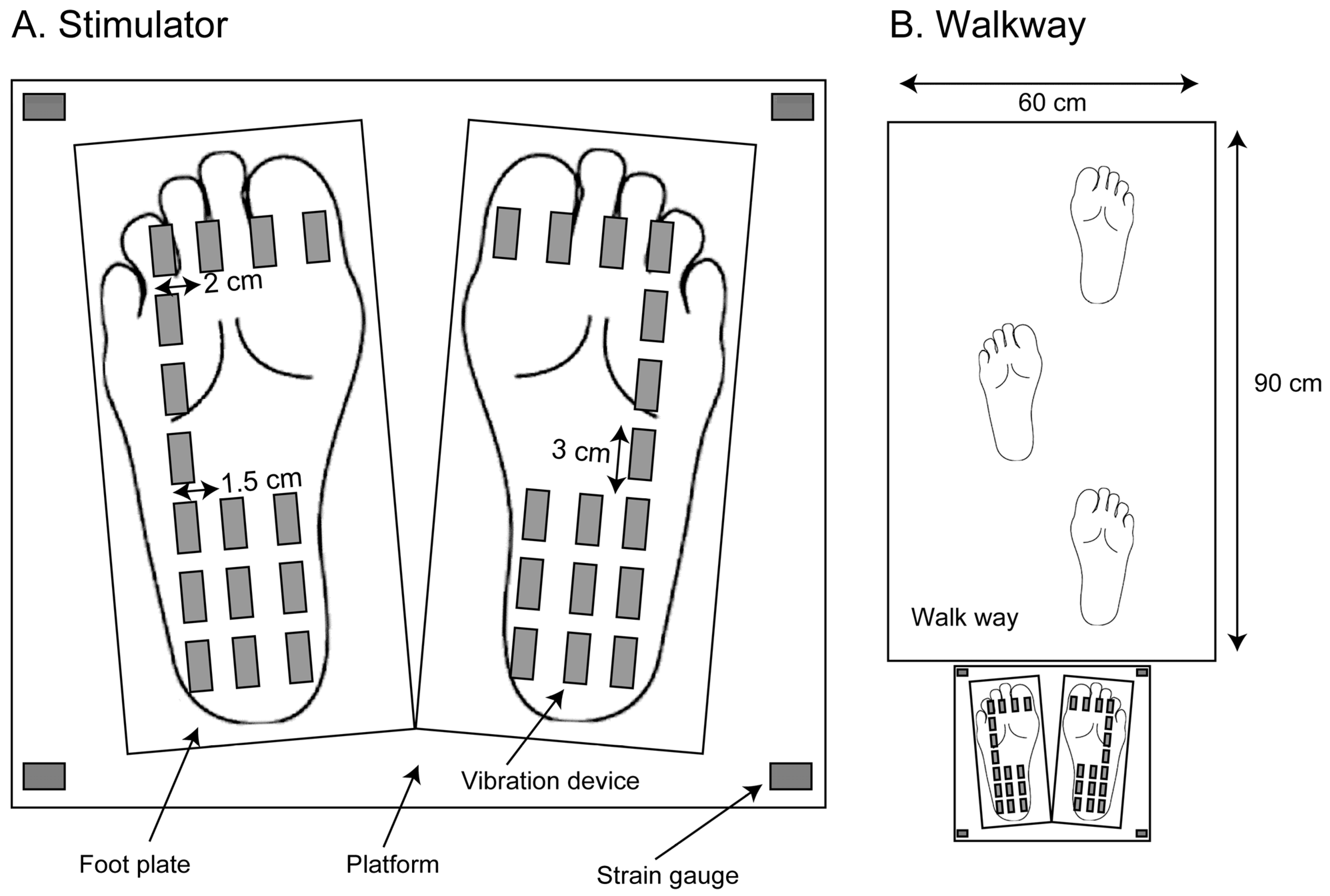
2.3. Apparatus
2.4. Procedure
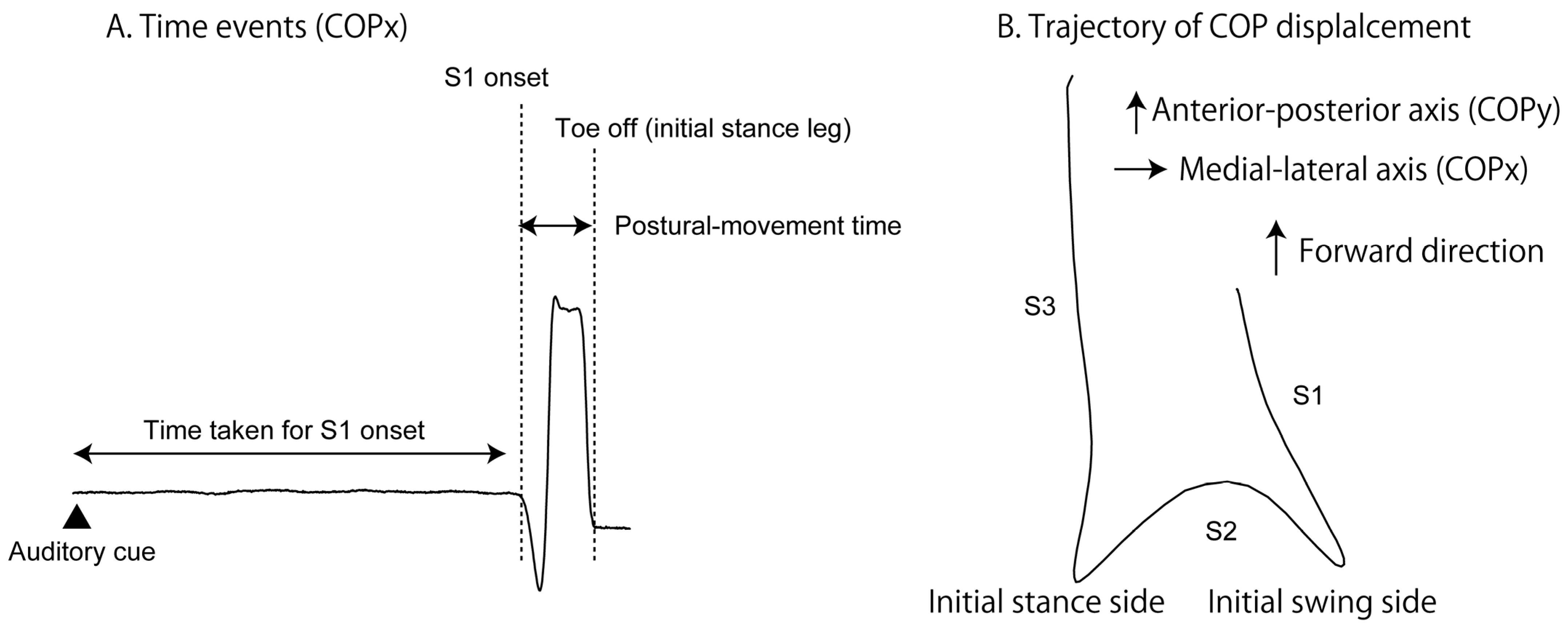
2.5. Variables
2.6. Statistical Procedure
3. Results
3.1. COP before S1 Onset
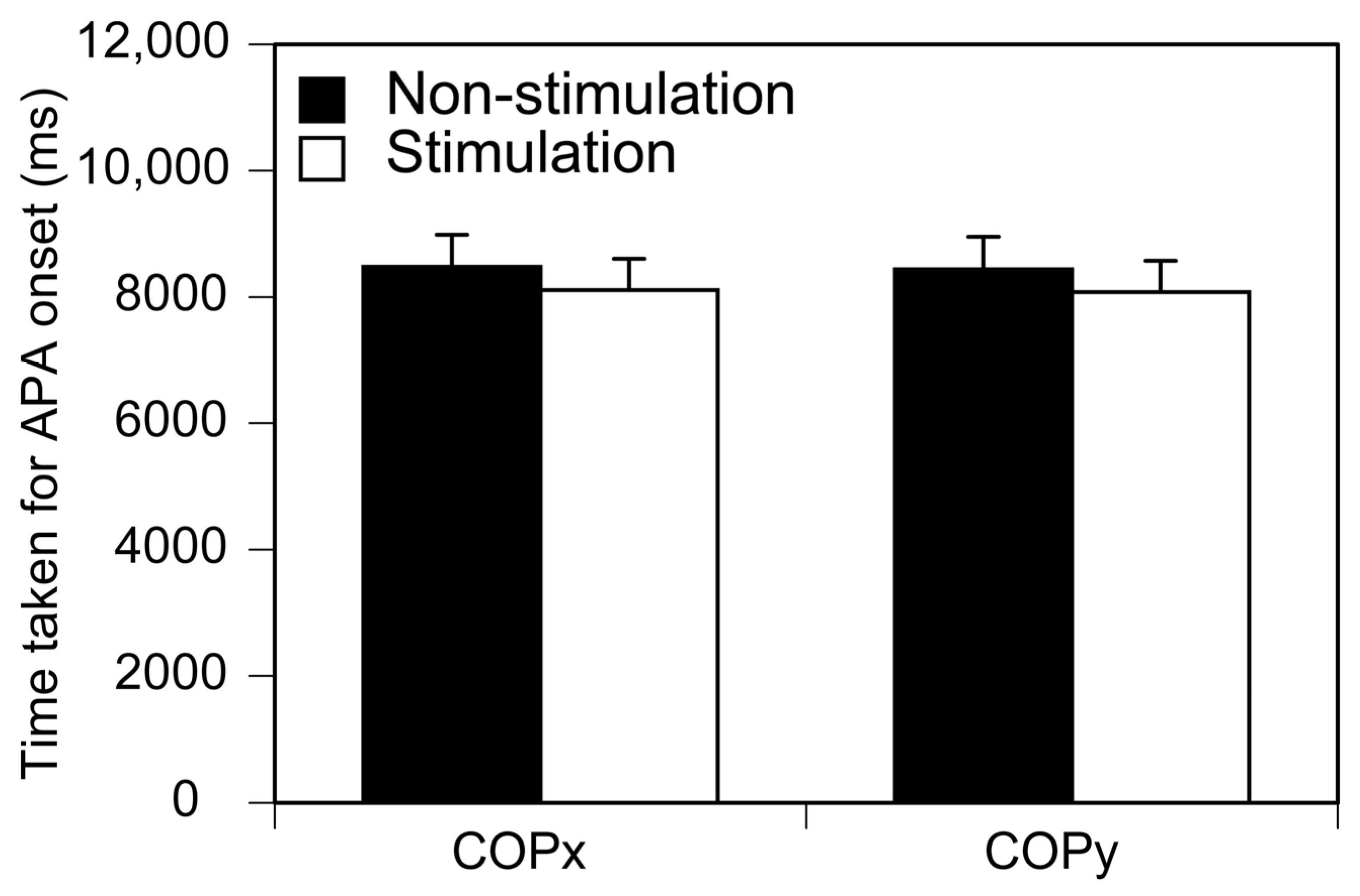
3.2. S1 Onset
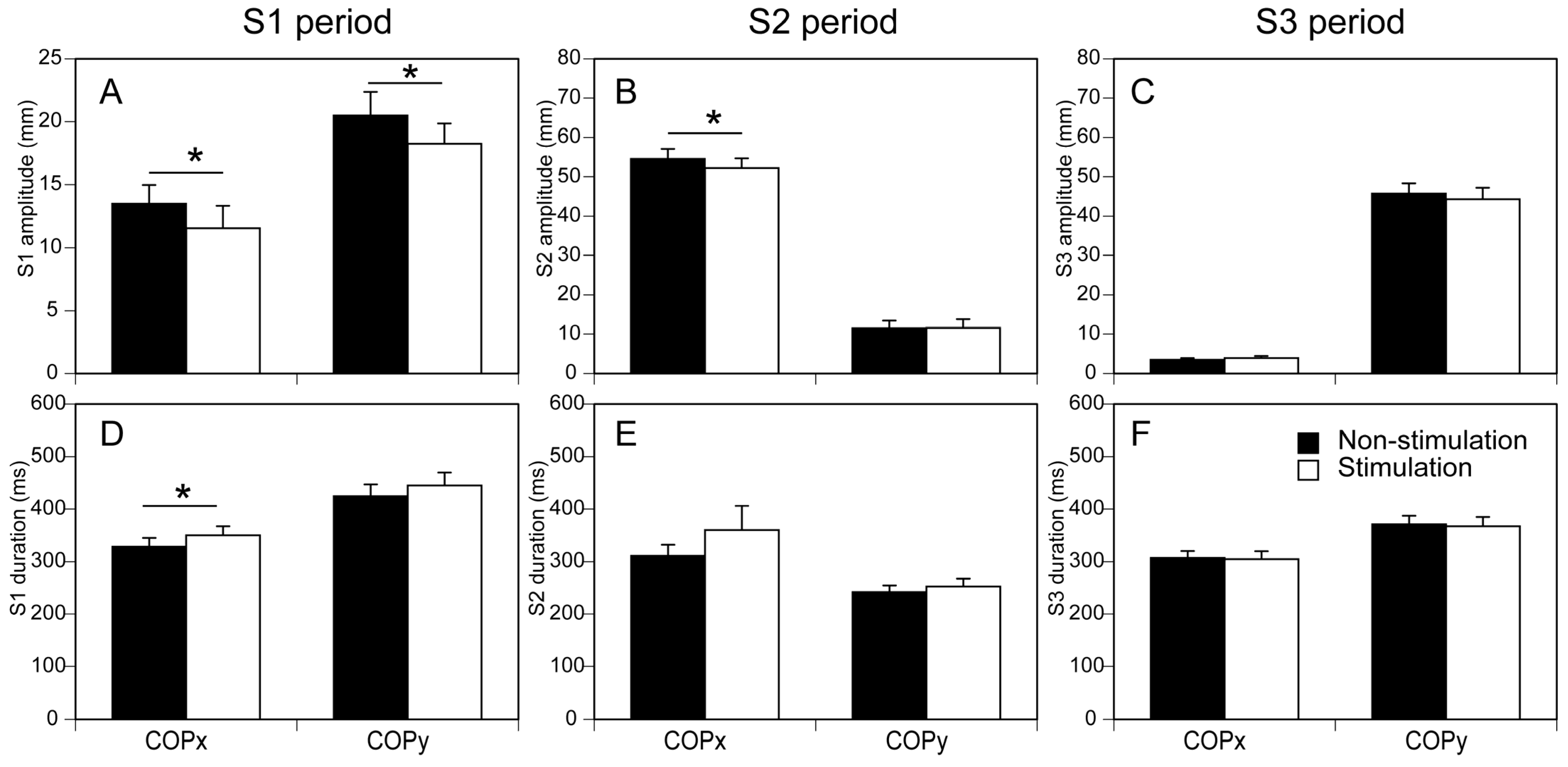
3.3. COP Displacement
3.4. Postural Movement Time
3.5. Selecting Initial Swing Leg
4. Discussion
4.1. COP Displacement in S1 and S2 Periods
4.2. APA and Postural Movement Time
4.3. Trigger of Gait Initiation
4.4. Selecting Initial Swing Leg
4.5. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Summers, I.R.; Francis, S.T.; Bowtell, R.W.; McGlone, F.P.; Clemence, M. A functional-magnetic-resonance-imaging investigation of cortical activation from moving vibrotactile stimuli on the fingertip. J. Acoust. Soc. Am. 2009, 125, 1033–1039. [Google Scholar] [CrossRef]
- Wacker, E.; Spitzer, B.; Lützkendorf, R.; Bernarding, J.; Blankenburg, F. Tactile motion and pattern processing assessed with high-field FMRI. PLoS ONE 2011, 6, e24860. [Google Scholar] [CrossRef] [PubMed]
- Amemiya, T.; Beck, B.; Walsh, V.; Gomi, H.; Haggard, P. Visual area V5/hMT+ contributes to perception of tactile motion direction: A TMS study. Sci. Rep. 2017, 7, 40937. [Google Scholar] [CrossRef] [PubMed]
- Sawaguchi, Y.; Kawasaki, T.; Hiraoka, K. Effect of Moving Tactile Stimuli to Mimic Altered Weight Distribution During Gait on Quiet Stance Body Sway. Percept. Mot. Ski. 2023; in press. [Google Scholar]
- Rogers, M.W.; Mille, M.L. Balance perturbations. Handb. Clin. Neurol. 2018, 159, 85–105. [Google Scholar]
- Mann, R.A.; Hagy, J.L.; White, V.; Liddell, D. The initiation of gait. JBJS 1979, 61, 232–239. [Google Scholar] [CrossRef]
- Burleigh-Jacobs, A.; Horak, F.B.; Nutt, J.G.; Obeso, J.A. Step initiation in Parkinson’s disease: Influence of levodopa and external sensory triggers. Mov. Disord. 1997, 12, 206–215. [Google Scholar] [CrossRef]
- McIlroy, W.E.; Maki, B.E. The control of lateral stability during rapid stepping reactions evoked by antero-posterior perturbation: Does anticipatory control play a role? Gait Posture 1999, 9, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Hass, C.J.; Gregor, R.J.; Waddell, D.E.; Oliver, A.; Smith, D.W.; Fleming, R.P.; Wolf, S.L. The influence of Tai Chi training on the center of pressure trajectory during gait initiation in older adults. Arch. Phys. Med. Rehabil. 2004, 85, 1593–1598. [Google Scholar] [CrossRef]
- Caderby, T.; Yiou, E.; Peyrot, N.; Begon, M.; Dalleau, G. Influence of gait speed on the control of mediolateral dynamic stability during gait initiation. J. Biomech. 2014, 47, 417–423. [Google Scholar] [CrossRef]
- Halliday, S.E.; Winter, D.A.; Frank, J.S.; Patla, A.E.; Prince, F. The initiation of gait in young, elderly, and Parkinson’s disease subjects. Gait Posture 1998, 8, 8–14. [Google Scholar] [CrossRef]
- Carpinella, I.; Crenna, P.; Calabrese, E.; Rabuffetti, M.; Mazzoleni, P.; Nemni, R.; Ferrarin, M. Locomotor function in the early stage of Parkinson’s disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Okada, Y.; Fukumoto, T.; Takatori, K.; Nagino, K.; Hiraoka, K. Variable initial swing side and prolonged double limb support represent abnormalities of the first three steps of gait initiation in patients with Parkinson’s disease with freezing of gait. Front. Neurol. 2011, 2, 85. [Google Scholar] [CrossRef]
- Dibble, L.E.; Nicholson, D.E.; Shultz, B.; MacWilliams, B.A.; Marcus, R.L.; Moncur, C. Sensory cueing effects on maximal speed gait initiation in persons with Parkinson’s disease and healthy elders. Gait Posture 2004, 19, 215–225. [Google Scholar] [CrossRef]
- Hiraoka, K.; Kunimura, H.; Oda, H.; Kawasaki, T.; Sawaguchi, Y. Rhythmic movement and rhythmic auditory cues enhance anticipatory postural adjustment of gait initiation. Somatosens. Mot. Res. 2020, 37, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, K.; Ae, M.; Ogura, N.; Sano, C.; Shiomi, K.; Morita, Y.; Yokoyama, H.; Iwata, Y.; Jono, Y.; Nomura, Y.; et al. Monaural Auditory Cue Affects the Process of Choosing the Initial Swing Leg in Gait Initiation. J. Mot. Behav. 2015, 47, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Hamill, P.V. NCHS Growth Curves for Children: Birth-18 Years, United States (No. 165); US Department of Health, Education, and Welfare: Washington, DC, USA; Public Health Service: Rockville, MD, USA; National Center for Health Statistics: Hyattsville, MD, USA, 1977. [Google Scholar]
- Thomas, J.R.; French, K.E. Gender differences across age in motor performance: A meta-analysis. Psychol. Bull. 1985, 98, 260. [Google Scholar] [CrossRef]
- Elias, L.J.; Bryden, M.P.; Bulman-Fleming, M.B. Footedness is a better predictor than is handedness of emotional lateralization. Neuropsychologia 1998, 36, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Zverev, Y.P. Spatial parameters of walking gait and footedness. Ann. Hum. Biol. 2006, 33, 161–176. [Google Scholar] [CrossRef]
- Perry, J.; Burnfield, J.M. Gait Analysis: Normal and Pathological Function, 2nd ed.; Slack: San Francisco, CA, USA, 2010. [Google Scholar]
- Dickstein, R.; Abulaffio, N. Postural sway of the affected and nonaffected pelvis and leg in stance of hemiparetic patients. Arch. Phys. Med. Rehabil. 2000, 81, 364–367. [Google Scholar] [CrossRef]
- Carpenter, M.G.; Frank, J.S.; Silcher, C.P.; Peysar, G.W. The influence of postural threat on the control of upright stance. Exp. Brain Res. 2001, 138, 210–218. [Google Scholar] [CrossRef]
- Yiou, E.; Do, M.C. Effects of medio-lateral postural perturbation induced by voluntary arm raising on the biomechanical organization of rapid step initiation. Mot. Control. 2011, 15, 507–524. [Google Scholar] [CrossRef] [PubMed]
- Yiou, E.; Caderby, T.; Delafontaine, A.; Fourcade, P.; Honeine, J.L. Balance control during gait initiation: State-of-the-art and research perspectives. World J. Orthop. 2017, 8, 815. [Google Scholar] [CrossRef] [PubMed]
- Mille, M.L.; Simoneau, M.; Rogers, M.W. Postural dependence of human locomotion during gait initiation. J. Neurophysiol. 2014, 112, 3095–3103. [Google Scholar] [CrossRef]
- Wang, T.Y.; Lin, S.I. Sensitivity of plantar cutaneous sensation and postural stability. Clin. Biomech. 2008, 23, 493–499. [Google Scholar] [CrossRef]
- Turcot, K.; Allet, L.; Golay, A.; Hoffmeyer, P.; Armand, S. Investigation of standing balance in diabetic patients with and without peripheral neuropathy using accelerometers. Clin. Biomech. 2009, 24, 716–721. [Google Scholar] [CrossRef]
- Sawaguchi, Y.; Kawasaki, T.; Oda, H.; Kunimura, H.; Hiraoka, K. Contribution of vision and tactile sensation on body sway during quiet stance. J. Phys. Ther. Sci. 2022, 34, 393–399. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kunimura, H.; Oda, H.; Kawasaki, T.; Tsujinaka, R.; Hamada, N.; Fukuda, S.; Matsuoka, M.; Hiraoka, K. Effect of Laterally Moving Tactile Stimuli to Sole on Anticipatory Postural Adjustment of Gait Initiation in Healthy Males. Brain Sci. 2023, 13, 1411. https://doi.org/10.3390/brainsci13101411
Kunimura H, Oda H, Kawasaki T, Tsujinaka R, Hamada N, Fukuda S, Matsuoka M, Hiraoka K. Effect of Laterally Moving Tactile Stimuli to Sole on Anticipatory Postural Adjustment of Gait Initiation in Healthy Males. Brain Sciences. 2023; 13(10):1411. https://doi.org/10.3390/brainsci13101411
Chicago/Turabian StyleKunimura, Hiroshi, Hitoshi Oda, Taku Kawasaki, Ryo Tsujinaka, Naoki Hamada, Shiho Fukuda, Masakazu Matsuoka, and Koichi Hiraoka. 2023. "Effect of Laterally Moving Tactile Stimuli to Sole on Anticipatory Postural Adjustment of Gait Initiation in Healthy Males" Brain Sciences 13, no. 10: 1411. https://doi.org/10.3390/brainsci13101411