
Primary Progressive Aphasia: Use of Graphical Markers for an Early and Differential Diagnosis

 ,
,
Abstract
:1. Introduction
1.1. Diagnosis and Classification
1.2. Early Diagnosis
1.3. Contribution of Graphical Markers
2. Materials and Methods
2.1. Ethics
2.2. Population
2.3. Procedure
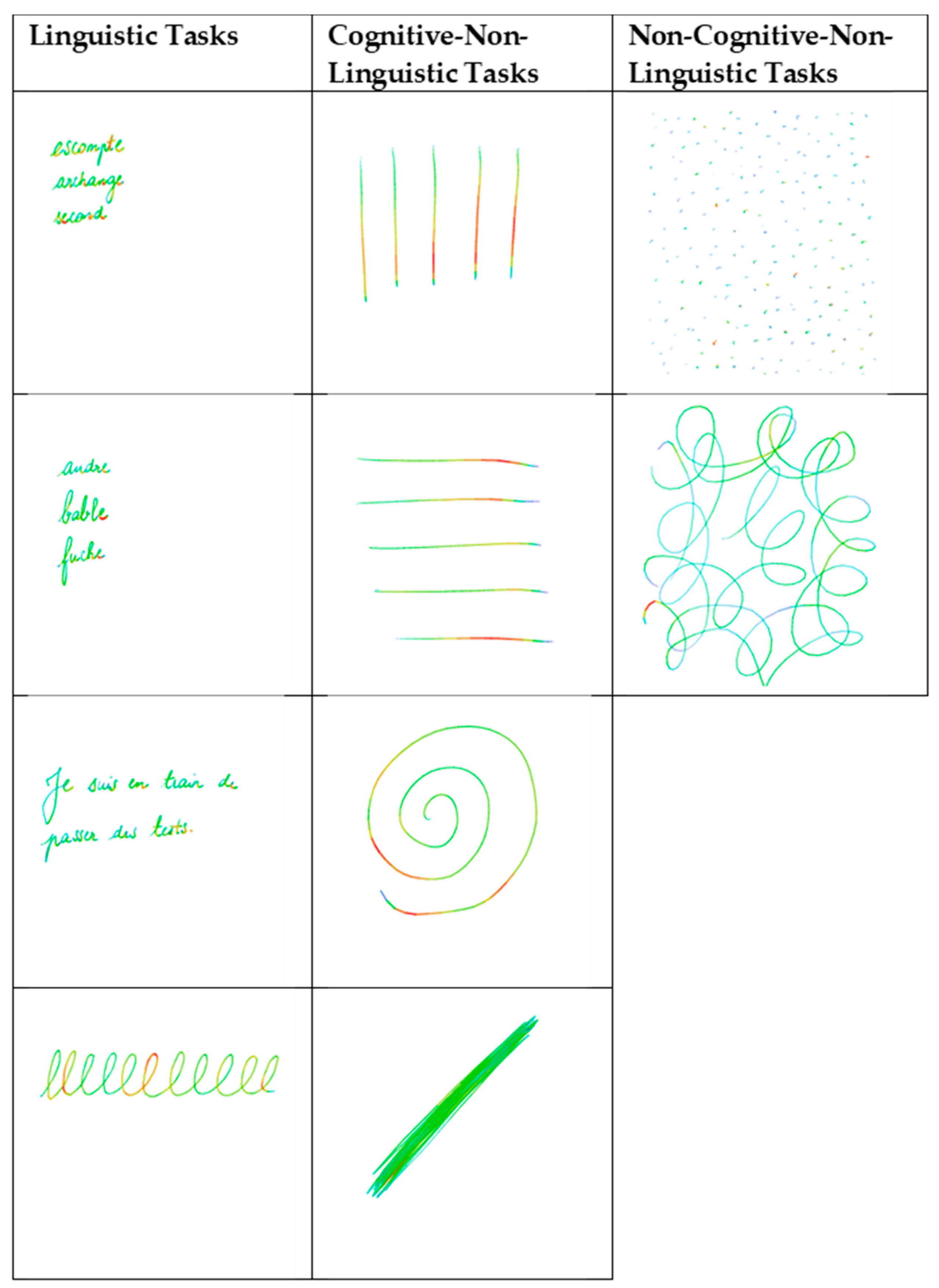
2.4. Material and Variables
2.5. Statistical Analyses
3. Results
3.1. Demographic and Clinical Information
3.2. Graphical Markers
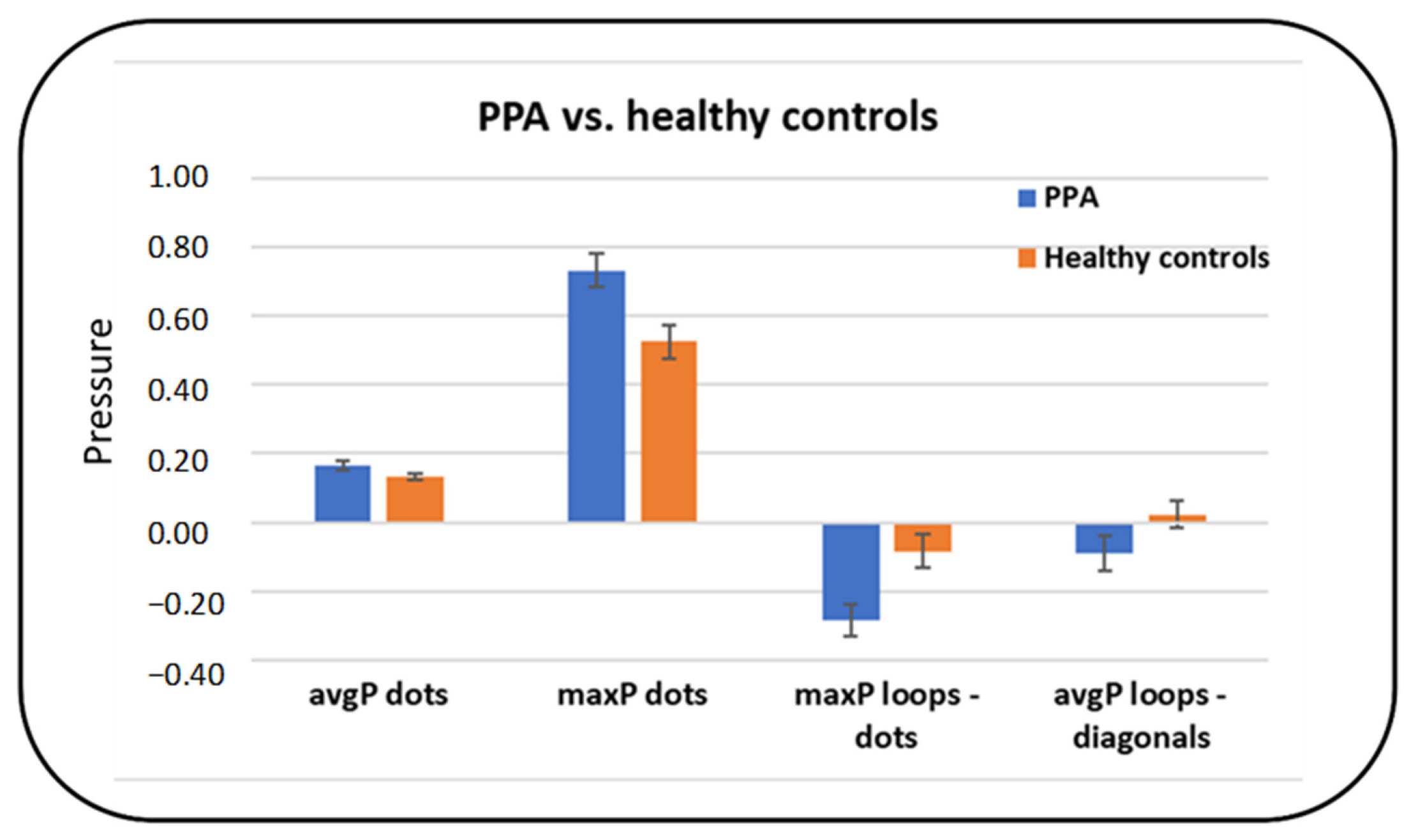
3.2.1. Average Pressure (avgP)
3.2.2. Maximum Pressure (maxP)
3.2.3. Summary of the Main Differences between PPA and Healthy Controls
3.2.4. Summary of the Main Differences between PPA and AD
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mesulam, M.M. Primary progressive aphasia. Ann. Neurol. 2001, 49, 425–432. [Google Scholar] [CrossRef]
- Mesulam, M.-M. Primary Progressive Aphasia—A Language-Based Dementia. N. Engl. J. Med. 2003, 349, 1535–1542. [Google Scholar] [CrossRef] [PubMed]
- Grossman, M.; Ash, S. Primary Progressive Aphasia: A Review. Neurocase 2004, 10, 3–18. [Google Scholar] [CrossRef]
- Marshall, C.R.; Hardy, C.J.D.; Volkmer, A.; Russell, L.L.; Bond, R.L.; Fletcher, P.D.; Clark, C.N.; Mummery, C.J.; Schott, J.M.; Rossor, M.N.; et al. Primary progressive aphasia: A clinical approach. J. Neurol. 2018, 265, 1474–1490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratnavalli, E.; Brayne, C.; Dawson, K.; Hodges, J.R. The prevalence of frontotemporal dementia. Neurology 2002, 58, 1615–1621. [Google Scholar] [CrossRef] [PubMed]
- Le Rhun, E.; Richard, F.; Pasquier, F. Natural history of primary progressive aphasia. Neurology 2005, 65, 887–891. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kertesz, A.; Morlog, D.; Light, M.; Blair, M.; Davidson, W.; Jesso, S.; Brashear, R. Galantamine in Frontotemporal Dementia and Primary Progressive Aphasia. Dement. Geriatr. Cogn. Disord. 2008, 25, 178–185. [Google Scholar] [CrossRef]
- Weintraub, S.; Rubin, N.P.; Mesulam, M.M. Primary progressive aphasia. Longitudinal course, neuropsychological profile, and language features. Arch. Neurol. 1990, 47, 1329–1335. [Google Scholar] [CrossRef]
- Mesulam, M. Primary progressive aphasia: A dementia of the language network. Dement. Neuropsychol. 2013, 7, 2–9. [Google Scholar] [CrossRef]
- Josephs, K.A. Clinicopathological and imaging correlates of progressive aphasia and apraxia of speech. Brain 2006, 129, 1385–1398. [Google Scholar] [CrossRef] [Green Version]
- Gorno-Tempini, M.L.; Dronkers, N.F.; Rankin, K.P.; Ogar, J.M.; Phengrasamy, L.; Rosen, H.J.; Johnson, J.K.; Weiner, M.W.; Miller, B.L. Cognition and anatomy in three variants of primary progressive aphasia. Ann. Neurol. 2004, 55, 335–346. [Google Scholar] [CrossRef] [Green Version]
- Gorno-Tempini, M.L.; Brambati, S.M.; Ginex, V.; Ogar, J.; Dronkers, N.F.; Marcone, A.; Perani, D.; Garibotto, V.; Cappa, S.F.; Miller, B.L. The logopenic/phonological variant of primary progressive aphasia. Neurology 2008, 71, 1227–1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, S.M.; Henry, M.L.; Besbris, M.; Ogar, J.M.; Dronkers, N.F.; Jarrold, W.; Miller, B.L.; Gorno-Tempini, M.L. Connected speech production in three variants of primary progressive aphasia. Brain 2010, 133, 2069–2088. [Google Scholar] [CrossRef] [Green Version]
- Rohrer, J.D.; Warren, J.D.; Modat, M.; Ridgway, G.R.; Douiri, A.; Rossor, M.N.; Ourselin, S.; Fox, N.C. Patterns of cortical thinning in the language variants of frontotemporal lobar degeneration. Neurology 2009, 72, 1562–1569. [Google Scholar] [CrossRef] [Green Version]
- Montembeault, M.; Brambati, S.M.; Gorno-Tempini, M.L.; Migliaccio, R. Clinical, Anatomical, and Pathological Features in the Three Variants of Primary Progressive Aphasia: A Review. Front. Neurol. 2018, 9, 692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, M.; Mickanin, J.; Onishi, K.; Hughes, E.; D’Esposito, M.; Ding, X.-S.; Alavi, A.; Reivich, M. Progressive Nonfluent Aphasia: Language, Cognitive, and PET Measures Contrasted with Probable Alzheimer’s Disease. J. Cogn. Neurosci. 1996, 8, 135–154. [Google Scholar] [CrossRef] [PubMed]
- Knibb, J.A.; Woollams, A.M.; Hodges, J.R.; Patterson, K. Making sense of progressive non-fluent aphasia: An analysis of conversational speech. Brain 2009, 132, 2734–2746. [Google Scholar] [CrossRef] [Green Version]
- Rohrer, J.D.; Warren, J.D. Phenomenology and anatomy of abnormal behaviours in primary progressive aphasia. J. Neurol. Sci. 2010, 293, 35–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohrer, J.D.; Ridgway, G.R.; Crutch, S.J.; Hailstone, J.; Goll, J.C.; Clarkson, M.J.; Mead, S.; Beck, J.; Mummery, C.; Ourselin, S.; et al. Progressive logopenic/phonological aphasia: Erosion of the language network. NeuroImage 2010, 49, 984–993. [Google Scholar] [CrossRef] [Green Version]
- Hodges, J.R.; Patterson, K.; Oxbury, S.; Funnell, E. Semantic dementia. Progressive fluent aphasia with temporal lobe atrophy. Brain J. Neurol. 1992, 115 Pt 6, 1783–1806. [Google Scholar] [CrossRef]
- Adlam, A.-L.R.; Patterson, K.; Rogers, T.T.; Nestor, P.J.; Salmond, C.H.; Acosta-Cabronero, J.; Hodges, J.R. Semantic dementia and fluent primary progressive aphasia: Two sides of the same coin? Brain 2006, 129, 3066–3080. [Google Scholar] [CrossRef] [Green Version]
- Mummery, C.J.; Patterson, K.; Price, C.J.; Ashburner, J.; Frackowiak, R.S.; Hodges, J.R. A voxel-based morphometry study of semantic dementia: Relationship between temporal lobe atrophy and semantic memory. Ann. Neurol. 2000, 47, 36–45. [Google Scholar] [CrossRef]
- Rosen, H.J.; Perry, R.J.; Murphy, J.; Kramer, J.H.; Mychack, P.; Schuff, N.; Weiner, M.; Levenson, R.W.; Miller, B.L. Emotion comprehension in the temporal variant of frontotemporal dementia. Brain J. Neurol. 2002, 125, 2286–2295. [Google Scholar] [CrossRef]
- Garrard, P.; Hodges, J.R. Semantic dementia: Clinical, radiological and pathological perspectives. J. Neurol. 2000, 247, 409–422. [Google Scholar] [CrossRef]
- Agosta, F.; Henry, R.G.; Migliaccio, R.; Neuhaus, J.; Miller, B.L.; Dronkers, N.F.; Brambati, S.M.; Filippi, M.; Ogar, J.M.; Wilson, S.M.; et al. Language networks in semantic dementia. Brain 2010, 133, 286–299. [Google Scholar] [CrossRef] [PubMed]
- Vandenberghe, R. Classification of the primary progressive aphasias: Principles and review of progress since 2011. Alzheimers Res. Ther. 2016, 8, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westbury, C.; Bub, D. Primary Progressive Aphasia: A Review of 112 Cases. Brain Lang. 1997, 60, 381–406. [Google Scholar] [CrossRef] [PubMed]
- Mouton, A.; Plonka, A.; Fabre, R.; Tran, M.; Robert, P.; Macoir, J.; Manera, V.; Gros, A. The Course of Primary Progressive Aphasia Diagnosis: A Cross-Sectional Study. Available online: https://www.researchsquare.com/article/rs-440319/v1 (accessed on 22 April 2021).
- Dubois, B.; Feldman, H.H.; Jacova, C.; Cummings, J.L.; Dekosky, S.T.; Barberger-Gateau, P.; Delacourte, A.; Frisoni, G.; Fox, N.C.; Galasko, D.; et al. Revising the definition of Alzheimer’s disease: A new lexicon. Lancet Neurol. 2010, 9, 1118–1127. [Google Scholar] [CrossRef]
- Harciarek, M.; Sitek, E.J.; Kertesz, A. The patterns of progression in primary progressive aphasia—Implications for assessment and management. Aphasiology 2014, 28, 964–980. [Google Scholar] [CrossRef]
- Routhier, S.; Gravel-Laflamme, K.; Macoir, J. Non-pharmacological therapies for language deficits in the agrammatic and logopenic variants of primary progressive aphasia: A literature review. Gériatrie Psychol. Neuropsychiatr. Viellissement 2013, 11, 87–97. [Google Scholar] [CrossRef]
- Nagai, C.; Iwata, M. Writing disorders in primary progressive aphasia. Rinsho Shinkeigaku 2003, 43, 84–92. [Google Scholar]
- Graham, N.L. Dysgraphia in primary progressive aphasia: Characterisation of impairments and therapy options. Aphasiology 2014, 28, 1092–1111. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Vilda, P.; Perez-Broncano, O.; Martinez-Olalla, R.; Rodellar-Biarge, V.; Lopez de Ipina Pena, K.; Ecay, M.; Martinez-Lage, P. Biomechanical characterization of phonation in Alzheimer’s Disease. In Proceedings of the 3rd IEEE International Work-Conference on Bioinspired Intelligence; IEEE: Liberia, Costa Rica, 2014; pp. 14–20. Available online: http://ieeexplore.ieee.org/document/6913931/ (accessed on 2 October 2014).
- Brown, L.J.E.; Adlam, T.; Hwang, F.; Khadra, H.; Maclean, L.M.; Rudd, B.; Smith, T.; Timon, C.; Williams, E.A.; Astell, A.J. Computer-based tools for assessing micro-longitudinal patterns of cognitive function in older adults. AGE 2016, 38, 335–350. [Google Scholar] [CrossRef] [Green Version]
- Wild, K.; Howieson, D.; Webbe, F.; Seelye, A.; Kaye, J. Status of computerized cognitive testing in aging: A systematic review. Alzheimers Dement. 2008, 4, 428–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afonso, O.; Álvarez, C.J.; Martínez, C.; Cuetos, F. Writing difficulties in Alzheimer’s disease and mild cognitive impairment. Read. Writ. 2019, 32, 217–233. [Google Scholar] [CrossRef] [Green Version]
- Nazir, T.A.; Hrycyk, L.; Moreau, Q.; Frak, V.; Cheylus, A.; Ott, L.; Lindemann, O.; Fischer, M.H.; Paulignan, Y.; Delevoye-Turrell, Y. A simple technique to study embodied language processes: The grip force sensor. Behav. Res. Methods 2017, 49, 61–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahindo, C.; El-Yacoubi, M.A.; Garcia-Salicetti, S.; Rigaud, A.-S.; Cristancho-Lacroix, V. Characterizing Early-Stage Alzheimer Through Spatiotemporal Dynamics of Handwriting. IEEE Signal Process. Lett. 2018, 25, 1136–1140. [Google Scholar] [CrossRef]
- Gros, A.; Plonka, A.; Manera, V. Graphic markers: Towards an early diagnosis of primary progressive aphasia. Alzheimers Dement. 2019, 15, P351–P352. [Google Scholar] [CrossRef]
- Macoir, J.; Fossard, M.; Lefebvre, L.; Monetta, L.; Renard, A.; Tran, T.M.; Wilson, M.A. Detection Test for Language Impairments in Adults and the Aged—A New Screening Test for Language Impairment Associated With Neurodegenerative Diseases: Validation and Normative Data. Am. J. Alzheimers Dis. Dementiasr 2017, 32, 382–392. [Google Scholar] [CrossRef] [Green Version]
- Macoir, J.; Fossard, M.; Lefebvre, L.; Monetta, L.; Renard, A.; Tran, T.M.; Wilson, M. DTLA-Détection des Troubles du Langage Chez L’adulte et la Personne Agée. 2017. Available online: https://www.researchgate.net/publication/317905040_DTLA_-_Detection_des_troubles_du_langage_chez_l%27adulte_et_la_personne_agee (accessed on 2 October 2014). [CrossRef]
- Werner, P.; Rosenblum, S.; Bar-On, G.; Heinik, J.; Korczyn, A. Handwriting process variables discriminating mild Alzheimer’s disease and mild cognitive impairment. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2006, 61, 228–236. [Google Scholar] [CrossRef]
- Van Galen, G.P. Handwriting: Issues for a psychomotor theory. Hum. Mov. Sci. 1991, 10, 165–191. [Google Scholar] [CrossRef]
- Nelissen, N.; Pazzaglia, M.; Vandenbulcke, M.; Sunaert, S.; Fannes, K.; Dupont, P.; Aglioti, S.M.; Vandenberghe, R. Gesture Discrimination in Primary Progressive Aphasia: The Intersection between Gesture and Language Processing Pathways. J. Neurosci. 2010, 30, 6334–6341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitek, E.J.; Barczak, A.; Kluj-Kozłowska, K.; Kozłowski, M.; Barcikowska, M.; Sławek, J. Is descriptive writing useful in the differential diagnosis of logopenic variant of primary progressive aphasia, Alzheimer’s disease and mild cognitive impairment? Neurol. Neurochir. Pol. 2015, 49, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Schröter, A.; Mergl, R.; Bürger, K.; Hampel, H.; Möller, H.-J.; Hegerl, U. Kinematic Analysis of Handwriting Movements in Patients with Alzheimer’s Disease, Mild Cognitive Impairment, Depression and Healthy Subjects. Dement. Geriatr. Cogn. Disord. 2003, 15, 132–142. [Google Scholar] [CrossRef] [Green Version]
- Slavin, M.J.; Phillips, J.G.; Bradshaw, J.L.; Hall, K.A.; Presnell, I. Consistency of handwriting movements in dementia of the Alzheimer’s type: A comparison with Huntington’s and Parkinson’s diseases. J. Int. Neuropsychol. Soc. 1999, 5, 20–25. [Google Scholar] [CrossRef]
- Yu, N.-Y.; Chang, S.-H. Kinematic Analyses of Graphomotor Functions in Individuals with Alzheimer’s Disease and Amnestic Mild Cognitive Impairment. J. Med. Biol. Eng. 2016, 36, 334–343. [Google Scholar] [CrossRef]
- Szatloczki, G.; Hoffmann, I.; Vincze, V.; Kalman, J.; Pakaski, M. Speaking in Alzheimer’s Disease, is That an Early Sign? Importance of Changes in Language Abilities in Alzheimer’s Disease. Front. Aging Neurosci. 2015, 7. [Google Scholar] [CrossRef] [Green Version]
- Platel, H.; Lambert, J.; Eustache, F.; Cadet, B.; Dary, M.; Viader, F.; Lechevalier, B. Characteristics and evolution of writing impairmant in Alzheimer’s disease. Neuropsychologia 1993, 31, 1147–1158. [Google Scholar] [CrossRef]
- Yan, J.H.; Rountree, S.; Massman, P.; Doody, R.S.; Li, H. Alzheimer’s disease and mild cognitive impairment deteriorate fine movement control. J. Psychiatr. Res. 2008, 42, 1203–1212. [Google Scholar] [CrossRef]
- Videt-Dussert, A.; Plonka, A.; Derreumaux, A.; Manera, V.; Leone, E.; Gros, A. Handwriting graphical parameters analysis in Posterior Cortical Atrophy: A case report. Clin. Neurol. Neurosurg. 2021, 208, 106876. [Google Scholar] [CrossRef] [PubMed]
- Impedovo, D.; Pirlo, G. Dynamic Handwriting Analysis for the Assessment of Neurodegenerative Diseases: A Pattern Recognition Perspective. IEEE Rev. Biomed. Eng. 2019, 12, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Macoir, J.; Lavoie, M.; Laforce, R.; Brambati, S.M.; Wilson, M.A. Dysexecutive Symptoms in Primary Progressive Aphasia: Beyond Diagnostic Criteria. J. Geriatr. Psychiatry Neurol. 2017, 30, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Fraser, K.C.; Meltzer, J.A.; Rudzicz, F. Linguistic Features Identify Alzheimer’s Disease in Narrative Speech. J. Alzheimers Dis. 2015, 49, 407–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| lvPPA | nfavPPA | svPPA | AD | HC | p-Value | |
|---|---|---|---|---|---|---|
| N | 20 | 6 | 6 | 22 | 26 | |
| Female, n (%) * | 8 (40%) | 3 (50%) | 3 (50%) | 9 (40.9%) | 18 (69%) | 0.081 |
| Age range (y) | 55–85 | 58–85 | 70–75 | 57–87 | 48–80 | |
| Mean age ** | 73.1 | 69.5 | 71.3 | 73.6 | 65.7 | 0.003 |
| SD age ** | 8.2 | 8.9 | 3.1 | 8.9 | 8.6 | |
| Mean Education (y) ** | 10.1 | 11.5 | 9.8 | 10.1 | 11.1 | 0.738 |
| Education SD ** | 3.8 | 3.7 | 5 | 4.8 | 5.4 | |
| Mean MMSE score ** | 23.6 | 20.5 | 20.7 | 21.5 | 28.5 | <0.001 |
| MMSE SD ** | 5.4 | 4.2 | 5 | 4.9 | 1.7 | |
| Mean DTLA score *** | 74.5 | 44.6 | 58.3 | 74.8 | 95.9 | <0.001 |
| DTLA SD *** | 16.6 | 10.9 | 19.9 | 17.1 | 5.6 |
| Task | Diagnosis | Mean | Standard Deviation | |
|---|---|---|---|---|
| Linguistic Tasks | Words | PPA AD Controls | 0.20 0.22 0.20 | 0.09 0.13 0.08 |
| Nonsense words | PPA AD Controls | 0.22 0.23 0.21 | 0.10 0.14 0.09 | |
| Sentence | PPA AD Controls | 0.23 0.26 0.22 | 0.11 0.13 0.09 | |
| Letter ‘l’ loops | PPA AD Controls | 0.25 0.28 0.26 | 0.12 0.15 0.10 | |
| Cognitive Non-Linguistic Tasks | Diagonal | PPA AD Controls | 0.28 0.26 0.24 | 0.14 0.13 0.10 |
| Vertical | PPA AD Controls | 0.28 0.30 0.22 | 0.08 0.15 0.12 | |
| Horizontal | PPA AD Controls | 0.21 0.31 0.18 | 0.55 0.21 0.08 | |
| Spiral | PPA AD Controls | 0.25 0.26 0.25 | 0.12 0.11 0.09 | |
| Non-Cognitive Non-Linguistic Tasks | Dots | PPA AD Controls | 0.17 0.19 0.13 | 0.07 0.09 0.04 |
| Filling Loops | PPA AD Controls | 0.28 0.31 0.27 | 0.11 0.15 0.09 |
| Task | Diagnosis | Mean | Standard Deviation | |
|---|---|---|---|---|
| Linguistic Tasks | Words | PPA AD Controls | 0.61 0.66 0.55 | 0.30 0.26 0.23 |
| Nonsense words | PPA AD Controls | 0.58 0.61 0.54 | 0.30 0.30 0.22 | |
| Sentence | PPA AD Controls | 0.65 0.78 0.53 | 0.33 0.27 0.25 | |
| Letter ‘l’ loops | PPA AD Controls | 0.45 0.48 0.44 | 0.23 0.22 0.23 | |
| Cognitive Non-Linguistic Tasks | Diagonal | PPA AD Controls | 0.54 0.49 0.42 | 0.27 0.25 0.21 |
| Vertical | PPA AD Controls | 0.55 0.57 0.43 | 0.19 0.23 0.21 | |
| Horizontal | PPA AD Controls | 0.45 0.58 0.32 | 0.21 0.30 0.16 | |
| Spiral | PPA AD Controls | 0.44 0.47 0.40 | 0.26 0.21 0.19 | |
| Non-Cognitive Non-Linguistic Tasks | Dots | PPA AD Controls | 0.73 0.71 0.53 | 0.27 0.25 0.24 |
| Filling Loops | PPA AD Controls | 0.52 0.54 0.51 | 0.20 0.22 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plonka, A.; Mouton, A.; Macoir, J.; Tran, T.-M.; Derremaux, A.; Robert, P.; Manera, V.; Gros, A. Primary Progressive Aphasia: Use of Graphical Markers for an Early and Differential Diagnosis. Brain Sci. 2021, 11, 1198. https://doi.org/10.3390/brainsci11091198
Plonka A, Mouton A, Macoir J, Tran T-M, Derremaux A, Robert P, Manera V, Gros A. Primary Progressive Aphasia: Use of Graphical Markers for an Early and Differential Diagnosis. Brain Sciences. 2021; 11(9):1198. https://doi.org/10.3390/brainsci11091198
Chicago/Turabian StylePlonka, Alexandra, Aurélie Mouton, Joël Macoir, Thi-Mai Tran, Alexandre Derremaux, Philippe Robert, Valeria Manera, and Auriane Gros. 2021. "Primary Progressive Aphasia: Use of Graphical Markers for an Early and Differential Diagnosis" Brain Sciences 11, no. 9: 1198. https://doi.org/10.3390/brainsci11091198