
Survival in the Three Common Variants of Primary Progressive Aphasia: A Retrospective Study in a Tertiary Memory Clinic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Data Collection
- Socio-demographic data: gender, years of education;
- Clinical data: diagnosis, MMSE at onset, age at symptoms onset, age at first visit, age at diagnosis, age of death, cause of death, duration from onset to diagnosis, duration from onset to first visit, duration from first visit to diagnosis, disease duration from diagnosis, and disease duration from onset.
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
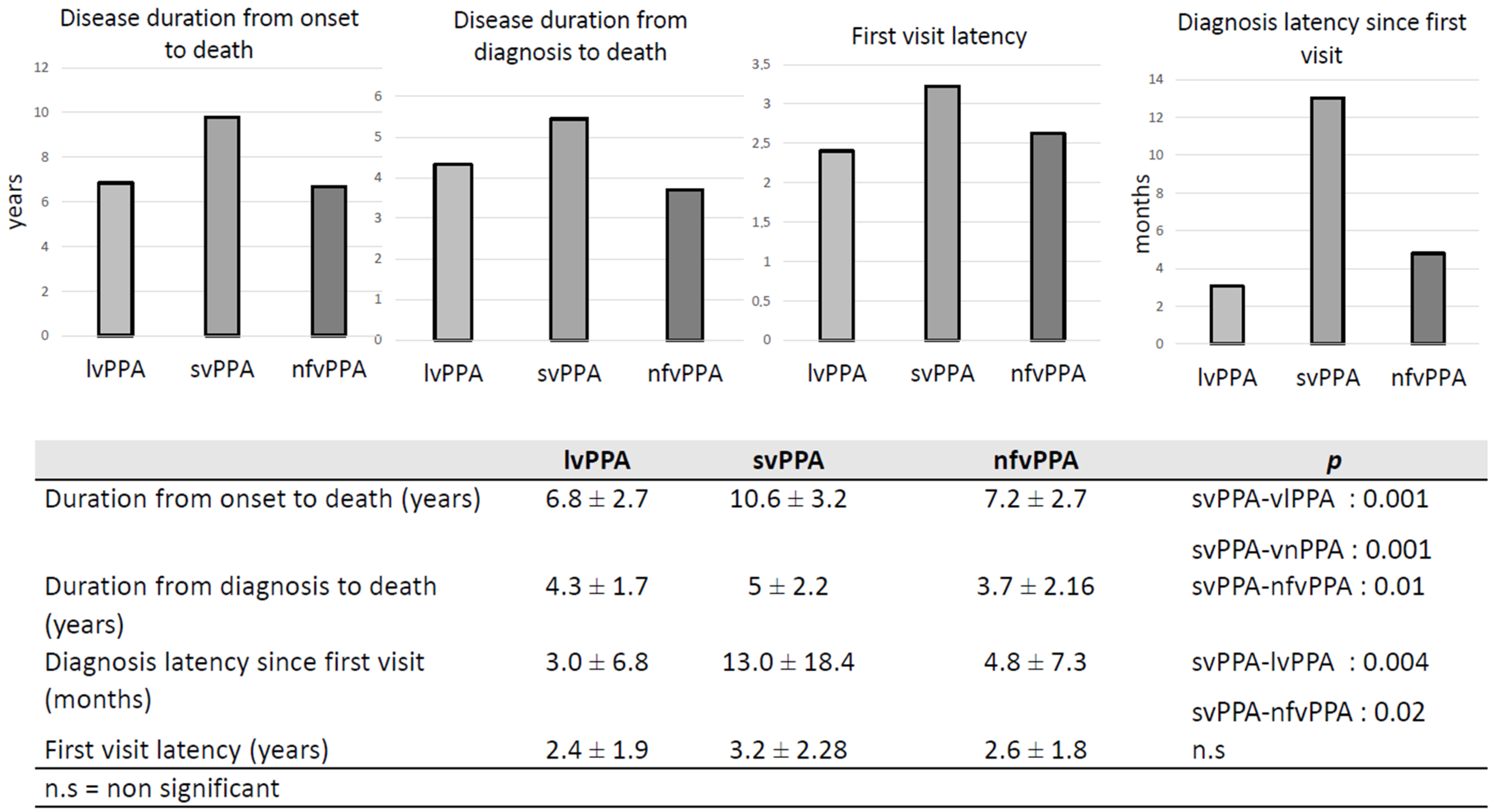
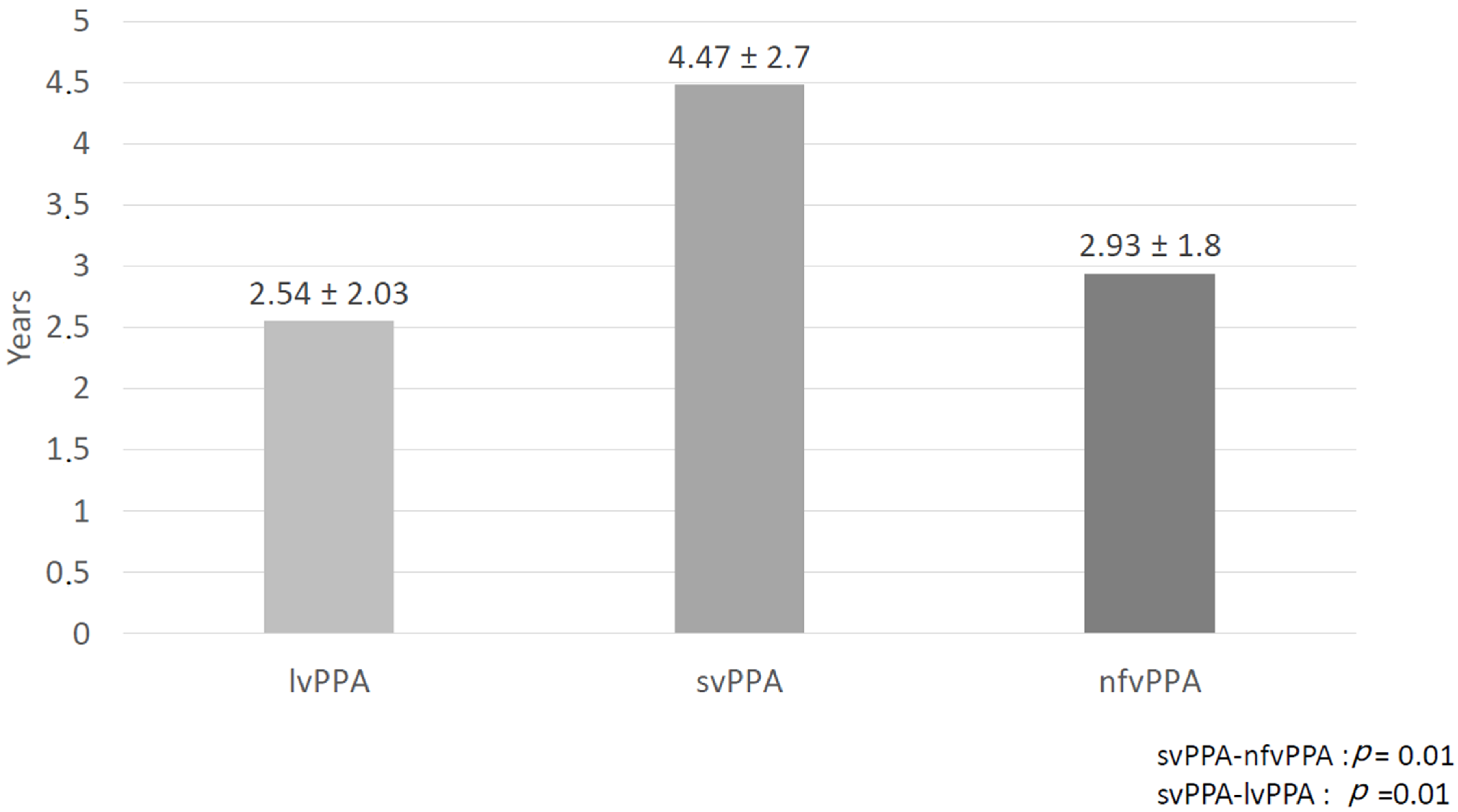
3.2. Disease Duration
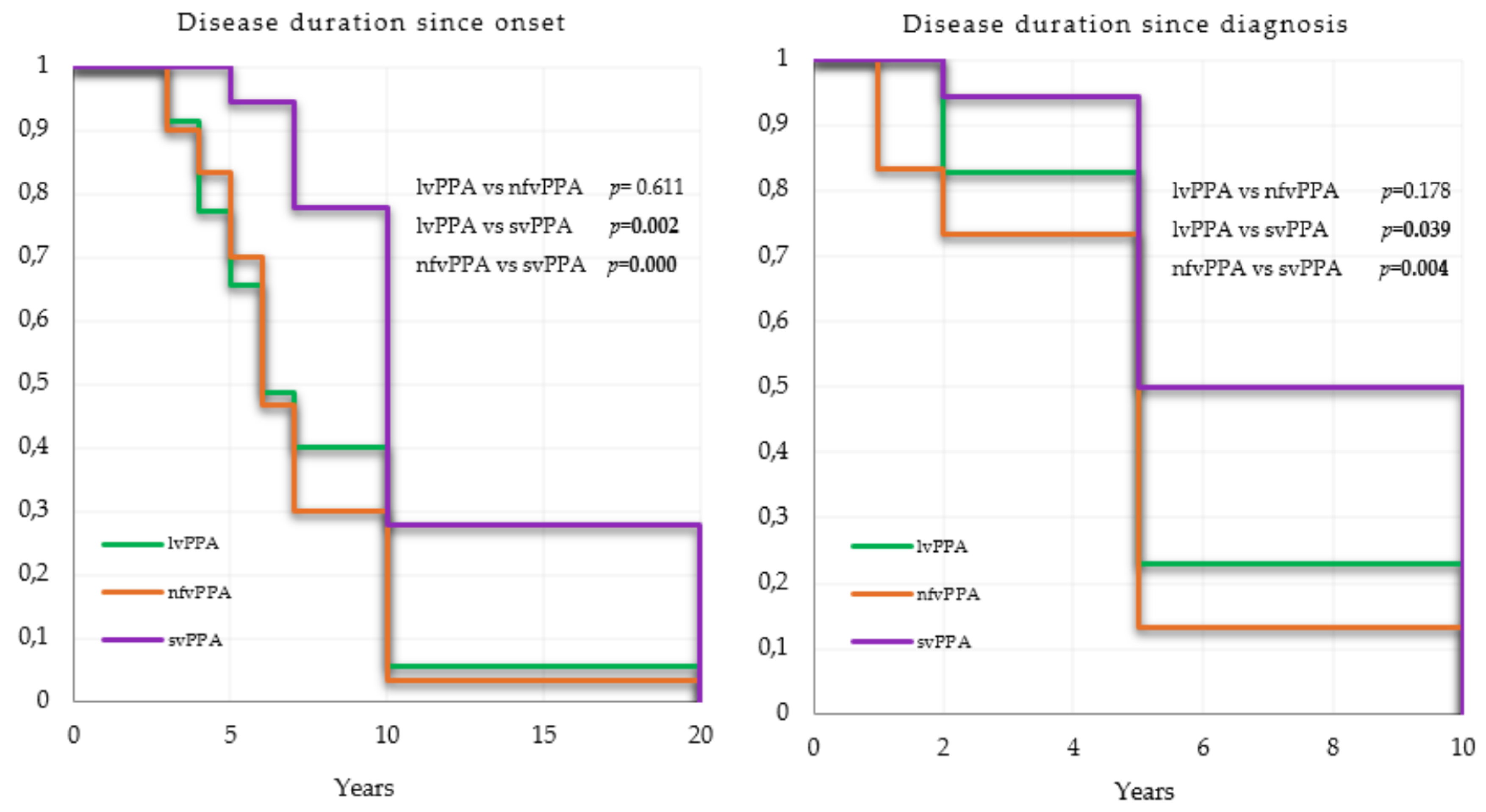
3.3. Survival Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mesulam, M.-M. Primary Progressive Aphasia. Ann. Neurol. 2001, 49, 425–432. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of Primary Progressive Aphasia and Its Variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [Green Version]
- Grossman, M. Primary Progressive Aphasia: Clinicopathological Correlations. Nat. Rev. Neurol. 2010, 6, 88–97. [Google Scholar] [CrossRef] [Green Version]
- Ratnavalli, E.; Brayne, C.; Dawson, K.; Hodges, J.R. The Prevalence of Frontotemporal Dementia. Neurology 2002, 58, 1615–1621. [Google Scholar] [CrossRef]
- Onyike, C.U.; Diehl-Schmid, J. The Epidemiology of Frontotemporal Dementia. Int. Rev. Psychiatry 2013, 25, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Gilberti, N.; Turla, M.; Alberici, A.; Bertasi, V.; Civelli, P.; Archetti, S.; Padovani, A.; Borroni, B. Prevalence of Frontotemporal Lobar Degeneration in an Isolated Population: The Vallecamonica Study. Neurol. Sci. 2012, 33, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Magnin, E.; Démonet, J.-F.; Wallon, D.; Dumurgier, J.; Troussière, A.-C.; Jager, A.; Duron, E.; Gabelle, A.; de la Sayette, V.; Volpe-Gillot, L.; et al. Primary Progressive Aphasia in the Network of French Alzheimer Plan Memory Centers. J. Alzheimers Dis. 2016, 54, 1459–1471. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, D.; Gorno-Tempini, M.L.; Rabinovici, G.D.; Santos-Santos, M.A.; Seeley, W.; Miller, B.L.; Pijnenburg, Y.; Keulen, M.A.; Groot, C.; van Berckel, B.N.M.; et al. Prevalence of Amyloid-β Pathology in Distinct Variants of Primary Progressive Aphasia. Ann. Neurol. 2018, 84, 729–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moyle, W.; Murfield, J.E. Health-Related Quality of Life in Older People with Severe Dementia: Challenges for Measurement and Management. Expert Rev. Pharm. Outcomes Res. 2013, 13, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Manuel, D.G.; Garner, R.; Finès, P.; Bancej, C.; Flanagan, W.; Tu, K.; Reimer, K.; Chambers, L.W.; Bernier, J. Alzheimer’s and Other Dementias in Canada, 2011 to 2031: A Microsimulation Population Health Modeling (POHEM) Study of Projected Prevalence, Health Burden, Health Services, and Caregiving Use. Popul. Health Metr. 2016, 14, 344–362. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.J.; Goodison, H.; Sampson, E.L. The Role of the Memory Service in Helping Carers to Prepare for End of Life: A Mixed Methods Study. Int. J. Geriatr. Psychiatry 2019, 34, 360–368. [Google Scholar] [CrossRef]
- Moore, K.J.; Davis, S.; Gola, A.; Harrington, J.; Kupeli, N.; Vickerstaff, V.; King, M.; Leavey, G.; Nazareth, I.; Jones, L.; et al. Experiences of End of Life amongst Family Carers of People with Advanced Dementia: Longitudinal Cohort Study with Mixed Methods. BMC Geriatr. 2017, 17, 135. [Google Scholar] [CrossRef]
- Kansal, K.; Mareddy, M.; Sloane, K.L.; Minc, A.A.; Rabins, P.V.; McGready, J.B.; Onyike, C.U. Survival in Frontotemporal Dementia Phenotypes: A Meta-Analysis. Dement. Geriatr. Cogn. Disord. 2016, 41, 109–122. [Google Scholar] [CrossRef]
- R Foundation for Statistical Computing; R Development Core Team R. A Language and Environment for Statistical Computing; R Development Core Team R: Vienna, Austria, 2008; ISBN 3900051070. [Google Scholar]
- Hodges, J.R.; Davies, R.; Xuereb, J.; Kril, J.; Halliday, G. Survival in Frontotemporal Dementia. Neurology 2003, 61, 349–354. [Google Scholar] [CrossRef]
- Kertesz, A.; Blair, M.; McMonagle, P.; Munoz, D.G. The Diagnosis and Course of Frontotemporal Dementia. Alzheimer Dis. Assoc. Disord. 2007, 21, 155–163. [Google Scholar] [CrossRef]
- Nunnemann, S.; Last, D.; Schuster, T.; Förstl, H.; Kurz, A.; Diehl-Schmid, J. Survival in a German Population with Frontotemporal Lobar Degeneration. Neuroepidemiology 2011, 37, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Roberson, E.D.; Hesse, J.H.; Rose, K.D.; Slama, H.; Johnson, J.K.; Yaffe, K.; Forman, M.S.; Miller, C.A.; Trojanowski, J.Q.; Kramer, J.H.; et al. Frontotemporal Dementia Progresses to Death Faster than Alzheimer Disease. Neurology 2005, 65, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, C.; Polito, C.; Vannucchi, S.; Piaceri, I.; Bagnoli, S.; Lombardi, G.; Lucidi, G.; Berti, V.; Nacmias, B.; Sorbi, S. Primary Progressive Aphasia: Natural History in an Italian Cohort. Alzheimer Dis. Assoc. Disord. 2019, 33, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Matias-Guiu, J.A.; Cabrera-Martín, M.N.; Moreno-Ramos, T.; García-Ramos, R.; Porta-Etessam, J.; Carreras, J.L.; Matías-Guiu, J. Clinical Course of Primary Progressive Aphasia: Clinical and FDG-PET Patterns. J. Neurol. 2015, 262, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Ulugut, H.; Stek, S.; Wagemans, L.E.E.; Jutten, R.J.; Keulen, M.A.; Bouwman, F.H.; Prins, N.D.; Lemstra, A.W.; Krudop, W.; Teunissen, C.E.; et al. The Natural History of Primary Progressive Aphasia: Beyond Aphasia. J. Neurol. 2021, 831, 442–468. [Google Scholar] [CrossRef]
- Van Langenhove, T.; Leyton, C.E.; Piguet, O.; Hodges, J.R. Comparing Longitudinal Behavior Changes in the Primary Progressive Aphasias. J. Alzheimers Dis. 2016, 53, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Foxe, D.; Irish, M.; Hu, A.; Carrick, J.; Hodges, J.R.; Ahmed, R.M.; Burrell, J.R.; Piguet, O. Longitudinal Cognitive and Functional Changes in Primary Progressive Aphasia. J. Neurol. 2021, 321, 23–36. [Google Scholar] [CrossRef]
- Rogalski, E.; Cobia, D.; Harrison, T.M.; Wieneke, C.; Weintraub, S.; Mesulam, M.-M. Progression of Language Decline and Cortical Atrophy in Subtypes of Primary Progressive Aphasia. Neurology 2011, 76, 1804–1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ash, S.; Nevler, N.; Phillips, J.; Irwin, D.J.; McMillan, C.T.; Rascovsky, K.; Grossman, M. A Longitudinal Study of Speech Production in Primary Progressive Aphasia and Behavioral Variant Frontotemporal Dementia. Brain Lang. 2019, 194, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.; Hodges, J.R.; Leyton, C.E.; Mioshi, E. Longitudinal Changes in Primary Progressive Aphasias: Differences in Cognitive and Dementia Staging Measures. Dement. Geriatr. Cogn. Disord. 2012, 34, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Henry, M.L.; Grasso, S.M. Assessment of Individuals with Primary Progressive Aphasia. Semin. Speech Lang. 2018, 39, 231–241. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| lvPPA (n = 35) | nfvPPA (n = 30) | svPPA (n = 18) | p | |
|---|---|---|---|---|
| Male/Female | 19/16 | 15/15 | 9/9 | n.s |
| Education years (mean ± SD) | 11.7 ±4.4 | 11.03 ± 4.2 | 13.17 ± 4.1 | n.s |
| Education level (>12 years) | 15 | 9 | 12 | 0.026 |
| MMSE 1st visit (mean ± SD) | 21.03 ± 5.9 | 21.67 ± −6.8 | 22.35 ± 7.4 | n.s |
| Age of onset (mean ± SD) | 69.05 ± 10.8 | 70.13 ± 6.9 | 64.38 ± 7.8 | n.s |
| Age at diagnosis (mean ± SD) | 71.65 ± 10.22 | 73.1 ± 6.79 | 68.68 ± 8.5 | n.s |
| Age of death (mean ± SD) | 75.90 ± 9.5 | 76.8 ± 6.3 | 74.11 ± 8.3 | n.s |
| Mean Survival | Estimated Median Survival | |||
|---|---|---|---|---|
| Since Onset | Since Diagnosis | Since Onset | Since Diagnosis | |
| lvPPA (n = 35) | 7.6 CI95%: 6.2–8.9 | 5.6 CI95%: 4.5–6.5 | 6 CI95%: 5.0–10.0 | 5 CI95%: 0.0–10 |
| nfvPPA (n = 30) | 7.1 CI95%: 5.9–8.3 | 4.7 CI95%: 3.7–7.6 | 6 CI95%: 6.00–7.00 | 5 CI95%: 0.0–10.0 |
| svPPA (n = 18) | 12 CI95%: 9.5–14.4 | 7.3 CI95%: 6.0–8.6 | 10 CI95%: 0.0–20.0) | 7.5 CI95%: 5.0–10.0 |
| lvPPA | nfvPPA | svPPA | ||||
|---|---|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| MMSE 1st visit | 0.96 (0.89–1.03) | 0.30 | 0.96 (0.89–1.02) | 0.21 | 0.99 (0.89–1.10) | 0.90 |
| Age of onset | 1.05 (1.00–1.08) | 0.02 | 1.03 (0.95–1.11) | 0.52 | 0.96 (0.86–1.07) | 0.43 |
| Years of education | 1.02 (0.94–1.11) | 0.56 | 1.02 (0.88–1.17) | 0.84 | 0.98 (0.82–1.16) | 0.81 |
| Gender | 1.36 (0.56–3.32) | 0.50 | 0.82 (0.33–2.08) | 0.68 | 0.46 (0.13–1.64) | 0.2 |
| lvPPA | nfvPPA | svPPA | ||||
|---|---|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| MMSE 1st visit | 0.98 (0.92–1.06) | 0.66 | 0.98 (0.87–1.10) | 0.39 | 0.99 (0.89–1.10) | 0.91 |
| Age of onset | 1.01 (0.98–1.06) | 0.48 | 1.02 (0.95–1.11) | 0.52 | 1.00 (0.91–1.09) | 0.99 |
| Years of education | 1.02 (0.94–1.10) | 0.57 | 0.98 (0.87–1.10) | 0.74 | 0.99 (0.82–1.20) | 0.98 |
| Gender | 0.80 (0.36–1.81) | 0.60 | 1.19 (0.49–2.84) | 0.70 | 1.12 (0.28–4.52) | 0.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tastevin, M.; Lavoie, M.; de la Sablonnière, J.; Carrier-Auclair, J.; Laforce, R., Jr. Survival in the Three Common Variants of Primary Progressive Aphasia: A Retrospective Study in a Tertiary Memory Clinic. Brain Sci. 2021, 11, 1113. https://doi.org/10.3390/brainsci11091113
Tastevin M, Lavoie M, de la Sablonnière J, Carrier-Auclair J, Laforce R Jr. Survival in the Three Common Variants of Primary Progressive Aphasia: A Retrospective Study in a Tertiary Memory Clinic. Brain Sciences. 2021; 11(9):1113. https://doi.org/10.3390/brainsci11091113
Chicago/Turabian StyleTastevin, Maud, Monica Lavoie, Justine de la Sablonnière, Julie Carrier-Auclair, and Robert Laforce, Jr. 2021. "Survival in the Three Common Variants of Primary Progressive Aphasia: A Retrospective Study in a Tertiary Memory Clinic" Brain Sciences 11, no. 9: 1113. https://doi.org/10.3390/brainsci11091113